
The Role of Artificial Intelligence in Anterior Cruciate Ligament Injuries: Current Concepts and Future Perspectives
 , , and
, , and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
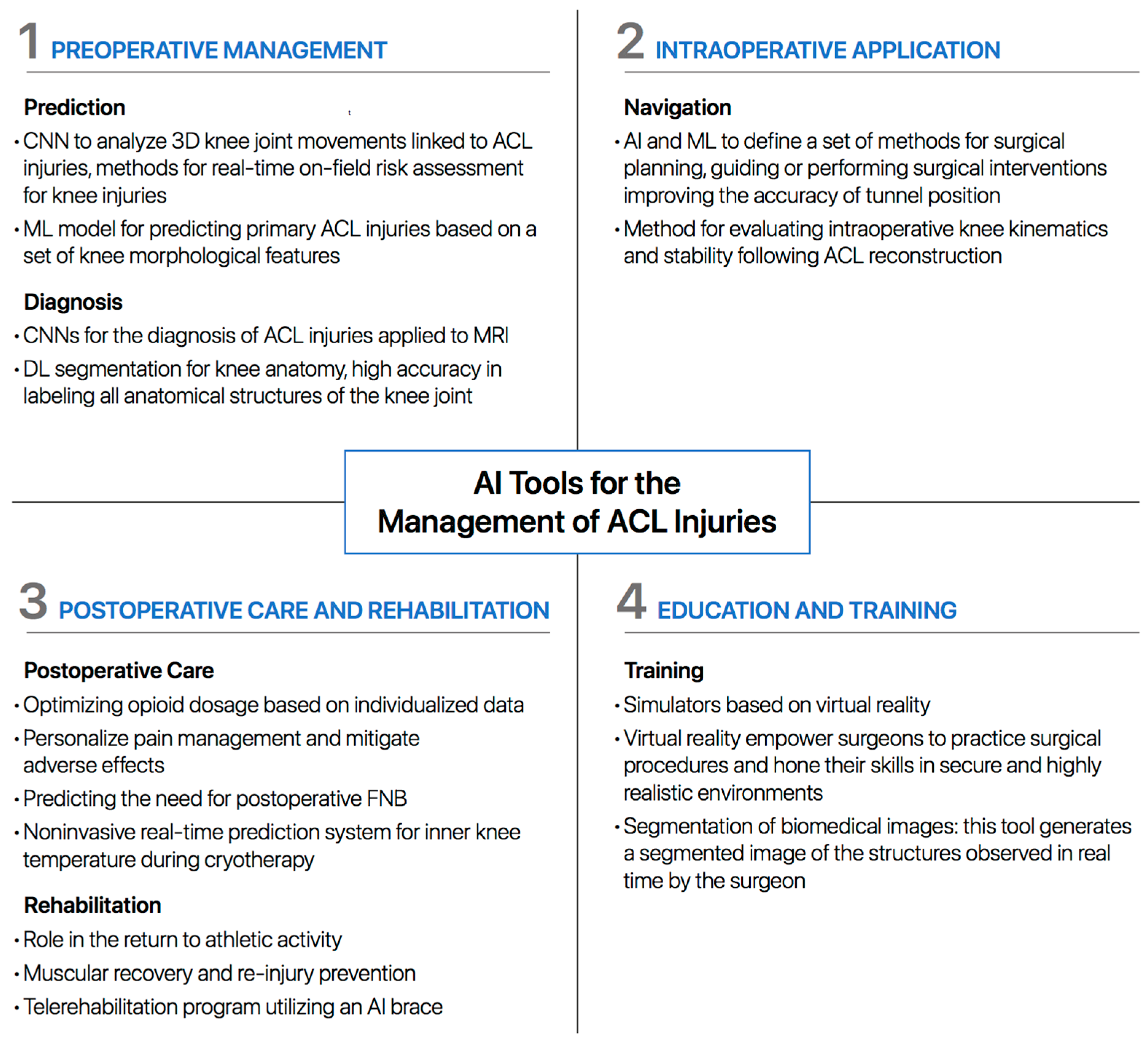
2. AI Tools
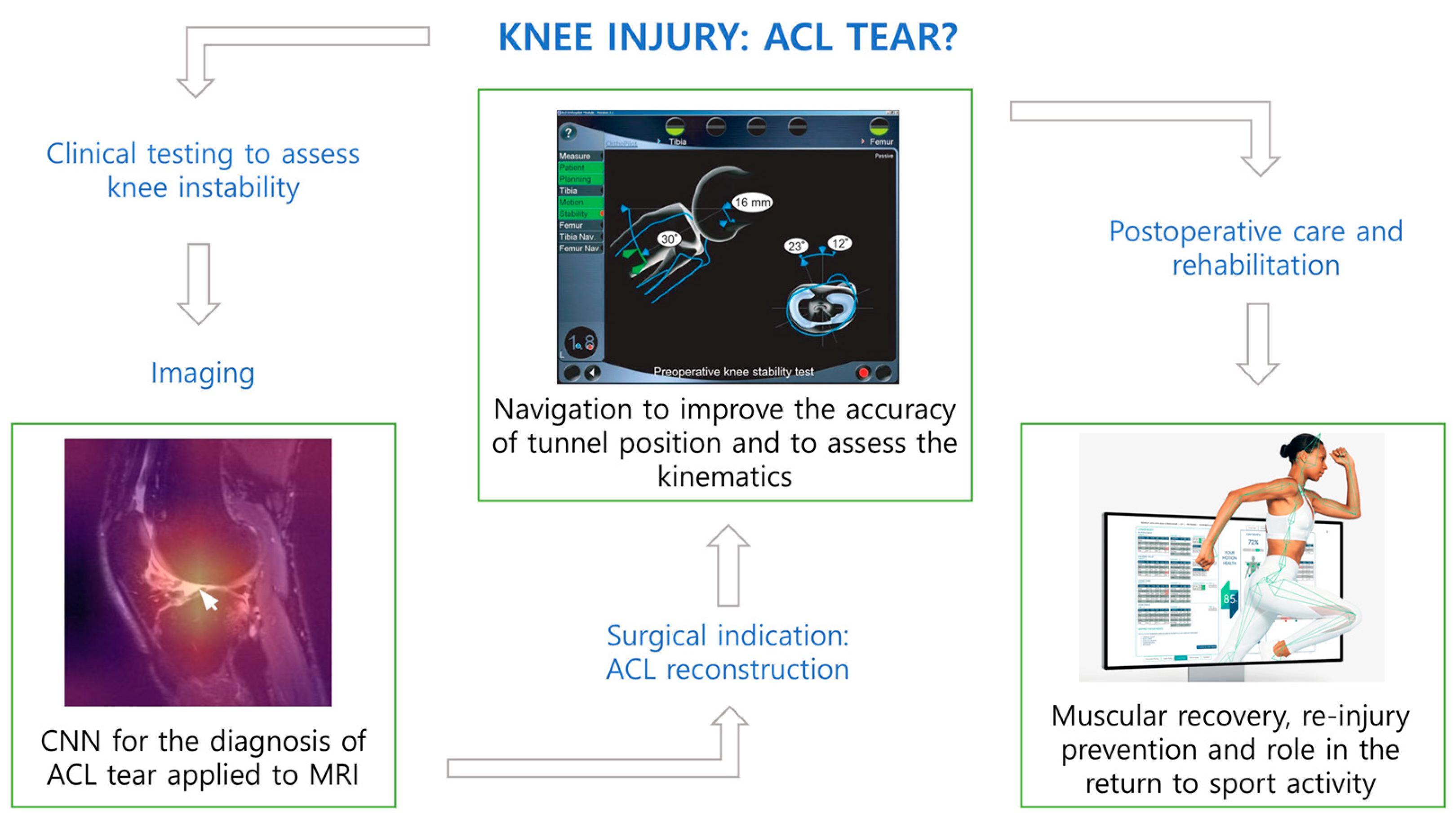
3. Preoperative Management
3.1. Prediction
3.2. Diagnosis
4. Intraoperative Application
5. Postoperative Care and Rehabilitation
5.1. Postoperative Care
5.2. Rehabilitation
6. Education and Training
7. Ethical Considerations and Critical Aspects
8. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beyaz, S. A Brief History of Artificial Intelligence and Robotic Surgery in Orthopedics & Traumatology and Future Expectations. Jt. Dis. Relat. Surg. 2020, 31, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Bini, S.A. Artificial Intelligence, Machine Learning, Deep Learning, and Cognitive Computing: What Do These Terms Mean and How Will They Impact Health Care? J. Arthroplast. 2018, 33, 2358–2361. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Poly, T.N.; Alsinglawi, B.; Lin, L.-F.; Chien, S.-C.; Liu, J.-C.; Jian, W.-S. Application of Artificial Intelligence in COVID-19 Pandemic: Bibliometric Analysis. Healthcare 2021, 9, 441. [Google Scholar] [CrossRef] [PubMed]
- Ramkumar, P.N.; Luu, B.C.; Haeberle, H.S.; Karnuta, J.M.; Nwachukwu, B.U.; Williams, R.J. Sports Medicine and Artificial Intelligence: A Primer. Am. J. Sports Med. 2022, 50, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.K.; Ley, C.; Pareek, A.; Groll, A.; Tischer, T.; Seil, R. Artificial Intelligence and Machine Learning: An Introduction for Orthopaedic Surgeons. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Makhni, E.C.; Makhni, S.; Ramkumar, P.N. Artificial Intelligence for the Orthopaedic Surgeon: An Overview of Potential Benefits, Limitations, and Clinical Applications. J. Am. Acad. Orthop. Surg. 2021, 29, 235–243. [Google Scholar] [CrossRef]
- Myers, T.G.; Ramkumar, P.N.; Ricciardi, B.F.; Urish, K.L.; Kipper, J.; Ketonis, C. Artificial Intelligence and Orthopaedics: An Introduction for Clinicians. J. Bone Jt. Surg. Am. Vol. 2020, 102, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Helm, J.M.; Swiergosz, A.M.; Haeberle, H.S.; Karnuta, J.M.; Schaffer, J.L.; Krebs, V.E.; Spitzer, A.I.; Ramkumar, P.N. Machine Learning and Artificial Intelligence: Definitions, Applications, and Future Directions. Curr. Rev. Musculoskelet. Med. 2020, 13, 69–76. [Google Scholar] [CrossRef]
- Grote, T.; Berens, P. On the Ethics of Algorithmic Decision-Making in Healthcare. J. Med. Ethics 2020, 46, 205–211. [Google Scholar] [CrossRef]
- Maccioni, G.; Ruscitto, S.; Gulino, R.A.; Giansanti, D. Opportunities and Problems of the Consensus Conferences in the Care Robotics. Healthcare 2021, 9, 1624. [Google Scholar] [CrossRef]
- Kaeding, C.C.; Léger-St-Jean, B.; Magnussen, R.A. Epidemiology and Diagnosis of Anterior Cruciate Ligament Injuries. Clin. Sports Med. 2017, 36, 1–8. [Google Scholar] [CrossRef]
- Marshall, S.W. Recommendations for Defining and Classifying Anterior Cruciate Ligament Injuries in Epidemiologic Studies. J. Athl. Train. 2010, 45, 516–518. [Google Scholar] [CrossRef] [PubMed]
- Rhatomy, S.; Ariyanto, M.W.; Fiolin, J.; Dilogo, I.H. Comparison of Clinical Outcomes between Isolated ACL Reconstruction and Combined ACL with Anterolateral Ligament Reconstruction: A Systematic Review and Meta-Analysis. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Minzlaff, P.; Heidt, T.; Feucht, M.J.; Plath, J.E.; Hinterwimmer, S.; Imhoff, A.B.; Saier, T. Patient Satisfaction with Health Is Substantially Improved Following ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Corban, J.; Lorange, J.-P.; Laverdiere, C.; Khoury, J.; Rachevsky, G.; Burman, M.; Martineau, P.A. Artificial Intelligence in the Management of Anterior Cruciate Ligament Injuries. Orthop. J. Sports Med. 2021, 9, 23259671211014206. [Google Scholar] [CrossRef]
