Barriers to and Facilitators of Adherence to Clinical Practice Guidelines in the Middle East and North Africa Region: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
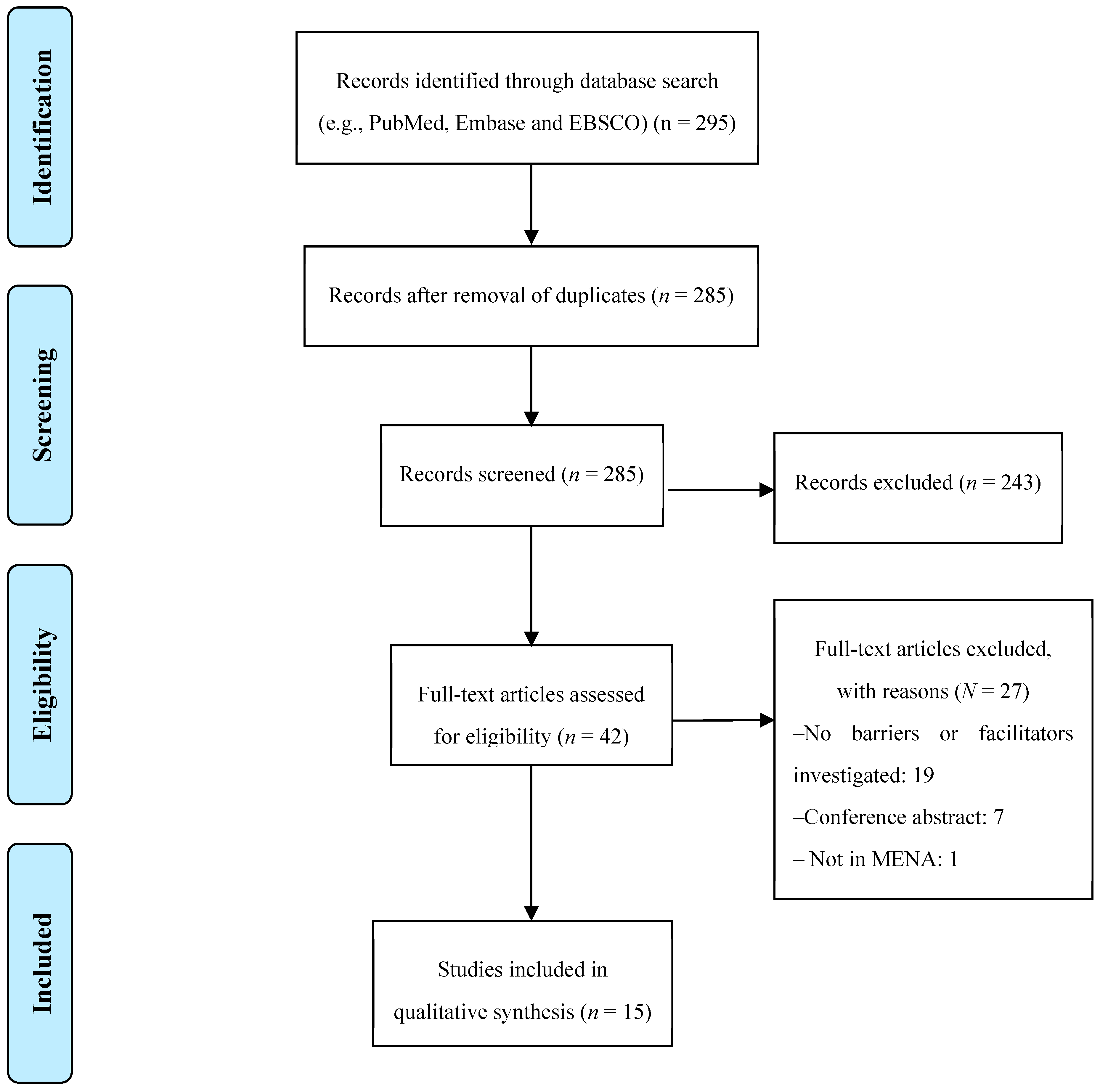
3.1. Literature Search
3.2. Study Characteristics
3.3. Study Quality Assessment
3.4. Barriers to and Facilitators of CPG Implementation
4. Discussion
4.1. Implications for Practice
4.2. Implications for Research
4.3. Strengths and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Steinberg, E.; Greenfield, S.; Wolman, D.M.; Mancher, M.; Graham, R. (Eds.) Clinical Practice Guidelines We Can Trust; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Rabin, B.A.; Brownson, R.C.; Haire-joshu, D.; Kreuter, M.W.; Weaver, N.L. A Glossary for Dissemination and Implementation Research in Health. J. Public Health Manag. Pract. 2008, 14, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagliardi, A.R.; Alhabib, S. Trends in guideline implementation: A scoping systematic review. Implement Sci. 2015, 10, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickan, S.; Burls, A.; Glasziou, P. Patterns of ‘leakage’ in the utilisation of clinical guidelines: A systematic review. Postgrad. Med. J. 2011, 87, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H. Why Don’t Physicians Follow A Framework for Improvement. JAMA 1999, 282, 1458–1465. [Google Scholar] [CrossRef]
- Francke, A.L.; Smit, M.C.; De Veer, A.J.E.; Mistiaen, P. BMC Medical Informatics and Factors influencing the implementation of clinical guidelines for health care professionals: A systematic meta-review. BMC Med. Inform. Decis. Mak. 2008, 8, 38. [Google Scholar] [CrossRef] [Green Version]
- Correa, V.C.; Lugo-agudelo, L.H.; Aguirre-acevedo, D.C.; Alberto, J.; Contreras, P.; María, A. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: A systematic metareview. Health Res. Policy Syst. 2020, 18, 74. [Google Scholar] [CrossRef]
- Gaston, S.; White, S.M.G. Venous Thromboembolism (VTE) Risk Assessment and Prophylaxis: A Comprehensive Systematic Review of the Facilitators and Barriers to Healthcare Worker Compliance with Clinical Practice Guidelines in the Acute Care Setting. JBI Libr. Syst. Rev. 2012, 10, 3812–3893. [Google Scholar] [CrossRef] [Green Version]
- Khatib, R.; Schwalm, J.-D.; Yusuf, S.; Haynes, R.B.; McKee, M.; Khan, M.; Nieuwlaat, R. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: A systematic review and meta-analysis of qualitative and quantitative studies. PLoS ONE 2014, 9, e84238. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi-Bazargani, H.; Tabrizi, J.S.; Azami-Aghdash, S. Barriers to evidence-based medicine: A systematic review. J. Eval. Clin. Pract. 2014, 20, 793–802. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 15 August 2020).
- Center for Evidence Based Management. Critical Appraisal Checklist for Cross-Sectional Study. July 2014. Available online: https://www.cebma.org (accessed on 18 August 2020).
- Wahabi, H.A.; Alziedan, R.A. Reasons behind non-adherence of healthcare practitioners to pediatric asthma guidelines in an emergency department in Saudi Arabia. BMC Health Serv. Res. 2012, 12, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsadig, H.; Scott, J. Use of clinical guidelines in cardiology practice in Sudan. J. Eval. Clin. Pract. 2017, 24, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Ketbi, L.M.B.; Al Deen, S.Z. The attitudes and beliefs of general practitioners towards clinical practice guidelines: A qualitative study in Al Ain, United Arab Emirates. Asia Pac. Fam. Med. 2018. [Google Scholar] [CrossRef]
