Designing an IT Ecosystem for Pregnancy Care Management Based on Pervasive Technologies


 ,
,
Abstract
:1. Introduction
2. Related Work
2.1. Electronic and Personal Health Records
2.2. Mobile Pregnancy Care Applications
- the area of mobile health is emerging with a wide corpus of applications and research
- the majority of the proposed solutions were applied in experimental conditions and are based on custom made systems not being a part of a comprehensive medical IT ecosystem
- mPHR has become the de facto standard in mHealth
- there is great potential for employing sensors and IoT in general
- the majority of mobile solutions do not have a scientific background
- pregnancy care is among the most interesting in the mHealth literature.
2.3. Research Questions
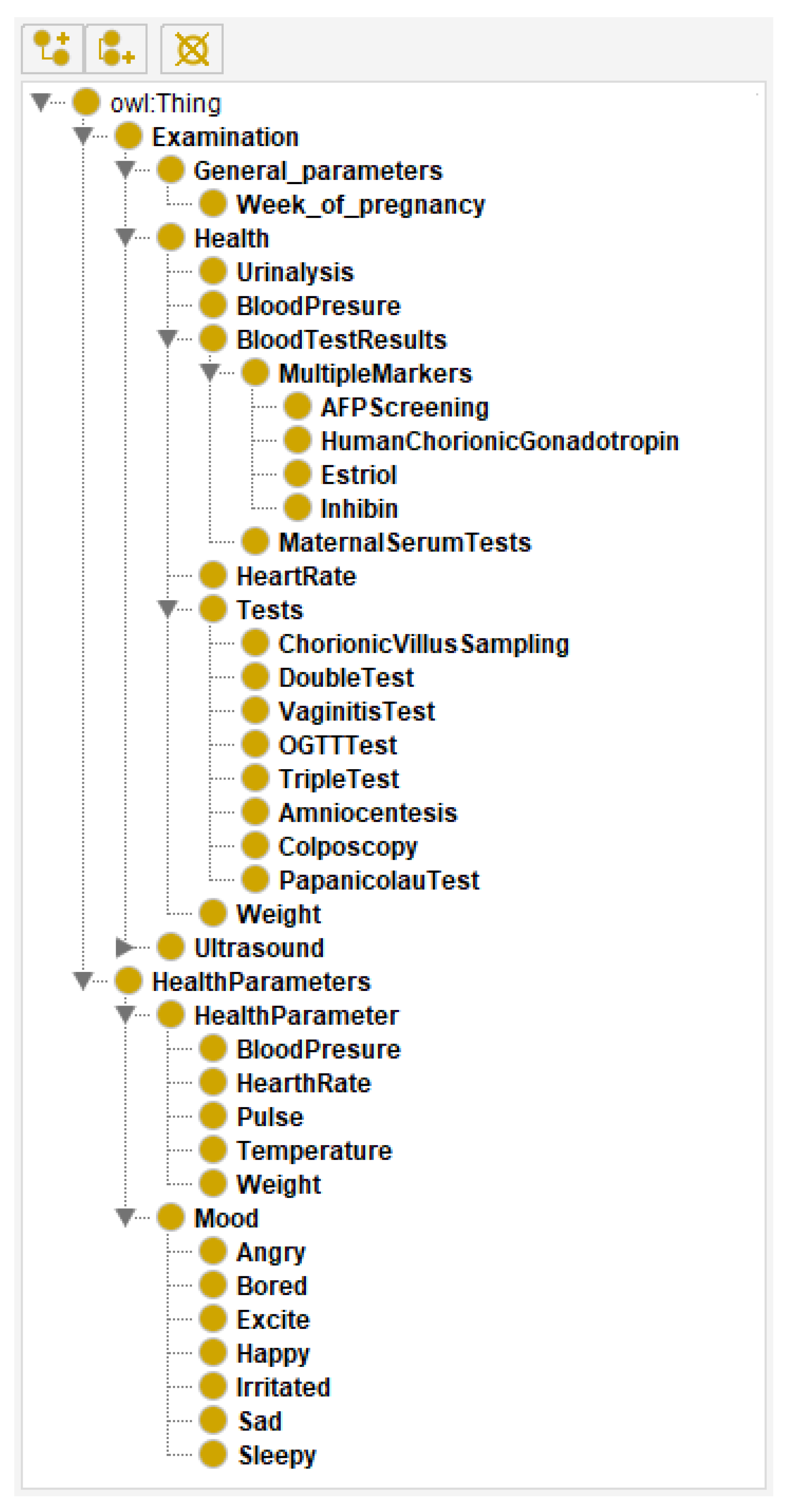
3. Designing a Pregnancy Care Ontology
- Class Examination includes all the important parts for a pregnancy check at the gynaecologist:
- -
- Tests—gynaecological and medical tests during pregnancy. Some of them (VaginitisTest and PapanicolauTest) are obligatory, while others depend on the pregnancy itself and imply additional checks, such as TripleTest and Amniocentesis.
- -
- General Parameters—parameters related to the current week of pregnancy and data about tests that should be performed.
- -
- Health—all important parameters that have to be tested on every check, such as blood pressure, urine analysis, heart rate and weight.
- -
- Ultrasound—this class includes two ultrasound checks that are performed during the pregnancy: transvaginal and abdominal.