- Lisacek-Kiosoglous, A.B.; Powling, A.S.; Fontalis, A.; Gabr, A.; Mazomenos, E.; Haddad, F.S. Artificial Intelligence in Orthopaedic Surgery. Bone Jt. Res. 2023, 12, 447–454. [Google Scholar] [CrossRef]
- Cabitza, F.; Locoro, A.; Banfi, G. Machine Learning in Orthopedics: A Literature Review. Front. Bioeng. Biotechnol. 2018, 6, 75. [Google Scholar] [CrossRef]
- Pedoia, V.; Lansdown, D.A.; Zaid, M.; McCulloch, C.E.; Souza, R.; Ma, C.B.; Li, X. Three-Dimensional MRI-Based Statistical Shape Model and Application to a Cohort of Knees with Acute ACL Injury. Osteoarthr. Cartil. 2015, 23, 1695–1703. [Google Scholar] [CrossRef]
- Johnson, W.R.; Mian, A.; Lloyd, D.G.; Alderson, J.A. On-Field Player Workload Exposure and Knee Injury Risk Monitoring via Deep Learning. J. Biomech. 2019, 93, 185–193. [Google Scholar] [CrossRef]
- Taborri, J.; Molinaro, L.; Santospagnuolo, A.; Vetrano, M.; Vulpiani, M.C.; Rossi, S. A Machine-Learning Approach to Measure the Anterior Cruciate Ligament Injury Risk in Female Basketball Players. Sensors 2021, 21, 3141. [Google Scholar] [CrossRef]
- Tamimi, I.; Ballesteros, J.; Lara, A.P.; Tat, J.; Alaqueel, M.; Schupbach, J.; Marwan, Y.; Urdiales, C.; Gomez-de-Gabriel, J.M.; Burman, M.; et al. A Prediction Model for Primary Anterior Cruciate Ligament Injury Using Artificial Intelligence. Orthop. J. Sports Med. 2021, 9, 23259671211027543. [Google Scholar] [CrossRef] [PubMed]
- Santomartino, S.M.; Kung, J.; Yi, P.H. Systematic Review of Artificial Intelligence Development and Evaluation for MRI Diagnosis of Knee Ligament or Meniscus Tears. Skelet. Radiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Guermazi, A.; Tannoury, C.; Kompel, A.J.; Murakami, A.M.; Ducarouge, A.; Gillibert, A.; Li, X.; Tournier, A.; Lahoud, Y.; Jarraya, M.; et al. Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence. Radiology 2022, 302, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Kunze, K.N.; Rossi, D.M.; White, G.M.; Karhade, A.V.; Deng, J.; Williams, B.T.; Chahla, J. Diagnostic Performance of Artificial Intelligence for Detection of Anterior Cruciate Ligament and Meniscus Tears: A Systematic Review. Arthroscopy 2021, 37, 771–781. [Google Scholar] [CrossRef]
- Fritz, B.; Fritz, J. Artificial Intelligence for MRI Diagnosis of Joints: A Scoping Review of the Current State-of-the-Art of Deep Learning-Based Approaches. Skelet. Radiol. 2022, 51, 315–329. [Google Scholar] [CrossRef]
- van Eck, C.F.; van den Bekerom, M.P.J.; Fu, F.H.; Poolman, R.W.; Kerkhoffs, G.M.M.J. Methods to Diagnose Acute Anterior Cruciate Ligament Rupture: A Meta-Analysis of Physical Examinations with and without Anaesthesia. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1895–1903. [Google Scholar] [CrossRef] [PubMed]
- Štajduhar, I.; Mamula, M.; Miletić, D.; Ünal, G. Semi-Automated Detection of Anterior Cruciate Ligament Injury from MRI. Comput. Methods Programs Biomed. 2017, 140, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Bien, N.; Rajpurkar, P.; Ball, R.L.; Irvin, J.; Park, A.; Jones, E.; Bereket, M.; Patel, B.N.; Yeom, K.W.; Shpanskaya, K.; et al. Deep-Learning-Assisted Diagnosis for Knee Magnetic Resonance Imaging: Development and Retrospective Validation of MRNet. PLoS Med. 2018, 15, e1002699. [Google Scholar] [CrossRef]
- Liu, F.; Guan, B.; Zhou, Z.; Samsonov, A.; Rosas, H.; Lian, K.; Sharma, R.; Kanarek, A.; Kim, J.; Guermazi, A.; et al. Fully Automated Diagnosis of Anterior Cruciate Ligament Tears on Knee MR Images by Using Deep Learning. Radiol. Artif. Intell. 2019, 1, 180091. [Google Scholar] [CrossRef]
