
Factors Related to Quality of Life of Hemodialysis Patients during the COVID-19 Pandemic
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
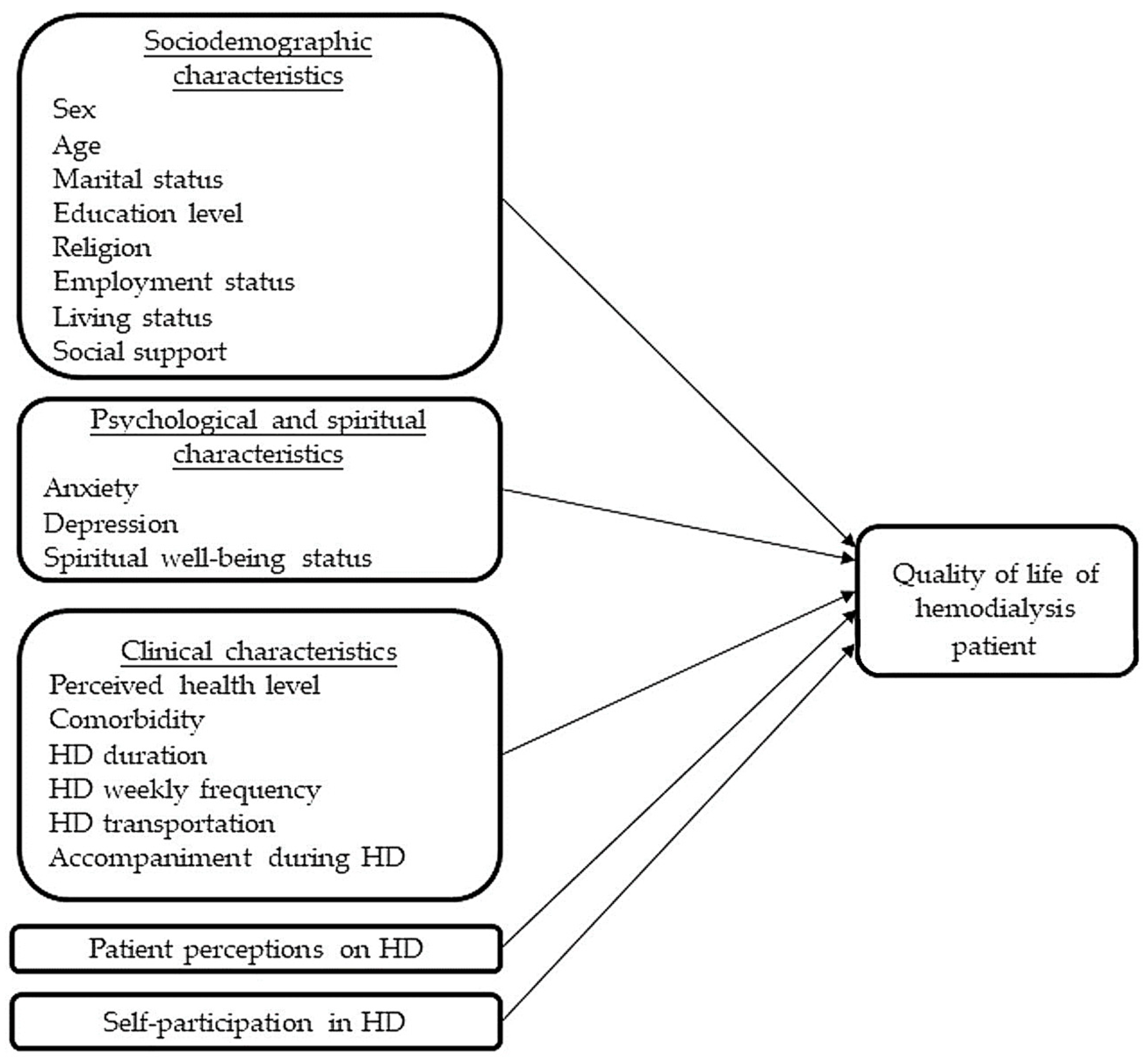
2.2. Study Framework
2.3. Participants and Setting
2.4. Instruments
2.4.1. Sociodemographic Characteristics
2.4.2. Psychological and Spiritual Characteristics
2.4.3. Clinical Characteristics
2.4.4. Perceptions of and Self-Participation in HD
2.4.5. KDQOL
2.5. Study Procedure
2.6. Ethical Considerations
2.7. Data Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Psychological and Spiritual Characteristics
3.3. Clinical Characteristics
3.4. Patient Perceptions of and Self-Participation in HD
3.5. KDQOL
3.6. Factors Related to Quality of Life of HD Patients
4. Discussion
4.1. Psychological and Spiritual Characteristics
4.2. KDQOL
4.3. Factors Related to HD Patients’ Quality of Life
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | b | 95% CI | p-Value | b | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Constant | NA | NA | NA | 35.02 | 17.78–52.27 | <0.001 |
| Sociodemographic characteristics | ||||||
| Sex | ||||||
| Female vs. male | 2.21 | −1.53–5.95 | 0.245 | |||
| Age | −0.11 | −0.27–0.06 | 0.216 | |||
| Marital status | ||||||
| Married vs. single | 1.19 | −5.28–7.65 | 0.718 | |||
| Divorce/cohabit vs. single | 4.99 | −4.93–14.91 | 0.323 | |||
| Widowed vs. single | −1.84 | −10.31–6.64 | 0.670 | |||
| Educational level | ||||||
| Junior high school vs. ≤elementary school | 1.57 | −3.56–6.70 | 0.548 | 0.42 | −3.48–4.33 | 0.832 |
| Senior high school/vocational school vs. ≤elementary school | 4.83 | 0.12–9.53 | 0.045 | 2.01 | −1.73–5.75 | 0.291 |
| College vs. ≤elementary school | 7.93 | 1.31–14.55 | 0.019 | 2.76 | −2.58–8.11 | 0.310 |
| University/≥master’s program vs. ≤elementary school | 1.78 | −6.87–10.42 | 0.687 | −2.02 | −8.58–4.54 | 0.545 |
| Religion | ||||||
| Buddhist vs. none identified | −0.76 | −6.47–4.95 | 0.794 | |||
| Taoist vs. none identified | −2.43 | −12.53–7.67 | 0.636 | |||
| Christian/Catholic vs. none identified | −8.61 | −25.42–8.20 | 0.314 | |||
| I-Kuan Tao vs. none identified | −5.80 | −20.66–9.06 | 0.444 | |||
| Employment status | ||||||
| Part-time vs. none | 1.67 | −5.83–9.17 | 0.662 | |||
| Full-time vs. none | 4.02 | −1.32–9.36 | 0.140 | |||
| Living status | 2.07 | −12.48–16.62 | 0.780 | |||
| Spouse vs. live alone | 3.05 | −11.45–17.55 | 0.680 | |||
| Children vs. live alone | 0.04 | −14.84–14.93 | 0.996 | |||
| Relatives vs. live alone | 4.61 | −11.13–20.35 | 0.565 | |||
| Friends/nurse aids vs. live alone | −14.02 | −34.27–6.23 | 0.174 | |||
| Other vs. live alone | −5.70 | −25.08–13.69 | 0.564 | |||
