
Clinical Characteristics of Lower-Limb Ischemia in Japanese Patients with Type 2 Diabetes and Usefulness of the Great Toe Blood Flow as a Predictive Indicator of Leg Arterial Obstruction

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
2.3. Physiological Measurement
2.3.1. ABI Value
2.3.2. Toe Blood Flow
2.3.3. Acceleration Pulse Wave Aging Index
2.3.4. TcPO2 of the Dorsal Foot
2.4. Examination Procedure
2.5. Data Analysis
3. Results
3.1. Overview of the Participants
3.2. Comparison of Demographic Data, Diabetic Complications, and Pre-Existing Diseases by the Degree of Lower-Limb Obstruction
3.3. Comparison of the Presence or Absence of Subjective and Objective Symptoms of Ischemia by the Degree of Lower-Limb Obstruction
3.4. Comparison of Physiological Indicators by the Degree of Lower-Limb Obstruction
3.5. Prediction of Lower-Limb Arterial Obstruction by the Physiological Index
4. Discussion
5. Limitations of This Study
6. Conclusions
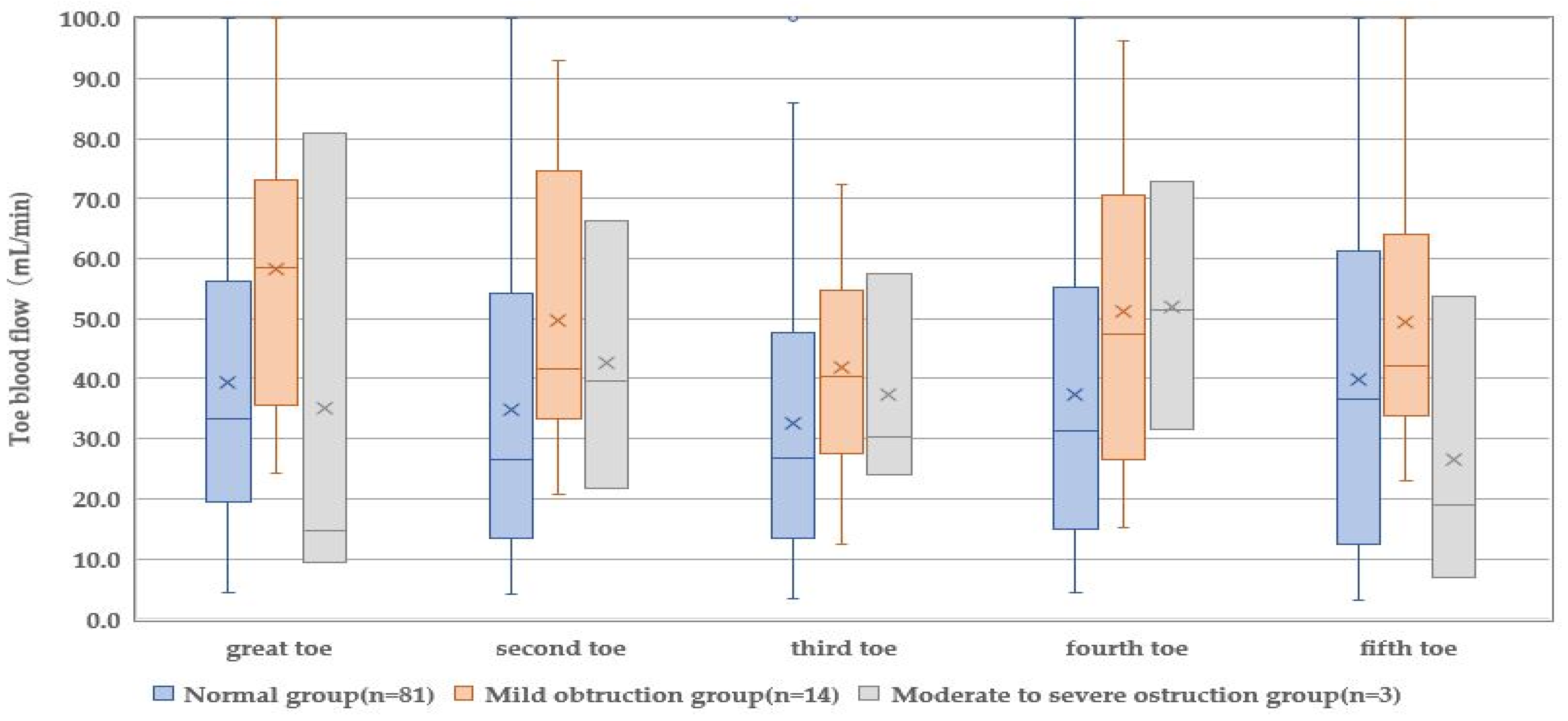
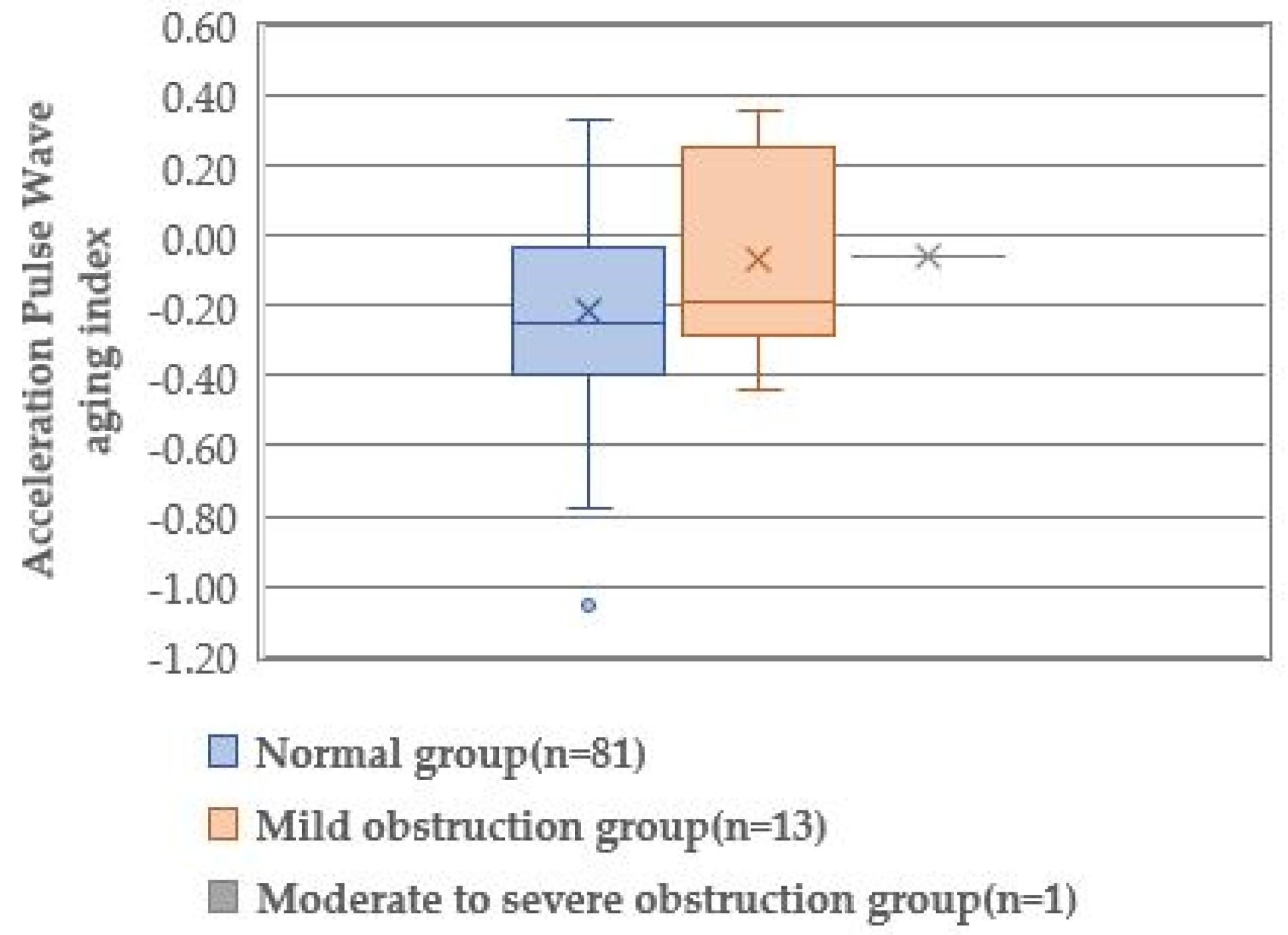
- Subjective symptoms of impaired blood flow and other symptoms such as pain at rest, cold sensation, skin pallor, and unpalpable dorsal foot artery were required when the ABI was ≤0.69. Toe blood flow was the lowest in the great toe, but the accelerated pulse wave aging index suggested progressive arteriosclerosis, and TcpO2 showed no characteristic values.