- Seyed, Z.B.; Nedjat, S.; Yazdizadeh, B.; Nedjat, S.; Majdzadeh, R. Barriers of Clinical Practice Guidelines Development and Implementation in Developing Countries: A Case Study in Iran. Int. J. Prev. Med. 2013, 4, 340. [Google Scholar]
- Majdzadeh, R.; Seyed, Z.B. How to Implement Clinical Practice Guidelines in Iran. Iran Red Crescent Med. J. 2013, 15, e9702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radwan, M.; Sari, A.A.; Rashidian, A.; Takian, A.; Elsous, A.; Abou-dagga, S. Factors hindering the adherence to clinical practice guideline for diabetes mellitus in the Palestinian primary healthcare clinics: A qualitative study. BMJ Open 2018, 8, e021195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aloush, S.M.A.; Abdelkader, F.; Al-Sayaghi, K.; Tawalbeh, L.I.; Suliman, M.; Al Bashtawy, M.; Shaban, I. Compliance of Nurses and Hospitals With Ventilator-Associated Pneumonia. J. Nurs. Care Qual. 2018, 33, E8–E14. [Google Scholar] [CrossRef]
- Radwan, M.; Sari, A.A. Influence of organizational culture on provider adherence to the diabetic clinical practice guideline: Using the competing values framework in Palestinian Primary Healthcare Centers. Int. J. Gen. Med. 2017, 10, 239. [Google Scholar] [CrossRef] [Green Version]
- Radwan, M.; Sari, A.A.; Rashidian, A.; Takian, A. Attitudes of Palestinian Health-Care Professionals in Gaza to Clinical Practice Guideline for Diagnosis and Treatment of Diabetes Mellitus Study Design and Sampling. Front. Endocrinol. 2017, 8, 288. [Google Scholar] [CrossRef] [Green Version]
- El Sharif, N.; Samara, I.; Titi, I.; Awartani, A. Compliance with and knowledge about diabetes guidelines among physicians and nurses in Palestine. East Mediterr. Health J. 2015, 21, 791–802. [Google Scholar] [CrossRef]
- Thabet, F.C.; Zahraa, J.; Chehab, M.S. Adherence to surviving sepsis guidelines among pediatric intensivists. Saudi Med. J. 2017, 38, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Jradi, H. Awareness, Practices, and Barriers regarding Smoking Cessation Treatment among Physicians in Saudi Arabia. J. Addict. Dis. 2017, 36, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Alsubaiei, M.E.; Frith, P.A.; Cafarella, P.A.; Quinn, S.; Al Moamary, M.S.; Mcevoy, R.D. COPD care in Saudi Arabia: physicians’ awareness and knowledge of guidelines and barriers to implementation. Int. J. Tuberc. Lung Dis. 2017, 21, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.A.; Mohammed, A.A.; Sayed, E.; El, E.; Said, R.M. Quality of care of Egyptian asthmatic children: Clinicians adherence to asthma guidelines. Ital. J. Pediatr. 2010, 36, 33. [Google Scholar] [CrossRef] [Green Version]
- Al-azzam, S.I.; Alzoubi, K.H.; Mhaidat, N.M.; Haddadin, R.D.; Masadeh, M.M. Original Article Preoperative antibiotic prophylaxis practice and guideline adherence in Jordan: A multi-centre study in Jordanian hospitals. J. Infect. Dev. Ctries. 2012, 6, 715–720. [Google Scholar] [CrossRef] [Green Version]
- Tomasone, J.R.; Kauffeldt, K.D.; Chaudhary, R.; Brouwers, M.C. Effectiveness of guideline dissemination and implementation strategies on health care professionals’ behaviour and patient outcomes in the cancer care context: A systematic review. Implement Sci. 2020, 15, 41. [Google Scholar] [CrossRef]
- Dizon, J.M.; Machingaidze, S.; Grimmer, K. To adopt, to adapt, or to contextualise? The big question in clinical practice guideline development. BMC Res. Notes 2016, 9, 442. [Google Scholar] [CrossRef] [Green Version]