| Psychological and spiritual characteristics | ||||||
| Social support scale score | 0.26 | 0.07–0.44 | 0.008 | 0.05 | −0.12–0.21 | 0.584 |
| Beck Anxiety Inventory score | ||||||
| 8–15 (mild) vs. 0–7 (extremely mild) | −14.59 | −18.35–−10.84 | <0.001 | −8.40 | −12.32–−4.49 | <0.001 |
| 16–25 (moderate) vs. 0–7 (extremely mild) | −19.35 | −23.47–−15.22 | <0.001 | −10.54 | −15.03–−6.05 | <0.001 |
| 26–63 (severe) vs. 0–7 (extremely mild) | −26.81 | −32.35–−21.26 | <0.001 | −15.50 | −21.74–−9.26 | <0.001 |
| Beck Depression Inventory score | ||||||
| 4–6 (mild) vs. 0–3 (extremely mild) | −10.97 | −15.57–−6.36 | <0.001 | −2.91 | −6.91–1.09 | 0.154 |
| 7–9 (moderate) vs. 0–3 (extremely mild) | −14.98 | −22.24–−7.71 | <0.001 | −3.92 | −10.24–2.40 | 0.223 |
| 10–21 (severe) vs. 0–3 (extremely mild) | −17.16 | −22.65–−11.68 | <0.001 | −2.69 | −7.88–2.49 | 0.308 |
| Spiritual well-being status | 4.75 | 1.05–8.46 | 0.012 | |||
| Clinical characteristics | ||||||
| Perceived health status | 9.17 | 7.05–11.30 | <0.001 | 5.12 | 3.19–7.05 | <0.001 |
| Total comorbidities | ||||||
| 0 vs. 4 types | 10.28 | 0.25–20.32 | 0.045 | 6.28 | −1.41–13.97 | 0.109 |
| 1 vs. 4 types | 17.84 | 8.56–27.13 | <0.001 | 7.03 | −0.22–14.28 | 0.057 |
| 2 vs. 4 types | 18.56 | 9.42–27.69 | <0.001 | 7.52 | 0.28–14.76 | 0.042 |
| 3 vs. 4 types | 14.00 | 4.15–23.86 | 0.006 | 5.59 | −2.19–13.36 | 0.158 |
| Hemodialysis duration | 0.21 | −0.05–0.46 | 0.110 | |||
| Frequency of hemodialysis per week | ||||||
| 3 times per week vs. 2 times per week | −8.96 | −20.48–2.55 | 0.127 | −4.55 | −13.23–4.13 | 0.303 |
| Transportation for hemodialysis | ||||||
| Vehicle vs. self-preparation | −4.74 | −9.70–0.22 | 0.061 | −1.83 | −5.61–1.94 | 0.340 |
| Motorcycle vs. self-preparation | −9.20 | −16.90–−1.50 | 0.019 | −5.44 | −11.48–0.60 | 0.077 |
| Bus/transit/Formosa Fairway Corporation vs. self-preparation | −0.55 | −6.56–5.46 | 0.856 | −0.29 | −4.96–4.38 | 0.903 |
| Other vs. self-preparation | −12.72 | −20.94–−4.49 | 0.003 | −4.37 | −10.71–1.97 | 0.176 |
| Accompanied during hemodialysis | ||||||
| No vs. Yes | −4.38 | −8.19–−0.57 | 0.024 | −0.52 | −3.81–2.77 | 0.754 |
| Feelings about hemodialysis at present | 0.58 | 0.32–0.83 | <0.001 | 0.09 | −0.12–0.30 | 0.412 |
| Self-participation in hemodialysis | 0.34 | 0.27–0.41 | <0.001 | 0.15 | 0.08–0.22 | <0.001 |
References
- United States Renal Data System [USRDS]. 2022 USRDS Annual Data Report; National Institutes of Health: Bethesda, MD, USA, 2022. Available online: https://adr.usrds.org/2020/end-stage-renal-disease/1-incidence-prevalence-patient-characteristics-and-treatment-modalities (accessed on 22 November 2022).
