
Effects of Self-Care Education Intervention Program (SCEIP) on Activation Level, Psychological Distress, and Treatment-Related Information

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
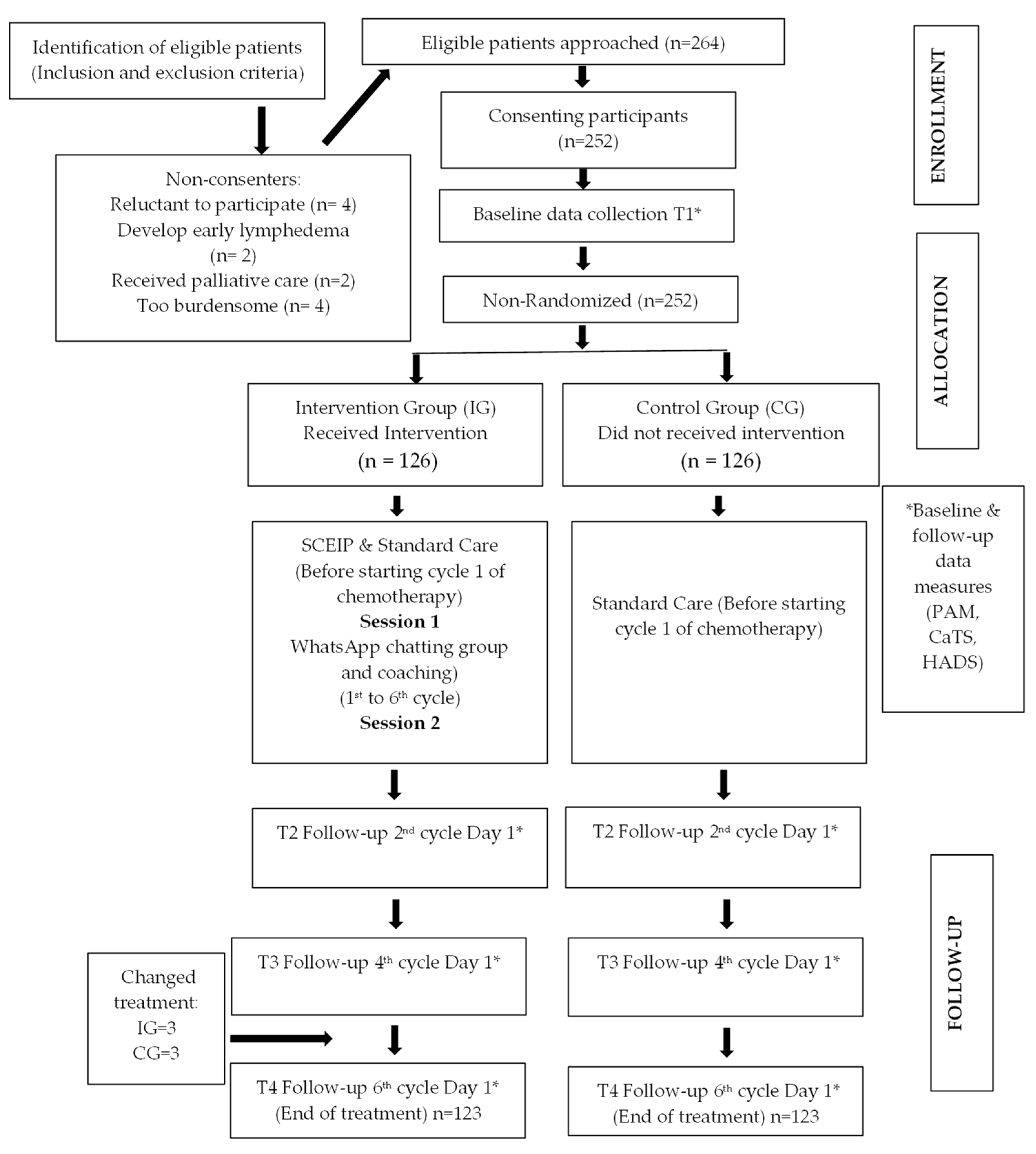
2.1. Study Design, Participants, and Procedures
2.2. Intervention
2.3. Standard Care
2.4. Research Instruments
2.4.1. Cancer Treatment Survey (CaTS)
2.4.2. Hospital Anxiety and Depression Scale (HADS)
2.4.3. Patient Activation Measure (PAM)
2.4.4. Ethical Consideration
2.5. Data Analysis Method
3. Results
3.1. Demographic and Medical Variables of Intervention and Control Groups
3.2. The Effectiveness of the SCEIP on Study Variables
3.2.1. Patient Activation Measure
3.2.2. Psychological Distress
3.2.3. Cancer Treatment Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charalambous, A.; Wells, M.; Campbell, P.; Torrens, C.; Östlund, U.; Oldenmenger, W.; Patiraki, E.; Sharp, L.; Nohavova, I.; Domenech-Climent, N.; et al. A scoping review of trials of interventions led or delivered by cancer nurses. Int. J. Nurs. Stud. 2018, 86, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Bana, M.; Ribi, K.; Kropf-Staub, S.; Näf, E.; Schramm, M.S.; Zürcher-Florin, S.; Peters, S.; Eicher, M. Development and implementation strategies of a nurse-led symptom self-management program in outpatient cancer centres: The Symptom Navi© Programme. Eur. J. Oncol. Nurs. 2020, 44, 101714. [Google Scholar] [CrossRef] [PubMed]
- Webber, D.; Guo, Z.; Mann, S. Self-care in health: We can define it, but should we also measure it. Selfcare 2013, 4, 101–106. [Google Scholar]
- Moursy, A.M.E.S.; Ead, A.Y.S. Self-Care Practices of Chemotherapy Patients. Life Sci. J. 2015, 12, 118–128. [Google Scholar]
- El-Nemer, A.M.R.; El-Zafrani, M.I.I.; El-Sayed, H.E.S.M.; Saadoon, O.H.M.M. Utilization of a Self-Care Educational Program for Alleviating Chemotherapy Induced Physical Side Effects. J. Cancer Treat. Res. 2015, 3, 8–16. [Google Scholar] [CrossRef]
- McCorkle, R.; Ercolano, E.; Lazenby, M.; Schulman-Green, D.; Schilling, L.S.; Lorig, K.; Wagner, E.H. Self-management: Enabling and empowering patients living with cancer as a chronic illness. CA Cancer J. Clin. 2011, 61, 50–62. [Google Scholar] [CrossRef]
- Howell, D.; Harth, T.; Brown, J.; Bennett, C.; Boyko, S. Self-management education interventions for patients with cancer: A systematic review. Support. Care Cancer 2017, 25, 1323–1355. [Google Scholar] [CrossRef]
- Budhwani, S.; Wodchis, W.P.; Zimmermann, C.; Moineddin, R.; Howell, D. Self-management, self-management support needs and interventions in advanced cancer: A scoping review. BMJ Support. Palliat. Care 2019, 9, 12–25. [Google Scholar] [CrossRef]
- Bonetti, L.; Tolotti, A.; Anderson, G.; Nania, T.; Vignaduzzo, C.; Sari, D.; Barello, S. Nursing interventions to promote patient engagement in CANCER care: A systematic review. Int. J. Nurs. Stud. 2022, 133, 104289. [Google Scholar] [CrossRef]
- Aranda, S.; Jefford, M.; Yates, P.; Gough, K.; Seymour, J.; Francis, P.; Baravelli, C.; Breen, S.; Schofield, P. Impact of a novel nurse-led prechemotherapy education intervention (ChemoEd) on patient distress, symptom burden, and treatment-related information and support needs: Results from a randomized, controlled trial. Ann. Oncol. 2012, 23, 222–231. [Google Scholar] [CrossRef]
