
Knowledge, Practice, Compliance, and Barriers toward Ventilator-Associated Pneumonia among Critical Care Nurses in Eastern Mediterranean Region: A Systematic Review

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.4. Study Identification
2.5. Risk of Bias
3. Results
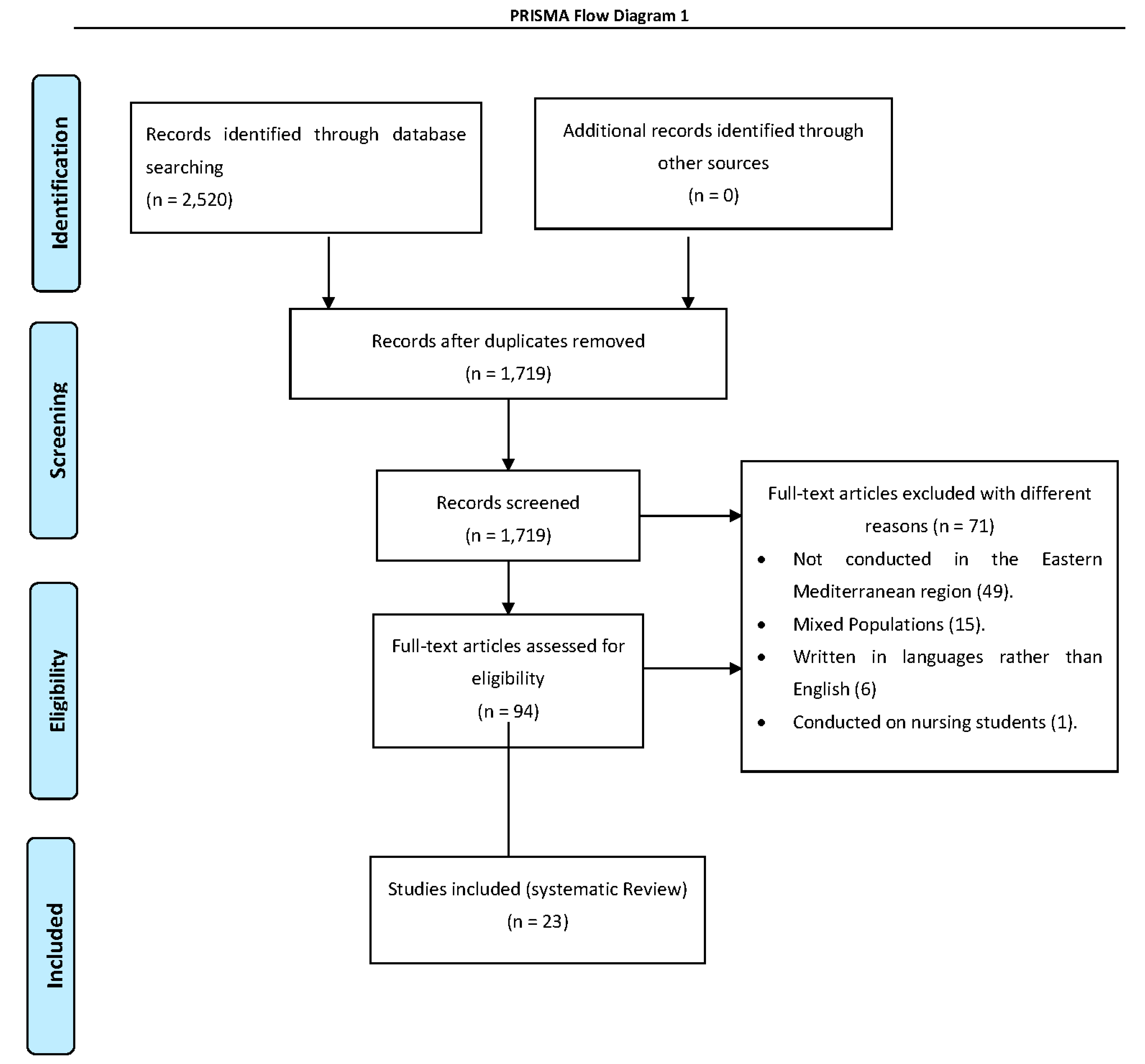
3.1. Study Selection
3.2. Study Characteristics
3.3. Used Instruments
3.4. Nurses’ General Knowledge of VAP
3.5. Nurses’ Compliance and Practice of VAP
3.6. Quality of Studies
3.7. Barriers to Adherence to VAP Guidelines
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pradhan, R.; Singh, S.; Modi, C.; Khandelwal, V.; Agrawal, R. Antimicrobial susceptibility pattern of isolates from cases of ventilator associated pneumonia (VAP) in medical and surgical intensive care units. Natl. J. Integr. Res. Med. 2017, 8, 48–53. [Google Scholar]
- İşgüder, R.; Gökhan, C.; Hasan, A.; Gamze, G.; Yüce, A.; İlker, D. New parameters for childhood ventilator associated pneumonia diagnosis. Pediatr. Pulmonol. 2017, 52, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Azzab, M.M.; El-Sokkary, R.H.; Tawfeek, M.M.; Gebriel, M.G. Multidrug-resistant bacteria among patients with ventilator-associated pneumonia in an emergency intensive care unit, Egypt. East. Mediterr. Health. J. 2016, 22, 894–903. [Google Scholar] [CrossRef] [PubMed]
- Yepez, E.S.; Bovera, M.M.; Rosenthal, V.D. Device associated infection rates, mortality, length of stay and bacterial resistance in intensive care units in Ecuador: International Nosocomial Infection Control Consortium’s findings. World J. Biol. Chem. 2017, 8, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Alp, E.; Kalin, G.; Coskun, R.; Sungur, M.; Guven, M.; Doganay, M. Economic burden of ventilator associated pneumonia in a developing country. J. Hosp. Infect. 2012, 81, 128–130. [Google Scholar] [PubMed]
- Galal, Y.S.; Youssef, L.; Ibrahiem, K. Ventilator-Associated Pneumonia: Incidence, Risk Factors and Outcome in Paediatric Intensive Care Units at Cairo University Hospital. J. Clin. Diagn. Res. 2016, 10, 6–11. [Google Scholar] [CrossRef]
- Farag, A.M.; Tawfick, M.M.; Abozeed, M.Y.; Shaban, E.A.; Abo-Shadi, M.A. Microbiological profile of ventilator-associated pneumonia among intensive care unit patients in tertiary Egyptian hospitals. J. Infect. Dev. Ctries. 2020, 14, 153–161. [Google Scholar] [CrossRef]