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2020, 75, A6–A7. [Google Scholar] [CrossRef]
- Flythe, J.E.; Powell, J.D.; Poulton, C.J.; Westreich, K.D.; Handler, L.; Reeve, B.B.; Carey, T.S. Patient-Reported Outcome Instruments for Physical Symptoms among Patients Receiving Maintenance Dialysis: A Systematic Review. Am. J. Kidney Dis. 2015, 66, 1033–1046. [Google Scholar] [CrossRef]
- Cao, X.; Tian, L.; Lin, C. Symptom Clusters in Patients Receiving Hemodialysis: A Systematic Review of Observational Studies. J. Clin. Nurs. 2017, 26, 2545–2557. [Google Scholar] [CrossRef]
- Horigan, A.E.; Schneider, S.M.; Docherty, S.; Barroso, J. The Experience and Self-Management of Fatigue in Patients on Hemodialysis. Nephrol. Nurs. J. 2013, 40, 113–123. [Google Scholar]
- Morfin, J.A.; Fluck, R.J.; Weinhandl, E.D.; Kansal, S.; McCullough, P.A.; Komenda, P. Intensive Hemodialysis and Treatment Complications and Tolerability. Am. J. Kidney Dis. 2016, 68, S43–S50. [Google Scholar] [CrossRef]
- Wagner, J.; Jhaveri, K.D.; Rosen, L.; Sunday, S.; Mathew, A.T.; Fishbane, S. Increased Bone Fractures among Elderly United States Hemodialysis Patients. Nephrol. Dial. Transplant. 2014, 29, 146–151. [Google Scholar] [CrossRef]
- Roshanravan, B.; Khatri, M.; Robinson-Cohen, C.; Levin, G.; Patel, K.V.; de Boer, I.H.; Seliger, S.; Ruzinski, J.; Himmelfarb, J.; Kestenbaum, B. A Prospective Study of Frailty in Nephrology-Referred Patients with CKD. Am. J. Kidney Dis. 2012, 60, 912–921. [Google Scholar] [CrossRef]
- Xing, L.; Chen, R.; Diao, Y.; Qian, J.; You, C.; Jiang, X. Do Psychological Interventions Reduce Depression in Hemodialysis Patients?: A Meta-Analysis of Randomized Controlled Trials Following PRISMA. Medicine 2016, 95, e4675. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M. Patient Empowerment: Myths and Misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef]
- Tsay, S.L.; Healstead, M. Self-Care Self-Efficacy, Depression, and Quality of Life among Patients Receiving Hemodialysis in Taiwan. Int. J. Nurs. Stud. 2002, 39, 245–251. [Google Scholar] [CrossRef]
- Tobiano, G.; Bucknall, T.; Marshall, A.; Guinane, J.; Chaboyer, W. Nurses’ Views of Patient Participation in Nursing Care. J. Adv. Nurs. 2015, 71, 2741–2752. [Google Scholar] [CrossRef]
- Castro, E.M.; Van Regenmortel, T.; Vanhaecht, K.; Sermeus, W.; Van Hecke, A. Patient Empowerment, Patient Participation and Patient-Centeredness in Hospital Care: A Concept Analysis Based on a Literature Review. Patient Educ. Couns. 2016, 99, 1923–1939. [Google Scholar] [CrossRef]
- Chen, J.J.; Lee, T.H.; Tian, Y.C.; Lee, C.C.; Fan, P.C.; Chang, C.H. Immunogenicity Rates After SARS-CoV-2 Vaccination in People with End-stage Kidney Disease: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2131749. [Google Scholar] [CrossRef]
- Chen, C.Y.; Shao, S.C.; Chen, Y.T.; Hsu, C.K.; Hsu, H.J.; Lee, C.C.; Sun, C.Y.; Chen, Y.C.; Hung, M.J.; Wu, I.W. Incidence and Clinical Impacts of COVID-19 Infection in Patients with Hemodialysis: Systematic Review and Meta-Analysis of 396,062 Hemodialysis Patients. Healthcare 2021, 9, 47. [Google Scholar] [CrossRef]
- Taji, L.; Thomas, D.; Oliver, M.J.; Ip, J.; Tang, Y.; Yeung, A.; Cooper, R.; House, A.A.; McFarlane, P.; Blake, P.G. COVID-19 in Patients Undergoing Long-term Dialysis in Ontario. CMAJ 2021, 193, E278–E284. [Google Scholar] [CrossRef]
- United States Renal Data System [USRDS]. COVID-19 Supplements: COVID-19; Racial and Ethnic Disparities: Chapter 13: COVID-19. 2022. Available online: https://usrds-adr.niddk.nih.gov/2022/supplements-covid-19-disparities/13-covid-19-supplement (accessed on 22 November 2022).