- Coolbrandt, A.; Wildiers, H.; Aertgeerts, B.; Van der Elst, E.; Laenen, A.; de Casterle, B.D.; van Achterberg, T.; Milisen, K. Characteristics and effectiveness of complex nursing interventions aimed at reducing symptom burden in adult patients treated with chemotherapy: A systematic review of randomized controlled trials. Int. J. Nurs. Stud. 2014, 51, 495–510. [Google Scholar] [CrossRef]
- Coolbrandt, A.; Milisen, K.; Wildiers, H.; Aertgeerts, B.; van Achterberg, T.; Van der Elst, E.; de Casterlé, B.D. A nursing intervention aimed at reducing symptom burden during chemotherapy (CHEMO-SUPPORT): A mixed-methods study of the patient experience. Eur. J. Oncol. Nurs. 2018, 34, 35–41. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Tusler, M. Assessing activation stage and employing a “next steps” approach to supporting patient self-management. J. Ambul. Care Manag. 2007, 30, 2–8. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Mahoney, E.R.; Stock, R.; Tusler, M. Do increases in patient activation result in improved self-management behaviors? Health Serv. Res. 2007, 42, 1443–1463. [Google Scholar] [CrossRef]
- Greene, J.; Hibbard, J.H. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J. Gen. Intern. Med. 2012, 27, 520–526. [Google Scholar] [CrossRef]
- Greene, J.; Hibbard, J.H.; Sacks, R.; Overton, V.; Parrotta, C.D. When patient activation levels change, health outcomes and costs change too. Health Aff. 2015, 34, 431–437. [Google Scholar] [CrossRef]
- Tabrizi, J.S.; Wilson, A.J.; O’Rourke, P.K. Customer quality and type 2 diabetes from the patients’ perspective: A cross-sectional study. J. Res. Health Sci 2010, 10, 69–76. [Google Scholar]
- Salyers, M.P.; Godfrey, J.L.; McGuire, A.B.; Gearhart, T.; Rollins, A.L.; Boyle, C. Implementing the illness management and recovery program for consumers with severe mental illness. Psychiatr. Serv. 2009, 60, 483–490. [Google Scholar] [CrossRef]
- Fowles, J.B.; Terry, P.; Xi, M.; Hibbard, J.; Bloom, C.T.; Harvey, L. Measuring self-management of patients’ and employees’ health: Further validation of the Patient Activation Measure (PAM) based on its relation to employee characteristics. Patient Educ. Couns. 2009, 77, 116–122. [Google Scholar] [CrossRef]
- Wong, S.T.; Peterson, S.; Black, C. Patient activation in primary healthcare: A comparison between healthier individuals and those with a chronic illness. Med. Care 2011, 49, 469–479. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Cunningham, P.J. How Engaged are Consumers in Their Health and Health Care, and Why Does It Matter; Center for Studying Health System Change: Washington, DC, USA, 2008; pp. 1–9. [Google Scholar]
- Suls, J.; Wan, C.K. Effects of sensory and procedural information on coping with stressful medical procedures and pain: A meta-analysis. J. Consult. Clin. Psychol. 1989, 57, 372–379. [Google Scholar] [CrossRef]
- Schofield, P.; Gough, K.; Ugalde, A.; Carey, M.; Aranda, S.; Sanson-Fisher, R. Cancer Treatment Survey (CaTS): Development and validation of a new instrument to measure patients’ preparation for chemotherapy and radiotherapy. Psycho Oncol. 2012, 21, 307–315. [Google Scholar] [CrossRef]
