An Exercise Training and Healthy Eating Group Program (ATHENA) for Overweight and Obese Women with Urinary Incontinence: An Intervention Description

 ,
, 
 and
and 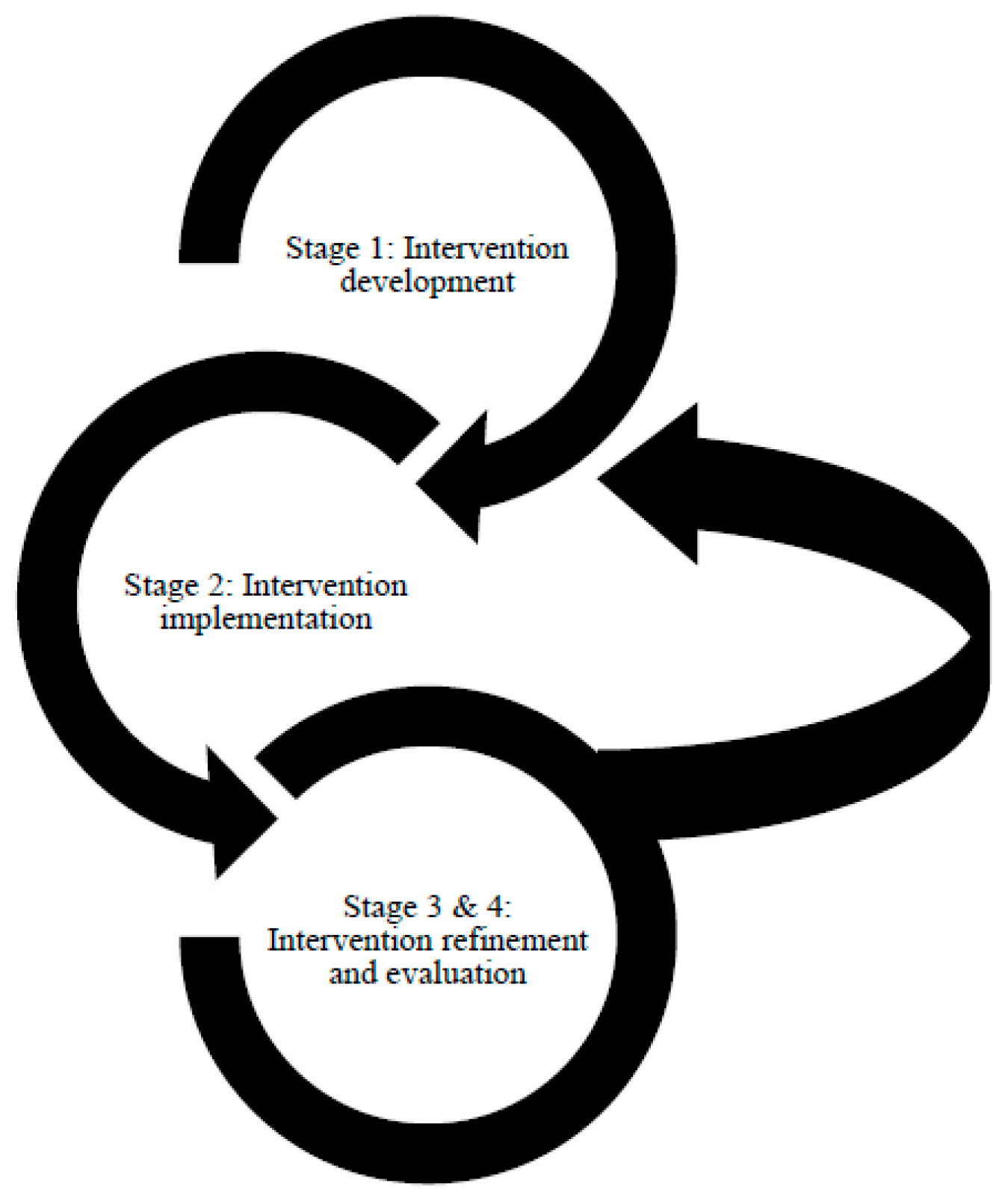{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Procedure
2.2.1. Stage 1: Intervention Development
Establishment of Research Co-Production Team
Collaborative Design of Evidence-Based Intervention and Supporting Clinician and Patient Resources
Resources
Establishment of Intervention Team
2.2.2. Stage 2: Intervention Implementation
Participant Recruitment Procedures
Participant Experience
2.2.3. Stage 3: Intervention Refinement
2.2.4. Stage 4: Intervention Evaluation
3. Results
3.1. Intervention Description
3.1.1. Component 1: Supervised PFMT
3.1.2. Component 2: General Exercise Training
3.1.3. Component 3: Pelvic Health Education
3.1.4. Component 4: Healthy Eating Education
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Haylen, B.T.; De Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. Off. J. Int. Cont. Soc. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Carls, C. The prevalence of stress urinary incontinence in high school and college-age female athletes in the midwest: Implications for education and prevention. Urol. Nurs. 2007, 27, 21. [Google Scholar] [PubMed]
- Kinchen, K.S.; Lee, J.; Fireman, B.; Hunkeler, E.; Nehemiah, J.L.; Curtice, T.G. The prevalence, burden, and treatment of urinary incontinence among women in a managed care plan. J. Women’s Health 2007, 16, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Sampselle, C.M.; Harlow, S.D.; Skurnick, J.; Brubaker, L.; Bondarenko, I. Urinary incontinence predictors and life impact in ethnically diverse perimenopausal women. Obstet. Gynecol. 2002, 100, 1230–1238. [Google Scholar] [PubMed]
- Milsom, I.; Coyne, K.S.; Nicholson, S.; Kvasz, M.; Chen, C.-I.; Wein, A.J. Global prevalence and economic burden of urgency urinary incontinence: A systematic review. Eur. Urol. 2014, 65, 79–95. [Google Scholar] [CrossRef]
- Subak, L.L.; Wing, R.; West, D.S.; Franklin, F.; Vittinghoff, E.; Creasman, J.M.; Richter, H.E.; Myers, D.; Burgio, K.L.; Gorin, A.A.; et al. Weight Loss to Treat Urinary Incontinence in Overweight and Obese Women. N. Engl. J. Med. 2009, 360, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Qaseem, A.; Dallas, P.; Forciea, M.A.; Starkey, M.; Denberg, T.D.; Shekelle, P. Nonsurgical management of urinary incontinence in women: A clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 2014, 161, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Doran, C.M.; Chiarelli, P.; Cockburn, J. Economic costs of urinary incontinence in community-dwelling Australian women. Med. J. Aust. 2001, 174, 456–458. [Google Scholar] [CrossRef]
- Wyndaele, M.; Hashim, H. Pathophysiology of urinary incontinence. Surg. Infect. (Oxf.) 2017, 35, 287–292. [Google Scholar] [CrossRef]
- Elenskaia, K.; Haidvogel, K.; Heidinger, C.; Doerfler, D.; Umek, W.; Hanzal, E. The greatest taboo: Urinary incontinence as a source of shame and embarrassment. Wien. Klin. Wochenschr. 2011, 123, 607–610. [Google Scholar] [CrossRef]
- Hägglund, D.; Wadensten, B. Fear of humiliation inhibits women’s care-seeking behaviour for long-term urinary incontinence. Scand. J. Caring Sci. 2007, 21, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, D.; Walker-Engström, M.-L.; Larsson, G.; Leppert, J. Reasons why women with long-term urinary incontinence do not seek professional help: A cross-sectional population-based cohort study. Int. Urogynecol. J. 2003, 14, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Dumoulin, C.; Cacciari, L.; Hay-Smith, J. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Cardozo, L.; Wagg, A.; Wein, A. (Eds.) Chapter 12: Adult Conservative management. In Incontinence 6th Edition; ICI-ICS, International Continence Society: Bristol, UK, 2017. [Google Scholar]