- Karoui, K.E.; De Vriese, A.S. COVID-19 in Dialysis: Clinical Impact, Immune Response, Prevention, and Treatment. Kidney Int. 2022, 101, 883–894. [Google Scholar] [CrossRef]
- Patel, M.P.; Kute, V.B.; Prasad, N.; Agarwal, S.K. COVID-19 Working Group of Indian Society of Nephrology. COVID 19 and Hemodialysis Anxiety. Indian J. Nephrol. 2020, 30, 174–175. [Google Scholar] [CrossRef]
- Al Wakeel, J.; Al Harbi, A.; Bayoumi, M.; Al-Suwaida, K.; Al Ghonaim, M.; Mishkiry, A. Quality of Life in Hemodialysis and Peritoneal Dialysis Patients in Saudi Arabia. Ann. Saudi Med. 2012, 32, 570–574. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, B.; Park, K.S.; Choi, J.Y.; Seo, J.J.; Park, S.H.; Kim, C.D.; Kim, Y.L. Health-related Quality of Life with KDQOL-36 and Its Association with Self-efficacy and Treatment Satisfaction in Korean Dialysis Patients. Qual. Life Res. 2013, 22, 753–758. [Google Scholar] [CrossRef]
- Moura, A.; Madureira, J.; Alija, P.; Fernandes, J.C.; Oliveira, J.G.; Lopez, M.; Filgueiras, M.; Amado, L.; Sameiro-Faria, M.; Miranda, V.; et al. Predictors of Health-related Quality of Life Perceived by End-stage Renal Disease Patients under Online Hemodiafiltration. Qual. Life Res. 2015, 24, 1327–1335. [Google Scholar] [CrossRef]
- Santos, P.R.; Capote Júnior, J.; Cavalcante Filho, J.; Ferreira, T.P.; Dos Santos Filho, J.; da Silva Oliveira, S. Religious Coping Methods Predict Depression and Quality of Life among End-Stage Renal Disease Patients Undergoing Hemodialysis: A Cross-Sectional Study. BMC Nephrol. 2017, 18, 197. [Google Scholar] [CrossRef]
- Zhou, X.; Xue, F.; Wang, H.; Qiao, Y.; Liu, G.; Huang, L.; Li, D.; Wang, S.; Wang, Q.; Li, L.; et al. The Quality of Life and Associated Factors in Patients on Maintenance Hemodialysis—A Multicenter Study in Shanxi Province. Ren. Fail. 2017, 39, 707–711. [Google Scholar] [CrossRef]
- Alhaji, M.M.; Tan, J.; Hamid, M.R.; Timbuak, J.A.; Naing, L.; Tuah, N.A. Determinants of Quality of Life as Measured with Variants of SF-36 in Patients with Predialysis Chronic Kidney Disease. Saudi Med. J. 2018, 39, 653–661. [Google Scholar] [CrossRef]
- Pretto, C.R.; Winkelmann, E.R.; Hildebrandt, L.M.; Barbosa, D.A.; Colet, C.F.; Stumm, E.M.F. Quality of Life of Chronic Kidney Patients on Hemodialysis and Related Factors. Rev. Lat. Am. Enfermangem. 2020, 28, e3327. [Google Scholar] [CrossRef]
- Yang, F.; Griva, K.; Lau, T.; Vathsala, A.; Lee, E.; Ng, H.J.; Mooppil, N.; Foo, M.; Newman, S.P.; Chia, K.S.; et al. Health-related Quality of Life of Asian Patients with End-stage Renal Disease (ESRD) in Singapore. Qual. Life Res. 2015, 24, 2163–2171. [Google Scholar] [CrossRef]
- Mousa, I.; Ataba, R.; Al-ali, K.; Alkaiyat, A.; Zyoud, S.H. Dialysis-related Factors Affecting Self-efficacy and Quality of Life in Patients on Haemodialysis: A Cross-Sectional Study from Palestine. Ren. Replace Ther. 2018, 4, 21. [Google Scholar] [CrossRef]
- Pan, C.W.; Wu, Y.; Zhou, H.J.; Xu, B.X.; Wang, P. Health-related Quality of Life and Its Factors of Hemodialysis Patients in Suzhou, China. Blood Purif. 2018, 45, 327–333. [Google Scholar] [CrossRef]
- García-Martínez, P.; Temprado-Albalat, M.D.; Ballester-Arnal, R.; Gandhi-Morar, K.; Castro-Calvo, J.; Collado-Boira, E. Predictive Model of Variables Associated with Health-Related Quality of Life in Patients with Advanced Chronic Kidney Disease Receiving Hemodialysis. Qual. Life Res. 2020, 29, 1817–1827. [Google Scholar] [CrossRef]
- Doan, K.; Nguyen, H.; Nguyen, N.; Dang, K.C.; Yang, S.H.; Duong, T.V. Associations of Socio-Demographic, Clinical and Biochemical Parameters with Healthcare Cost, Health- and Renal-related Quality of Life in Hemodialysis Patients: A Clinical Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 6552. [Google Scholar] [CrossRef]
- Mahato, S.; Apidechkul, T.; Sriwongpan, P.; Hada, R.; Sharma, G.N.; Nayak, S.K.; Mahato, R.K. Factors Associated with Quality of Life among Chronic Kidney Disease Patients in Nepal: A Cross-Sectional Study. Health Qual. Life Outcomes 2020, 18, 207. [Google Scholar] [CrossRef]