- Halkett, G.K.; O’Connor, M.; Aranda, S.; Jefford, M.; Shaw, T.; York, D.; Spry, N.; Taylor, M.; Schofield, P. Pilot randomized controlled trial of a radiation therapist-led educational intervention for breast cancer patients prior to commencing radiotherapy. Support. Care Cancer 2013, 21, 1725–1733. [Google Scholar] [CrossRef]
- Waller, A.; Forshaw, K.; Bryant, J.; Mair, S. Interventions for preparing patients for chemotherapy and radiotherapy: A systematic review. Support. Care Cancer 2014, 22, 2297–2308. [Google Scholar] [CrossRef]
- Halkett, G.K.; Kristjanson, L.J.; Lobb, E.; Little, J.; Shaw, T.; Taylor, M.; Spry, N. Information needs and preferences of women as they proceed through radiotherapy for breast cancer. Patient Educ. Couns. 2012, 86, 396–404. [Google Scholar] [CrossRef]
- Forshaw, K.L.; Carey, M.L.; Hall, A.E.; Boyes, A.W.; Sanson-Fisher, R. Preparing patients for medical interventions: A systematic review of the psychometric qualities of published instruments. Patient Educ. Couns. 2016, 99, 960–973. [Google Scholar] [CrossRef]
- Dodd, M.; Janson, S.; Facione, N.; Faucett, J.; Froelicher, E.S.; Humphreys, J.; Lee, K.; Miaskowski, C.; Puntillo, K.; Rankin, S.; et al. Advancing the science of symptom management. J. Adv. Nurs. 2001, 33, 668–676. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I. Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ Br. Med. J. 2008, 337, a1655. [Google Scholar] [CrossRef]
- Blackwood, B. Methodological issues in evaluating complex healthcare interventions. J. Adv. Nurs. 2006, 54, 612–622. [Google Scholar] [CrossRef]
- Eccles, M.; Grimshaw, J.; Campbell, M.; Ramsay, C. Research designs for studies evaluating the effectiveness of change and improvement strategies. BMJ Qual. Saf. 2003, 12, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-F.; Hemming, K.; Stevens, A.J.; Lilford, R.J. Secular trends and evaluation of complex interventions: The rising tide phenomenon. BMJ Qual. Saf. 2016, 25, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Hooper, R.; Froud, R.J.; Bremner, S.A.; Perera, R.; Eldridge, S. Cascade diagrams for depicting complex interventions in randomized trials. BMJ Brit. Med. J. 2013, 347, f6681. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; pp. 18–74. [Google Scholar]
- Nor Aziyan, Y. Development of a Self-Care Education Intervention Program and Its Effectiveness Outcomes among Women with Breast Cancer Undergoing Chemotherapy. Ph.D. Thesis, Universiti Malaya, Kuala Lumpur, Malaysia, 24 March 2021. [Google Scholar]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G. Intervention mapping: A process for developing theory and evidence-based health education programs. Health Educ. Behav. 1998, 25, 545–563. [Google Scholar] [CrossRef]
- Bartholomew, L.K.; Markham, C.M.; Ruiter, R.A.; Fernández, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs: An Intervention Mapping Approach, 4th ed.; Jossey-Bass, John Wiley & Sons: Hoboken, NJ, USA, 2016; pp. 209–585. [Google Scholar]