- Binomial logistic regression analysis was performed on the relationship between the presence of impaired blood flow in the lower limbs and physiological indices in patients with T2D, and the great toe blood flow by pocket LDF was established as predictive of impaired blood flow in the lower limbs.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare. The Patient Survey 2017. 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kanja/17/dl/toukei.pdf (accessed on 15 June 2022). (In Japanese).
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef]
- Sen, P.; Demirdal, T.; Emir, B. Meta-analysis of risk factors for amputation in diabetic foot infections. Diabetes Metab. Res. Rev. 2019, 35, e3165. [Google Scholar] [CrossRef]
- Chan, J.C.N.; Lim, L.L.; Wareham, N.J.; Shaw, J.E.; Orchard, T.J.; Zhang, P.; Lau, E.S.H.; Eliasson, B.; Kong, A.P.S.; Ezzati, M.; et al. The Lancet Commission on diabetes: Using data to transform diabetes care and patient lives. Lancet 2021, 396, 2019–2082. [Google Scholar] [CrossRef]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J.A.; Eid, M.A.; Creager, M.A.; Goodney, P.P. Epidemiology and risk of amputation in patients with diabetes mellitus and peripheral artery disease. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1808–1817. [Google Scholar] [CrossRef] [PubMed]
- Pinzur, M.S.; Kernan-Schroeder, D.; Emanuele, N.V.; Emanuel, M. Development of a nurse-provided health system strategy for diabetic foot care. Foot Ankle Int. 2001, 22, 744–746. [Google Scholar] [CrossRef]
- Sakamoto, A.; Ikeda, M. A survey on foot care for diabetic patients in Kochi. J. Kochi Women’s Univ. Acad. Nurs. 2018, 44, 136–144. (In Japanese) [Google Scholar]
- Gazzaruso, C.; Coppola, A.; Falcone, C.; Luppi, C.; Montalcini, T.; Baffero, E.; Gallotti, P.; Pujia, A.; Solerte, S.B.; Pelissero, G.; et al. Transcutaneous oxygen tension as a potential predictor of cardiovascular events in type 2 diabetes: Comparison with ankle-brachial index. Diabetes Care 2013, 36, 1720–1725. [Google Scholar] [CrossRef]
- Mackiewicz-Wysocka, M.; Araszkiewicz, A.; Schlaffke, J.; Kuczynski, S.; Micek, I.; Zozulinska-Ziolkiewicz, D. Lower melanin content in the skin of type 1 diabetic patients and the risk of microangiopathy. Exp. Clin. Endocrinol. Diabetes 2014, 122, 231–235. [Google Scholar] [CrossRef]
- Holland-Letz, T.; Endres, H.G.; Biedermann, S.; Mahn, M.; Kunert, J.; Groh, S.; Pittrow, D.; von Bilderling, P.; Sternitzky, R.; Diehm, C. Reproducibility and reliability of the ankle-brachial index as assessed by vascular experts, family physicians and nurses. Vasc. Med. 2007, 12, 105–112. [Google Scholar] [CrossRef]
- Casey, S.L.; Lanting, S.M.; Chuter, V.H. The ankle brachial index in people with and without diabetes: Intra-tester reliability. J. Foot Ankle Res. 2020, 13, 21. [Google Scholar] [CrossRef] [PubMed]
