The Effect of Spinal Manipulation on the Electrophysiological and Metabolic Properties of the Tibialis Anterior Muscle

 ,
,  , ,
, ,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Design and Setting
2.2. Participants
2.3. Sample Size
2.4. Randomization and Blinding
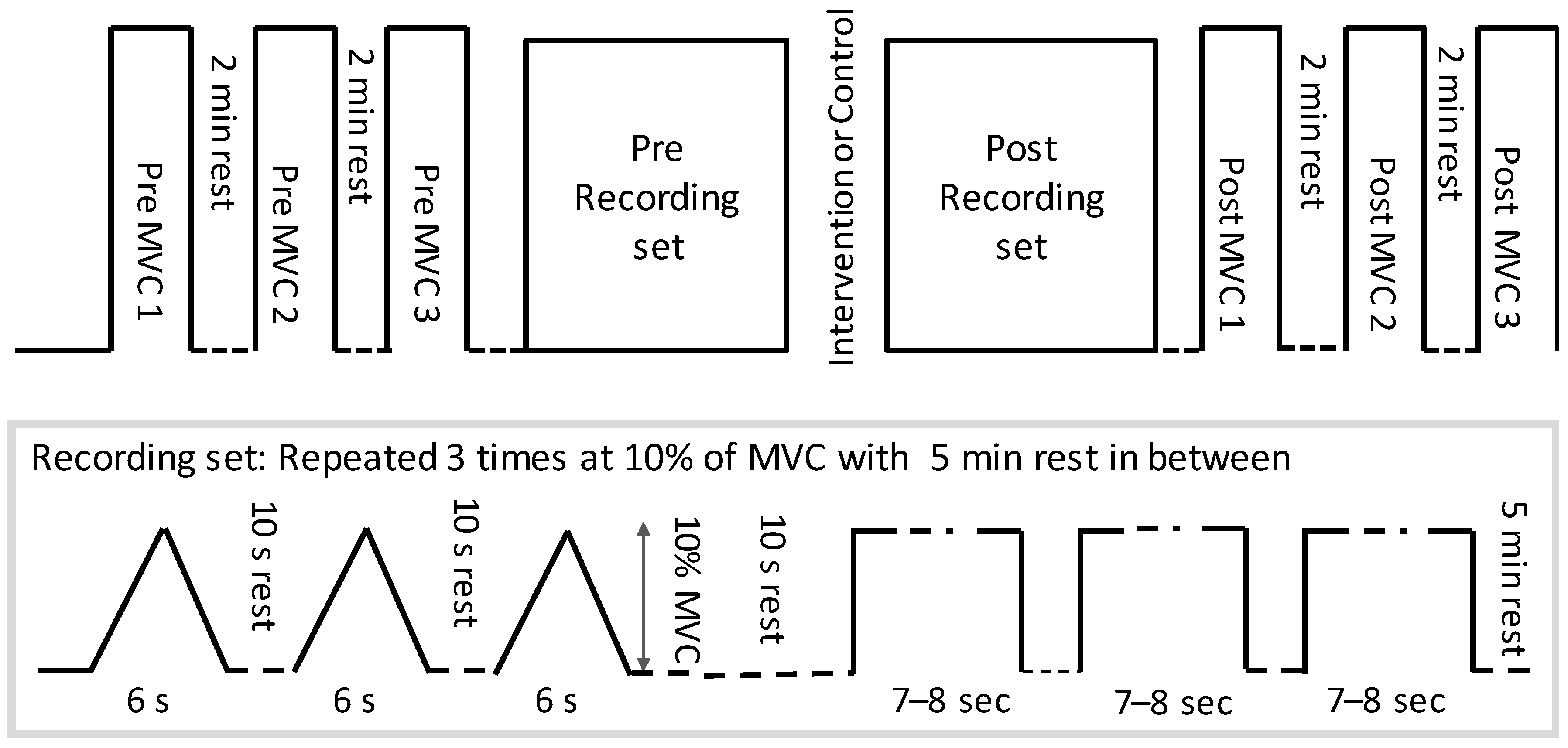
2.5. Experimental Procedure
2.6. Interventions
2.6.1. Spinal Manipulation
2.6.2. Control Intervention
2.7. Outcome Measures
2.7.1. Intramuscular and High-Density EMG Experimental Procedure (Including MVC’s)
2.7.2. Near-Infrared Spectroscopy Experimental Procedure (Including MVC’s)
2.8. Data Analysis
2.8.1. Conduction Velocity with High-Density EMG
2.8.2. Intramuscular EMG
2.8.3. NIRS Signals
2.9. Statistical Analysis
3. Results
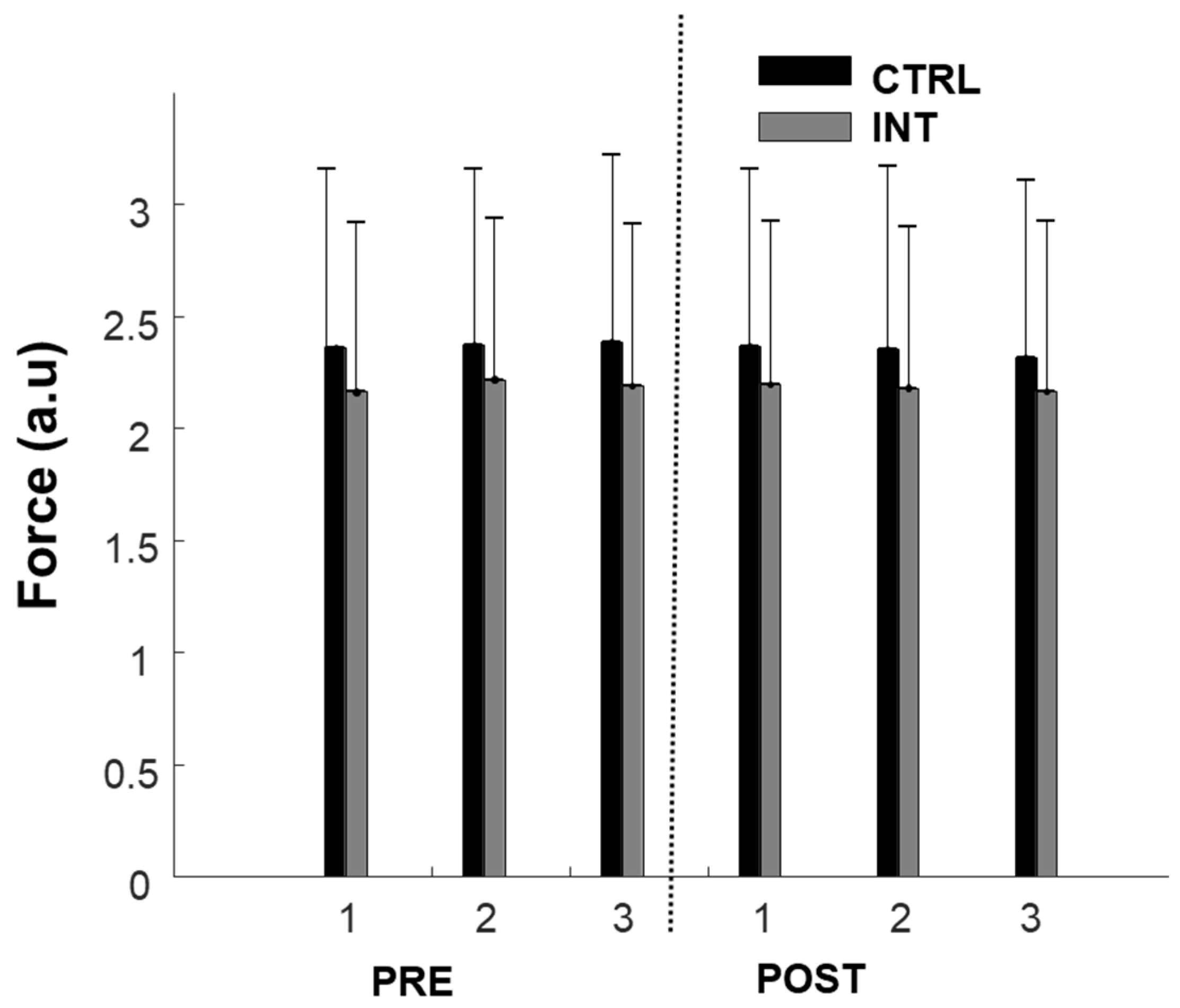
3.1. MVC
3.2. Discharge Rate/Firing Frequency (Intramuscular EMG)
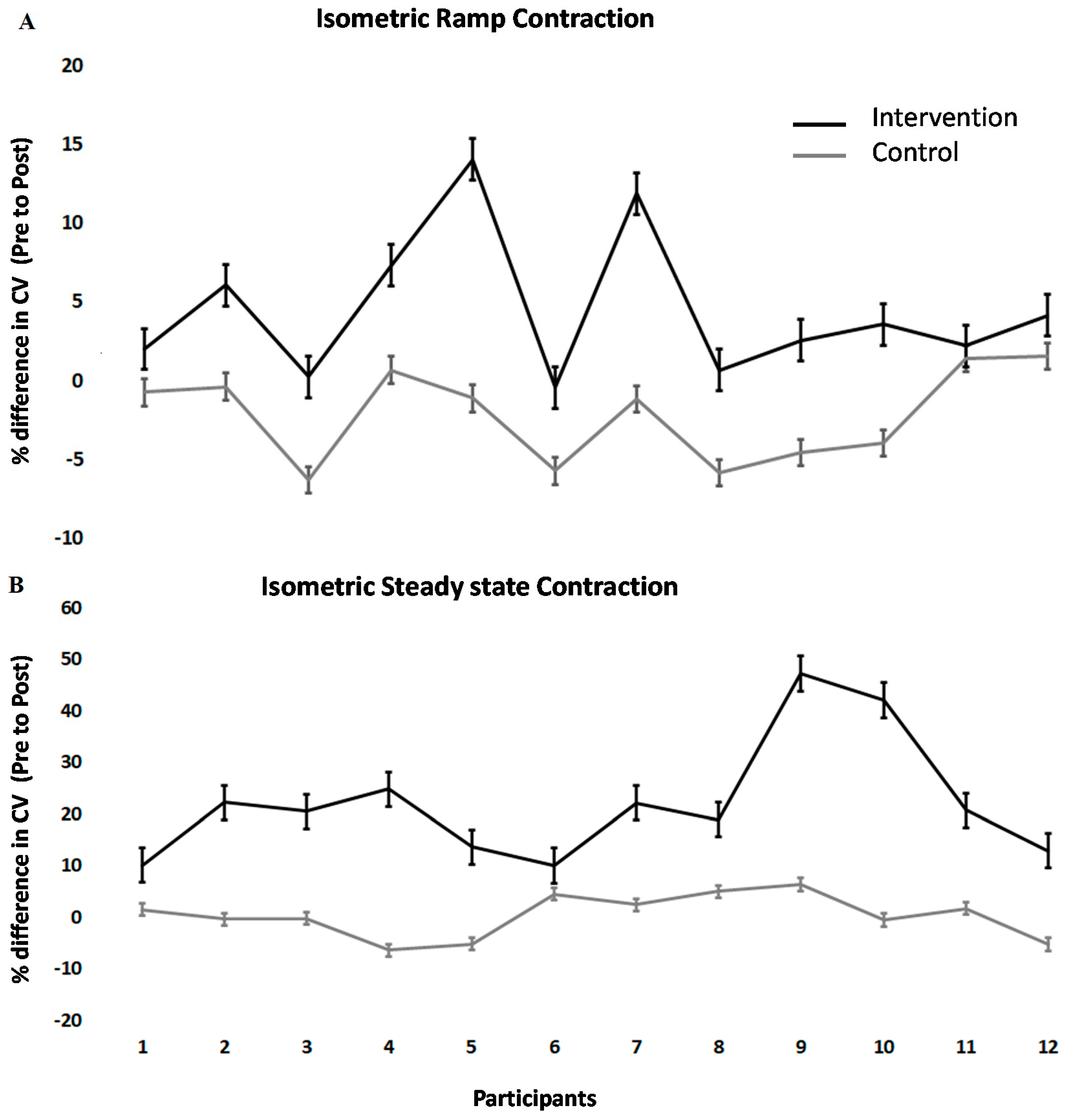
3.3. Conduction Velocity (HDsEMG)
3.4. Metabolic Properties
4. Discussion
4.1. Chiropractic Adjustments Alter Muscle Strength
4.2. Electrophysiological and Metabolic Changes