- Richardson, M.L. MR Protocol Optimization With Deep Learning: A Proof of Concept. Curr. Probl. Diagn. Radiol. 2021, 50, 168–174. [Google Scholar] [CrossRef]
- Chang, P.D.; Wong, T.T.; Rasiej, M.J. Deep Learning for Detection of Complete Anterior Cruciate Ligament Tear. J. Digit. Imaging 2019, 32, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, M.; Zhou, Y.; Lu, G.; Zhou, Q. Deep Learning Approach for Anterior Cruciate Ligament Lesion Detection: Evaluation of Diagnostic Performance Using Arthroscopy as the Reference Standard. J. Magn. Reson. Imaging 2020, 52, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Germann, C.; Marbach, G.; Civardi, F.; Fucentese, S.F.; Fritz, J.; Sutter, R.; Pfirrmann, C.W.A.; Fritz, B. Deep Convolutional Neural Network-Based Diagnosis of Anterior Cruciate Ligament Tears: Performance Comparison of Homogenous Versus Heterogeneous Knee MRI Cohorts With Different Pulse Sequence Protocols and 1.5-T and 3-T Magnetic Field Strengths. Investig. Radiol. 2020, 55, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Namiri, N.K.; Flament, I.; Astuto, B.; Shah, R.; Tibrewala, R.; Caliva, F.; Link, T.M.; Pedoia, V.; Majumdar, S. Deep Learning for Hierarchical Severity Staging of Anterior Cruciate Ligament Injuries from MRI. Radiol. Artif. Intell. 2020, 2, e190207. [Google Scholar] [CrossRef] [PubMed]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Mohammed, M.A.; Garcia-Zapirain, B.; Abdulkareem, K.H. Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach. Diagnostics 2021, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ren, S.; Zhou, R.; Jiang, X.; You, T.; Li, C.; Zhang, W. Deep Learning-Based Magnetic Resonance Imaging Image Features for Diagnosis of Anterior Cruciate Ligament Injury. J. Health Eng. 2021, 2021, 4076175. [Google Scholar] [CrossRef] [PubMed]
- Astuto, B.; Flament, I.; KNamiri, N.; Shah, R.; Bharadwaj, U.; MLink, T.; DBucknor, M.; Pedoia, V.; Majumdar, S. Automatic Deep Learning-Assisted Detection and Grading of Abnormalities in Knee MRI Studies. Radiol. Artif. Intell. 2021, 3, e200165. [Google Scholar] [CrossRef]
- Jeon, Y.; Yoshino, K.; Hagiwara, S.; Watanabe, A.; Quek, S.T.; Yoshioka, H.; Feng, M. Interpretable and Lightweight 3-D Deep Learning Model for Automated ACL Diagnosis. IEEE J. Biomed. Health Inform. 2021, 25, 2388–2397. [Google Scholar] [CrossRef]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Rehman, A.; Nobanee, H.; Shabir, H. Improved Deep Convolutional Neural Network to Classify Osteoarthritis from Anterior Cruciate Ligament Tear Using Magnetic Resonance Imaging. J. Pers. Med. 2021, 11, 1163. [Google Scholar] [CrossRef]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Rehman, A.; Garcia-Zapirain, B. Automated Knee MR Images Segmentation of Anterior Cruciate Ligament Tears. Sensors 2022, 22, 1552. [Google Scholar] [CrossRef]
- Sridhar, S.; Amutharaj, J.; Valsalan, P.; Arthi, B.; Ramkumar, S.; Mathupriya, S.; Rajendran, T.; Waji, Y.A. A Torn ACL Mapping in Knee MRI Images Using Deep Convolution Neural Network with Inception-V3. J. Health Eng. 2022, 2022, 7872500. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Bai, H.; Zhang, F.; Zhou, Y.; Lin, Q.; Zhou, Q.; Feng, Q.; Zhang, L. Automatic Segmentation Model of Intercondylar Fossa Based on Deep Learning: A Novel and Effective Assessment Method for the Notch Volume. BMC Musculoskelet. Disord. 2022, 23, 426. [Google Scholar] [CrossRef]
- Minamoto, Y.; Akagi, R.; Maki, S.; Shiko, Y.; Tozawa, R.; Kimura, S.; Yamaguchi, S.; Kawasaki, Y.; Ohtori, S.; Sasho, T. Automated Detection of Anterior Cruciate Ligament Tears Using a Deep Convolutional Neural Network. BMC Musculoskelet. Disord. 2022, 23, 577. [Google Scholar] [CrossRef]