- Shahabi, M.; Yousefi, H.; Yazdannik, A.R.; Alikiaii, B. The effect of daily sedation interruption protocol on early incidence of ventilator-associated pneumonia among patients hospitalized in critical care units receiving mechanical ventilation. Iran. J. Nurs. Midwifery Res. 2016, 21, 541–546. [Google Scholar]
- Samrah, S.; Bashtawi, Y.; Hayajneh, W.; Almomani, B.; Momany, S.; Khader, Y. Impact of colistin-initiation delay on mortality of ventilator-associated pneumonia caused by A. baumannii. J. Infect. Dev. Ctries. 2016, 10, 1129–1134. [Google Scholar] [CrossRef]
- Torres-Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez, V.P.; Hanberger, H.; Wunderink, R. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar]
- Klompas, M.; Branson, R.; Eichenwald, E.C.; Linda, R.; Michael, D.; Grace, L.; Society for Healthcare Epidemiology of America (SHEA). Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update Infect. Infect. Control. Hosp. Epidemiol. 2014, 35, 133–154. [Google Scholar] [CrossRef] [PubMed]
- Fathy, A.; Abdelhafeez, R.; El-Gilany, A.; AbdElhafez, S.A. Analysis of ventilator associated pneumonaia (VAP) studies in Egyptian University Hospitals. Egypt J. Chest. Dis. Tuberc. 2013, 62, 17–25. [Google Scholar] [CrossRef]
- Xie, D.S.; Xiong, W.; Lai, R.P.; Liu, L.; Gan, X.M.; Wang, X.H.; Shao, F.N. Ventilator-associated pneumonia in intensive care units in Hubei Province, China: A multicenter prospective cohort survey. J. Hosp. Infect. 2011, 78, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Rafiei, H.; Rahimi, S.; Shafaei, H.; Ommatmohammadi, M. Emergency nurses’ knowledge about ventilator-associated pneumonia. Int. Emerg. Nurs. 2019, 48, 100783. [Google Scholar] [CrossRef]
- Al-Mugheed, K.; Bayraktar, N. Patient safety attitudes among critical care nurses: A case study in North Cyprus. Int. J. Health. Plann. Manag. 2020, 35, 910–921. [Google Scholar] [CrossRef]
- Al-Mugheed, K.; Bayraktar, N.; Al-Bsheish, M.; AlSyouf, A.; Jarrar, M.; AlBaker, W.; Aldhmadi, B.K. Patient Safety Attitudes among Doctors and Nurses: Associations with Workload, Adverse Events, Experience. Healthcare 2022, 10, 631. [Google Scholar] [CrossRef]
- Hellyer, P.; Ewan, V.; Wilson, P.; Simpson, J. The Intensive Care Society recommended bundle of interventions for the prevention of ventilator-associated pneumonia. J. Intensive Care. Soci. 2016, 17, 238–243. [Google Scholar] [CrossRef]
- American Thoracic Society, Infectious Diseases Society of America. Guidelines for the Management of Adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef]