- Owolabi, M.O.; Yaria, J.O.; Daivadanam, M.; Makanjuola, A.I.; Parker, G.; Oldenburg, B.; Vedanthan, R.; Norris, S.; Oguntoye, A.R.; Osundina, M.A.; et al. Gaps in Guidelines for the Management of Diabetes in Low- and Middle-Income Versus High-Income Countries—A Systematic Review. Diabetes Care 2018, 41, 1097–1105. [Google Scholar] [CrossRef] [Green Version]
- Koornneef, E.; Robben, P.; Hajat, C.; Ali, A.; Uk, M. The development, implementation and evaluation of clinical practice guidelines in Gulf Cooperation Council ( GCC ) countries: A systematic review of literature. J. Eval. Clin. Pract. 2015, 21, 1006–1013. [Google Scholar] [CrossRef]
- Villarosa, A.R.; Maneze, D.; Ramjan, L.M.; Srinivas, R.; Camilleri, M. The effectiveness of guideline implementation strategies in the dental setting: A systematic review. Implement Sci. 2019, 14, 106. [Google Scholar] [CrossRef]
- Spoon, D.; Rietbergen, T.; Huis, A.; Heinen, M.; Van Dijk, M.; Van Bodegom-vos, L.; Ista, E. International Journal of Nursing Studies Implementation strategies used to implement nursing guidelines in daily practice: A systematic review. Int. J. Nurs. Stud. 2020, 111, 103748. [Google Scholar] [CrossRef] [PubMed]
- Ebben, R.H.A.; Siqeca, F.; Madsen, U.R.; Vloet, L.C.M.; Van Achterberg, T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: A systematic review. BMC Open 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Prior, M.; Guerin, M.; Grimmer-Somers, K. The effectiveness of clinical guideline implementation strategies—A synthesis of systematic review findings. J. Eval. Clin. Pract. 2008, 14, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Flottorp, S.A.; Oxman, A.D.; Krause, J.; Musila, N.R.; Wensing, M.; Godycki-Cwirko, M.; Baker, R.; Eccles, M.P. A checklist for identifying determinants of practice: A systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013, 8, 35. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, A.B.; Finley, E.P. Reprint of: Qualitative methods in implementation research. An. Psychiatry Res. 2020, 283, 112629. [Google Scholar] [CrossRef]
- Akala, F.A.; El-Saharty, S. Public-Health Challenges in the Middle East and North Africa. Lancet 2006, 367, 961–964. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year, Country | Study Objectives | Study Methods | Sample Size | Type of Participants (Setting) |
|---|---|---|---|---|
| Qualitative Studies | ||||
| Baradaran-Seyed Z., 2013 Iran | To identify the barriers and implementation of CPGs in Iran. | Interviews and 1 focus group | 12 and 11 | Health policy- and decision- makers, the experts of CPGs development, and the experts of EBM (General) |
| Majdzadeh R., 2013 Iran | To identify the strategies for application of CPGs produced in Iran. | Interviews and 1 focus group | 12 and 11 | Health policy- and decision-makers, the experts of CPGs development, and the experts of EBM (General) |
| Al Ketbi L.M., 2018 United Arab Emirates | To determine the barriers and facilitators of CPG implementation and to determine ways to improve the implementation of CPG recommendations | 6 focus groups | 25 | Physicians (Ambulatory) |
| Radwan M., 2018, Palestine (West Bank and Gaza) | To assess the attitudes of Palestinian health care professionals toward the most perceived factors influencing the adherence to the CPG for diabetes mellitus | Interviews | 20 | Physicians + nurses who were managing/supervising the functions related to chronic diseases (Ambulatory) |
| Mixed Methods | ||||
