The Effects of Long-Term 40-Hz Physioacoustic Vibrations on Motor Impairments in Parkinson’s Disease: A Double-Blinded Randomized Control Trial


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
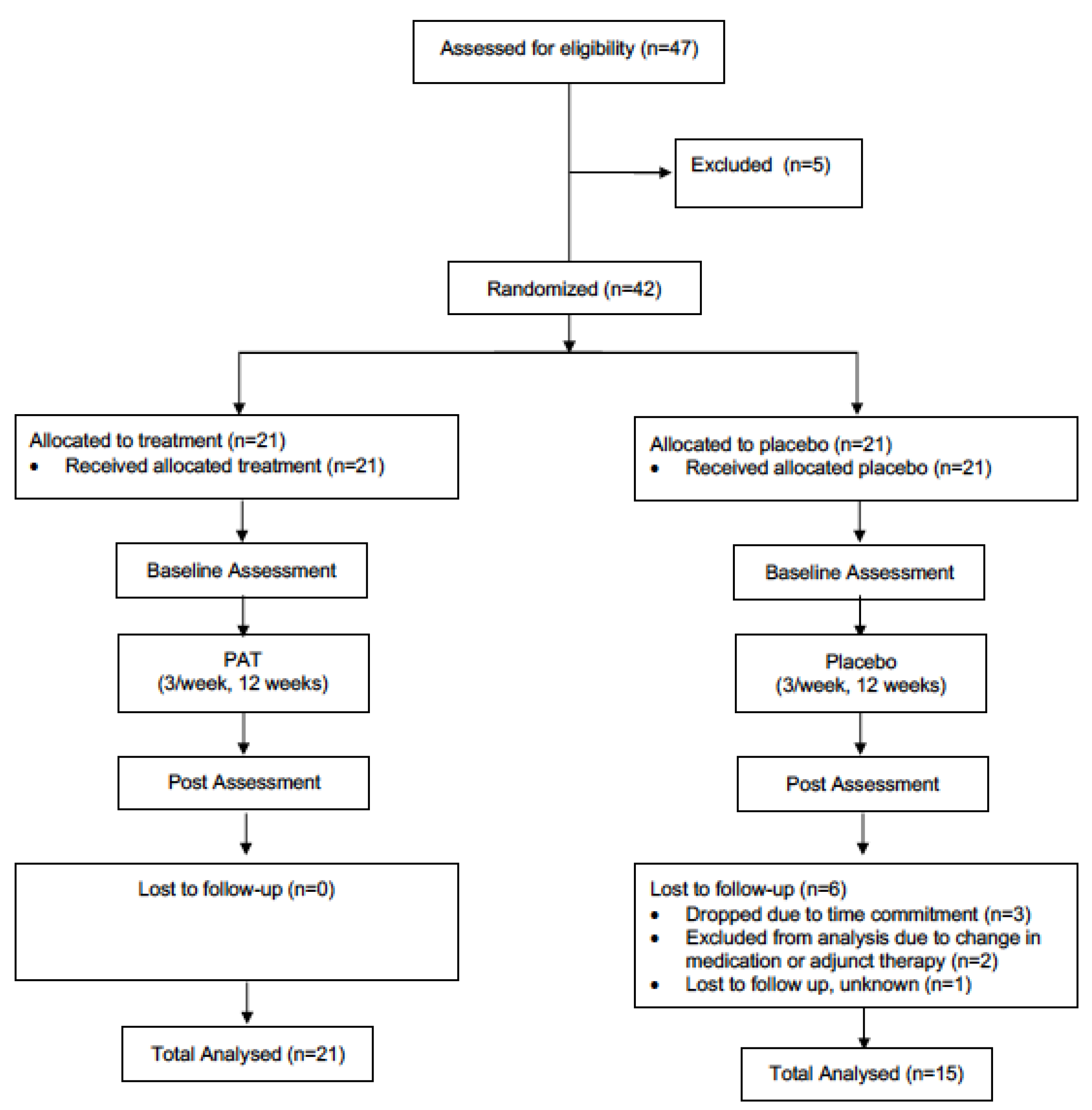
2.1. Participants
2.2. Experimental Design/Procedure
2.3. Treatments
2.4. Assessments
2.5. Statistical Analysis
3. Results
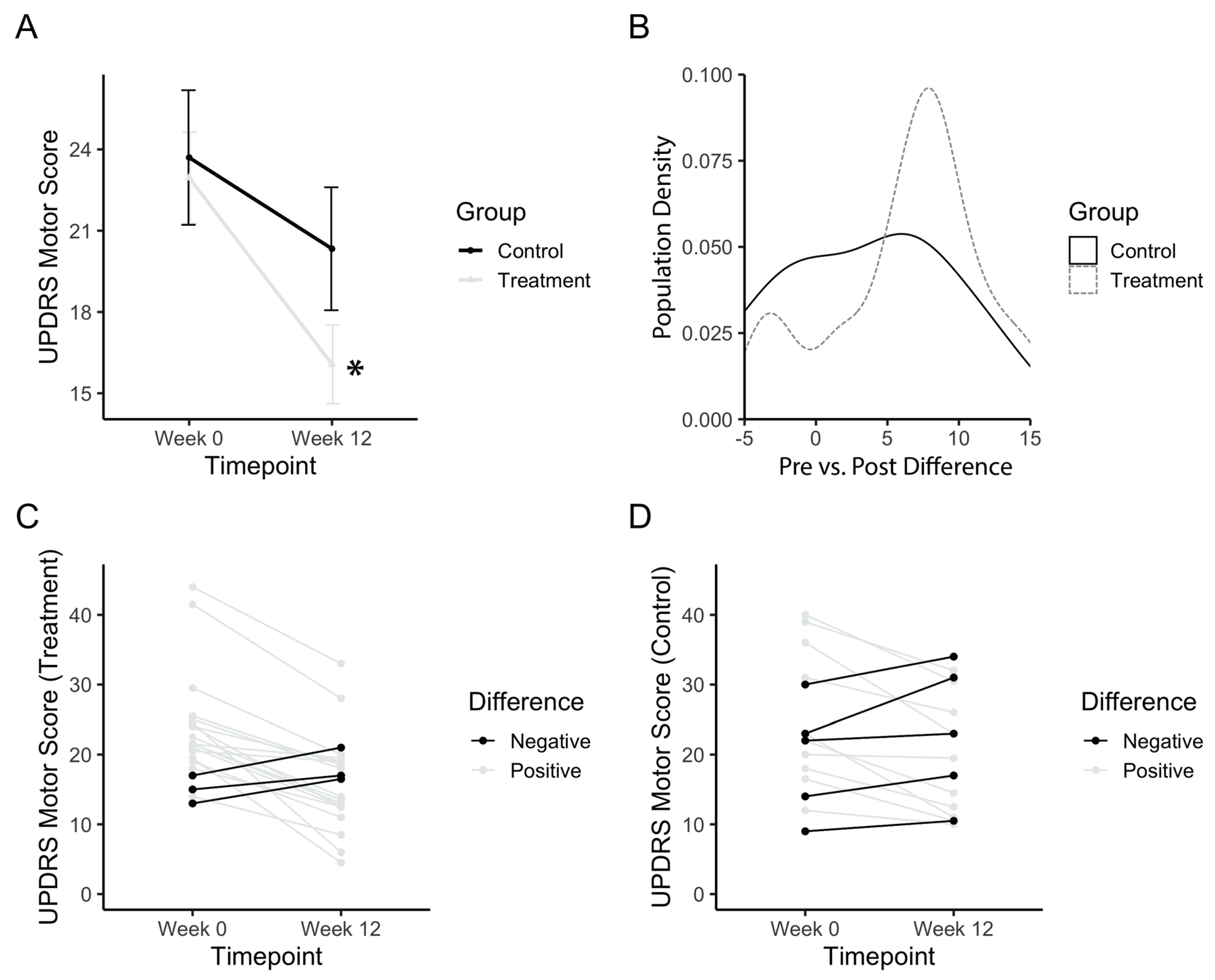
3.1. UPDRS Motor Score at Baseline and Post PAT
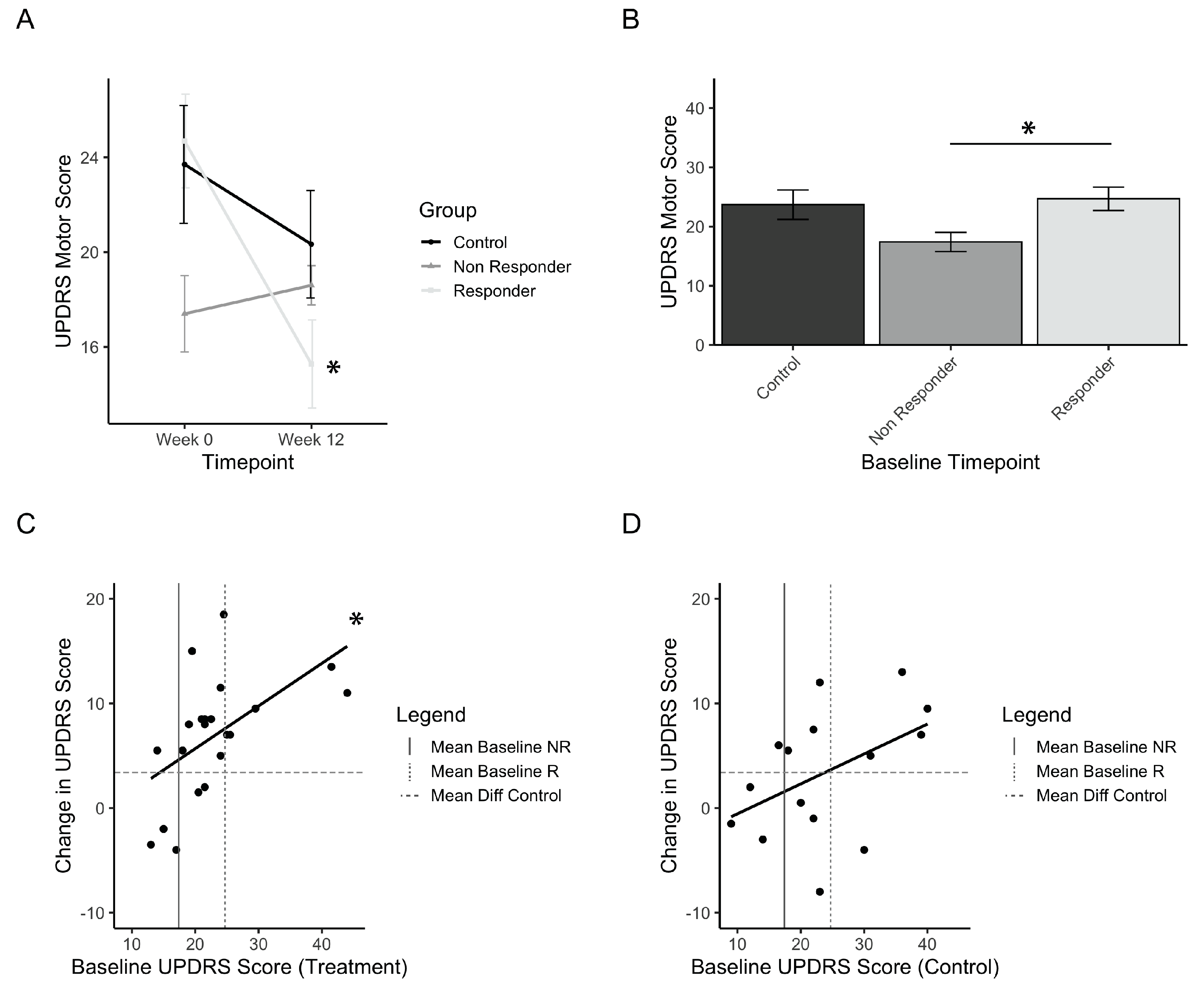
3.2. Treatment Responders to PAT
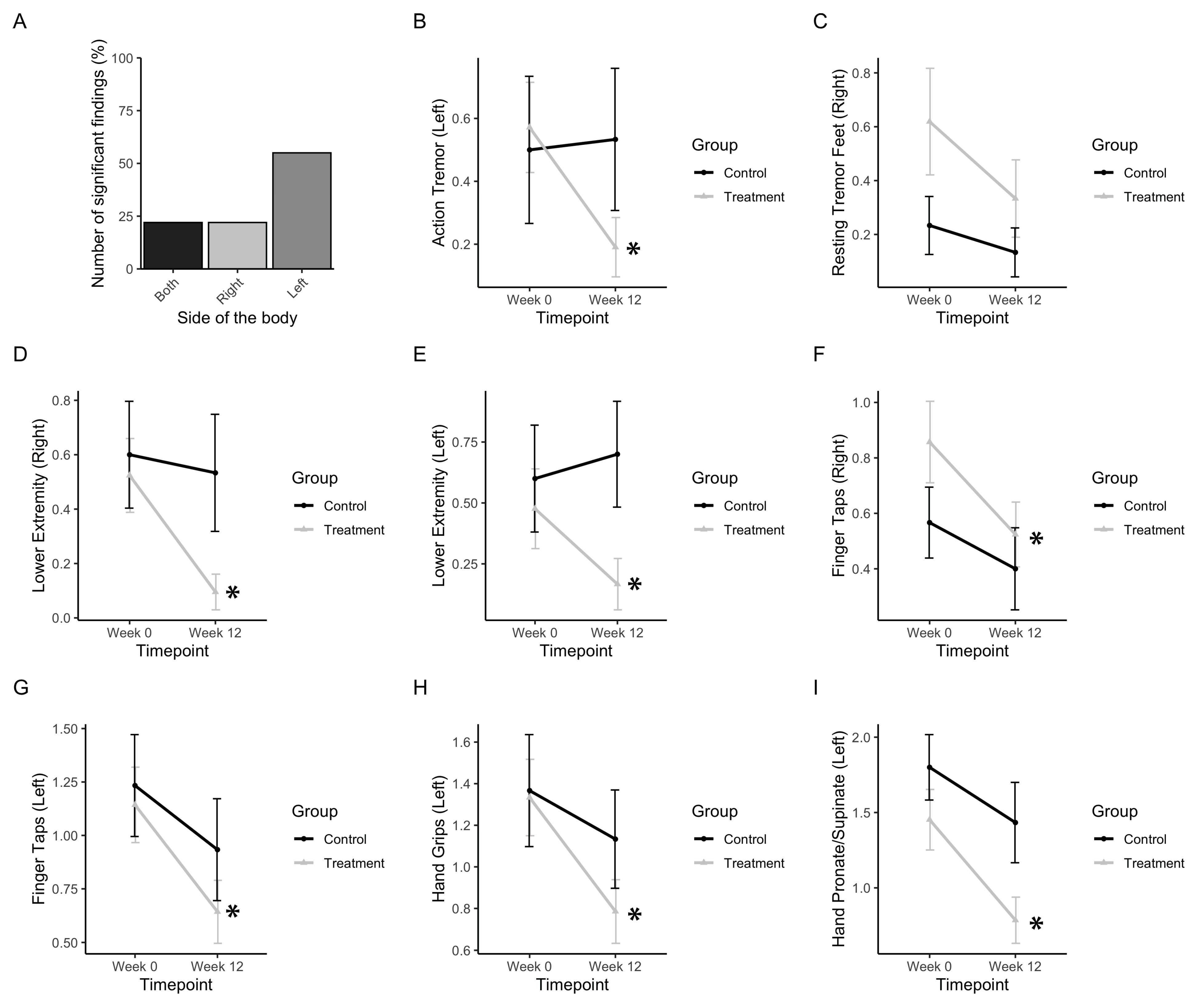
3.3. Tremor, Rigidity, and Fine Motor Movements
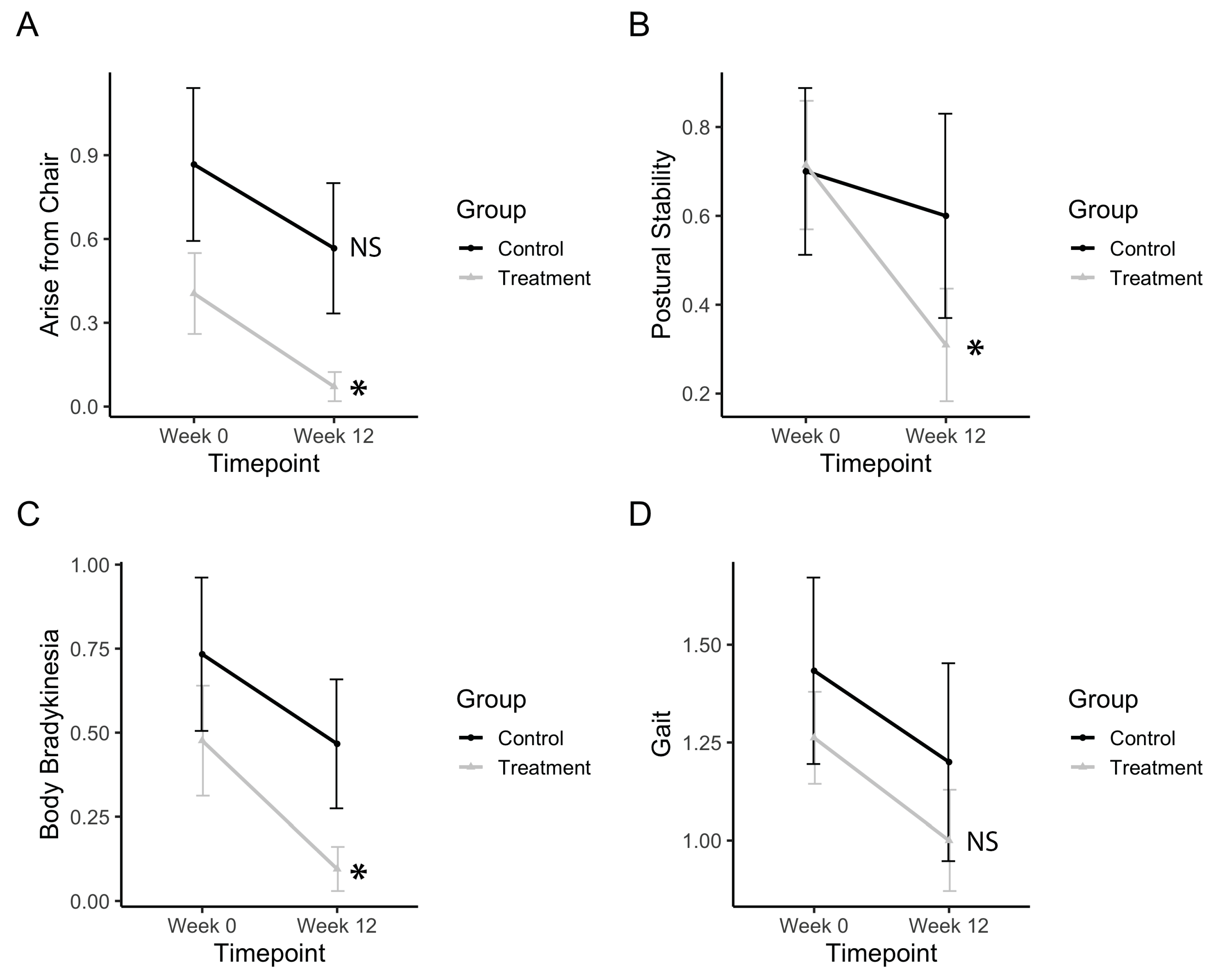
3.4. Bradykinesia, Postural Stability, and Gross Motor Movements
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marsden, C.D. Problems with long-term levodopa therapy for Parkinson’s disease. Clin Neuropharmacol. 1994, 2, S32–S44. [Google Scholar] [CrossRef]
- Rao, S.S.; Hofmann, L.A.; Shakil, A. Parkinson’s disease: Diagnosis and treatment. Am. Fam. Physician 2006, 74, 2046–2054. [Google Scholar] [PubMed]