- Lamerton, T.; Torquati, L.; Brown, W. Overweight and obesity as major, modifiable risk factors for urinary incontinence in young to mid-aged women: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1735–1745. [Google Scholar] [CrossRef]
- Schreiber Pedersen, L.; Lose, G.; Høybye, M.T.; Elsner, S.; Waldmann, A.; Rudnicki, M. Prevalence of urinary incontinence among women and analysis of potential risk factors in Germany and Denmark. Acta Obstet. Gynecol. Scand. 2017, 96, 939–948. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; Australian Government, Department of Health: Canberra, Australia, 2013.
- Moreno, J.P.; Johnston, C.A. Barriers to physical activity in women. Am. J. Lifestyle Med. 2014, 8, 164–166. [Google Scholar] [CrossRef]
- Breyer, B.N.; Creasman, J.M.; Richter, H.E.; Myers, D.; Burgio, K.L.; Wing, R.R.; West, D.S.; Kusek, J.W.; Subak, L.L. A behavioral weight loss program and nonurinary incontinence lower urinary tract symptoms in overweight and obese women with urinary incontinence: A secondary data analysis of PRIDE. J. Urol. 2018, 199, 215–222. [Google Scholar] [CrossRef]
- Dumoulin, C.; Morin, M.; Danieli, C.; Mayrand, M.-H.; Tousignant, M.; Abrahamowicz, M. Group physiotherapy compared to individual physiotherapy to treat urinary incontinence in older women: A non-inferiority randomized control trial. In Proceedings of the International Continence Society 49th Annual Meeting, Gothenburg, Sweden, 6 September 2019; p. 486. [Google Scholar]
- Lamb, S.; Pepper, J.; Lall, R.; Jørstad-Stein, E.; Clark, M.; Hill, L.; Fereday-Smith, J. Group treatments for sensitive health care problems: A randomised controlled trial of group versus individual physiotherapy sessions for female urinary incontinence. BMC Women’s Health 2009, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, L.; Archibald, M.; Arseneau, D.; Scott, S.D. Development of a checklist to assess the quality of reporting of knowledge translation interventions using the Workgroup for Intervention Development and Evaluation Research (WIDER) recommendations. Implement. Sci. 2013, 8, 52. [Google Scholar] [CrossRef] [Green Version]
- Canadian Institute of Health Research. Guide to Knowledge Translation Planning at CIHR: Integrated and End-of-Grant Approaches; Her Majesty the Queen in Right of Canada: Ottawa, ON, Canada, 2012. [Google Scholar]
- Pereira, V.S.; Correia, G.N.; Driusso, P. Individual and group pelvic floor muscle training versus no treatment in female stress urinary incontinence: A randomized controlled pilot study. Eur. J. Obs. Gynecol. Reprod. Biol. 2011, 159, 465–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Urinary Incontinence and Pelvic Organ Prolapse in Women: Management; NICE: London, UK, 2019. [Google Scholar]
- Langston, K.; Ross, L.J.; Byrnes, A.; Hay, R. Secondary-prevention behaviour-change strategy for high-risk patients: Benefits for all classes of body mass index. Nutr. Diet. 2020, 77, 499–507. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Obesity: Identification, Assessment and Management; National Institute for Health and Care Excellence (NICE): London, UK, 2014. [Google Scholar]
- Demain, S.; Smith, J.F.; Hiller, L.; Dziedzic, K. Comparison of group and individual physiotherapy for female urinary incontinence in primary care: Pilot study. Physiotherapy 2001, 87, 235–242. [Google Scholar] [CrossRef]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217. [Google Scholar] [CrossRef] [Green Version]