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jenkins, H.J.; Downie, A.S.; Moore, C.S.; French, S.D. Current evidence for spinal X-ray use in the chiropractic profession: A narrative review. Chiropr. Man. Ther. 2018, 26, 48. [Google Scholar] [CrossRef] [Green Version]
- McGill, S.M. Stability: From biomechanical concept to chiropractic practice. J. Can. Chiropr. Assoc. 1999, 43, 75. [Google Scholar]
- Gross, A.; Langevin, P.; Burnie, S.J.; Bédard-Brochu, M.S.; Empey, B.; Dugas, E.; Faber-Dobrescu, M.; Andres, C.; Graham, N.; Goldsmith, C.H.; et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Miller, J.; D’Sylva, J.; Burnie, S.J.; Goldsmith, C.H.; Graham, N.; Haines, T.; Brønfort, G.; Hoving, J.L. Manipulation or mobilisation for neck pain: A Cochrane Review. Man. Ther. 2010, 15, 315–333. [Google Scholar] [CrossRef] [PubMed]
- Bryans, R.; Decina, P.; Descarreaux, M.; Duranleau, M.; Marcoux, H.; Potter, B.; Ruegg, R.P.; Shaw, L.; Watkin, R.; White, E. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J. Manip. Physiol. Ther. 2014, 37, 42–63. [Google Scholar] [CrossRef] [PubMed]