- Class Health Parameters includes all the parameters and emotional states of the pregnant women that have to be controlled daily. These parameters include two groups:
- -
- Health Parameter—parameters that a pregnant woman has to pay attention to. The idea is to prevent or detect problems before they escalate.
- -
- Mood—a pregnant woman’s mood and mental health, such as stress, depression and other unwanted moods that could impact the foetal development.
4. Designing a Platform for Pregnancy Care Management
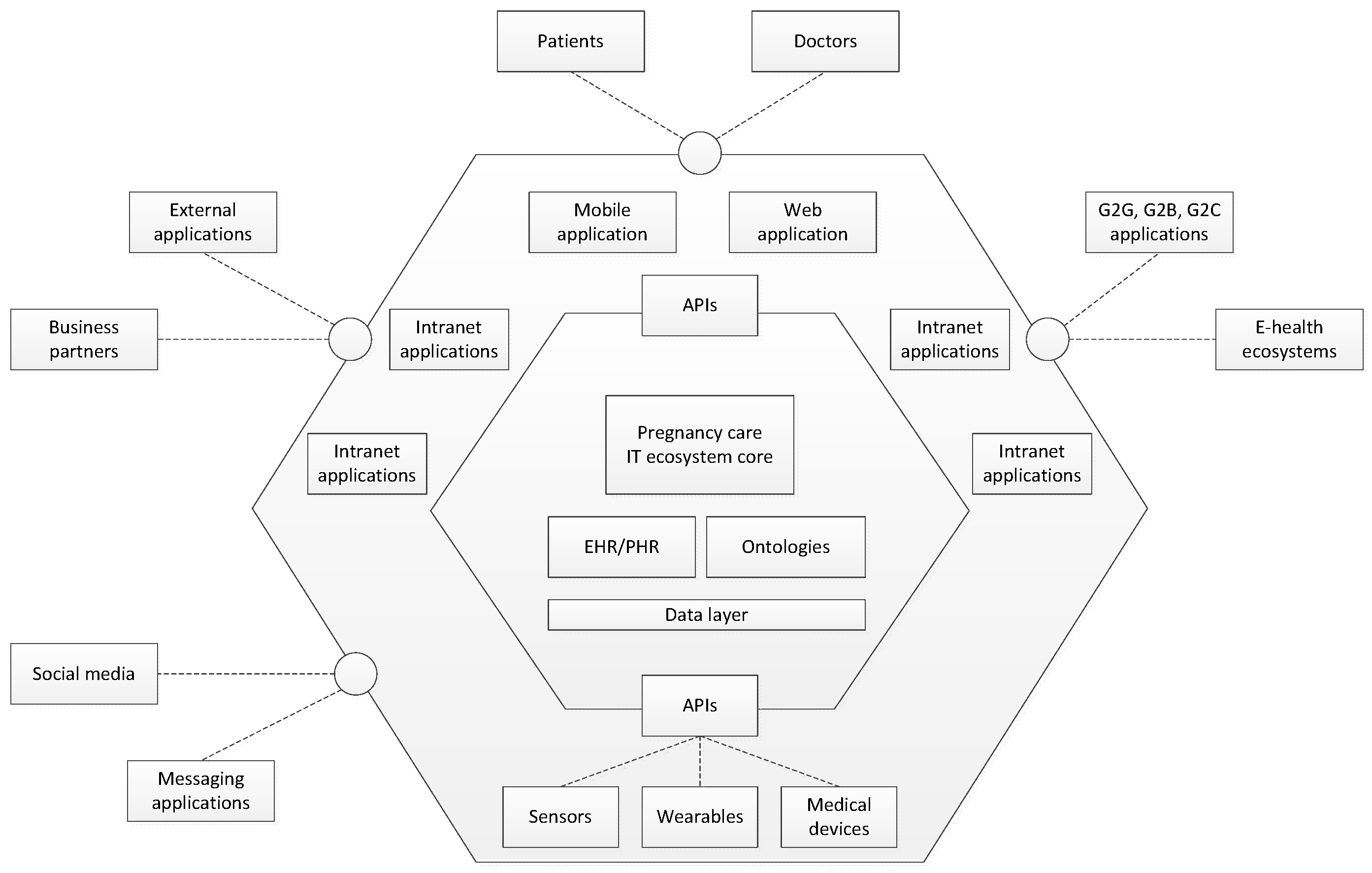
4.1. IT Ecosystem for Pregnancy Care Management
- Core—this is the central part of the platform that manages all the data, logic and relationships.
- Application layer—this layer includes several components:
- -
- Platform APIs—a corpus of REST APIs that connects the core part of the platform with all other components.
- -
- Mobile app—native Android application that helps pregnant women and doctors to manage pregnancy easier
- -
- Web application/portal/website—a common web application that enables pregnant women to manage their data related to the pregnancy as well as educational content, while the doctors are enabled to manage the whole platform data. The platform administrator manages the platform via the portal. It is also a single access point to the platform services and applications, including a lot of education content: texts, blogs, knowledge tests, FAQs, videos, forums, etc.
- -
- Internal applications (intranet)—the solutions that are necessary for both common and particular processes and activities: supply chain management, CRM, document management system, marketing, etc.
- -
- Devices and sensors—the system should be connected automatically to different kinds of devices, such as the ultrasound device. Different kinds of sensors can be integrated into the system.