- Haas, C.T.; Turbanski, S.; Kessler, K.; Schmidtbleicher, D. The effects of random whole-body-vibration on motor symptoms in Parkinson’s disease. NeuroRehabilitation 2006, 21, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, L.K.; Almeida, Q.J.; Ahonen, H. Short-term effects of vibration therapy on motor impairments in Parkinson’s disease. NeuroRehabilitation 2009, 25, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, S.; Kiper, P.; Palmer, K.; Agostini, M.; Turolla, A. Effects of vibratory stimulation on balance and gait in Parkinson’s disease: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2020. [Google Scholar] [CrossRef]
- Dostrovsky, J.; Bergman, H. Oscillatory activity in the basal ganglia-relationship to normal physiology and pathophysiology. Brain 2004, 127, 721–722. [Google Scholar] [CrossRef] [Green Version]
- Hammond, C.; Bergman, H.; Brown, P. Pathological synchronization in Parkinson’s disease: Networks, models and treatments. Trends Neurosci. 2007, 30, 357–364. [Google Scholar] [CrossRef]
- Schnitzler, A.; Gross, J. Normal and pathological oscillatory communication in the brain. Nat. Rev. Neurosci. 2005, 6, 285–296. [Google Scholar] [CrossRef]
- Levy, R.; Ashby, P.; Hutchison, W.D.; Lang, A.E.; Lozano, A.M.; Dostrovsky, J.O. Dependence of subthalamic nucleus oscillations on movement and dopamine in Parkinson’s disease. Brain 2002, 125, 1196–1209. [Google Scholar] [CrossRef]
- Sarnthein, J.; Jeanmonod, D. High thalamocortical theta coherence in patients with Parkinson’s disease. J. Neurosci. 2007, 27, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Brown, P. Oscillatory nature of human basal ganglia activity: Relationship to the pathophysiology of parkinson’s disease. Mov. Disord. 2003, 18, 357–363. [Google Scholar] [CrossRef]
- Crowell, A.L.; Ryapolova-Webb, E.S.; Ostrem, J.L.; Galifianakis, N.B.; Shimamoto, S.; Lim, D.A.; Starr, P.A. Oscillations in sensorimotor cortex in movement disorders: An electrocorticography study. Brain 2012, 135, 615–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.; Oliviero, A.; Mazzone, P.; Insola, A.; Tonali, P.; Di Lazzaro, V. Dopamine dependency of oscillations between subthalamic nucleus and pallidum in Parkinson’s disease. J. Neurosci. 2001, 21, 1033–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronte-Stewart, H.; Barberini, C.; Koop, M.M.; Hill, B.C.; Henderson, J.M.; Wingeier, B. The STN beta-band profile in Parkinson’s disease is stationary and shows prolonged attenuation after deep brain stimulation. Exp. Neurol. 