- Tablan, O.; Anderson, L.; Besser, R.; Bridges, C.; Hajjeh, R.; CDC; healthcare infection control practices advisory committee. Guidelines for preventing health-care-associated pneumonia, 2003: Recommendations of CDC and the healthcare infection control practices advisory committee. MMWR-Recomm. Rep. 2004, 53, 1–36. [Google Scholar]
- IHI. How-to Guide: Prevent Ventilator Associated Pneumonia; Institute for Healthcare Improvement: Cambridge, UK, 2012. [Google Scholar]
- Akın, K.E.; Hakverdioğlu, Y.G.; Parlar, K.S.; Uzelli, D. Knowledge levels of intensive care nurses on prevention of ventilator-associated pneumonia. Nurs. Crit. Care 2014, 19, 26–33. [Google Scholar] [CrossRef]
- Al-Sayaghi, K.M. Prevention of ventilator-associated pneumonia. A Knowl. Surv. Among Intensive Care Nurses Yemen. Saudi. Med. J. 2014, 35, 269–276. [Google Scholar]
- Aloush, S.M. Nurses’ implementation of ventilator-associated pneumonia prevention guidelines: An observational study in Jordan. Nurs. Crit. Care 2017, 23, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Alkhazali, M.N.; Bayraktar, N.; Al-Mugheed, K.A. Knowledge and barriers of critical care nurses regarding evidence-based practices in ventilator-associated pneumonia prevention. Cyprus J. Med. Sci. 2021, 6, 185–191. [Google Scholar] [CrossRef]
- Aloush, S.M.; Al-Rawajfa, O.M. Prevention of ventilator-associated pneumonia in intensive care units: Barriers and compliance. Int. J. Nurs. Pract. 2020, 5, 12838. [Google Scholar] [CrossRef] [PubMed]
- Batiha, M.; Bashaireh, I.; AlBashtawy, M.; Shennaq, S. Exploring the competency of the Jordanian intensive care nurses towards endotracheal tube and oral care practices for mechanically ventilated patients: An observational study. Glob. J. Health Sci. 2013, 5, 203–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsadat, R.; Al-Bardan, H.; Mazloum, N.; Shamah, A.; Eltayeb, F.; Marie, A.; Kherallah, M. Use of ventilator associated pneumonia bundle and statistical process control chart to decrease VAP rate in Syria. Avicenna. J. Med. 2012, 2, 79–83. [Google Scholar] [CrossRef]
- Safdar, N.; Musuuza, J.S.; Xie, A.; Hundt, A.S.; Hall, M.; Wood, K.; Carayon, P. Management of ventilator-associated pneumonia in intensive care units: A mixed methods study assessing barriers and facilitators to guideline adherence. BMC Infect. Dis. 2016, 16, 349. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- WHO. EMRO Countries List; WHO: Geneva, Switzerland, 2019; Available online: http://www.emro.who.int/countries.html (accessed on 12 July 2019).