| Wahabi H.A., 2012 Saudi Arabia | To examine the compliance of the healthcare providers in the Pediatrics Emergency Department, with the recommendations of the Pediatrics Asthma Management Protocol (PAMP), and to explore the reasons behind non-adherence. | Chart review and 2 focus groups and 4 interviews | 10 and 10 and 4 | Physicians + nurse + 1 pharmacist interviewed (Hospital) |
| Elsadig H., 2018, Sudan | To explore the views of prescribers in cardiology in Sudan about the use of guidelines in clinical practice and the extent to which guidelines whether national or international can be adopted in clinical practice in Sudan. | Interviews and survey | 25 and 72 | Physician (Hospital) |
| Quantitative | ||||
| Radwan M., 2017 Palestine (West Bank and Gaza) | Identifying the predominant culture within the Palestinian Primary healthcare centers settings and testing its role in the adherence to CPG for diabetes mellitus. | Questionnaire | 323 | Physicians and nurses (Ambulatory) |
| Radwan M., 2017 Palestine (West Bank and Gaza) | To explore adherence level and the most perceived barriers of the adherence to the CPG for diabetes mellitus | Questionnaire | 323 | Physicians and nurses (Ambulatory) |
| Alsubaiei M.E., 2017 Saudi Arabia | To assess assessed physicians’ knowledge of the Global Initiative for Chronic Obstructive Lung Disease (recommendations in terms of the diagnosis, assessment and management of patients with chronic obstructive pulmonary disease (COPD) | Questionnaire | 44 | Physicians (Hospital) |
| Salama A.A., 2010 Egypt | To assess the current situation as regard clinician attitude towards national and international guidelines for management of pediatric asthma and their adherence to its recommendations through written questionnaire. | Questionnaire | 352 | Physicians (Not clear) |
| Aloush SM., 2017 Jordan, Egypt, and Saudi Arabia | To evaluate nurses’ and hospitals’ compliance with ventilator-associated pneumonia prevention guidelines, the factors that affect their level of compliance, and barriers to compliance. | Questionnaire | 471 | Nurses (Hospital) |
| Thabet F.C., 2017 Saudi Arabia | To describe the initial management of pediatric patients with severe sepsis, to assess the compliance of this management with the 2006 the American College of Critical Care Medicine-Pediatric Advanced Life Support (ACCM-PALS) guidelines, and the 2012 surviving sepsis campaign (SSC) guidelines, and to identify barriers to adherence to these guidelines | Questionnaire | 61 | Pediatric intensivists (Hospital) |
| Sharif N.E., 2016 Palestine | To analyze the pattern of diabetes mellitus care by physicians and nurses and their self-reported compliance with the guidelines | Questionnaire | 401 | Physicians and nurses (Ambulatory) |
| Jradi H., 2015 Saudi Arabia | To assess knowledge, use, and barriers to the implementation of tobacco dependence (the 5A’s: Ask, Assist, Assess, Advise, and Arrange), | Questionnaire | 124 | Physicians (Ambulatory) |
| Al-Azzam S.I., 2012 Jordan | To assess the practice of surgical antibiotic prophylaxis and adherence of practitioners to the American Society of Health System Pharmacists (ASHP) guidelines for antimicrobial prophylaxis in surgery and to explore reasons for non-compliance. | Questionnaire | 160 | Surgeons (Hospital) |
| First Author (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Baradaran-Seyed Z. (2013) | Y | Y | Y | Y | C | C | C | C | Y |
| Majdzadeh R. (2013) | Y | Y | Y | Y | C | Y | Y | C | Y |