- Environment—the layer that interacts with stakeholders, i.e., exchange data and managing requests from the environment. It includes integrations with external services and apps. The system needs data from other systems, web services and applications, such as calendars, disease databases, and weather services.
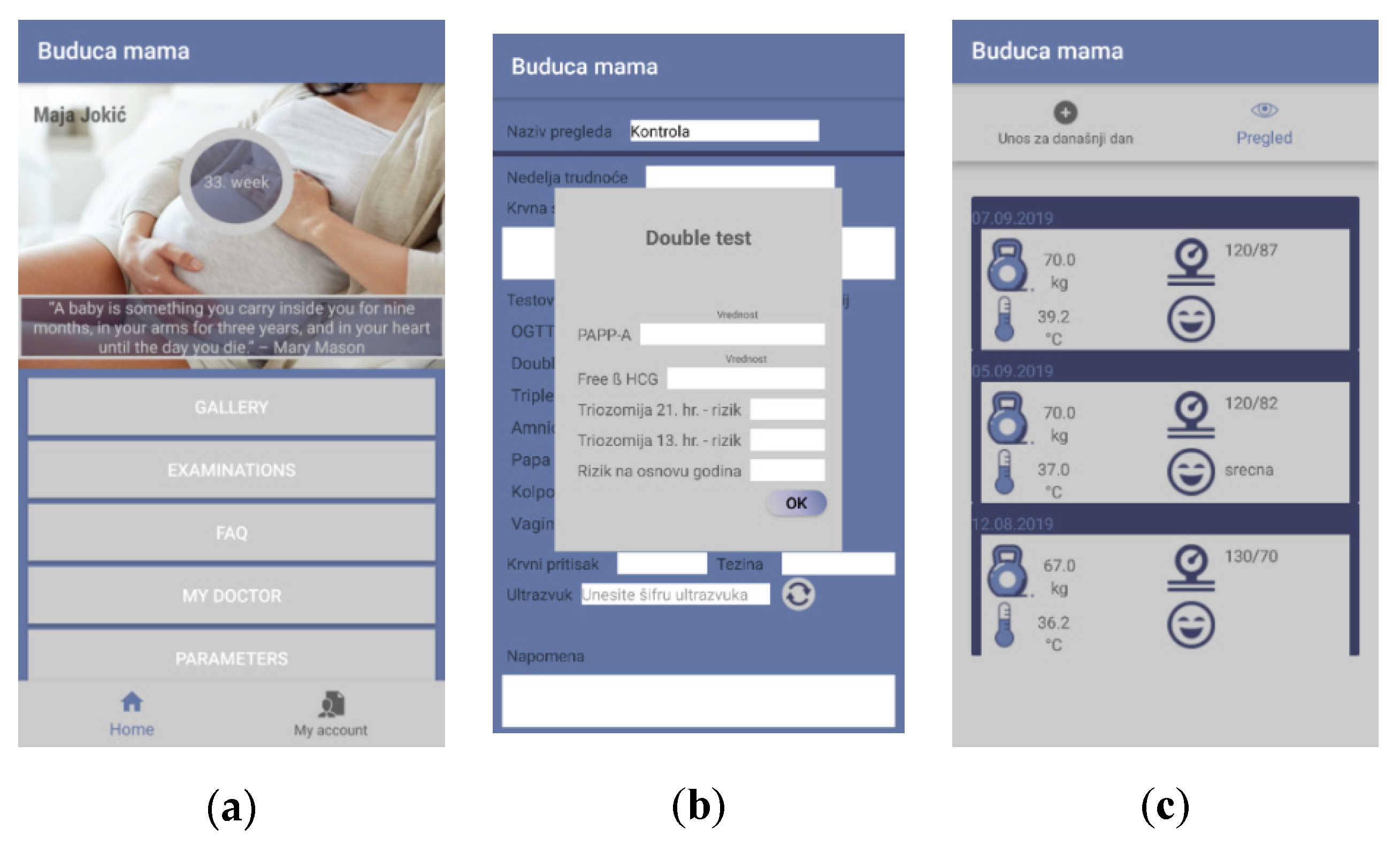
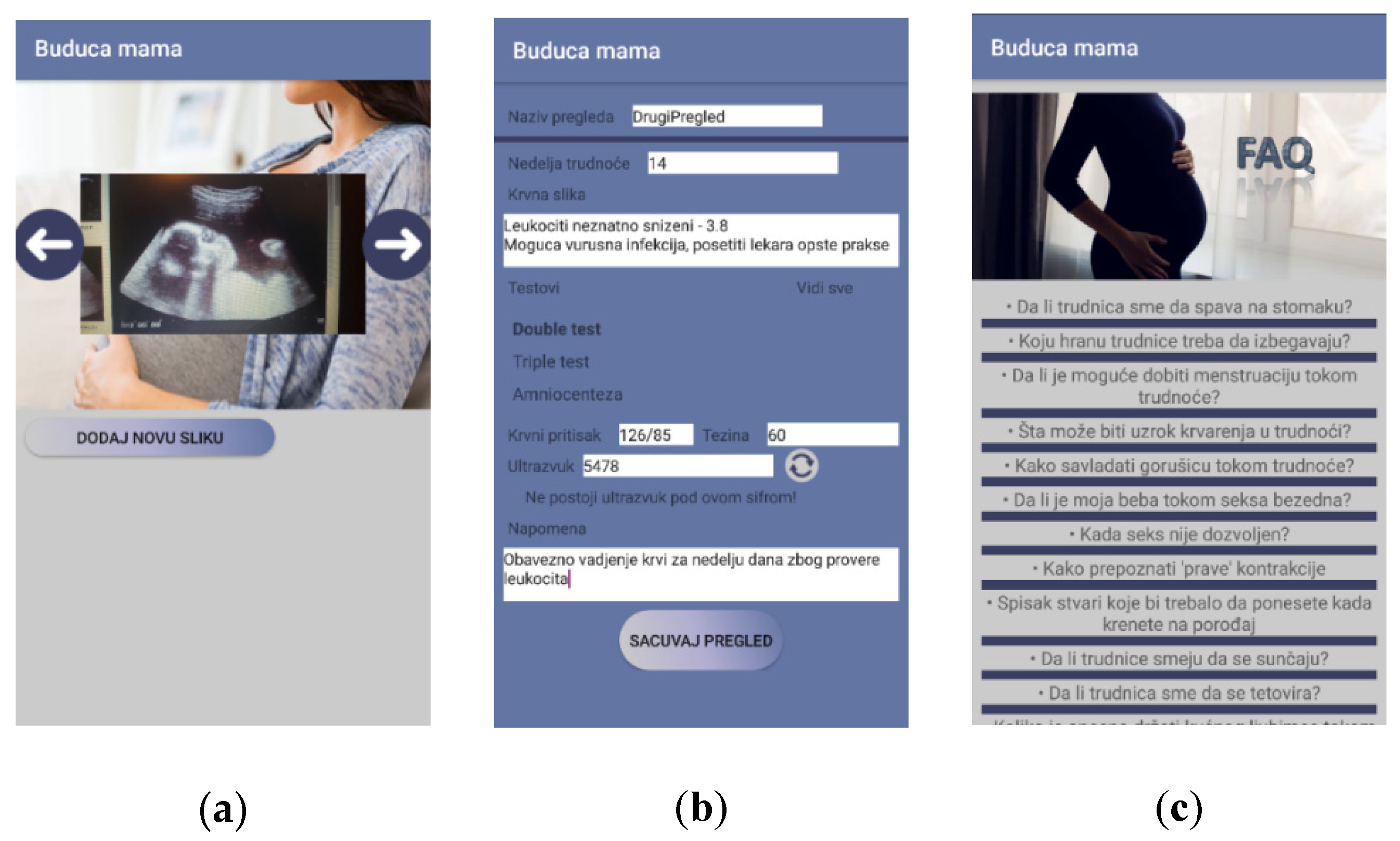