- Goertz, C.M.; Pohlman, K.A.; Vining, R.D.; Brantingham, J.W.; Long, C.R. Patient-centered outcomes of high-velocity, low-amplitude spinal manipulation for low back pain: A systematic review. J. Electromyogr. Kinesiol. 2012, 22, 670–691. [Google Scholar] [CrossRef] [PubMed]
- Ruddock, J.K.; Sallis, H.; Ness, A.; Perry, R.E. Spinal Manipulation vs. Sham Manipulation for Nonspecific Low Back Pain: A Systematic Review and Meta-analysis. J. Chiropr. Med. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryans, R.; Descarreaux, M.; Duranleau, M.; Marcoux, H.; Potter, B.; Ruegg, R.; Shaw, L.; Watkin, R.; White, E. Evidence-based guidelines for the chiropractic treatment of adults with headache. J. Manip. Physiol. Ther. 2011, 34, 274–289. [Google Scholar] [CrossRef]
- Haavik, H.; Murphy, B. The role of spinal manipulation in addressing disordered sensorimotor integration and altered motor control. J. Electromyogr. Kinesiol. 2012, 22, 768–776. [Google Scholar] [CrossRef]
- Christiansen, T.L.; Niazi, I.K.; Holt, K.; Nedergaard, R.W.; Duehr, J.; Allen, K.; Marshall, P.; Türker, K.S.; Hartvigsen, J.; Haavik, H. The effects of a single session of spinal manipulation on strength and cortical drive in athletes. Eur. J. Appl. Physiol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Holt, K.; Niazi, I.K.; Nedergaard, R.W.; Duehr, J.; Amjad, I.; Shafique, M.; Anwar, M.N.; Ndetan, H.; Turker, K.S.; Haavik, H. The effects of a single session of chiropractic care on strength, cortical drive, and spinal excitability in stroke patients. Sci. Rep. 2019, 9, 2637. [Google Scholar] [CrossRef] [PubMed]
- Haavik, H.; Murphy, B. Subclinical neck pain and the effects of cervical manipulation on elbow joint position sense. J. Manipulative Physiol. Ther. 2011, 34, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Holt, K.R.; Haavik, H.; Lee, A.C.L.; Murphy, B.; Elley, C.R. Effectiveness of Chiropractic Care to Improve Sensorimotor Function Associated with Falls Risk in Older People: A Randomized Controlled Trial. J. Manipulative Physiol. Ther. 2016, 39, 267–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Rubicon Group Definition and Position Statement on the Chiropractic Subluxation. 2017. Available online: http://www.therubicongroup.org/#/policies/ (accessed on 10 October 2020).