- Office of Health Assessment and Translation (OHAT). Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; National Institute of Environmental Health Sciences: Durham, NC, USA, 2019. Available online: https://ntp.niehs.nih.gov/ntp/ohat/pubs/handbookmarch2019_508.pdf (accessed on 12 July 2019).
- Darawad, M.W.; Sa’aleek, M.A.; Shawashi, T. Evidence-based guidelines for prevention of ventilator-associated pneumonia: Evaluation of intensive care unit nurses’ adherence. Am. J. Infect. Control. 2018, 46, 711–713. [Google Scholar] [CrossRef]
- Aloush, S.M. Does educating nurses with ventilator-associated pneumonia prevention guidelines improve their compliance? Am. J. Infect. Control. 2017, 45, 969–973. [Google Scholar] [CrossRef]
- Aloush, S.M.; Abdelkader, F.A.; Al-Sayaghi, K.; Tawalbeh, L.I.; Suliman, M.; Al Bashtawy, M.; Shaban, I. Compliance of nurses and hospitals with ventilator-associated pneumonia prevention guidelines a Middle Eastern survey. J. Nurs. Care Qual. 2017, 33, 8–14. [Google Scholar]
- Hassan, Z.M.; Wahsheh, M.A. Knowledge level of nurses in Jordan on ventilator-associated pneumonia and preventive measures. Nurs. Crit. Care 2017, 22, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Atashi, V.; Yousefi, H.; Mahjobipoor, H.; Yazdannik, A. The barriers to the prevention of ventilator-associated pneumonia from the perspective of critical care nurses: A qualitative descriptive study. J. Clin. Nurs. 2018, 5, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Hamishehkar, H.; Vahidinezhad, M.; Mashayekhi, S.O.; Asgharian, P.; Hassankhani, H.; Mahmoodpoor, A. Education alone is not enough in ventilator associated pneumonia care bundle compliance. J. Res. Pharm. Pract. 2014, 3, 51–55. [Google Scholar]
- Rashnou, F.; Toulabi, T.; Hasanvand, S.; Tarrahi, M.J. Barriers to the management of ventilator-associated pneumonia: A qualitative study of critical care nurses’ experiences. Middle East. J. Fam. Med. 2017, 15, 174–182. [Google Scholar] [CrossRef]
- Bagheri, M.; Amiri, M. Nurses’ knowledge of evidence-based guidelines for preventing ventilator associated pneumonia in intensive care units. J. Nurs. Midw. Sci. 2014, 1, 44–48. [Google Scholar] [CrossRef]
- Tabaeian, S.M.; Yazdannik, A.; Abbasi, S. Compliance with the Standards for Prevention of Ventilator Associated Pneumonia by Nurses in the Intensive Care Units. Iran. J. Nurs. Midwifery. Res. 2017, 22, 31–36. [Google Scholar]
- Yeganeh, M.; Yekta, H.; Farmanbar, R.; Khalili, M.; Roushan, Z.A. Knowledge of evidence-based guidelines in ventilator-associated pneumonia prevention. J. Evid. Based. Med. 2016, 12, 16–21. [Google Scholar] [CrossRef]
- Hawsawi, T.H.; Al-Naghshabandi, E.; Sofar, S.M. Effectiveness of Electronic Learning Module in Implementing Ventilator-Associated Pneumonia Prevention Measures of Intensive Care Unit Nurses. J. Adv. Health Med. Sci. 2018, 3, 126–149. [Google Scholar]
- Yaseen, R.W.; Salameh, T.N. Saudi critical care nurses’ knowledge of and barriers toward adherence to prevention of ventilator associated pneumonia guidelines. J. Nurs. Health. Sci. 2015, 4, 65–69. [Google Scholar]
- Al-Sayaghi, K.M. Critical care nurses’ compliance and barriers toward ventilator associated pneumonia prevention guidelines: Cross-sectional survey. J. Taibah. Univ. Med. Sci. 2020, 16, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, E.M.; Eldin, S. The impact of an educational training program on nurses in reduction of ventilator associated pneumonia. Egypt. J. Occup. Med. 2020, 43, 709–726. [Google Scholar]