4.2. Mobile Application for Pregnancy Care Management
- Mother—monitoring and entering data related to the mother herself. Further, there is a lot of educational content regarding pregnancy.
- Baby—monitoring and collecting data related to the foetus.
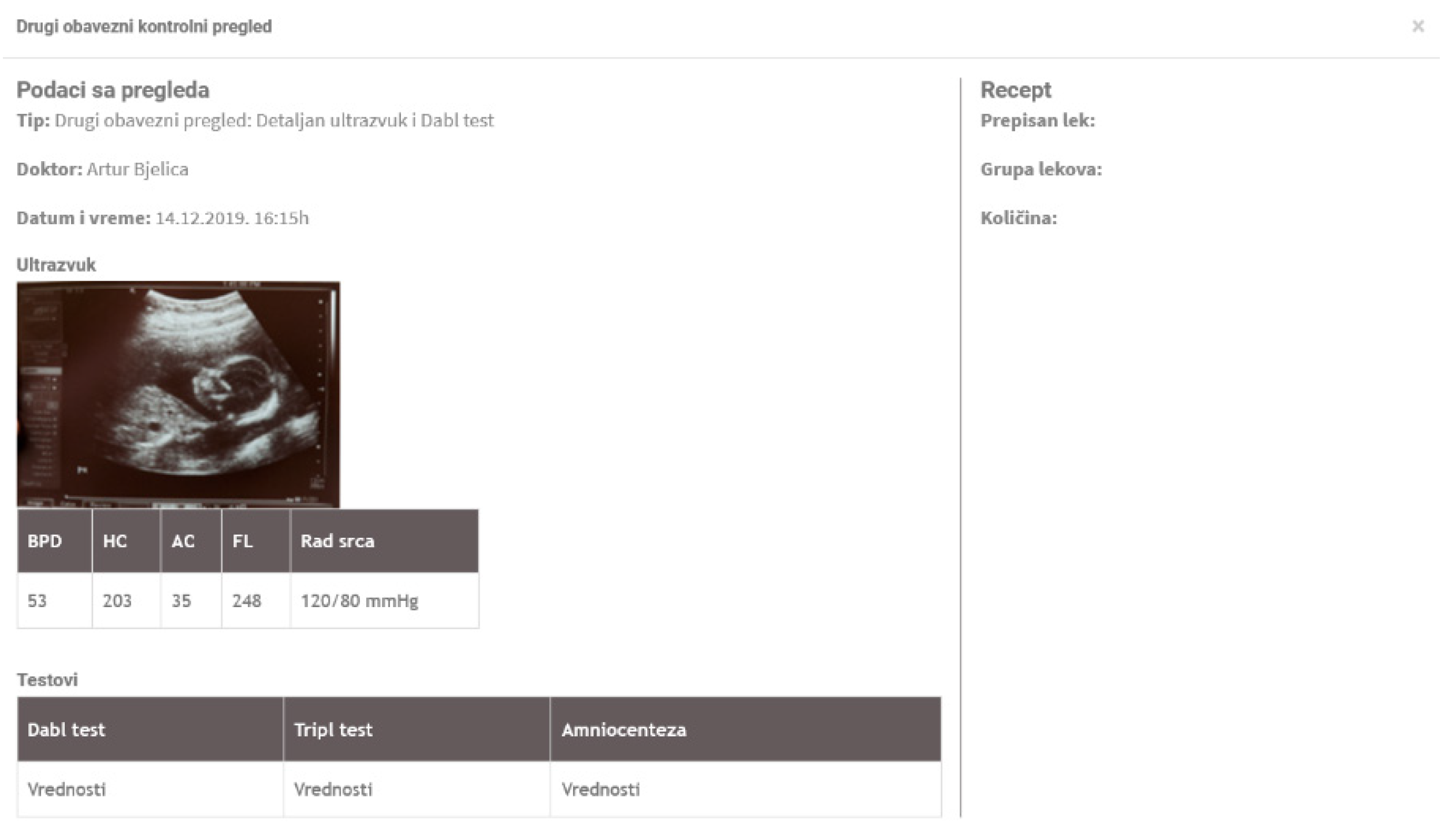
- Smart examination—collecting data within examinations. Data could be inserted both manually and automatically loaded from the devices/sensors.