- Gedney, N. Long-term Hemodialysis during the COVID-19 Pandemic. CJASN 2020, 15, 1073–1074. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.H.; Pan, X.T.; Chen, Y.; Wang, L.; Chen, Q.X.; Zhu, Y.; Zhu, Y.J.; Chen, Y.X.; Chen, X.N. Psychological Profiles of Chinese Patients with Hemodialysis during the Panic of Coronavirus Disease 2019. Front. Psychiatry 2021, 12, 616016. [Google Scholar] [CrossRef] [PubMed]
- Al Salmi, I.; Kamble, P.; Lazarus, E.R.; D’Souza, M.S.; Al Maimani, Y.; Hannawi, S. Kidney Disease-Specific Quality of Life among Patients on Hemodialysis. Int. J. Nephrol. 2021, 2021, 8876559. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.N.; Shapiro, B.; Kim, J.C.; Zhang, M.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Martin, D.; Kalantar-Zadeh, K.; et al. Association between Quality of Life and Anxiety, Depression, Physical Activity and Physical Performance in Maintenance Hemodialysis Patients. Chronic Dis. Transl. Med. 2016, 2, 110–119. [Google Scholar] [CrossRef]
- De Brito, D.; Machado, E.L.; Reis, I.A.; Carmo, L.; Cherchiglia, M.L. Depression and Anxiety among Patients Undergoing Dialysis and Kidney Transplantation: A Cross-sectional Study. Sao Paulo Med. J. 2019, 137, 137–147. [Google Scholar] [CrossRef]
- Kim, K.; Kang, G.W.; Woo, J. The Quality of Life of Hemodialysis Patients is Affected Not Only by Medical but also Psychosocial Factors: A Canonical Correlation Study. J. Korean Med. Sci. 2018, 33, e111. [Google Scholar] [CrossRef]
- Davison, S.N.; Jhangri, G.S. The Relationship between Spirituality, Psychosocial Adjustment to Illness, and Health-Related Quality of Life in Patients with Advanced Chronic Kidney Disease. J. Pain Symptom Manag. 2013, 45, 170–178. [Google Scholar] [CrossRef]
- De Olivera, L.M.; Okuno, M.F.P.; Barbosa, D.A.; Sesso, R.; Scherrer Júnior, G.; Pessoa, J.; Fonseca, C.; Belasco, A. Quality of Life and Spirituality of Patients with Chronic Kidney Disease: Pre- and Post-transplant Analysis. Rev. Bras. Enferm. 2020, 73 (Suppl. S5), e20190408. [Google Scholar] [CrossRef]
- Al-Ghabeesh, S.H.; Alshraifeen, A.A.; Saifan, A.R.; Bashayreh, I.H.; Alnuaimi, K.M.; Masalha, H.A. Spirituality in the Lives of Patients with End-Stage Renal Disease: A Systematic Review. J. Relig. Health 2018, 57, 2461–2477. [Google Scholar] [CrossRef]
- Musa, A.S.; Elbqowm, O.; AlBashtawy, M.; Al Qadire, M.I.; Suliman, M.; Tawalbeh, L.I.; Alkhawaldeh, A.; Batiha, A.M.M. Spiritual Wellbeing and Quality of Life among Hemodialysis Patients in Jordan: A Cross-Sectional Correlational Study. J. Holist. Nurs. 2022. [Google Scholar] [CrossRef]
- Vo, T.Q.; Tran, T.Q.; Duong, K.N.C.; Pham, K.C. Impact of Chronic Kidney Disease on Health-Related Quality of Life: A Prospective Observational Study Using the KDQoL-36 Instrument. J. Clin. Diagn. Res. 2018, 12 (Suppl. S1), LC66–LC71. [Google Scholar] [CrossRef]
- Plantinga, L.C.; Fink, N.E.; Harrington-Levey, R.; Finkelstein, F.O.; Hebah, N.; Powe, N.R.; Jaar, B.G. Association of Social Support with Outcomes in Incident Dialysis Patients. CJASN 2010, 5, 1480–1488. [Google Scholar] [CrossRef]
- Lin, C.C.; Ko, N.Y.; Tsai, L.C.; Chen, C.H. Assessing the Effect of Health Belief, Knowledge, and Social Support on Compliance Behaviors in Chronic Hemodialysis Patients. Kaohsiung J. Med. Sci. 1995, 11, 470–480. [Google Scholar] [CrossRef]
- Cukor, D.; Donahue, S.; Tummalapalli, S.L.; Bohmart, A.; Silberzweig, J. Anxiety, Comorbid Depression, and Dialysis Symptom Burden. CJASN 2022, 17, 1216–1217. [Google Scholar] [CrossRef]
- Nadort, E.; Rijkers, N.; Schouten, R.W.; Hoogeveen, E.K.; Bos, W.; Vleming, L.J.; Westerman, M.; Schouten, M.; Dekker, M.; Smets, Y.; et al. Depression, Anxiety and Quality of Life of Hemodialysis Patients before and during the COVID-19 Pandemic. J. Psychosom. Res. 2022, 158, 110917. [Google Scholar] [CrossRef]
- Cohen, D.E.; Lee, A.; Sibbel, S.; Benner, D.; Brunelli, S.M.; Tentori, F. Use of the KDQOL-36™ for Assessment of Health-Related Quality of Life among Dialysis Patients in the United States. BMC Nephrol. 2019, 20, 112. [Google Scholar] [CrossRef]