- Nahla, S.A. Critical care nurses’ knowledge and compliance with ventilator associated pneumonia bundle at Cairo University hospitals. J. Educ. Pract. 2013, 4, 66–77. [Google Scholar]
- Hussein, M.H.; Kassi, N.M.; Al-Naamy, Y.; Abdul-Hussein, A.F.; Abadi, R.M.; Jassim, K.H. Nurses knowledge assessment concerning prevention of ventilator-associated pneumonia. Med. Legal. Update 2020, 20, 1420–1425. [Google Scholar]
- Zeb, A.; Hasnain, M.; Ahmad, I.; Khan, S.; Shah, A.A. Nurses’ knowledge regarding prevention of ventilator associated pneumonia. LOJ Nurs. Health. Care 2018, 2. [Google Scholar]
- Al-jaradi, A.S.; Al-Rabeei, N.A.; Al-Wesaby, S.A.; Alrubaiee, G.G. Knowledge of ICU Nurses toward prevention of ventilator associated pneumonia at public hospitals in Sana’a, City-Yemen. Al-Razi. Unvi. J. Med. Sci. 2020, 4, 17–27. [Google Scholar]
- Al-Shameri, F.A. Critical care nurse’s knowledge of ventilator-associated pneumonia prevention in selected hospitals, Khartoum. Nurs. Healthc. Int. J. 2017, 1, 2575–9981. [Google Scholar] [CrossRef]
- Jam, R.; Hernández, O.; Mesquida, J.; Turégano, C.; Carrillo, E.; Pedragosa, R.; Gómez, V.; Martí, L.; Vallés, J.; Delgado-Hito, P. Nursing workload and adherence to non-pharmacological measures in the prevention of ventilator-associated pneumonia. A Pilot Study Enferm. Intensiva. 2017, 28, 178–186. [Google Scholar] [CrossRef]
- Jansson, M.M.; Syrjälä, H.P.; Talman, K.; Meriläinen, M.H.; Ala-Kokko, T.I. Critical care nurses’ knowledge of, adherence to, and barriers toward institution-specific ventilator bundle. Am. J. Infect. Control. 2018, 46, 1051–1056. [Google Scholar] [CrossRef]
- Rosenthal, V.D.; Ramachandran, B.; Villamil-Gómez, W.; Armas-Ruiz, A.; Navoa-Ng, J.A.; Matta-Cortés, L. Impact of a multidimensional infection control strategy on central line-associated bloodstream infection rates in pediatric intensive care units of five developing countries: Findings of the International Nosocomial Infection Control Consortium (INICC). Infection 2012, 40, 415–423. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, Z. Cross-sectional studies strengths, weaknesses, and recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.M. Methodology Series Module 3: Cross-sectional Studies. Indian. J. Dermatol. 2016, 61, 261–264. [Google Scholar]
- Issa, M.R.; Muslim, N.A.; Alzoubi, R.H.; Jarrar, M.T.; Alkahtani, M.A.; Al-Bsheish, M.; Alomran, A.K. The Relationship between Emotional Intelligence and Pain Management Awareness among Nurses. Healthcare 2022, 10, 1047. [Google Scholar] [CrossRef] [PubMed]
- Al-Bsheish, M.; Jarrar, M.T.; Mustafa, M.B.; Zubaidi, F.; Azril, M.; Meri, A.; Dauwed, M. ICU nurses’ safety performance related to respect for safety and management commitment: A cross-sectional study. Contemporary. Nurse 2022, 1–23. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research: Appraising Evidence for Nursing Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Al-Mugheed, K.; Bayraktar, N. Effectiveness of a venous thromboembolism course using flipped classroom with nursing students: A randomized controlled trial. Nursing. Nurs. Forum 2021, 56, 623–629. [Google Scholar] [CrossRef]
