
Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Narrative Review
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction, Synthesis, and Analysis
2.4. Quality Assessment
3. Results
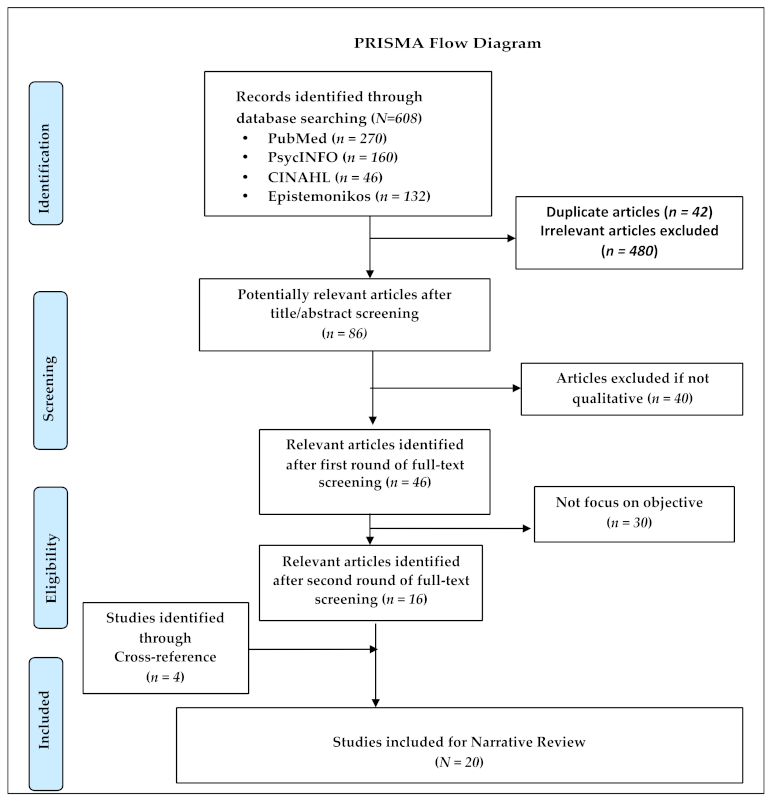
3.1. Study Selection and Characteristics
3.2. Theme 1: Maternal Health Services during an Emergency
3.2.1. Antenatal Check-Up
3.2.2. Delivery and Post-Natal Care
3.3. Theme 2: Child Health Services during an Emergency
3.3.1. Immunization Services for the Child
3.3.2. Management of Sick Infants
4. Discussion
4.1. Implication for Practice and Policy
4.2. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sobhy, S.; Arroyo-Manzano, D.; Murugesu, N.; Karthikeyan, G.; Kumar, V.; Kaur, I.; Fernandez, E.; Gundabattula, S.R.; Betran, A.P.; Khan, K.; et al. Maternal and perinatal mortality and complications associated with caesarean section in low-income and middle-income countries: A systematic review and meta-analysis. Lancet 2019, 393, 1973–1982. [Google Scholar] [CrossRef]
- World Health Organization. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Hug, L.; Alexander, M.; You, D.; Alkema, L. UIAG. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: A systematic analysis. Lancet Global Health 2019, 7, e710–e720. [Google Scholar]
- Story, W.T.; LeBan, K.; Altobelli, L.C.; Gebrian, B.; Hossain, J.; Lewis, J.; Morrow, M.; Nielsen, J.N.; Rosales, A.; Rubardt, M.; et al. Institutionalizing community-focused maternal, newborn, and child health strategies to strengthen health systems: A new framework for the sustainable development goal era. Glob. Health 2017, 13, 1–3. [Google Scholar]
- Girum, T.; Wasie, A. Correlates of maternal mortality in developing countries: An ecological study in 82 countries. Matern. Health Neonatol. Perinatol. 2017, 3, 1–6. [Google Scholar]
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef]
- Akseer, N.; Kandru, G.; Keats, E.C.; Bhutta, Z.A. COVID-19 pandemic and mitigation strategies: Implications for maternal and child health and nutrition. Am. J. Clin. Nutr. 2020, 112, 251–256. [Google Scholar] [CrossRef]
- Park, M.; Cook, A.R.; Lim, J.T.; Sun, Y.; Dickens, B.L. A systematic review of COVID-19 epidemiology based on current evidence. J. Clin. Med. 2020, 9, 967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pati, S.; Mahapatra, P.; Kanungo, S.; Uddin, A.; Sahoo, K.C. Managing Multimorbidity (Multiple Chronic Diseases) Amid COVID-19 Pandemic: A Community Based Study from Odisha, India. Front. Public Health 2021, 8, 1026. [Google Scholar] [CrossRef]
- Chen, Y.; Li, Z.; Zhang, Y.Y.; Zhao, W.H.; Yu, Z.Y. Maternal health care management during the outbreak of coronavirus disease 2019. J. Med. Virol. 2020, 92, 731–739. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.A.; Smulian, J.C.; Lednicky, J.A.; Wen, T.S.; Jamieson, D.J. Coronavirus disease 2019 (COVID-19) and pregnancy: What obstetricians need to know. Am. J. Obstet. Gynecol. 2020, 222, 415–426. [Google Scholar] [CrossRef]