- Yazawa, M.; Omae, K.; Shibagaki, Y.; Inaba, M.; Tsuruya, K.; Kurita, N. The Effect of Transportation Modality to Dialysis Facilities on Health-related Quality of Life among Hemodialysis Patients: Results from the Japanese Dialysis Outcomes and Practice Pattern Study. Clin. Kidney J. 2019, 13, 640–646. [Google Scholar] [CrossRef]
- Heidarzadeh, M.; Atashpeikar, S.; Jalilazar, T. Relationship between Quality of Life and Self-Care Ability in Patients Receiving Hemodialysis. Iran J. Nurs. Midwifery Res. 2010, 15, 71–76. [Google Scholar]
- Wilkinson, T.J.; Memory, K.; Lightfoot, C.J.; Palmer, J.; Smith, A.C. Determinants of Patient Activation and Its Association with Cardiovascular Disease Risk in Chronic Kidney Disease: A Cross-Sectional Study. Health Expect. 2021, 24, 843–852. [Google Scholar] [CrossRef]
- Zimbudzi, E.; Lo, C.; Ranasinha, S.; Fulcher, G.R.; Jan, S.; Kerr, P.G.; Polkinghorne, K.R.; Russell, G.; Walker, R.G.; Zoungas, S. Factors Associated with Patient Activation in an Australian population with Comorbid Diabetes and Chronic Kidney Disease: A Cross-Sectional Study. BMJ Open 2017, 7, e017695. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An Inventory for Measuring Clinical Anxiety: Psychometric Properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Beck, A.T.; Guth, D.; Steer, R.A.; Ball, R. Screening for Major Depression Disorders in Medical Inpatients with the Beck Depression Inventory for Primary Care. Behav. Res. Ther. 1997, 35, 785–791. [Google Scholar] [CrossRef]
- Hungelmann, J.; Kenkel-Rossi, E.; Klassen, L.; Stollenwerk, R. Focus on Spiritual Well-Being: Harmonious Interconnectedness of Mind-Body-Spirit Use of the JAREL Spiritual Well-Being Scale. Geriatr. Nurs. 1996, 17, 262–266. [Google Scholar] [CrossRef]
- Hsieh, S.I.; Hsu, L.L.; Kao, C.Y.; Breckenridge-Sproat, S.; Lin, H.L.; Tai, H.C.; Huang, T.H.; Chu, T.L. Factors Associated with Spiritual Care Competency in Taiwan’s Clinical Nurses: A Descriptive Correlational Study. J. Clin. Nurs. 2019, 29, 1599–1613. [Google Scholar] [CrossRef]
- Szu, L.Y.; Tsao, L.I.; Chen, S.C.; Ho, M.L. Self-Participation Experiences among Well-Adapted Hemodialysis Patients. Healthcare 2021, 9, 1742. [Google Scholar] [CrossRef]
- Ricardo, A.C.; Hacker, E.; Lora, C.M.; Ackerson, L.; DeSalvo, K.B.; Go, A.; Kusek, J.W.; Nessel, L.; Ojo, A.; Townsend, R.R.; et al. Validation of the Kidney Disease Quality of Life Short Form 36 (KDQOL-36) US Spanish and English Versions in a Cohort of Hispanics with Chronic Kidney Disease. Ethn. Dis. 2013, 23, 202–209. [Google Scholar]
- Tao, X.; Chow, S.K.; Wong, F.K. Determining the Validity and Reliability of the Chinese Version of the Kidney Disease Quality of Life Questionnaire (KDQOL-36™). BMC Nephrol. 2014, 15, 115. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Schouten, R.W.; Haverkamp, G.L.; Loosman, W.L.; Shaw, C.P.K.; van Ittersum, F.J.; Smets, Y.C.C.; Vleming, L.J.; Dekker, F.W.; Honig, A.; Siegert, C.E.H. Anxiety Symptoms, Mortality, and Hospitalization in Patients Receiving Maintenance Dialysis: A Cohort Study. AJKD 2019, 74, 158–166. [Google Scholar] [CrossRef]
- Schouten, R.W.; Nadort, E.; van Ballegooijen, W.; Loosman, W.L.; Honig, A.; Siegert, C.E.H.; Meuleman, Y.; Broekman, B.F.P. General Distress and Symptoms of Anxiety and Depression: A Factor Analysis in Two Cohorts of Dialysis Patients. Gen. Hosp. Pscychiatry 2020, 65, 91–99. [Google Scholar] [CrossRef]
- Zhang, M.; Kim, J.C.; Li, Y.; Shapiro, B.B.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Martin, D.; Kalantar-Zadeh, K.; et al. Relation between Anxiety, Depression, and Physical Activity and Performance in Maintenance Hemodialysis Patients. J. Ren. Nutr. 2014, 24, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Kurtgoz, P.O.; Sackan, F.; Kizilarslanoglu, M.C.; Bilgin, O.; Guney, I. Effect of Anxiety on COVID-19 Infection in Hemodialysis Patients. Ther. Apher. Dial. 2021, 26, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Zahedian, F.; Rahimi, P.; Sarichloo, M.E.; Ghafelehbashi, S.H. Depression, Anxiety and Suicidal Ideation among Patients with Chronic Kidney Disease Undergoing Hemodialysis in Qazvin, Iran. J. Inflamm. Dis. 2020, 23, 550–561. [Google Scholar] [CrossRef]