- Al-Mugheed, K.; Bayraktar, N. Effectiveness of flipped classroom among nursing students on venous thromboembolism (VTE). Niger. J. Clin. Pract. 2021, 24, 1463–1470. [Google Scholar] [CrossRef]
- Bird, D.; Zambuto, A.; O’Donnell, C.; Silva, J.; Korn, C.; Burke, R.; Burke, P.; Agarwal, S. Adherence to ventilator-associated pneumonia bundle and incidence of ventilator-associated pneumonia in the surgical intensive care unit. JAMA Surg. 2010, 145, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.C.; Hay, A.W.; Swann, D.G.; Everingham, K.; McCulloch, C.; McNulty, J.; Brooks, O.; Laurenson, I.F.; Cook, B.; Walsh, T.S. Reducing ventilator-associated pneumonia in intensive care: Impact of implementing a care bundle. Crit. Care Med. 2011, 39, 2218–2224. [Google Scholar] [CrossRef]
- Stone, M.E., Jr.; Snetman, D.; O’Neill, A.; Cucuzzo, J.; Lindner, J.; Ahmad, S.; Teperman, S. Daily multidisciplinary rounds to implement the ventilator bundle decreases ventilator-associated pneumonia in trauma patients: But does it affect outcome? Surg. Infect. 2011, 12, 373–378. [Google Scholar] [CrossRef]
- Shaneyfelt, T.; Baum, K.D.; Bell, D.; Feldstein, D.; Houston, T.K.; Kaatz, S.; Whelan, C.; Green, M. Instruments for evaluating education in evidence-based practice: A systematic review. J. Amer. Med. Ass. 2006, 296, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. The inconvenient truth about convenience and purposive samples. Indian. J. Psycho. Med. 2021, 43, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Alsyouf, A.; Lutfi, A.; Al-Bsheish, M.; Jarrar, M.; Al-Mugheed, K.; Almaiah, M.A.; Alhazmi, F.N.; Masa’deh, R.; Anshasi, R.J.; Ashour, A. Exposure Detection Applications Acceptance: The Case of COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 7307. [Google Scholar] [CrossRef] [PubMed]
- Al-Mugheed, K.; Al Rawajfah, O.; Bani-Issa, W.; Rababa, M. Acceptance, Attitudes, and Barriers of Vaccine Booster Dose among Nursing Students: A Multicounty Survey. J. Nurs. Manag. 2022. [Google Scholar] [CrossRef]
- Jordan, A.; Badovinac, A.; Špalj, S.; Par, M.; Šlaj, M.; Plančak, D. Factors influencing intensive care nurses’ knowledge and attitudes regarding ventilator-associated pneumonia and oral care practice in intubated patients in Croatia. Am. J. Infect. Control 2014, 42, 1115–1117. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Database | Terms | Search Result |
|---|---|---|---|
| 1 | Pubmed (MeSH) | (“Intensive Care Units” [Mesh] OR “Critical Care Nursing” [tiab]) AND (“knowledge” [Mesh] [tiab] OR “Practice” [tiab]) AND (“Ventilator-Associated Pneumonia” [tiab] OR “VAP” [tiab]). | 1135 |
| 2 | EMBASE (emtree) | (“Nursing” [Mesh] OR “Critical Care”[tiab] OR “Intensive Care” [tiab])AND (“adherence” [Mesh] “[tiab] OR” Compliance [tiab]) AND (“Ventilator-Associated Pneumonia” [tiab] OR “VAP” [tiab]). | 299 |
| 3 | Web of Science | “Critical Care Nursing” [Mesh] OR “Critical Care Nurses” [tiab] OR “intensive care” [tiab]) AND (“practice” [tiab] OR “skills” [tiab] AND (“Ventilator-Associated Pneumonia” [tiab] OR “Healthcare-Associated Pneumonia” [tiab]) OR “Ventilator-Associated”[tiab]). | 338 |
| 4 | SCOPUS | “Critical Care Nursing” “[Mesh] OR “Critical Care Nurses” [tiab] OR “intensive care” [tiab]) AND (“barriers” [tiab] OR “obstacles” [tiab] OR “challenges” [tiab] OR “difficulties” [tiab] “issues” [tiab]) AND (“Ventilator-Associated Pneumonia” [tiab] OR “Healthcare-Associated Pneumonia” [tiab]) OR “Ventilator-Associated” [tiab]). | 748 |