- Takazawa, K.; Tanaka, N.; Fujita, M.; Matsuoka, O.; Saiki, T.; Aikawa, M.; Tamura, S.; Ibukiyama, C. Assessment of vasoactive agents and vascular aging by the second derivative of photoplethysmogram waveform. Hypertension 1998, 32, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Potier, L.; Abi Khalil, C.A.; Mohammedi, K.; Roussel, R. Use and utility of ankle brachial index in patients with diabetes. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Silvestre, E.; Somerville, M.; Bisset, L.; Coppieters, M.W. Altered pain processing in patients with type 1 and 2 diabetes: Systematic review and meta-analysis of pain detection thresholds and pain modulation mechanisms. BMJ Open Diabetes Res. Care 2020, 8, e001566. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Chong, C.K.; Sheu, J.J. Prevalence and risk factors of sensory symptoms in diabetes patients in Taiwan. Front. Endocrinol. 2020, 11, 580426. [Google Scholar] [CrossRef]
- Robertson, G.S.; Ristic, C.D.; Bullen, B.R. The incidence of congenitally absent foot pulses. Ann. R. Coll. Surg. Engl. 1990, 72, 99–100. [Google Scholar]
- Vijayalakshmi, S.; Raghunath, G.; Shenoy, V. Anatomical study of dorsalis pedis artery and its clinical correlations. J. Clin. Diag. Res. 2011, 5, 287–290. [Google Scholar]
- Quebedeaux, T.L.; Lavery, L.A.; Lavery, D.C. The development of foot deformities and ulcers after great toe amputation in diabetes. Diabetes Care 1996, 19, 165–167. [Google Scholar] [CrossRef]
- Mills, J.L.S.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on wound, ischemia, and foot infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234.e2. [Google Scholar] [CrossRef]
- Fejfarová, V.; Matuška, J.; Jude, E.; Piťhová, P.; Flekač, M.; Roztočil, K.; Wosková, V.; Dubský, M.; Jirkovská, A.; Bém, R.; et al. Stimulation TcPO2 testing improves diagnosis of peripheral arterial disease in patients with diabetic foot. Front. Endocrinol. 2021, 12, 744195. [Google Scholar] [CrossRef]
- Ubbink, D.T.; Jacobs, M.J.; Tangelder, G.J.; Slaaf, D.W.; Reneman, R.S. The usefulness of capillary microscopy, transcutaneous oximetry and laser Doppler fluxmetry in the assessment of the severity of lower limb ischaemia. Int. J. Microcirc. Clin. Exp. 1994, 14, 34–44. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Normal Group (n = 81) | Mild Obstruction Group (n = 14) | Moderate-to-Severe Obstruction Group (n = 3) | p a |
|---|---|---|---|---|
| Age (years) | 73.0 (65.0–83.0) | 73.0 (68.0–76.0) | 73.0 (68.0–75.0) | 0.973 |
| Diabetes history (years) | 13 (1.0–49.0) | 20.0 (13.0–37.0) | 20.0 (12.3–13.0) | 0.437 |
| HbA1c (%) | 7.1 (5.3–9.8) | 7.1 (6.7–7.4) | 7.1 (6.7–7.4) | 0.949 |
| Hb (g/dL) | 13.6 (11.3–17.8) | 12.3 (11.3–14.2) | 12.3 (11.3–14.2) | 0.300 |
| Variable | Normal Group (n = 81) | Mild Obstruction Group (n = 14) | Moderate-to-Severe Obstruction Group (n = 3) | p a | |||
|---|---|---|---|---|---|---|---|
| Absent (%) | Present (%) | Absent (%) | Present (%) | Absent (%) | Present (%) | ||
| Diabetes neuropathy | 74 (91.4) | 7 (8.6) | 14 (100.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | 0.001 |
| Diabetic retinopathy | 79 (97.5) | 2 (2.5) | 11 (78.6) | 3 (21.4) | 1 (33.3) | 2 (66.7) | <0.001 |