- Tran, A.; Lassalle, L.; Zille, P.; Guillin, R.; Pluot, E.; Adam, C.; Charachon, M.; Brat, H.; Wallaert, M.; d’Assignies, G.; et al. Deep Learning to Detect Anterior Cruciate Ligament Tear on Knee MRI: Multi-Continental External Validation. Eur. Radiol. 2022, 32, 8394–8403. [Google Scholar] [CrossRef] [PubMed]
- Mei, X.; Liu, Z.; Robson, P.M.; Marinelli, B.; Huang, M.; Doshi, A.; Jacobi, A.; Cao, C.; Link, K.E.; Yang, T.; et al. RadImageNet: An Open Radiologic Deep Learning Research Dataset for Effective Transfer Learning. Radiol. Artif. Intell. 2022, 4, e210315. [Google Scholar] [CrossRef] [PubMed]
- Dunnhofer, M.; Martinel, N.; Micheloni, C. Deep Convolutional Feature Details for Better Knee Disorder Diagnoses in Magnetic Resonance Images. Comput. Med. Imaging Graph. 2022, 102, 102142. [Google Scholar] [CrossRef]
- Flannery, S.W.; Beveridge, J.E.; Proffen, B.L.; Walsh, E.G.; BEAR Trial Team; Kramer, D.E.; Murray, M.M.; Kiapour, A.M.; Fleming, B.C. Predicting Anterior Cruciate Ligament Failure Load with T2* Relaxometry and Machine Learning as a Prospective Imaging Biomarker for Revision Surgery. Sci. Rep. 2023, 13, 3524. [Google Scholar] [CrossRef]
- Gaj, S.; Eck, B.L.; Xie, D.; Lartey, R.; Lo, C.; Zaylor, W.; Yang, M.; Nakamura, K.; Winalski, C.S.; Spindler, K.P.; et al. Deep Learning-Based Automatic Pipeline for Quantitative Assessment of Thigh Muscle Morphology and Fatty Infiltration. Magn. Reson. Med. 2023, 89, 2441–2455. [Google Scholar] [CrossRef]
- Wang, D.-Y.; Ding, J.; Sun, A.-L.; Liu, S.-G.; Jiang, D.; Li, N.; Yu, J.-K. Artificial Intelligence Suppression as a Strategy to Mitigate Artificial Intelligence Automation Bias. J. Am. Med. Inform. Assoc. 2023, 30, 1684–1692. [Google Scholar] [CrossRef]
- Wang, D.-Y.; Liu, S.-G.; Ding, J.; Sun, A.-L.; Jiang, D.; Jiang, J.; Zhao, J.-Z.; Chen, D.-S.; Ji, G.; Li, N.; et al. A Deep Learning Model Enhances Clinicians’ Diagnostic Accuracy to More Than 96% for Anterior Cruciate Ligament Ruptures on Magnetic Resonance Imaging. Arthroscopy 2023. S0749-8063(23)00663-1. [Google Scholar] [CrossRef]
- Liang, C.; Li, X.; Qin, Y.; Li, M.; Ma, Y.; Wang, R.; Xu, X.; Yu, J.; Lv, S.; Luo, H. Effective Automatic Detection of Anterior Cruciate Ligament Injury Using Convolutional Neural Network with Two Attention Mechanism Modules. BMC Med. Imaging 2023, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Kulseng, C.P.S.; Nainamalai, V.; Grøvik, E.; Geitung, J.-T.; Årøen, A.; Gjesdal, K.-I. Automatic Segmentation of Human Knee Anatomy by a Convolutional Neural Network Applying a 3D MRI Protocol. BMC Musculoskelet. Disord. 2023, 24, 41. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, F.; Figueroa, D.; Guiloff, R.; Putnis, S.; Fritsch, B.; Itriago, M. Navigation in Anterior Cruciate Ligament Reconstruction: State of the Art. J. ISAKOS 2023, 8, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Zaffagnini, S.; Urrizola, F.; Signorelli, C.; Grassi, A.; Di Sarsina, T.R.; Lucidi, G.A.; Marcheggiani Muccioli, G.M.; Bonanzinga, T.; Marcacci, M. Current Use of Navigation System in ACL Surgery: A Historical Review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3396–3409. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, B.H.; Mekuria, K.; Cho, H.; Park, S.; Wang, J.H.; Lee, D. Registration Accuracy Enhancement of a Surgical Navigation System for Anterior Cruciate Ligament Reconstruction: A Phantom and Cadaveric Study. Knee 2017, 24, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Karkenny, A.J.; Mendelis, J.R.; Geller, D.S.; Gomez, J.A. The Role of Intraoperative Navigation in Orthopaedic Surgery. J. Am. Acad. Orthop. Surg. 2019, 27, e849–e858. [Google Scholar] [CrossRef] [PubMed]