| Al Ketbi L.M. (2018) | Y | Y | Y | Y | Y | C | Y | Y | Y |
| Radwan M. (2018) | Y | Y | Y | Y | Y | C | Y | Y | Y |
| Wahabi H.A.* (2012) | Y | Y | Y | Y | Y | C | Y | Y | Y |
| Elsadig H. (2017) * | Y | Y | Y | Y | Y | C | C | C | Y |
| First Author (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Radwan M. (2017) | Y | Y | Y | N | Y | Y | Y | Y | Y | N | N |
| Radwan.M (2017) | Y | Y | Y | N | Y | Y | Y | Y | Y | N | N |
| Alsubaiei M.E. (2017) | Y | Y | Y | C | C | N | Y | C | Y | N | C |
| Salama A.A. (2010) | Y | Y | N | C | Y | Y | C | C | N | N | C |
| Aloush S.M. (2018) | Y | Y | N | Y | C | Y | Y | C | Y | N | C |
| Thabet F.C. (2017) | Y | Y | Y | N | Y | Y | Y | C | N | N | C |
| Sharif N.E. (2016) | Y | Y | Y | N | Y | Y | Y | C | Y | N | N |
| Jradi H. (2017) | Y | Y | N | C | C | N | N | C | Y | N | C |
| Al-Azzam S.I. (2012) | Y | Y | N | C | C | N | Y | C | N | N | C |
| Elsadig H. (2017) | Y | Y | C | C | C | N | Y | C | Y | N | C |
| Category | Barriers | Total Number of Mentions |
|---|---|---|
| Healthcare professional | Lack of awareness of the existence of guidelines | 2 |
| Lack of familiarity with CPGs recommendation | 3 | |
| Disagreement with the recommendations of the CPG | 3 | |
| Doubts about the positive impact of CPGs on outcomes | 2 | |
| Preference for experience over CPGs | 1 | |
| Lack of effective communication, research, and self-learning skills | 1 | |
| Lack of healthcare professional motivation | 3 | |
| Guidelines | Lack of clarity or complexity | 4 |
| Outdated guidelines | 1 | |
| Guideline trustworthiness (i.e., evidence quality, content, and developer) | 6 | |
| Patients | Language and literacy problems | 1 |
| Lack of motivation, compliance, and knowledge to follow the recommendations | 4 | |
| Patient comorbidities, mobility problems, polypharmacy, and self-empowerment capacity | 2 | |
| Patients’ financial situation and occupational status | 5 | |
| Environment | Lack of protocols and processes of dissemination and implementation | 7 |
| Lack of resources (staff, equipment, and beds) | 7 | |
| Lack of time | 2 | |
| Lack of clinical audit and feedback | 4 | |
| Difficulties with availability of medicines or test | 2 | |
| Lack of financial incentives | 3 | |
| Lack of training | 4 | |
| Insurance does not cover recommendations | 1 | |
| Lack of regulation and supervision | 1 | |
| Lack of evidence-based culture and education | 2 | |
| Lack of policy makers supports | 1 | |
| Deficiencies in the referral of patients to services | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almazrou, S.H.; Alfaifi, S.I.; Alfaifi, S.H.; Hakami, L.E.; Al-Aqeel, S.A. Barriers to and Facilitators of Adherence to Clinical Practice Guidelines in the Middle East and North Africa Region: A Systematic Review. Healthcare 2020, 8, 564. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040564
Almazrou SH, Alfaifi SI, Alfaifi SH, Hakami LE, Al-Aqeel SA. Barriers to and Facilitators of Adherence to Clinical Practice Guidelines in the Middle East and North Africa Region: A Systematic Review. Healthcare. 2020; 8(4):564. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040564
Chicago/Turabian StyleAlmazrou, Saja H., Sarah I. Alfaifi, Sumayyah H. Alfaifi, Lamees E. Hakami, and Sinaa A. Al-Aqeel. 2020. "Barriers to and Facilitators of Adherence to Clinical Practice Guidelines in the Middle East and North Africa Region: A Systematic Review" Healthcare 8, no. 4: 564. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040564