| Diabetic nephropathy | 81 (100.0) | 0 (0.0) | 14 (100.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | <0.001 |
| Hypertension | 48 (60.8) | 31 (39.2) | 4 (28.6) | 10 (71.4) | 2 (66.7) | 1 (33.3) | 0.077 |
| Hyperlipidemia | 71 (89.9) | 8 (10.1) | 13 (92.9) | 1 (7.1) | 3 (100.0) | 0 (0.0) | 0.806 |
| Arterioscleosis obliterans | 81(100.0) | 0 (0.0) | 14 (100.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | <0.001 |
| Ischemic heart disease/cerebrovascular disease | 65 (80.2) | 16 (19.8) | 12 (85.7) | 2 (14.3) | 2(66.7) | 1 (33.3) | 0.074 |
| Variable | Normal Group (n = 81) | Mild Obstruction Group (n = 14) | Moderate-to-Severe Obstruction Group (n = 3) | pa | |||
|---|---|---|---|---|---|---|---|
| Absent (%) | Present (%) | Absent (%) | Present (%) | Absent (%) | Present (%) | ||
| Subjective symptom | |||||||
| Cold sensation | 59 (72.8) | 22 (27.2) | 13 (92.9) | 1 (7.1) | 3 (100.0) | 0 (0.0) | 0.168 |
| Numbness | 63 (77.8) | 18 (22.2) | 11 (78.6) | 3 (21.4) | 3 (100.0) | 0 (0.0) | 0.008 |
| Resting pain | 81 (100.0) | 0 (0.0) | 14 (100.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | <0.001 |
| Objective symptom | |||||||
| Cold sensation | 49 (60.5) | 32 (39.5) | 13 (92.9) | 1 (7.1) | 1 (33.3) | 2 (66.7) | 0.034 |
| Pallor | 70 (86.4) | 11 (13.6) | 13 (92.9) | 1 (7.1) | 1 (33.3) | 2 (66.7) | 0.025 |
| Dry skin | 45 (55.6) | 36 (44.4) | 5 (35.7) | 9 (64.3) | 3 (100.0) | 0 (0.0) | 0.106 |
| Palpation of the dorsalis pedis artery | 4 (4.9) | 77 (95.1) | 2 (14.3) | 12 (85.7) | 2 (66.7) | 1 (33.3) | <0.001 |
| Palpation of the posterior tibial artery | 14 (17.3) | 67 (82.7) | 3 (23.1) b | 10 (76.9) | 3 (100.0) | 0 (0.0) | 0.002 |
| Variable | Partial Regression Variable | Standard Error | Wald | p | Odds Ratio | 95% Confidence Interval for Odds Ratio | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Blood flow in the the great toe Variable | −0.021 2.579 | 0.010 0.586 | 4.425 19.383 | 0.035 < 0.001 | 0.979 13.181 | 0.900 | 0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakamoto, A.; Ikeda, M. Clinical Characteristics of Lower-Limb Ischemia in Japanese Patients with Type 2 Diabetes and Usefulness of the Great Toe Blood Flow as a Predictive Indicator of Leg Arterial Obstruction. Healthcare 2022, 10, 1753. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10091753
Sakamoto A, Ikeda M. Clinical Characteristics of Lower-Limb Ischemia in Japanese Patients with Type 2 Diabetes and Usefulness of the Great Toe Blood Flow as a Predictive Indicator of Leg Arterial Obstruction. Healthcare. 2022; 10(9):1753. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10091753
Chicago/Turabian StyleSakamoto, Aya, and Mitsunori Ikeda. 2022. "Clinical Characteristics of Lower-Limb Ischemia in Japanese Patients with Type 2 Diabetes and Usefulness of the Great Toe Blood Flow as a Predictive Indicator of Leg Arterial Obstruction" Healthcare 10, no. 9: 1753. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10091753