- Niazi, I.K.; Türker, K.S.; Flavel, S.; Kinget, M.; Duehr, J.; Haavik, H. Changes in H-reflex and V-waves following spinal manipulation. Exp. Brain Res. 2015, 233, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Daligadu, J.; Haavik, H.; Yielder, P.C.; Baarbe, J.; Murphy, B. Alterations in cortical and cerebellar motor processing in subclinical neck pain patients following spinal manipulation. J. Manipulative Physiol. Ther. 2013, 36, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Haavik, H.; Niazi, I.K.; Jochumsen, M.; Sherwin, D.; Flavel, S.; Türker, K.S. Impact of spinal manipulation on cortical drive to upper and lower limb muscles. Brain Sci. 2017, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Haavik, H.; Niazi, I.K.; Jochumsen, M.; Uginčius, P.; Sebik, O.; Yılmaz, G.; Navid, M.S.; Özyurt, M.G.; Türker, K.S. Chiropractic spinal manipulation alters TMS induced I-wave excitability and shortens the cortical silent period. J. Electromyogr. Kinesiol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Haavik-Taylor, H.; Murphy, B. Cervical spine manipulation alters sensorimotor integration: A somatosensory evoked potential study. Clin. Neurophysiol. 2007. [Google Scholar] [CrossRef]
- Taylor, H.H.; Murphy, B. Altered Sensorimotor Integration with Cervical Spine Manipulation. J. Manipulative Physiol. Ther. 2008, 31, 115–126. [Google Scholar] [CrossRef]
- Taylor, H.H.; Murphy, B. Altered Central Integration of Dual Somatosensory Input After Cervical Spine Manipulation. J. Manipulative Physiol. Ther. 2010, 33, 178–188. [Google Scholar] [CrossRef]
- Taylor, H.H.; Murphy, B. The Effects of Spinal Manipulation on Central Integration of Dual Somatosensory Input Observed After Motor Training: A Crossover Study. J. Manipulative Physiol. Ther. 2010, 33, 261–272. [Google Scholar] [CrossRef]
- Lelic, D.; Niazi, I.K.; Holt, K.; Jochumsen, M.; Dremstrup, K.; Yielder, P.; Murphy, B.; Drewes, A.M.; Haavik, H. Manipulation of dysfunctional spinal joints affects sensorimotor integration in the prefrontal cortex: A brain source localization study. Neural Plast. 2016, 2016, 3704964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navid, M.S.; Lelic, D.; Niazi, I.K.; Holt, K.; Mark, E.B.; Drewes, A.M.; Haavik, H. The effects of chiropractic spinal manipulation on central processing of tonic pain—A pilot study using standardized low-resolution brain electromagnetic tomography (sLORETA). Sci. Rep. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haavik, H.; Murphy, B.A. Transient modulation of intracortical inhibition following spinal manipulation. Chiropr. J. Aust. 2007, 37, 106–116. [Google Scholar]
- Allison, T.; McCarthy, G.; Wood, C.C.; Darcey, T.M.; Spencer, D.D.; Williamson, P.D. Human cortical potentials evoked by stimulation of the median nerve. II. Cytoarchitectonic areas generating short-latency activity. J. Neurophysiol. 1989, 62, 694–710. [Google Scholar] [CrossRef]
- Allison, T.; McCarthy, G.; Wood, C.C.; Williamson, P.D.; Spencer, D.D. Human cortical potentials evoked by stimulation of the median nerve. II. Cytoarchitectonic areas generating long-latency activity. J. Neurophysiol. 1989. [Google Scholar] [CrossRef]
- Waberski, T.D.; Buchner, H.; Perkuhn, M.; Gobbelé, R.; Wagner, M.; Kücker, W.; Silny, J. N30 and the effect of explorative finger movements: A model of the contribution of the motor cortex to early somatosensory potentials. Clin. Neurophysiol. 1999, 110, 1589–1600. [Google Scholar] [CrossRef]
- Kaňovský, P.; Bareš, M.; Rektor, I. The selective gating of the N30 cortical component of the somatosensory evoked potentials of median nerve is different in the mesial and dorsolateral frontal cortex: Evidence from intracerebral recordings. Clin. Neurophysiol. 2003, 114, 981–991. [Google Scholar] [CrossRef]
- Allison, T.; Mccarthy, G.; Wood, C.C.; Jones, S.J. Potentials evoked in human and monkey cerebral cortex by stimulation of the median nerve: A review of scalp and intracranial recordings. Brain 1991. [Google Scholar] [CrossRef]