| Study Authors (Year) | Outcome Measures | Country | Study Characteristics | Study Design | Instrumentation | Main Outcomes |
|---|---|---|---|---|---|---|
| Darawad et al. [32], 2018 | Knowledge and Practices | Jordan |
| Experimental |
| Poor knowledge and high practices |
| Hamishehkar, et al. [37], 2014. | Compliance | Iran |
| Observational |
| Insufficient Compliance |
| Aloush, et al. [34], 2017. | Compliance and Barriers | Jordan, Egypt, and Saudi Arabia |
| Observational |
| Insufficient Compliance. Lack of education. Lack of a professional model. Poor integration of research findings in practice |
| Al-Sayaghi et al. [44], 2014 | Knowledge | Yemen |
| Observational |
| Low Knowledge |
| Atashi et al. [26], 2018 | Barriers | Iran |
| Qualitative |
| Lack of education. Lack of a professional model. Unfavourable environmental conditions. Shortage of nursing staff. Lack of time and resources Passive human resource and organizational management |
| Rashnou et al. [38], 2017 | Barriers | Iran |
| Qualitative |
| Unfavourable environmental conditions. Passive human resource and organizational management |
| Yaseen and Salameh, [43], 2015 | Knowledge, Barriers | Saudi Arabia |
| Observational |
| Low Knowledge. Lack of education. Shortage of nursing staff. Lack of policies and protocols. |
| Aloush, [23], 2017 | Compliance. | Jordan |
| Observational |
| Insufficient Compliance |
| Tabaeian et al. [40], 2017 | Compliance | Iran |
| Observational |
| Acceptable Compliance |
| Aloush SM, [33], 2017 | Compliance | Jordan |
| Quasi-experimental |
| Moderate Compliance. There was no statistically significant difference between experimental group and the control group |
| Al-Shameri FA, [50], 2017 | Knowledge | Sudan |
| Observational |
| Inadequate Knowledge. |
| Al-Sayaghi KM, [44], 2020 | Compliance and Barriers | Saudi Arabia |
| Observational |
| Acceptable Complianc. Shortage of nursing staff. Forgetfulness Lack of policies and protocols. |
| Hussein et al. [47], 2020 | Knowledge | Iraq |
| Observational |
| Poor knowledge |
| Al-khazali et al. [24], 2021 | Knowledge and Barriers | Jordan |
| Observational |
| Adequate Knowledge. Lack of education. Shortage of nursing staff. Forgetfulness |
| Khalifa et al. [45], 2020 | Knowledge and Practices | Egypt |
| A quasi- experimental |
| Significant improvement after education in terms of knowledge and practices |
| Al-jaradi et al. [49], 2020 | Knowledge | Yemen |
| Observational |
| Inadequate knowledge |
| Yeganeh et al. [41], 2016 | Knowledge and Barriers | Iran |
| Observational |
| Inadequate knowledge. Lack of education. |
| Nahla SA., [46], 2013 | Knowledge and Compliance | Egypt |
| Observational |
| Unsatisfactory knowledge and insufficient compliance |
| Hawsawi et al. [42], 2018 | knowledge and practices | Saudi Arabia |
| Quasi experimental |
| Significant improvement after education interms of knowledge and practices |
| Hassan and Wahsheh, [26], 2017 | Knowledge and Barriers | Jordan |
| Quasi experimental |
| Significant improvement after education interms of knowledge. Lack of policies and protocols. Lack of time |
| Aloush and Al-Rawajfa, [19], 2020 | Compliance and Barriers | Jordan |