2009, 215, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Kühn, A.A.; Kempf, F.; Brücke, C.; Doyle, L.G.; Martinez-Torres, I.; Pogosyan, A.; Trottenberg, T.; Kupsch, A.; Schneider, G.H.; Hariz, M.I.; et al. High-frequency stimulation of the subthalamic nucleus suppresses oscillatory β activity in patients with Parkinson’s disease in parallel with improvement in motor performance. J. Neurosci. 2008, 28, 6165–6173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thut, G.; Schyns, P.G.; Gross, J. Entrainment of perceptually relevant brain oscillations by non-invasive rhythmic stimulation of the human brain. Front. Psychol. 2011, 2, 170. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.Z. Steady-state vibration evoked potentials: Description of technique and characterization of responses. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1992, 84, 257–268. [Google Scholar] [CrossRef]
- Tobimatsu, S.; Zhang, Y.M.; Suga, R.; Kato, M. Differential temporal coding of the vibratory sense in the hand and foot in man. Clin. Neurophysiol. 2000, 111, 398–404. [Google Scholar] [CrossRef]
- Nakamura, H.; Moroji, T.; Nohara, S.; Nakamura, H.; Okada, A. Activation of cerebral dopaminergic systems by noise and whole-body vibration. Environ. Res. 1992, 57, 10–18. [Google Scholar] [CrossRef]
- Zhao, L.; He, L.X.; Huang, S.N.; Gong, L.J.; Li, L.; Lv, Y.Y.; Qian, Z.M. Protection of dopamine neurons by vibration training and up-regulation of brain-derived neurotrophic factor in a MPTP mouse model of Parkinson’s disease. Physiol. Res. 2014, 63, 649–657. [Google Scholar]
- Jöbges, E.M.; Elek, J.; Rollnik, J.D.; Dengler, R.; Wolf, W. Vibratory proprioceptive stimulation affects Parkinsonian tremor. Parkinsonism Relat. Disord. 2002, 8, 171–176. [Google Scholar] [CrossRef]
- Vincente, P.; Manchola, I.; Serna, E. The use of vibroacoustics in idiopathic Parkinson’s Disease. In Music Vibration and Health; Wigram, T., Dileo, C., Eds.; Jeffrey Books: Cherry Hill, NJ, USA, 1997. [Google Scholar]
- Skille, O.; Wigram, T.; Weekes, L. Vibroacoustic Therapy: The therapeutic effect of low frequency sound on specific physical disorders and disabilities. J. Br. Music Ther. 1989, 3, 6–10. [Google Scholar] [CrossRef]