- Desmedt, J.E.; Cheron, G. Non-cephalic reference recording of early somatosensory potentials to finger stimulation in adult or aging normal: Differentiation of widespread N18 and contralateral N20 from the prerolandic p22 and N30 components. Electroencephalogr. Clin. Neurophysiol. 1981. [Google Scholar] [CrossRef]
- Desmedt, J.E.; Huy, N.T.; Bourguet, M. The cognitive P40, N60 and P100 components of somatosensory evoked potentials and the earliest electrical signs of sensory processing in man. Electroencephalogr. Clin. Neurophysiol. 1983. [Google Scholar] [CrossRef]
- Mauguière, F.; Desmedt, J.E.; Courjon, J. Astereognosis and dissociated loss of frontal or parietal components of somatosensory evoked potentials in hemispheric lesions: Detailed correlations with clinical signs and computerized tomographic scanning. Brain 1983, 106, 271–311. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Babiloni, F.; Bernardi, G.; Cecchi, L.; Johnson, P.B.; Malentacca, A.; Stanzione, P.; Urbano, A. Abnormalities of short-latency somatosensory evoked potentials in parkinsonian patients. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1989, 74, 277–289. [Google Scholar] [CrossRef]
- Rossini, P.M.; Gigli, G.L.; Marciani, M.G.; Zarola, F.; Caramia, M. Non-invasive evaluation of input-output characteristics of sensorimotor cerebral areas in healthy humans. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1987, 68, 88–100. [Google Scholar] [CrossRef]
- Cheron, G.; Borenstein, S. Gating of the early components of the frontal and parietal somatosensory evoked potentials in different sensory-motor interference modalities. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1991. [Google Scholar] [CrossRef]
- Cheron, G.; Borenstein, S. Mental movement simulation affects the N30 frontal component of the somatosensory evoked potential. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1992. [Google Scholar] [CrossRef]
- Rossi, S.; Della Volpe, R.; Ginanneschi, F.; Ulivelli, M.; Bartalini, S.; Spidalieri, R.; Rossi, A. Early somatosensory processing during tonic muscle pain in humans: Relation to loss of proprioception and motor “defensive” strategies. Clin. Neurophysiol. 2003, 114, 1351–1358. [Google Scholar] [CrossRef]
- Duchateau, J.; Semmler, J.G.; Enoka, R.M. Training adaptations in the behavior of human motor units. J. Appl. Physiol. 2006. [Google Scholar] [CrossRef] [Green Version]
- Folland, J.P.; Williams, A.G. The adaptations to strength training: Morphological and neurological contributions to increased strength. Sports Med. 2007, 37, 145–168. [Google Scholar] [CrossRef]
- Kidgell, D.J.; Bonanno, D.R.; Frazer, A.K.; Howatson, G.; Pearce, A.J. Corticospinal responses following strength training: A systematic review and meta-analysis. Eur. J. Neurosci. 2017, 46, 2648–2661. [Google Scholar] [CrossRef]
- Narici, M.V.; Hoppeler, H.; Kayser, B.; Landoni, L.; Claassen, H.; Gavardi, C.; Conti, M.; Cerretelli, P. Human quadriceps cross-sectional area, torque and neural activation during 6 months strength training. Acta Physiol. Scand. 1996. [Google Scholar] [CrossRef] [PubMed]
- Gandevia, S.C. Spinal and supraspinal factors in human muscle fatigue. Physiol. Rev. 2001. [Google Scholar] [CrossRef] [PubMed]
- Vila-Chã, C.; Falla, D.; Correia, M.V.; Farina, D. Adjustments in motor unit properties during fatiguing contractions after training. Med. Sci. Sports Exerc. 2012. [Google Scholar] [CrossRef] [PubMed]
- Vila-Chã, C.; Falla, D.; Farina, D. Motor unit behavior during submaximal contractions following six weeks of either endurance or strength training. J. Appl. Physiol. 2010. [Google Scholar] [CrossRef] [Green Version]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 2004. [Google Scholar] [CrossRef] [Green Version]