- Doctor—the pregnant woman and the baby data management.
- My profile—common profile page with details related to the pregnant woman
- Authentication/Registration—common features related to opening an account within the system and access to the system
- FAQ—the part that contains a vast set of information and answers that should help pregnant women
- Dashboard—a page that presents the most important data related to the pregnancy: current week, links to both checks and messages
- Doctor/Pregnant woman overview—common overview of the doctor’s/pregnant woman’s profile with basic info related to the person
- Communication—this is the common messaging system
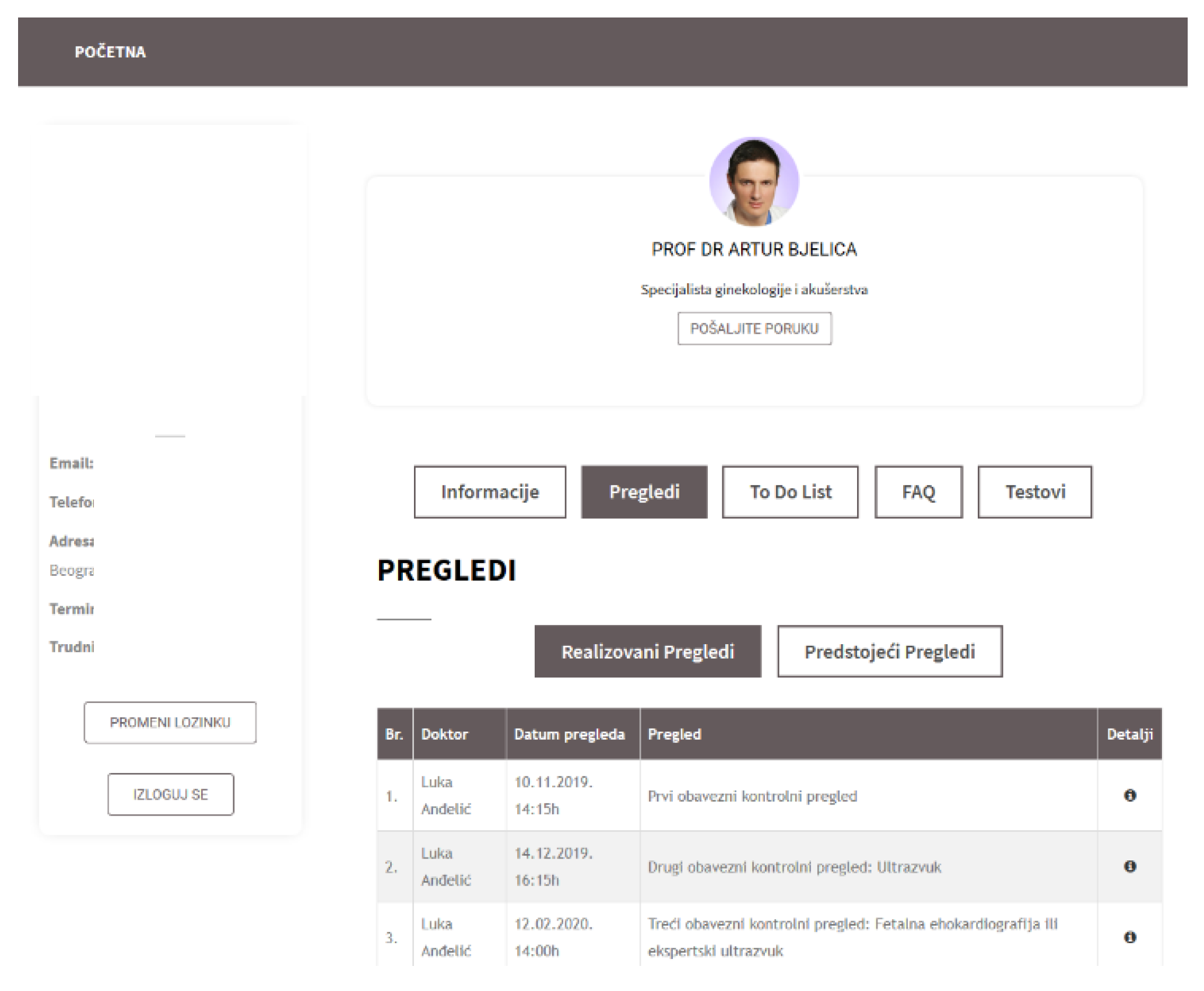
- My checks—a list of all the recorded checks a woman had
- Check details—data related to a single check
- Image gallery—Common gallery with all the images generated through the app or via external devices within the checks
- Pregnancy parameters—this feature enables a pregnant woman to enter a set of parameters important for pregnancy, such as height, weight, mood, and blood pressure.