- Bø, K.; Talseth, T.; Holme, I. Single blind, randomised controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women. BMJ 1999, 318, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Berzuk, K.; Shay, B. Effect of increasing awareness of pelvic floor muscle function on pelvic floor dysfunction: A randomized controlled trial. Int. Urogynecol. J. 2015, 26, 837–844. [Google Scholar] [CrossRef]
- McConnell, T.; Best, P.; Davidson, G.; McEneaney, T.; Cantrell, C.; Tully, M.J.R.I. Engagement. Coproduction for feasibility and pilot randomised controlled trials: Learning outcomes for community partners, service users and the research team. Res. Involv. Engagem. 2018, 4, 32. [Google Scholar] [CrossRef] [Green Version]
- Hickey, G.; Richards, T.; Sheehy, J. Co-Production from Proposal to Paper; Nature Publishing Group: Berlin, Germany, 2018. [Google Scholar]
- Dwamena, F.; Holmes-Rovner, M.; Gaulden, C.M.; Jorgenson, S.; Sadigh, G.; Sikorskii, A.; Lewin, S.; Smith, R.C.; Coffey, J.; Olomu, A. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef]
- Weingart, S.N.; Zhu, J.; Chiappetta, L.; Stuver, S.O.; Schneider, E.C.; Epstein, A.M.; David-Kasdan, J.A.; Annas, C.L.; Fowler, F.J.; Weissman, J.S. Hospitalized patients’ participation and its impact on quality of care and patient safety. Int. J. Qual. Health Care 2011, 23, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Sahlsten, M.; Larsson, I.; Sjostrom, B.; Plos, K. An analysis of the concept of patient participation. Nurs. Forum 2008, 43, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Health Literacy. Available online: https://www.aihw.gov.au/reports/australias-health/health-literacy (accessed on 23 November 2020).
- Australian Bureau of Statistics. National Health Survey: Health Literacy. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-health-literacy/latest-release (accessed on 23 November 2020).
- Balzarro, M.; Rubilotta, E.; Goss, C.; Costantini, E.; Artibani, W.; Sand, P. Counseling in urogynecology: A difficult task, or simply good surgeon–patient communication? Int. Urogynecol. J. 2018, 29, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Coyne, J.C. Towards a cumulative science of behaviour change: Do current conduct and reporting of behavioural interventions fall short of best practice. Psychol. Health 2007, 22, 869–874. [Google Scholar]
- Michie, S.; Fixsen, D.; Grimshaw, J.M.; Eccles, M.P. Specifying and reporting complex behaviour change interventions: The need for a scientific method. Implement. Sci. 2009, 4, 40. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howard, Z.; Ross, L.; Smith, L.; Baker, N.; Nucifora, J.; Townsend, H.; Weir, K.; Roberts, S. An Exercise Training and Healthy Eating Group Program (ATHENA) for Overweight and Obese Women with Urinary Incontinence: An Intervention Description. Healthcare 2020, 8, 575. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040575
Howard Z, Ross L, Smith L, Baker N, Nucifora J, Townsend H, Weir K, Roberts S. An Exercise Training and Healthy Eating Group Program (ATHENA) for Overweight and Obese Women with Urinary Incontinence: An Intervention Description. Healthcare. 2020; 8(4):575. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040575
Chicago/Turabian StyleHoward, Zara, Lynda Ross, Leanne Smith, Nadine Baker, Jennifer Nucifora, Heidi Townsend, Kelly Weir, and Shelley Roberts. 2020. "An Exercise Training and Healthy Eating Group Program (ATHENA) for Overweight and Obese Women with Urinary Incontinence: An Intervention Description" Healthcare 8, no. 4: 575. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare8040575