- Wu, Y.H.; Hsu, Y.J.; Tzeng, W.C. Correlation between Physical Activity and Psychological Distress in Patients Receiving Hemodialysis with Comorbidities: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 3972. [Google Scholar] [CrossRef]
- Sensoy, B.; Gunes, A.; Ari, S. Anxiety and Depression Levels in COVID-19 Disease and Their Relation to Hypertension. Clin. Exp. Hypertens. 2021, 43, 237–241. [Google Scholar] [CrossRef]
- Alsaleh, M.; Videloup, L.; Lobbedez, T.; Lebreuilly, J.; Morello, R.; Lecouf, A.T. Improved Detection and Evaluation of Depression in Patients with Chronic Kidney Disease: Validity and Reliability of Screening (PHQ-2) and Diagnostic (BDI-FS-Fr) Tests of Depression in Chronic Kidney Disease. Kidney Dis. 2019, 5, 228–238. [Google Scholar] [CrossRef]
- Neitzer, A.; Sun, S.; Doss, S.; Moran, J.; Schiller, B. Beck Depression Inventory-Fast Screen (BDI-FS): An Efficient Tool for Depression Screening in Patients with End-stage Renal Disease. Hemodial. Int. 2012, 16, 207–213. [Google Scholar] [CrossRef]
- Andrade, C.P.; Sesso, R.C. Depression in Chronic Kidney Disease and Hemodialysis Patients. Psychology 2012, 3, 974–978. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental Health Problems and Social Media Exposure during COVID-19 Outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Legrand, K.; Speyer, E.; Stengel, B.; Frimat, L.; Ngueyon Sime, W.; Massy, Z.A.; Fouque, D.; Laville, M.; Combe, C.; Jacquelinet, C.; et al. Perceived Health and Quality of Life in Patients with CKD, Including Those with Kidney Failure: Findings from National Surveys in France. Am. J. Kidney Dis. 2020, 75, 868–878. [Google Scholar] [CrossRef]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of Quality of Life between Patients Underwent Peritoneal Dialysis and Hemodialysis: A Systematic Review and Meta-analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Gela, D.; Mengistu, D. Self-management and Associated Factors among Patients with End-Stage Renal Disease Undergoing Hemodialysis at Health Facilities in Addis Ababa, Ethiopia. Int. J. Nephrol. Renovasc. Dis. 2018, 11, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ginieri-Coccossis, M.; Theofilou, P.; Synodinou, C.; Tomaras, V.; Soldatos, C. Quality of Life, Mental Health and Health Beliefs in Haemodialysis and Peritoneal Dialysis Patients: Investigating Differences in Early and Later Years of Current Treatment. BMC Nephrol. 2008, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Yu, I.C.; Fang, J.T.; Tsai, Y.F. Exploring Demands of Hemodialysis Patients in Taiwan: A Two-step Cluster Analysis. PLoS ONE 2020, 15, e0228259. [Google Scholar] [CrossRef] [PubMed]
- Floria, I.; Kontele, I.; Grammatikopoulou, M.G.; Sergentanis, T.N.; Vassilakou, T. Quality of Life of Hemodialysis Patients in Greece: Associations with Socio-Economic, Anthropometric and Nutritional Factors. Int. J. Environ. Res. Public Health 2022, 19, 15389. [Google Scholar] [CrossRef]
- Frost, J. Regression Analysis: An Intuitive Guide for Using and Interpreting Linear Models; Jim Publishing: State College, PA, USA, 2019. [Google Scholar]
- Brioni, E.; Delli Zotti, G.; Apuzzo, L.; Magnaghi, C.; Iodice, M.; Burrai, F.; Manunta, P.; Vezzoli, G.; Manara, D.F.; Villa, G. Self-efficacy and Self-management in Patients in Hemodialysis: A Narrative Review of Multidisciplinary theories. G. Ital. Nefrol. 2021, 38, 2021-vol3. [Google Scholar]
- Griva, K.; Nandakumar, M.; Ng, J.H.; Lam, K.F.Y.; McBain, H.; Newman, S.P. Hemodialysis Self-Management Intervention Randomized Trial (HED-SMART): A Practical Low-intensity Intervention to Improve Adherence and Clinical Markers in Patients Receiving Hemodialysis. Am. J. Kidney Dis. 2018, 71, 371–381. [Google Scholar] [CrossRef]


| Variable | Category | Range | Mean (SD) | n (%) |
|---|---|---|---|---|
| Age in years | 35–91 | 62.24 (11.13) | ||
| Sex | Female | 140 (47.0) | ||
| Male | 158 (53.0) | |||
| Marital status | Single | 28 (9.4) | ||
| Married | 223 (74.8) | |||
| Divorced/living together | 17 (5.7) | |||
| Widow | 30 (10.1) | |||
| Education level | ≤Elementary | 95 (31.9) | ||
| Junior high school | 66 (22.1) | |||