| Observational |
| Poor Compliance. Lack of education. Shortage of nursing staff. Lack of policies and protocols. |
| Bagheri et al. [30], 2013 | Knowledge | Iran |
| Observational |
| Low Knowledge |
| Zeb et al. [39], 2018 | Knowledge | Pakistan |
| Observational |
| Low Knowledge |
| Selection | Confounding | Performance | Attrition/Exclusion | Detection | Selective Reporting | |
|---|---|---|---|---|---|---|
| Darawad et al., 2018 | DL | DL | DL | DL | PL | PL |
| Hamishehkar, et al., 2014 | PL | DL | DL | DL | DL | PL |
| Aloush, et al., 2017. | PL | PL | DL | DL | DL | DL |
| Atashi et al., 2018 | DL | DH | PL | PL | PL | PL |
| Rashnou et al., 2017 | DL | DL | PH | DL | DL | PL |
| Al-Sayaghi et al., 2014 | PL | DL | DL | PL | PL | DL |
| Aloush, 2017 | DL | DL | DL | DL | DL | DL |
| Yaseen and Salameh, 2015 | DL | DH | PH | PH | PL | PL |
| Al-Oush SM, 2017 | DL | DL | DL | DL | DL | DL |
| Al-Shameri FA, 2017 | PH | PH | DH | DL | PL | PL |
| Al-Sayaghi KM, 2020 | PL | PL | DL | DL | DL | DL |
| Tabaeian et al., 2017 | DL | DL | DL | PL | PL | PL |
| Al-Khazali et al., 2021 | DL | PL | DL | DL | PL | DL |
| Khalifa et al., 2020 | PL | DL | PL | DL | DL | PL |
| Al-Jaradi et al., 2020 | PL | DL | DL | DL | DL | DL |
| Nahla SA., 2013 | DL | DL | PL | PL | DL | DL |
| Hussein et al., 2020 | PL | DL | PL | DL | DL | PL |
| Yeganeh et al., 2016 | DL | DL | PL | DL | DL | DL |
| Hawsawi et al., 2018 | PL | DH | DL | DH | DL | DL |
| Hassan and Wahsheh, 2017 | PL | DL | PL | PL | DL | DL |
| Aloush and Al-Rawajfa, 2020 | DL | PL | PL | DL | DL | DL |
| Bagheri et al., 2013 | PL | DL | DL | PL | PL | DL |
| Zeb et al., 2018 | DL | DH | DL | DL | PL | DL |
| Aloush, et al., 2017 | Atashi et al., 2018 | Rashnou et al., 2017 | Yaseen and Salameh, 2015 | Al-Sayaghi KM, 2020 | Alkhazali et al., 2021 | Yeganeh et al., 2016 | Hassan and Wahsheh, 2017 | Aloush and Al-Rawajfa, 2020 | |
|---|---|---|---|---|---|---|---|---|---|
| √ | √ | √ | √ | √ | √ | |||
| √ | √ | |||||||
| √ | ||||||||
| √ | √ | |||||||
| √ | √ | √ | √ | √ | ||||
| √ | √ | |||||||
| √ | √ | √ | √ | |||||
| √ | √ | |||||||
| √ | √ | √ | √ | |||||
| √ | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AL-Mugheed, K.; Bani-Issa, W.; Rababa, M.; Hayajneh, A.A.; Syouf, A.A.; Al-Bsheish, M.; Jarrar, M. Knowledge, Practice, Compliance, and Barriers toward Ventilator-Associated Pneumonia among Critical Care Nurses in Eastern Mediterranean Region: A Systematic Review. Healthcare 2022, 10, 1852. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10101852
AL-Mugheed K, Bani-Issa W, Rababa M, Hayajneh AA, Syouf AA, Al-Bsheish M, Jarrar M. Knowledge, Practice, Compliance, and Barriers toward Ventilator-Associated Pneumonia among Critical Care Nurses in Eastern Mediterranean Region: A Systematic Review. Healthcare. 2022; 10(10):1852. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10101852
Chicago/Turabian StyleAL-Mugheed, Khaild, Wegdan Bani-Issa, Mohammad Rababa, Audai A. Hayajneh, Adi Al Syouf, Mohammad Al-Bsheish, and Mu’taman Jarrar. 2022. "Knowledge, Practice, Compliance, and Barriers toward Ventilator-Associated Pneumonia among Critical Care Nurses in Eastern Mediterranean Region: A Systematic Review" Healthcare 10, no. 10: 1852. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10101852