- Samitier, G.; Marcano, A.I.; Alentorn-Geli, E.; Cugat, R.; Farmer, K.W.; Moser, M.W. Failure of Anterior Cruciate Ligament Reconstruction. Arch. Bone Jt. Surg. 2015, 3, 220–240. [Google Scholar]
- Endele, D.; Jung, C.; Becker, U.; Bauer, G.; Mauch, F. Anterior Cruciate Ligament Reconstruction with and without Computer Navigation: A Clinical and Magnetic Resonance Imaging Evaluation 2 Years after Surgery. Arthroscopy 2009, 25, 1067–1074. [Google Scholar] [CrossRef]
- Kawakami, Y.; Hiranaka, T.; Matsumoto, T.; Hida, Y.; Fukui, T.; Uemoto, H.; Doita, M.; Tsuji, M.; Kurosaka, M.; Kuroda, R. The Accuracy of Bone Tunnel Position Using Fluoroscopic-Based Navigation System in Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1503–1510. [Google Scholar] [CrossRef]
- Luites, J.W.H.; Wymenga, A.B.; Blankevoort, L.; Eygendaal, D.; Verdonschot, N. Accuracy of a Computer-Assisted Planning and Placement System for Anatomical Femoral Tunnel Positioning in Anterior Cruciate Ligament Reconstruction. Int. J. Med. Robot. 2014, 10, 438–446. [Google Scholar] [CrossRef]
- Shafizadeh, S.; Balke, M.; Wegener, S.; Tjardes, T.; Bouillon, B.; Hoeher, J.; Baethis, H. Precision of Tunnel Positioning in Navigated Anterior Cruciate Ligament Reconstruction. Arthroscopy 2011, 27, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Taketomi, S.; Inui, H.; Sanada, T.; Nakamura, K.; Yamagami, R.; Masuda, H.; Tanaka, S.; Nakagawa, T. Remnant-Preserving Anterior Cruciate Ligament Reconstruction Using a Three-Dimensional Fluoroscopic Navigation System. Knee Surg. Relat. Res. 2014, 26, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Plaweski, S.; Schlatterer, B.; Saragaglia, D.; Computer Assisted Orthopedic Surgery—France (CAOS—France). The Role of Computer Assisted Navigation in Revision Surgery for Failed Anterior Cruciate Ligament Reconstruction of the Knee: A Continuous Series of 52 Cases. Orthop. Traumatol. Surg. Res. 2015, 101, S227–S231. [Google Scholar] [CrossRef] [PubMed]
- Taketomi, S.; Inui, H.; Nakamura, K.; Hirota, J.; Takei, S.; Takeda, H.; Tanaka, S.; Nakagawa, T. Three-Dimensional Fluoroscopic Navigation Guidance for Femoral Tunnel Creation in Revision Anterior Cruciate Ligament Reconstruction. Arthrosc. Tech. 2012, 1, e95–e99. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Kum, D.H.; Rhyu, I.J.; Kim, Y.; Cho, H.; Wang, J.H. Clinical Advantages of Image-Free Navigation System Using Surface-Based Registration in Anatomical Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3556–3564. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.; Björnsson, H.; Musahl, V.; Bhandari, M.; Petzold, M.; Fu, F.H.; Samuelsson, K. Anatomic Single- versus Double-Bundle ACL Reconstruction: A Meta-Analysis. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1009–1023. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, H.; Desai, N.; Musahl, V.; Alentorn-Geli, E.; Bhandari, M.; Fu, F.; Samuelsson, K. Is Double-Bundle Anterior Cruciate Ligament Reconstruction Superior to Single-Bundle? A Comprehensive Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 696–739. [Google Scholar] [CrossRef] [PubMed]
- Komzák, M.; Hart, R.; Feranec, M.; Šmíd, P.; Kocová, R. In Vivo Knee Rotational Stability 2 Years after Double-Bundle and Anatomic Single-Bundle ACL Reconstruction. Eur. J. Trauma Emerg. Surg. 2018, 44, 105–111. [Google Scholar] [CrossRef]
- Zaffagnini, S.; Signorelli, C.; Lopomo, N.; Bonanzinga, T.; Marcheggiani Muccioli, G.M.; Bignozzi, S.; Visani, A.; Marcacci, M. Anatomic Double-Bundle and over-the-Top Single-Bundle with Additional Extra-Articular Tenodesis: An In Vivo Quantitative Assessment of Knee Laxity in Two Different ACL Reconstructions. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 153–159. [Google Scholar] [CrossRef]