- Miller, W.R.; Rollnick, S. The effectiveness and ineffectiveness of complex behavioral interventions: Impact of treatment fidelity. Contemp. Clin. Trials 2014, 37, 234–241. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Peters, G.J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Borsa, J.C.; Damásio, B.F.; Bandeira, D.R. Cross-cultural adaptation and validation of psychological instruments: Some considerations. Paidéia (Ribeirão Preto) 2012, 22, 423–432. [Google Scholar] [CrossRef]
- Lise, F.; Schwartz, E.; Friedemann, M.L.; Anderson, K.H. Proposal for cross-cultural adaptation and validation of the instrument. J. Nurs. UFPE Online 2018, 12, 808–811. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Vodermaier, A.; Millman, R.D. Accuracy of the Hospital Anxiety and Depression Scale as a screening tool in cancer patients: A systematic review and meta-analysis. Support. Care Cancer 2011, 19, 1899–1908. [Google Scholar] [CrossRef]
- Hashim, Z. Reliability and Validity of Hospital Anxiety and Depression Scale (HADS) on Breast Cancer Survivors: Malaysia Case Study. Asia Pac. Environ. Occup. Health J. 2016, 2, 19–24. [Google Scholar]
- Insignia Health. Patient Activation Measure (PAM 13). TM Licence Materials Copyright; Insignia Health, LLC: Portland, OR, USA, 2011. [Google Scholar]
- Ngooi, B.X.; Packer, T. What Are the Crucial Components of Patient Activation Interventions? Biomed. J. Sci Technol. Res. 2017, 1, 439–452. [Google Scholar] [CrossRef]
- Verot, E.; Bouleftour, W.; Macron, C.; Rivoirard, R.; Chauvin, F. Effect of PARACT (PARAmedical Interventions on Patient ACTivation) on the Cancer Care Pathway: Protocol for Implementation of the Patient Activation Measure-13 Item (PAM-13) Version. JMIR Res. Protoc. 2020, 9, 17485. [Google Scholar] [CrossRef]
- Hibbard, J.; Gilburt, H. Supporting People to Manage Their Health. An Introduction to Patient Activation; The King’s Fund: London, UK, 2014; pp. 2–51. [Google Scholar]
- Hibbard, J.H.; Mahoney, E.; Sonet, E. Does patient activation level affect the cancer patient journey? Patient Educ. Couns. 2017, 100, 1276–1279. [Google Scholar] [CrossRef]
- Lindner, H.; Menzies, D.; Kelly, J.; Taylor, S.; Shearer, M. Coaching for behaviour change in chronic disease: A review of the literature and the implications for coaching as a self-management intervention. Aust. J. Prim. Health 2003, 9, 177–185. [Google Scholar] [CrossRef]
- Solomon, M.; Wagner, S.L.; Goes, J. Effects of a Web-based intervention for adults with chronic conditions on patient activation: Online randomized controlled trial. J. Med. Internet Res. 2012, 14, e1924. [Google Scholar] [CrossRef]
- Bartels, S.J.; Aschbrenner, K.A.; Rolin, S.A.; Hendrick, D.C.; Naslund, J.A.; Faber, M.J. Activating older adults with serious mental illness for collaborative primary care visits. Psychiatr. Rehabil. J. 2013, 36, 278–288. [Google Scholar] [CrossRef]
- Magnezi, R.; Bergman, Y.S.; Grosberg, D. Online activity and participation in treatment affects the perceived efficacy of social health networks among patients with chronic illness. J. Med. Internet Res. 2014, 16, e2630. [Google Scholar] [CrossRef]