- Perform check—this is the page where a new check is performed, i.e., the values of the parameters are populated and saved.
4.3. Web Application for Pregnancy Care Management
5. Evaluation
5.1. Research Settings
5.2. Data Collection and Sample
5.3. Measurement Development
5.4. Research Results
- -
- “It would be good if the application could enable communication about gynaecological issues other than just pregnancy”
- -
- “Expand the list of frequently asked questions—include some topics around the birth itself and the period after it”
- -
- “Make scheduling checks easier”
- -
- “The application would help a lot and provide answers to questions where gynaecologists would not have to bother with regular questions. I think that this would calm pregnant women but also relieve doctors. However, I still prefer meeting with the doctor in person. “
- -
- “Add Reminders for scheduled checks”
- -
- “Expand the list of frequently asked questions—to include some topics around the birth itself and the period after it”
- -
- “Ensure access to all pregnant women”
- -
- “Make scheduling controls easier”
- -
- “Emergency contact alarm when a patient has an emergency so that she can immediately receive a referral for further steps”
- -
- Dashboard page (initial page after logging in),
- -
- Entering pregnancy parameters,
- -
- Messaging,
- -
- FAQ,
- -
- Check details,
6. Discussion
7. Conclusions and Future Work
7.1. Limitations
7.2. Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krishnamurti, T.; Davis, A.L.; Wong-Parodi, G.; Fischhoff, B.; Sadovsky, Y.; Simhan, H.N. Development and Testing of the MyHealthyPregnancy App: A Behavioral Decision Research-Based Tool for Assessing and Communicating Pregnancy Risk. JMIR mHealth uHealth 2017, 5, e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Heuvel, J.F.M.; Kariman, S.S.; van Solinge, W.W.; Franx, A.; Lely, A.T.; Bekker, M.N. SAFE@HOME—Feasibility study of a telemonitoring platform combining blood pressure and preeclampsia symptoms in pregnancy care. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Bachiri, M.; Idri, A.; Fernández-Alemán, J.L.; Toval, A. Mobile personal health records for pregnancy monitoring functionalities: Analysis and potential. Comput. Methods Progr. Biomed. 2016, 134, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Van Den Heuvel, J.F.; Groenhof, T.K.; Veerbeek, J.H.; Van Solinge, W.W.; Lely, A.T.; Franx, A.; Bekker, M.N. eHealth as the next-generation perinatal care: An overview of the literature. J. Med. Internet Res. 2018, 20, e202. [Google Scholar] [CrossRef]
- Şat, S.Ö.; Sözbir, Ş.Y. Use of mobile applications and blogs by pregnant women in Turkey and the impact on adaptation to pregnancy. Midwifery 2018, 62, 273–277. [Google Scholar]
- Haddad, S.M.; Souza, R.T.; Cecatti, J.G. Mobile technology in health (mHealth) and antenatal care–searching for apps and available solutions: A systematic review. Int. J. Med. Inform. 2019, 127, 1–8. [Google Scholar] [CrossRef]
- Fonseca, F.; Peixoto, H.; Braga, J.; Machado, J.; Abelha, A. Smart Mobile Computing in Pregnancy Care. In Proceedings of the CATA, Breckenridge, CO, USA, 26–29 August 2019; pp. 219–224. [Google Scholar]
- Carter, J.; Sandall, J.; Shennan, A.H.; Tribe, R.M. Mobile phone apps for clinical decision support in pregnancy: A scoping review. BMC Med Inform. Decis. Mak. 2019, 19, 219. [Google Scholar] [CrossRef]
- Signorini, M.; Lanzola, G.; Torti, E.; Fanelli, A.; Magenes, G. Antepartum Fetal Monitoring through a Wearable System and a Mobile Application. Technologies 2018, 6, 44. [Google Scholar] [CrossRef] [Green Version]
- Saarikko, J.; Niela-Vilen, H.; Ekholm, E.; Hamari, L.; Azimi, I.; Liljeberg, P.; Rahmani, A.M.; Löyttyniemi, E.; Axelin, A. Continuous 7-Month Internet of Things–Based Monitoring of Health Parameters of Pregnant and Postpartum Women: Prospective Observational Feasibility Study. JMIR Form. Res. 2020, 4, e12417. [Google Scholar] [CrossRef]
- Krey, M. Wearable Technology in Health Care-Acceptance and Technical Requirements for Medical Information Systems. In Proceedings of the 2020 IEEE 6th International Conference on Information Management (ICIM), London, UK, 27–29 March 2020; pp. 274–283. [Google Scholar]
- Muthiah, A.; Ajitha, S.; KS, M.T.; Kavitha, K.; Marimuthu, R. Maternal ehealth Monitoring System using LoRa Technology. In Proceedings of the 2019 IEEE 10th International Conference on Awareness Science and Technology (iCAST), Morioka, Japan, 23–25 October 2019; pp. 1–4. [Google Scholar]