- Next Wave Physioacoustic MX Therapy Chair|Next Wave World Wide. Available online: http://www.nextwaveworldwide.com/products/physioacoustic-mx-therapy-chair/ (accessed on 9 March 2020).
- Fischer, M.; Vialleron, T.; Laffaye, G.; Fourcade, P.; Hussein, T.; Chèze, L.; Deleu, P.-A.; Honeine, J.-L.; Yiou, E.; Delafontaine, A. Long-term effects of whole-body vibration on human gait: A systematic review and meta-analysis. Front. Neurol. 2019, 10, 627. [Google Scholar] [CrossRef]
- Piecha, M.; Juras, G.; Król, P.; Sobota, G.; Polak, A.; Bacik, B. The effect of a short-term and long-term whole-body vibration in healthy men upon the postural stability. PLoS ONE 2014, 9, e88295. [Google Scholar] [CrossRef] [PubMed]
- Dincher, A.; Schwarz, M.; Wydra, G. Analysis of the effects of whole-body vibration in parkinson disease—Systematic review and meta-analysis. PM&R 2019, 11, 640–653. [Google Scholar]
- McDermott, B.; Porter, E.; Hughes, D.; McGinley, B.; Lang, M.; O’Halloran, M.; Jones, M. Gamma band neural stimulation in humans and the promise of a new modality to prevent and treat Alzheimer’s Disease. J. Alzheimers. Dis. 2018, 65, 363–392. [Google Scholar] [CrossRef] [Green Version]