- Neri, T.; Dabirrahmani, D.; Beach, A.; Grasso, S.; Putnis, S.; Oshima, T.; Cadman, J.; Devitt, B.; Coolican, M.; Fritsch, B.; et al. Different Anterolateral Procedures Have Variable Impact on Knee Kinematics and Stability When Performed in Combination with Anterior Cruciate Ligament Reconstruction. J. ISAKOS 2021, 6, 74–81. [Google Scholar] [CrossRef]
- Saltzman, B.M.; Cvetanovich, G.L.; Nwachukwu, B.U.; Mall, N.A.; Bush-Joseph, C.A.; Bach, B.R. Economic Analyses in Anterior Cruciate Ligament Reconstruction: A Qualitative and Systematic Review. Am. J. Sports Med. 2016, 44, 1329–1335. [Google Scholar] [CrossRef]
- Baldini, A.; Von Korff, M.; Lin, E.H.B. A Review of Potential Adverse Effects of Long-Term Opioid Therapy: A Practitioner’s Guide. Prim. Care Companion J. Clin. Psychiatry 2012, 14, 23cr03567. [Google Scholar] [CrossRef] [PubMed]
- Emam, O.S.; Eldaly, A.S.; Avila, F.R.; Torres-Guzman, R.A.; Maita, K.C.; Garcia, J.P.; Anne Brown, S.; Haider, C.R.; Forte, A.J. Machine Learning Algorithms Predict Long-Term Postoperative Opioid Misuse: A Systematic Review. Am. Surg. 2023, 90, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Bumgarner, J.R.; Becker-Krail, D.D.; White, R.C.; Nelson, R.J. Machine Learning and Deep Learning Frameworks for the Automated Analysis of Pain and Opioid Withdrawal Behaviors. Front. Neurosci. 2022, 16, 953182. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, T.; Knight, R.; Nolan, S.; Quick, O.; Ti, L. Artificial Intelligence Interventions Focused on Opioid Use Disorders: A Review of the Gray Literature. Am. J. Drug Alcohol Abus. 2021, 47, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Bharat, C.; Hickman, M.; Barbieri, S.; Degenhardt, L. Big Data and Predictive Modelling for the Opioid Crisis: Existing Research and Future Potential. Lancet Digit. Health 2021, 3, e397–e407. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.B.; Grazal, C.F.; Balazs, G.C.; Potter, B.K.; Dickens, J.F.; Forsberg, J.A. Can Predictive Modeling Tools Identify Patients at High Risk of Prolonged Opioid Use after ACL Reconstruction? Clin. Orthop. Relat. Res. 2020, 478, 1610–1618. [Google Scholar] [CrossRef] [PubMed]
- Garbin, C.; Marques, N.; Marques, O. Machine Learning for Predicting Opioid Use Disorder from Healthcare Data: A Systematic Review. Comput. Methods Programs Biomed. 2023, 236, 107573. [Google Scholar] [CrossRef]
- Liu, H.; Song, X.; Li, C.; Li, Y.; Guo, W.; Zhang, H. Femoral Nerve Block and Local Instillation Analgesia Associated with More Reliable Efficacy in Regional Anesthesia Interventions within 24 Hours Following Anterior Cruciate Ligament Reconstruction: A Network Meta-Analysis. Arthroscopy 2023, 39, 1273–1295. [Google Scholar] [CrossRef]
- Hussain, N.; Brull, R.; Vannabouathong, C.; Speer, J.; Lagnese, C.; McCartney, C.J.L.; Abdallah, F.W. Network Meta-Analysis of the Analgesic Effectiveness of Regional Anaesthesia Techniques for Anterior Cruciate Ligament Reconstruction. Anaesthesia 2023, 78, 207–224. [Google Scholar] [CrossRef]
- Tighe, P.; Laduzenski, S.; Edwards, D.; Ellis, N.; Boezaart, A.P.; Aygtug, H. Use of Machine Learning Theory to Predict the Need for Femoral Nerve Block Following ACL Repair. Pain Med. 2011, 12, 1566–1575. [Google Scholar] [CrossRef]
- Glattke, K.E.; Tummala, S.V.; Chhabra, A. Anterior Cruciate Ligament Reconstruction Recovery and Rehabilitation: A Systematic Review. JBJS 2022, 104, 739–754. [Google Scholar] [CrossRef]