- Methenitis, S.; Karandreas, N.; Spengos, K.; Zaras, N.; Stasinaki, A.N.; Terzis, G. Muscle Fiber Conduction Velocity, Muscle Fiber Composition, and Power Performance. Med. Sci. Sports Exerc. 2016. [Google Scholar] [CrossRef]
- Hargreaves, M.; Spriet, L.L. Skeletal muscle energy metabolism during exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- McCully, K.K.; Hamaoka, T. Near-infrared spectroscopy: What can it tell us about oxygen saturation in skeletal muscle? Exerc. Sport Sci. Rev. 2000, 28, 123–127. [Google Scholar]
- Hamaoka, T.; McCully, K.K.; Niwayama, M.; Chance, B. The use of muscle near-infrared spectroscopy in sport, health and medical sciences: Recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2011, 369, 4591–4604. [Google Scholar] [CrossRef] [Green Version]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016. [Google Scholar] [CrossRef] [Green Version]
- Allen, D.G.; Lamb, G.D.; Westerblad, H. Skeletal Muscle Fatigue: Cellular Mechanisms. Physiol. Rev. 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enoka, R.M.; Duchateau, J. Muscle fatigue: What, why and how it influences muscle function. J. Physiol. 2008, 586, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.J.; Stomski, N.J.; French, S.D.; Rubinstein, S.M. Serious Adverse Events and Spinal Manipulative Therapy of the Low Back Region: A Systematic Review of Cases. J. Manipulative Physiol. Ther. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt, K.; Russell, D.; Cooperstein, R.; Young, M.; Sherson, M.; Haavik, H. Interexaminer reliability of a multidimensional battery of tests used to assess for vertebral subluxations. Chiropr. J. Aust. 2018, 46, 100–117. [Google Scholar]
- Masuda, T.; Miyano, H.; Sadoyama, T. The Position of Innervation Zones in the Biceps Brachii Investigated by Surface Electromyography. IEEE Trans. Biomed. Eng. 1985, BME-32, 36–42. [Google Scholar] [CrossRef]
- Kamavuako, E.N.; Scheme, E.J.; Englehart, K.B. Combined surface and intramuscular EMG for improved real-time myoelectric control performance. Biomed. Signal Process. Control 2014, 10, 102–107. [Google Scholar] [CrossRef]
- Farina, D.; Pozzo, M.; Merlo, E.; Bottin, A.; Merletti, R. Assessment of average muscle fiber conduction velocity from surface EMG signals during fatiguing dynamic contractions. IEEE Trans. Biomed. Eng. 2004. [Google Scholar] [CrossRef] [Green Version]
- McGill, K.C.; Lateva, Z.C.; Marateb, H.R. EMGLAB: An interactive EMG decomposition program. J. Neurosci. Methods 2005, 149, 121–133. [Google Scholar] [CrossRef]
- Ryan, T.E.; Erickson, M.L.; Brizendine, J.T.; Young, H.-J.; McCully, K.K. Noninvasive evaluation of skeletal muscle mitochondrial capacity with near-infrared spectroscopy: Correcting for blood volume changes. J. Appl. Physiol. 2012, 113, 175–183. [Google Scholar] [CrossRef]
- Thomas, P.K.; Sears, T.A.; Gilliatt, R.W. The range of conduction velocity in normal motor nerve fibres to the small muscles of the hand and foot. J. Neurol. Neurosurg. Psychiatry 1959, 22, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Hillermann, B.; Gomes, A.N.; Korporaal, C.; Jackson, D. A pilot study comparing the effects of spinal manipulative therapy with those of extra-spinal manipulative therapy on quadriceps muscle strength. J. Manip. Physiol. Ther. 2006, 29, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Suter, E.; McMorland, G.; Herzog, W.; Bray, R. Decrease in quadriceps inhibition after sacroiliac joint manipulation in patients with anterior knee pain. J. Manip. Physiol. Ther. 1999. [Google Scholar] [CrossRef]
- Haavik, H.; Özyurt, M.G.; Niazi, I.K.; Holt, K.; Nedergaard, R.W.; Yilmaz, G.; Türker, K.S. Chiropractic manipulation increases maximal bite force in healthy individuals. Brain Sci. 2018, 8, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunning, J.; Rushton, A. The effects of cervical high-velocity low-amplitude thrust manipulation on resting electromyographic activity of the biceps brachii muscle. Man. Ther. 2009. [Google Scholar] [CrossRef] [PubMed]