- Silva, B.M.; Rodrigues, J.J.; de la Torre Díez, I.; López-Coronado, M.; Saleem, K. Mobile-health: A review of current state in 2015. J. Biomed. Inform. 2015, 56, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Hawthorne, K.H.; Richards, L. Personal health records: A new type of electronic medical record. Rec. Manag. J. 2017, 27, 286–301. [Google Scholar] [CrossRef]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inform. 2016, S48–S61. [Google Scholar] [CrossRef] [PubMed]
- Plastiras, P.; O’Sullivan, D. Exchanging personal health data with electronic health records: A standardized information model for patient generated health data and observations of daily living. Int. J. Med. Inform. 2018, 120, 116–125. [Google Scholar] [CrossRef] [PubMed]
- AHIMA e-HIM Personal Health Record Work Group. Practice brief. The role of the personal health record in the EHR. J. AHIMA 2005, 76, 64A–64D. [Google Scholar]
- Kharrazi, H.; Chisholm, R.; VanNasdale, D.; Thompson, B. Mobile personal health records: An evaluation of features and functionality. Int. J. Med. Inform. 2012, 81, 579–593. [Google Scholar] [CrossRef] [PubMed]
- The Value of Personal Health Record (PHR) Systems. Available online: https://www.researchgate.net/publication/23463787_The_Value_of_Personal_Health_Record_PHR_Systems (accessed on 7 July 2020).
- Showell, C. Barriers to the use of personal health records by patients: A structured review. PeerJ 2017, 5, e3268. [Google Scholar] [CrossRef] [Green Version]
- Roehrs, A.; da Costa, C.A.; da Rosa Righi, R.; da Silva, V.F.; Goldim, J.R.; Schmidt, D.C. Analyzing the performance of a blockchain-based personal health record implementation. J. Biomed. Inform. 2019, 92, 103140. [Google Scholar] [CrossRef]
- Rajput, A.R.; Li, Q.; Ahvanooey, M.T.; Masood, I. EACMS: Emergency access control management system for personal health record based on blockchain. IEEE Access 2019, 7, 84304–84317. [Google Scholar] [CrossRef]
- Sardi, L.; Idri, A.; Redman, L.M.; Alami, H.; Bezad, R.; Fernández-Alemán, J.L. Mobile health applications for postnatal care: Review and analysis of functionalities and technical features. Comput. Methods Progr. Biomed. 2020, 184, 105114. [Google Scholar] [CrossRef]
- Olivero, E.; Bert, F.; Thomas, R.; Scarmozzino, A.; Raciti, I.M.; Gualano, M.R.; Siliquini, R. E-tools for hospital management: An overview of smartphone applications for health professionals. Int. J. Med. Inform. 2019, 124, 58–67. [Google Scholar] [CrossRef]
- Tripp, N.; Hainey, K.; Liu, A.; Poulton, A.; Peek, M.; Kim, J.; Nanan, R. An emerging model of maternity care: Smartphone, midwife, doctor? Women Birth 2014, 27, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Moon, M. Utilization and content evaluation of mobile applications for pregnancy, birth, and child care. Healthc. Inform. Res. 2016, 22, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Huang, Y.; Yu, K.; Fan, R.; Zhou, J. Maternal health care wearing equipment based on fetal information monitoring. J. Infect. Public Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Song, T.M.; Park, H.A.; Jin, D.L. Development of health information search engine based on metadata and ontology. Healthc. Inform. Res. 2014, 20, 88–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, R.; Dwivedi, D.S. Ontology Description using OWL to Support Semantic Web Applications. Int. J. Comput. Appl. 2011, 14, 30–33. [Google Scholar]
- Luna-Aveiga, H.; Medina-Moreira, J.; Apolinario-Arzube, O.; Paredes-Valverde, M.A.; Lagos-Ortiz, K.; Valencia-García, R. Astmapp: A Platform for Asthma Self-Management. J. Univ. Comput. Sci. 2018, 24, 1496–1514. [Google Scholar]
- SNOMED CT Pregnancy Detection Examination. Available online: http://purl.bioontology.org/ontology/SNOMEDCT/74036000%0A%0A (accessed on 8 July 2020).
- METHONTOLOGY: From Ontological Art towards Ontological Engineering. Available online: https://www.researchgate.net/publication/50236211_METHONTOLOGY_from_ontological_art_towards_ontological_engineering (accessed on 16 July 2020).
- Grau, B.C.; Horrocks, I.; Motik, B.; Parsia, B.; Patel-Schneider, P.; Sattler, U. OWL 2: The next step for OWL. Web Semant. 2008, 6, 309–322. [Google Scholar] [CrossRef]
- Noy, N.; McGuinness, D. Ontology Development 101: A Guide to Creating Your First Ontology. Available online: https://protege.stanford.edu/publications/ontology_development/ontology101-noy-mcguinness.html (accessed on 8 July 2020).