- Rashkovska, A.; Kocev, D.; Trobec, R. Non-Invasive Real-Time Prediction of Inner Knee Temperatures during Therapeutic Cooling. Comput. Methods Programs Biomed. 2015, 122, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Corban, J.; Karatzas, N.; Zhao, K.Y.; Babouras, A.; Bergeron, S.; Fevens, T.; Rivaz, H.; Martineau, P.A. Using an Affordable Motion Capture System to Evaluate the Prognostic Value of Drop Vertical Jump Parameters for Noncontact ACL Injury. Am. J. Sports Med. 2023, 51, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Daggett, M.C.; Witte, K.A.; Cabarkapa, D.; Cabarkapa, D.V.; Fry, A.C. Evidence-Based Data Models for Return-to-Play Criteria after Anterior Cruciate Ligament Reconstruction. Healthcare 2022, 10, 929. [Google Scholar] [CrossRef]
- Lee, O.T.; Williams, M.A.; Shaw, C.D.; Delextrat, A. The Role of Strength-Related Factors on Psychological Readiness for Return to Sport Following Anterior Cruciate Ligament (ACL) Reconstruction. Healthcare 2023, 11, 2787. [Google Scholar] [CrossRef] [PubMed]
- Richter, C.; King, E.; Strike, S.; Franklyn-Miller, A. Objective Classification and Scoring of Movement Deficiencies in Patients with Anterior Cruciate Ligament Reconstruction. PLoS ONE 2019, 14, e0206024. [Google Scholar] [CrossRef]
- Fouasson-Chailloux, A.; Crenn, V.; Louguet, B.; Grondin, J.; Menu, P.; Dauty, M. Therapeutic Patient Education after Anterior Cruciate Ligament Reconstruction: Evaluation of the Knowledge and Certitudes with a Self-Report Questionnaire. Healthcare 2022, 10, 934. [Google Scholar] [CrossRef]
- Zhao, D.; Pan, J.-K.; Lin, F.-Z.; Luo, M.-H.; Liang, G.-H.; Zeng, L.-F.; Huang, H.-T.; Han, Y.-H.; Xu, N.-J.; Yang, W.-Y.; et al. Risk Factors for Revision or Rerupture after Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. Am. J. Sports Med. 2023, 51, 3053–3075. [Google Scholar] [CrossRef]
- Pillitteri, G.; Petrigna, L.; Ficarra, S.; Giustino, V.; Thomas, E.; Rossi, A.; Clemente, F.M.; Paoli, A.; Petrucci, M.; Bellafiore, M.; et al. Relationship between External and Internal Load Indicators and Injury Using Machine Learning in Professional Soccer: A Systematic Review and Meta-Analysis. Res. Sports Med. 2023, 1–38. [Google Scholar] [CrossRef]
- Martin, R.K.; Wastvedt, S.; Pareek, A.; Persson, A.; Visnes, H.; Fenstad, A.M.; Moatshe, G.; Wolfson, J.; Lind, M.; Engebretsen, L. Machine Learning Algorithm to Predict Anterior Cruciate Ligament Revision Demonstrates External Validity. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.K.; Wastvedt, S.; Pareek, A.; Persson, A.; Visnes, H.; Fenstad, A.M.; Moatshe, G.; Wolfson, J.; Engebretsen, L. Predicting Anterior Cruciate Ligament Reconstruction Revision: A Machine Learning Analysis Utilizing the Norwegian Knee Ligament Register. JBJS 2022, 104, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.K.; Wastvedt, S.; Pareek, A.; Persson, A.; Visnes, H.; Fenstad, A.M.; Moatshe, G.; Wolfson, J.; Lind, M.; Engebretsen, L. Ceiling Effect of the Combined Norwegian and Danish Knee Ligament Registers Limits Anterior Cruciate Ligament Reconstruction Outcome Prediction. Am. J. Sports Med. 2023, 51, 2324–2332. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-J.; Lee, K.-T.; Chiang, L.-Y.; Liang, C.-H.; Chen, C.-P. Postoperative Rehabilitation after Anterior Cruciate Ligament Reconstruction through Telerehabilitation with Artificial Intelligence Brace during COVID-19 Pandemic. J. Clin. Med. 2023, 12, 4865. [Google Scholar] [CrossRef]
- Rossi, S.M.P.; Panzera, R.M.; Sangaletti, R.; Andriollo, L.; Giudice, L.; Lecci, F.; Benazzo, F. Problems and Opportunities of a Smartphone-Based Care Management Platform: Application of the Wald Principles to a Survey-Based Analysis of Patients’ Perception in a Pilot Center. Healthcare 2024, 12, 153. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, F.; Thomsen, A.S.S.; Nayahangan, L.J.; Konge, L. Surgical Simulation: Current Practices and Future Perspectives for Technical Skills Training. Med. Teach. 2018, 40, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Bajka, M.; Tuchschmid, S.; Fink, D.; Székely, G.; Harders, M. Establishing Construct Validity of a Virtual-Reality Training Simulator for Hysteroscopy via a Multimetric Scoring System. Surg. Endosc. 2010, 24, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.M.P.; Mancino, F.; Sangaletti, R.; Perticarini, L.; Lucenti, L.; Benazzo, F. Augmented Reality in Orthopedic Surgery and Its Application in Total Joint Arthroplasty: A Systematic Review. Appl. Sci. 2022, 12, 5278. [Google Scholar] [CrossRef]