- Iaccarino, H.F.; Singer, A.C.; Martorell, A.J.; Rudenko, A.; Gao, F.; Gillingham, T.Z.; Mathys, H.; Seo, J.; Kritskiy, O.; Abdurrob, F.; et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature 2016, 540, 230–235. [Google Scholar] [CrossRef] [Green Version]
- Adaikkan, C.; Middleton, S.J.; Marco, A.; Pao, P.C.; Mathys, H.; Kim, D.N.W.; Gao, F.; Young, J.Z.; Suk, H.J.; Boyden, E.S.; et al. Gamma entrainment binds higher-order brain regions and offers neuroprotection. Neuron 2019, 102, 929–943.e8. [Google Scholar] [CrossRef]
- Bartel, L.R.; Chen, R.; Alain, C.; Ross, B. Vibroacoustic stimulation and brain oscillation: From basic research to clinical application. Music Med. 2017, 9, 153–166. [Google Scholar]
- Fish, J. Unified Parkinson’s Disease rating scale. In Encyclopedia of Clinical Neuropsychology; Springer: New York, NY, USA, 2011; pp. 2576–2577. [Google Scholar]
- Giabbiconi, C.M.; Trujillo-Barreto, N.J.; Gruber, T.; Müller, M.M. Sustained spatial attention to vibration is mediated in primary somatosensory cortex. Neuroimage 2007, 35, 255–262. [Google Scholar] [CrossRef]
- PKMAS—ProtoKinetics Movement Analysis Software » ProtoKinetics. Available online: https://www.protokinetics.com/pkmas/ (accessed on 2 April 2020).