| High school/vocational school | 90 (30.2) | |||
| Diploma (2-year, 3-year, or 5-year program) | 31 (10.4) | |||
| ≥University | 16 (5.4) | |||
| Religion | No | 48 (16.1) | ||
| Yes | 250 (83.9) | |||
| Buddhist | 137 (46.0) | |||
| Taoist | 96 (32.2) | |||
| Christian/Catholic | 13 (4.4) | |||
| I-Kuan Tao | 4 (1.3) | |||
| Employment status | No | 235 (78.9) | ||
| Yes | 63 (21.1) | |||
| Part-time | 20 (6.7) | |||
| Full-time | 43 (14.4) | |||
| Living status | Living alone | 5 (1.7) | ||
| Living with relative or other | 293 (98.3) | |||
| Spouse | 196 (65.8) | |||
| Children | 62 (20.8) | |||
| Relatives | 24 (8.1) | |||
| Friend/nursing aids | 5 (1.7) | |||
| Other | 6 (2.0) | |||
| Social Support | 28–72 | 57.92 (9.83) | ||
| Family, relatives, and friends’ dimension | 16–36 | 29.11 (4.64) | ||
| Medical and nursing staff dimension | 11–36 | 28.81 (6.29) |
| Variable | Items | Range | Mean (SD) | n (%) |
|---|---|---|---|---|
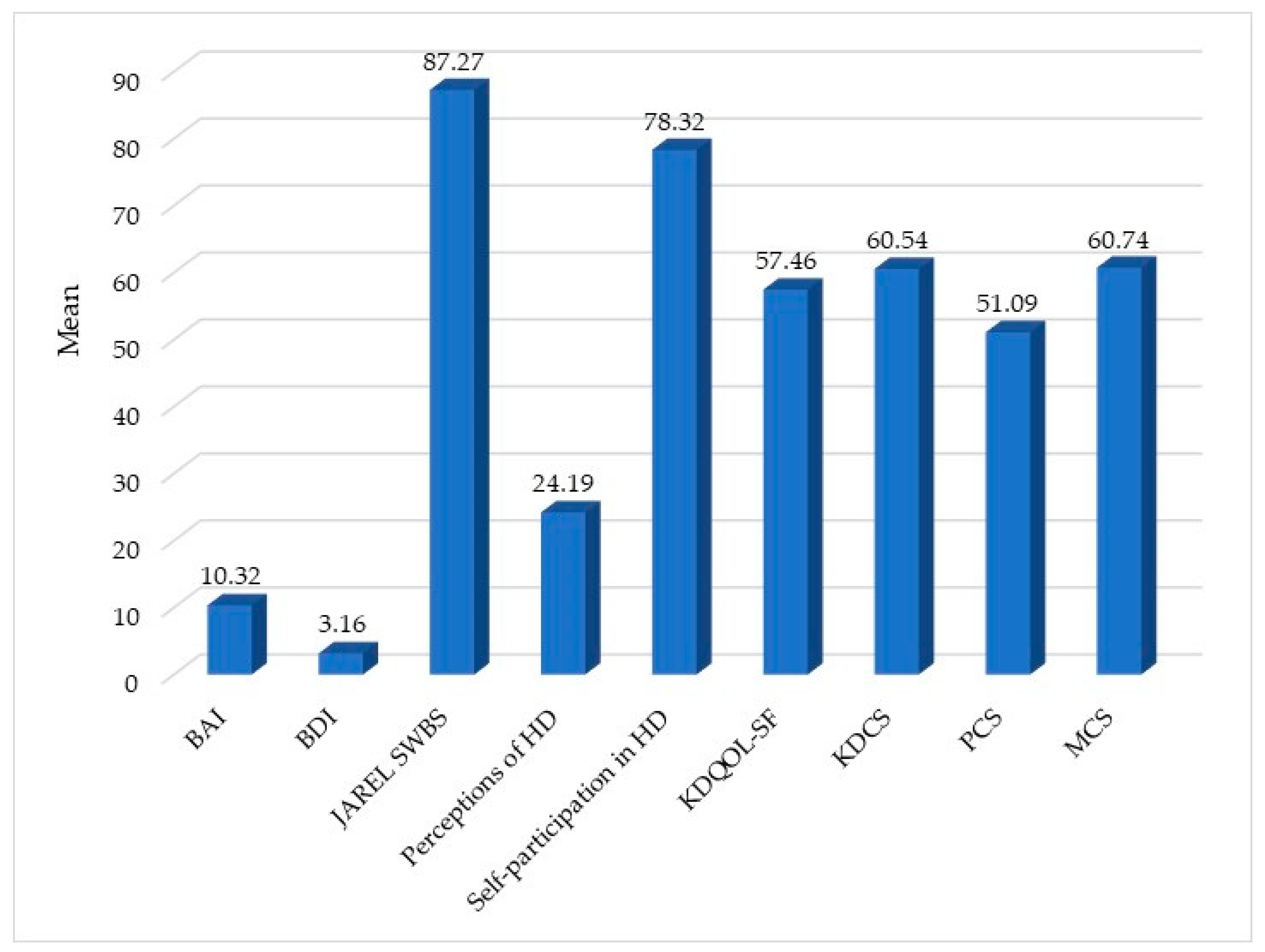
| Beck Anxiety Inventory | 21 | 0–46 | 10.32 (9.73) | |
| 0–7 (Minimal level of anxiety) | 145 (48.7) | |||
| 8–15 (Mild anxiety) | 72 (24.2) | |||
| 16–25 (Moderate anxiety) | 55 (18.5) | |||
| 26–63 (Severe anxiety) | 26 (8.7) | |||
| Beck Depression Inventory | 7 | 0–21 | 3.16 (4.08) | |
| 0–3 (Minimal depression) | 194 (65.1) | |||
| 4–6 (Mild depression) | 52 (17.4) | |||
| 7–9 (Moderate depression) | 18 (6.0) | |||
| 10–21 (Severe depression) | 34 (11.4) | |||
| JAREL Spiritual Well-Being Scale | 21 | 63–123 | 87.27 (9.98) | |
| 51–84 (Moderate) | 140 (47.0) | |||
| 85–126 (High) | 158 (53.0) |
| Variable | Category | Range | Mean (SD) | n (%) |
|---|---|---|---|---|
| Perceived health level | Very poor | 0–4 | 2.19 (0.79) | 4 (1.3) |
| Poor | 46 (15.4) | |||
| Common | 150 (50.3) | |||
| Good | 86 (28.9) | |||
| Very good | 12 (4.0) | |||
| Comorbidity | No | 0–4 | 1.53 (1.03) | 44 (14.8) |
| Yes (multiple choice) | 254(85.2) | |||
| Hypertension | 196 (65.8) | |||
| Diabetes | 121 (40.6) | |||
| Heart disease | 74 (24.8) | |||
| Arthritis | 21 (7.0) | |||
| Stroke | 22 (7.4) | |||
| Other | 22 (7.4) | |||
| Number of comorbidities | None | 0–4 | 1.53 (1.03) | 44 (14.8) |
| 1 type | 116 (38.9) | |||
| 2 types | 87 (29.2) | |||
| 3 types | 38 (12.8) | |||
| 4 types | 13 (4.4) | |||
| HD duration in years | 0–33 | 9.38 (7.30) | ||
| Frequency of hemodialysis per week | 3 times | 290 (97.3) | ||
| 2 times | 8 (2.7) | |||
| HD transportation | Self-preparation (taxi or Rehabus) | 57 (19.1) | ||
| Vehicle | 143 (48.0) | |||
| Motorcycle | 24 (8.1) | |||
| Bus/transit/Formosa Fairway Corporation | 54 (18.1) | |||
| Other | 20 (6.7) | |||
| Accompaniment during HD | No | 114 (38.3) | ||
| Yes | 184 (61.7) | |||
| Family member | 172 (57.7) | |||
| Friend/relative | 5 (1.7) | |||
| Nursing aid | 7 (2.3) |
| Variable | Item | Range | Mean (SD) |
|---|---|---|---|
| Perceptions of HD | 8 | 8–32 | 24.19 (7.07) |
| Self-participation in HD | 29 | 12–116 | 78.32 (23.15) |
| Kidney Disease Quality of Life Short Form (KDQOL-SFtm) | 40 | 22–94 | 57.46 (16.37) |
| Kidney disease composite summary (KDCS) | 24 | 20–100 | 60.54 (14.86) |
| Physical composite summary (PCS) | 9 | 0–94 | 51.09 (20.89) |
| Mental composite summary (MCS) | 7 | 8–100 | 60.74 (22.47) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szu, L.-Y.; Chang, C.-H.; Hsieh, S.-I.; Shih, W.-M.; Huang, L.-M.; Tsai, M.-C.; Tseng, S.-M. Factors Related to Quality of Life of Hemodialysis Patients during the COVID-19 Pandemic. Healthcare 2023, 11, 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11081155
Szu L-Y, Chang C-H, Hsieh S-I, Shih W-M, Huang L-M, Tsai M-C, Tseng S-M. Factors Related to Quality of Life of Hemodialysis Patients during the COVID-19 Pandemic. Healthcare. 2023; 11(8):1155. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11081155
Chicago/Turabian StyleSzu, Li-Yun, Chih-Hsiang Chang, Suh-Ing Hsieh, Whei-Mei Shih, Lan-Mei Huang, Mei-Chu Tsai, and Su-Mei Tseng. 2023. "Factors Related to Quality of Life of Hemodialysis Patients during the COVID-19 Pandemic" Healthcare 11, no. 8: 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11081155