- DiPietro, R.; Ahmidi, N.; Malpani, A.; Waldram, M.; Lee, G.I.; Lee, M.R.; Vedula, S.S.; Hager, G.D. Segmenting and Classifying Activities in Robot-Assisted Surgery with Recurrent Neural Networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 2005–2020. [Google Scholar] [CrossRef]
- Beaudoin, A.; Larrivée, S.; McRae, S.; Leiter, J.; Stranges, G. Module-Based Arthroscopic Knee Simulator Training Improves Technical Skills in Naive Learners: A Randomized Trial. Arthrosc. Sports Med. Rehabil. 2021, 3, e757–e764. [Google Scholar] [CrossRef]
- Antonis, J.; Bahadori, S.; Gallagher, K.; Immins, T.; Wainwright, T.W.; Middleton, R. Validation of the Anterior Cruciate Ligament (ACL) Module of the VirtaMed Virtual Reality Arthroscopy Trainer. Surg. Technol. Int. 2019, 35, 311–319. [Google Scholar] [PubMed]
- Vaghela, K.R.; Trockels, A.; Carobene, M. Active vs Passive Haptic Feedback Technology in Virtual Reality Arthroscopy Simulation: Which Is Most Realistic? J. Clin. Orthop. Trauma 2021, 16, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Tronchot, A.; Casy, T.; Vallee, N.; Common, H.; Thomazeau, H.; Jannin, P.; Huaulmé, A. Virtual Reality Simulation Training Improve Diagnostic Knee Arthroscopy and Meniscectomy Skills: A Prospective Transfer Validity Study. J. Exp. Orthop. 2023, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Paysan, D.; Haug, L.; Bajka, M.; Oelhafen, M.; Buhmann, J.M. Self-Supervised Representation Learning for Surgical Activity Recognition. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 2037–2044. [Google Scholar] [CrossRef] [PubMed]
- Palet, M.J.; Antúnez-Riveros, M.; Barahona, M. Construct Validity of a Virtual Reality Simulator for Surgical Training in Knee Arthroscopy. Cureus 2021, 13, e15237. [Google Scholar] [CrossRef] [PubMed]
- Jonmohamadi, Y.; Takeda, Y.; Liu, F.; Sasazawa, F.; Maicas, G.; Crawford, R.; Roberts, J.; Pandey, A.K.; Carneiro, G. Automatic Segmentation of Multiple Structures in Knee Arthroscopy Using Deep Learning. IEEE Access 2020, 8, 51853–51861. [Google Scholar] [CrossRef]
- Kaya Bicer, E.; Fangerau, H.; Sur, H. Artifical Intelligence Use in Orthopedics: An Ethical Point of View. EFORT Open Rev. 2023, 8, 592–596. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andriollo, L.; Picchi, A.; Sangaletti, R.; Perticarini, L.; Rossi, S.M.P.; Logroscino, G.; Benazzo, F. The Role of Artificial Intelligence in Anterior Cruciate Ligament Injuries: Current Concepts and Future Perspectives. Healthcare 2024, 12, 300. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12030300
Andriollo L, Picchi A, Sangaletti R, Perticarini L, Rossi SMP, Logroscino G, Benazzo F. The Role of Artificial Intelligence in Anterior Cruciate Ligament Injuries: Current Concepts and Future Perspectives. Healthcare. 2024; 12(3):300. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12030300
Chicago/Turabian StyleAndriollo, Luca, Aurelio Picchi, Rudy Sangaletti, Loris Perticarini, Stefano Marco Paolo Rossi, Giandomenico Logroscino, and Francesco Benazzo. 2024. "The Role of Artificial Intelligence in Anterior Cruciate Ligament Injuries: Current Concepts and Future Perspectives" Healthcare 12, no. 3: 300. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12030300