- Periasamy, U.; Sidik, S.; Rampal, L.; Ismail, S.I.F. Outcome of chemotherapy counseling by pharmacists on psychological effects and self-esteem among oncology patients in a Government Hospital in Malaysia. Int. Med. J. Malays. 2015, 70, 131–141. [Google Scholar]
- Periasamy, U.; Mohd Sidik, S.; Rampal, L.; Fadhilah, S.I.; Akhtari-Zavare, M.; Mahmud, R. Effect of chemotherapy counseling by pharmacists on quality of life and psychological outcomes of oncology patients in Malaysia: A randomized control trial. Health Qual. 2017, 15, 104. [Google Scholar] [CrossRef]
- Mohd-Sidik, S.; Akhtari-Zavare, M.; Periasamy, U.; Rampal, L.; Fadhilah, S.I.; Mahmud, R. Effectiveness of chemotherapy counselling on self-esteem and psychological affects among cancer patients in Malaysia: Randomized controlled trial. Patient Educ. Couns. 2018, 101, 862–871. [Google Scholar] [CrossRef]
- Williams, S.; Dale, J. The effectiveness of treatment for depression/depressive symptoms in adults with cancer: A systematic review. Br. J. Cancer 2006, 94, 372–390. [Google Scholar] [CrossRef]
- Osborn, R.L.; Demoncada, A.C.; Feuerstein, M. Psychosocial interventions for depression, anxiety, and quality of life in cancer survivors: Meta-analyses. Int. J. Psychiatry Med. 2006, 36, 13–34. [Google Scholar] [CrossRef]
- Spencer, J.C.; Wheeler, S.B. A systematic review of Motivational Interviewing interventions in cancer patients and survivors. Patient Educ. Couns. 2016, 99, 1099–1105. [Google Scholar] [CrossRef]
- Johnson, J.E. Psychological interventions and coping with surgery. In Handbook of Psychology and Health (Volume IV); Taylor, S.E., Singer, J.E., Baum, A., Eds.; Routledge: London, UK, 2020; Volume 4, pp. 167–187. [Google Scholar]
- Roussi, P.; Miller, S.M. Monitoring style of coping with cancer related threats: A review of the literature. J. Behav. Med. 2014, 37, 931–954. [Google Scholar] [CrossRef] [PubMed]
- Vosbergen, S.; Peek, N.; Mulder-Wiggers, J.M.; Kemps, H.M.; Kraaijenhagen, R.A.; Jaspers, M.W.; Lacroix, J.P. An online survey to study the relationship between patients’ health literacy and coping style and their preferences for self-management-related information. Patient Prefer. Adherence 2014, 8, 631–642. [Google Scholar] [CrossRef]
- Kwan, C.M.; Chun, K.M.; Chesla, C.A. Cultural norms shaping research group interviews with Chinese American immigrants. Asian Am. J. Psychol. 2011, 2, 115. [Google Scholar] [CrossRef]


{kind=link}
| Variables | IG (n = 123) | CG (n = 123) | df | t/χ2 | p-Value | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Age, years | |||||||
| Mean | 123 | 50.14 | 123 | 49.89 | 244 | 0.192 ª | 0.848 |
| SD | ±9.48 | ±11.03 | |||||
| Age range | 30–71 | 24–75 | |||||
| Ethnic group | |||||||
| Malay | 80 | 65 | 76 | 61.8 | 2 | 0.618 ª | 0.734 |
| Chinese | 23 | 18.7 | 28 | 22.8 | |||
| Indian | 20 | 16.3 | 19 | 15.4 | |||
| Educational level | |||||||
| Primary | 24 | 19.5 | 30 | 24.4 | 2 | 2.008 ª | 0.366 |
| Secondary | 68 | 55.3 | 57 | 46.3 | |||
| Tertiary | 31 | 25.2 | 36 | 29.3 | |||
| Marital status | |||||||
| Single/divorced/widowed | 26 | 21.1 | 25 | 20.3 | 1 | 0.025 ª | 0.875 |
| Married | 97 | 78.9 | 98 | 79.7 | |||
| Employment status | |||||||
| Working | 54 | 43.9 | 52 | 42.3 | 1 | 0.066 ª | 0.797 |