- Musen, M.A. The protégé project. AI Matters 2015, 1, 4–12. [Google Scholar] [CrossRef]
- Fowler, M. Patterns of Enterprise Application Architecture; Addison-Wesley: Boston, MA, USA, 2004. [Google Scholar]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Rodić-Trmčić, B.; Labus, A.; Barać, D.; Popović, S.; Radenković, B. Designing a course for smart healthcare engineering education. Comput. Appl. Eng. Educ. 2018, 26, 484–499. [Google Scholar] [CrossRef]
- Chan, K.L.; Chen, M. Effects of social media and mobile health apps on pregnancy care: Meta-analysis. JMIR mHealth uHealth 2019, 7, e11836. [Google Scholar] [CrossRef] [PubMed]
- Musgrave, L.M.; Kizirian, N.V.; Homer, C.S.E.; Gordon, A. Mobile Phone Apps in Australia for Improving Pregnancy Outcomes: Systematic Search on App Stores. JMIR mHealth uHealth 2020, 8, e22340. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Item | No. | % |
|---|---|---|---|
| Pregnant women (420) | |||
| Age | ≤25 | 64 | 15.23 |
| 25–35 | 196 | 46.67 | |
| 36+ | 160 | 38.1 | |
| Pregnancy (order number) | First | 144 | 34.29 |
| Second | 133 | 31.67 | |
| Third | 109 | 25.95 | |
| Forth | 34 | 8.1 | |
| Educational level | Secondary school | 114 | 27.14 |
| Vocational school | 89 | 21.19 | |
| University degree | 217 | 51.67 | |
| Gynaecologists (75) | |||
| Sex | Female | 45 | 60 |
| Male | 30 | 40 | |
| Age | ≤40 | 30 | 40 |
| 41–50 | 24 | 32 | |
| 51–60 | 14 | 18.67 | |
| 61+ | 7 | 9.33 | |
| Years of work experience in gynaecology | 0–10 | 23 | 30.67 |
| 11–20 | 34 | 45.33 | |
| 21+ | 18 | 24 |
| Indicator | Mean | SD | CI (Alpha = 0.05) |
|---|---|---|---|
| Readiness and potential of mobile technologies—pregnant women/doctors | |||
| How frequently do you use mobile technologies | 4.41 | 0.658 | 0.421 |
| 4.55 | 0.53 | 1.029 | |
| How frequently do you install mobile applications | 3.495 | 1.253 | 0.334 |
| 3.707 | 0.983 | 0.839 | |
| I am informed about the IoT concept and omnipresent technologies for measuring body parameters | 4.1 | 1.34 | 0.392 |
| 4.373 | 0.97 | 0.99 | |
| Health institutions should use mobile services and applications for communication with patients | 4.795 | 0.611 | 0.456 |
| 4.65 | 0.73 | 1.095 | |
| Acceptance of the application—pregnant women/doctors (adjusted TAM questions) | |||
| The applications is useful | 4.761 | 0.634 | 0.455 |
| 4.667 | 0.664 | 1.056 | |
| I would use the application again | 4.24 | 0.938 | 0.405 |
| 4.547 | 0.759 | 1.03 | |
| I think the application improves communication between pregnant woman and gynaecologist | 4.795 | 0.65 | 0.459 |
| 4.84 | 0.494 | 1.095 | |
| It is easy to find information and options within the application | 4.7 | 0.674 | 0.45 |
| 4.787 | 0.552 | 1.083 | |
| The application allows me to follow data related to the checks in an easier way | 4.681 | 0.802 | 0.416 |
| 4.773 | 0.534 | 1.08 | |
| The applications structures data related to the checks in the proper way | 4.642 | 0.709 | 0.444 |
| 4.707 | 0.564 | 1.065 | |
| IoT component would improve the application to a great extent | 4.662 | 0.754 | 0.433 |
| 4.707 | 0.653 | 1.065 | |
| The application’s flow suits me | 4.536 | 0.909 | 0.434 |
| 4.733 | 0.577 | 1.071 | |
| I would recommend the app to other pregnant women | 4.786 | 0.608 | 0.458 |
| 4.787 | 0.527 | 1.083 | |
| The application makes pregnancy care easier | 4.662 | 0.754 | 0.446 |
| 4.787 | 0.501 | 1.083 | |
| The app enables faster and more efficient treatment of the patients | 4.758 | 0.640 | 0.455 |
| 4.733333 | 0.578 | 1.083 | |
| All the important parameters from the checks are included within the application | / | / | / |
| 4.747 | 0.572 | 1.074 | |
| The application improves existing PHR | / | / | / |
| 4.867 | 0.476 | 1.101 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bjelica, D.; Bjelica, A.; Despotović-Zrakić, M.; Radenković, B.; Barać, D.; Đogatović, M. Designing an IT Ecosystem for Pregnancy Care Management Based on Pervasive Technologies. Healthcare 2021, 9, 12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010012
Bjelica D, Bjelica A, Despotović-Zrakić M, Radenković B, Barać D, Đogatović M. Designing an IT Ecosystem for Pregnancy Care Management Based on Pervasive Technologies. Healthcare. 2021; 9(1):12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010012
Chicago/Turabian StyleBjelica, Daniel, Artur Bjelica, Marijana Despotović-Zrakić, Božidar Radenković, Dušan Barać, and Marko Đogatović. 2021. "Designing an IT Ecosystem for Pregnancy Care Management Based on Pervasive Technologies" Healthcare 9, no. 1: 12. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010012