- Keller, T.S.; Colloca, C.J. Mechanical force spinal manipulation increases trunk muscle strength assessed by electromyography: A comparative clinical trial. J. Manipulative Physiol. Ther. 2000. [Google Scholar] [CrossRef] [PubMed]
- Vining, R.; Long, C.R.; Minkalis, A.; Gudavalli, M.R.; Xia, T.; Walter, J.; Coulter, I.; Goertz, C.M. Effects of Chiropractic Care on Strength, Balance, and Endurance in Active-Duty U.S. Military Personnel with Low Back Pain: A Randomized Controlled Trial. J. Altern. Complement. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Duchateau, J.; Baudry, S. Maximal discharge rate of motor units determines the maximal rate of force development during ballistic contractions in human. Front. Hum. Neurosci. 2014, 8. [Google Scholar] [CrossRef] [Green Version]
- Del Vecchio, A.; Casolo, A.; Negro, F.; Scorcelletti, M.; Bazzucchi, I.; Enoka, R.; Felici, F.; Farina, D. The increase in muscle force after 4 weeks of strength training is mediated by adaptations in motor unit recruitment and rate coding. J. Physiol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Del Vecchio, A.; Negro, F.; Holobar, A.; Casolo, A.; Folland, J.P.; Felici, F.; Farina, D. You are as fast as your motor neurons: Speed of recruitment and maximal discharge of motor neurons determine the maximal rate of force development in humans. J. Physiol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Blijham, P.J.; Ter Laak, H.J.; Schelhaas, H.J.; Van Engelen, B.G.M.; Stegeman, D.F.; Zwarts, M.J. Relation between muscle fiber conduction velocity and fiber size in neuromuscular disorders. J. Appl. Physiol. 2006. [Google Scholar] [CrossRef] [Green Version]
- Del Vecchio, A.; Negro, F.; Felici, F.; Farina, D. Associations between motor unit action potential parameters and surface EMG features. J. Appl. Physiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.A. AAEM minimonograph #13: H reflexes and F waves: Physiology and clinical indications. Muscle Nerve 1992, 15, 1223–1233. [Google Scholar] [CrossRef]
- Tucker, K.J.; Tuncer, M.; Türker, K.S. A review of the H-reflex and M-wave in the human triceps surae. Hum. Mov. Sci. 2005. [Google Scholar] [CrossRef] [PubMed]
- Vila-Chã, C.; Falla, D.; Correia, M.V.; Farina, D. Changes in H reflex and V wave following short-term endurance and strength training. J. Appl. Physiol. 2012. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Neural adaptation to resistance training: Changes in evoked V-wave and H-reflex responses. J. Appl. Physiol. 2002. [Google Scholar] [CrossRef]
- Berchicci, M.; Lucci, G.; Di Russo, F. Benefits of physical exercise on the aging brain: The role of the prefrontal cortex. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013. [Google Scholar] [CrossRef] [Green Version]
- Chaibi, A.; Benth, J.Š.; Russell, M.B. Validation of placebo in a manual therapy randomized controlled trial. Sci. Rep. 2015. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niazi, I.K.; Kamavuako, E.N.; Holt, K.; Janjua, T.A.M.; Kumari, N.; Amjad, I.; Haavik, H. The Effect of Spinal Manipulation on the Electrophysiological and Metabolic Properties of the Tibialis Anterior Muscle. Healthcare 2020, 8, 548. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040548
Niazi IK, Kamavuako EN, Holt K, Janjua TAM, Kumari N, Amjad I, Haavik H. The Effect of Spinal Manipulation on the Electrophysiological and Metabolic Properties of the Tibialis Anterior Muscle. Healthcare. 2020; 8(4):548. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040548
Chicago/Turabian StyleNiazi, Imran Khan, Ernest Nlandu Kamavuako, Kelly Holt, Taha Al Muhammadee Janjua, Nitika Kumari, Imran Amjad, and Heidi Haavik. 2020. "The Effect of Spinal Manipulation on the Electrophysiological and Metabolic Properties of the Tibialis Anterior Muscle" Healthcare 8, no. 4: 548. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040548