| Not working | 69 | 56.1 | 71 | 57.7 | |||
| Income level | |||||||
| Less than RM 1500 | 31 | 25.2 | 35 | 28.5 | 2 | 2.492 ª | 0.288 |
| RM 1501–3000 | 37 | 30.1 | 45 | 36.5 | |||
| More than RM 3001 | 55 | 44.7 | 43 | 35.0 | |||
| Menopausal status | |||||||
| Pre-menopausal | 65 | 52.8 | 65 | 52.8 | 1 | 0.000 ª | 1.000 |
| Post-menopausal | 58 | 47.2 | 58 | 47.2 | |||
| ECOG performance status | |||||||
| 0 | 53 | 43.1 | 57 | 46.3 | 1 | 0.263 ª | 0.608 |
| 1 | 70 | 56.9 | 66 | 53.7 | |||
| Staging of cancer | |||||||
| I | 6 | 4.9 | 3 | 2.5 | 2 | 1.011 b | 0.677 |
| II | 47 | 38.2 | 48 | 39.0 | |||
| III | 70 | 56.9 | 72 | 58.5 | |||
| Chemotherapy regimen | |||||||
| Anthracycline alone | 60 | 48.8 | 73 | 59.3 | 1 | 2.766 ª | 0.125 |
| Anthracycline- and taxane-based | 63 | 51.2 | 50 | 41.7 | |||
| Measure | Time | Group | |
|---|---|---|---|
| Intervention M (±SD) | Control M (±SD) | ||
| Patient Activation Level | Baseline (T1) | 64.79 (7.66) a,x | 64.92 (8.63) a,x |
| Cycle 2 (T2) | 66.97 (7.87) a,x,y | 62.69 (6.80) b,x,y | |
| Cycle 4 (T3) | 67.00 (7.93) a,y | 62.34 (8.26) b,y | |
| Cycle 6 (T4) | 68.13 (7.84) a,z | 61.23 (2.54) b,z | |
| Measure | Time | Group | |
|---|---|---|---|
| Intervention M (±SD) | Control M (±SD) | ||
| Anxiety | Baseline (T1) | 5.84 (3.54) a,x | 5.98 (3.63) a,x |
| Depression | 4.10 (3.08) a,x | 4.60 (3.30) a,x | |
| Anxiety | Cycle 2 (T2) | 2.80 (2.19) a,x,y | 4.72 (3.05) b,x,y |
| Depression | 3.27 (2.51) a,x,y | 4.77 (3.42) b,x,y | |
| Anxiety | Cycle 4 (T3) | 4.24 (3.09) a,y | 5.01 (3.40) b,y |
| Depression | 3.76 (2.52) a,y | 4.55 (3.40) b,y | |
| Anxiety | Cycle 6 (T4) | 3.98 (2.52) a,z | 5.13 (3.30) b,z |
| Depression | 4.03 (2.73) a,z | 4.66 (3.28) b,z | |
| Measure | Group | Pre-Test (T1) M (±SD) | p-Value (Between Group) | Post-Test (T4) M (±SD) | p-Value (Between Group) | p-Value (Within Group) |
|---|---|---|---|---|---|---|
| CaTS-SPC | Control | 3.73 (0.38) | 0.955 | 3.14 (0.82) | 0.042 * | <0.001 ** |
| Intervention | 3.72 (0.42) | 2.90 (1.04) | <0.001 ** | |||
| CaTS-PC | Control | 4.18 (0.41) | 0.250 | 3.83 (0.23) | <0.001 ** | <0.001 ** |
| Intervention | 4.24 (0.42) | 3.21 (1.27) | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yahaya, N.A.; Abdullah, K.L.; Ramoo, V.; Zainal, N.Z.; Wong, L.P.; Danaee, M. Effects of Self-Care Education Intervention Program (SCEIP) on Activation Level, Psychological Distress, and Treatment-Related Information. Healthcare 2022, 10, 1572. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10081572
Yahaya NA, Abdullah KL, Ramoo V, Zainal NZ, Wong LP, Danaee M. Effects of Self-Care Education Intervention Program (SCEIP) on Activation Level, Psychological Distress, and Treatment-Related Information. Healthcare. 2022; 10(8):1572. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10081572
Chicago/Turabian StyleYahaya, Nor Aziyan, Khatijah Lim Abdullah, Vimala Ramoo, Nor Zuraida Zainal, Li Ping Wong, and Mahmoud Danaee. 2022. "Effects of Self-Care Education Intervention Program (SCEIP) on Activation Level, Psychological Distress, and Treatment-Related Information" Healthcare 10, no. 8: 1572. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10081572