- Schrag, A.; Sampaio, C.; Counsell, N.; Poewe, W. Minimal clinically important change on the Unified Parkinson’s Disease rating scale. Mov. Disord. 2006, 21, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Horváth, K.; Aschermann, Z.; Ács, P.; Deli, G.; Janszky, J.; Komoly, S.; Balázs, É.; Takács, K.; Karádi, K.; Kovács, N. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Park. Relat. Disord. 2015, 21, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M.; Gruber-Baldini, A.L.; Anderson, K.E.; Fishman, P.S.; Reich, S.G.; Weiner, W.J. The clinically important difference on the unified parkinson’s disease rating scale. Arch. Neurol. 2010, 67, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Sharififar, S.; Coronado, R.A.; Romero, S.; Azari, H.; Thigpen, M. The effects of whole body vibration on mobility and balance in Parkinson disease: A systematic review. Iran. J. Med. Sci. 2014, 39, 318–326. [Google Scholar] [PubMed]
- Kiiski, J.; Heinonen, A.; Järvinen, T.L.; Kannus, P.; Sievänen, H. Transmission of vertical whole body vibration to the human body. J. Bone Miner. Res. 2008, 23, 1318–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fratini, A.; La Gatta, A.; Bifulco, P.; Romano, M.; Cesarelli, M. Muscle motion and EMG activity in vibration treatment. Med. Eng. Phys. 2009, 31, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.M.; Deane, K.H.O.; Wheatley, K.; et al. Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Reif, M.; Field, T.; Largie, S.; Cullen, C.; Beutler, J.; Sanders, C.; Weiner, W.; Rodriguez-Bateman, D.; Zelaya, L.; Schanber, S.; et al. Parkinson’s disease symptoms are differentially affected by massage therapy vs. progressive muscle relaxation: A pilot study. J. Bodyw. Mov. Ther. 2002, 6, 177–182. [Google Scholar] [CrossRef]
- Casciaro, Y. Massage therapy treatment and outcomes for a patient with parkinson’s disease: A case report. Int. J. Ther. Massage Bodyw. Res. Educ. Pract. 2016, 9, 11–18. [Google Scholar]
- Paterson, C.; Allen, J.A.; Browning, M.; Barlow, G.; Ewings, P. A pilot study of therapeutic massage for people with Parkinson’s disease: The added value of user involvement ARTICLE IN PRESS. Complement. Ther. Clin. Pract. 2005, 11, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.T.; Buhlmann, A.; Turbanski, S.; Schmidtbleicher, D. Proprioceptive and sensorimotor performance in Parkinson’s disease. Res. Sports Med. 2006, 14, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Hannah, R.; Minshull, C.; Folland, J.P. Whole-body vibration does not influence knee joint neuromuscular function or proprioception. Scand. J. Med. Sci. Sports 2013, 23, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Lau, R.W.K.; Teo, T.; Yu, F.; Chung, R.C.K.; Pang, M.Y.C. Effects of whole-body vibration on sensorimotor performance in people with parkinson disease: A systematic review. Phys. Ther. 2011, 91, 198–209. [Google Scholar] [CrossRef] [Green Version]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosabbir, A.; Almeida, Q.J.; Ahonen, H. The Effects of Long-Term 40-Hz Physioacoustic Vibrations on Motor Impairments in Parkinson’s Disease: A Double-Blinded Randomized Control Trial. Healthcare 2020, 8, 113. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8020113
Mosabbir A, Almeida QJ, Ahonen H. The Effects of Long-Term 40-Hz Physioacoustic Vibrations on Motor Impairments in Parkinson’s Disease: A Double-Blinded Randomized Control Trial. Healthcare. 2020; 8(2):113. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8020113
Chicago/Turabian StyleMosabbir, Abdullah, Quincy J. Almeida, and Heidi Ahonen. 2020. "The Effects of Long-Term 40-Hz Physioacoustic Vibrations on Motor Impairments in Parkinson’s Disease: A Double-Blinded Randomized Control Trial" Healthcare 8, no. 2: 113. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8020113