- Kallem, V.R.; Sharma, D. COVID 19 in neonates. J. Matern. Fetal Neonatal Med. 2020, 1–9. [Google Scholar] [CrossRef]
- Sochas, L.; Channon, A.A.; Nam, S. Counting indirect crisis-related deaths in the context of a low-resilience health system: The case of maternal and neonatal health during the Ebola epidemic in Sierra Leone. Health Policy Plan. 2017, 32 (Suppl. 3), iii32–iii39. [Google Scholar] [CrossRef] [Green Version]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, A.S.M.; Dalal, K.; Halim, A.; Rahman, A.K.M.; Biswas, A. Effects of climate change and maternal morality: Perspective from case studies in the rural area of Bangladesh. Int. J. Environ. Res. Public Health 2019, 16, 4594. [Google Scholar] [CrossRef] [Green Version]
- Oluoch-Aridi, J.; Chelagat, T.; Nyikuri, M.M.; Onyango, J.; Guzman, D.; Makanga, C.; Miller-Graff, L.; Dowd, R. COVID-19 Effect on Access to Maternal Health Services in Kenya. Front. Glob. Women’s Health 2020, 1, 19. [Google Scholar]
- Bakouei, F.; Nikpour, M.; Rad, H.A.; Marzoni, Z.A. Exploration of the Pregnant Women’s Experiences during COVID-19 Disease Crisis: A Qualitative Study. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3634840 (accessed on 24 March 2021).
- Brunson, J. Maternal, newborn, and child health after the 2015 Nepal earthquakes: An investigation of the long-term gendered impacts of disasters. Matern. Child. Health J. 2017, 21, 2267–2273. [Google Scholar] [CrossRef]
- Dynes, M.M.; Miller, L.; Sam, T.; Vandi, M.A.; Tomczyk, B.; Centers for Disease Control and Prevention (CDC). Perceptions of the risk for Ebola and health facility use among health workers and pregnant and lactating women—Kenema District, Sierra Leone, September 2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 63, 1226–1227. [Google Scholar]
- Elston, J.W.T.; Moosa, A.J.; Moses, F.; Walker, G.; Dotta, N.; Waldman, R.J.; Wright, J. Impact of the Ebola outbreak on health systems and population health in Sierra Leone. J. Public Health 2016, 38, 673–678. [Google Scholar] [CrossRef] [Green Version]
- Fredricks, K.; Dinh, H.; Kusi, M.; Yogal, C.; Karmacharya, B.M.; Burke, T.F.; Nelson, B.D. Community health workers and disasters: Lessons learned from the 2015 earthquake in Nepal. Prehosp. Disaster. Med. 2017, 32, 604. [Google Scholar] [CrossRef]
- Gomez, H.M.; Mejia Arbelaez, C.; Ocampo Cañas, J.A. A qualitative study of the experiences of pregnant women in accessing healthcare services during the Zika virus epidemic in Villavicencio, Colombia, 2015–2016. Int. J. Gynecol. Obstet. 2020, 148, 29–35. [Google Scholar] [CrossRef]
- Jones, S.; Sam, B.; Bull, F.; Pieh, S.B.; Lambert, J.; Mgawadere, F.; Gopalakrishnan, S.; Ameh, C.A.; van den Broek, N. ‘Even when you are afraid, you stay’: Provision of maternity care during the Ebola virus epidemic: A qualitative study. Midwifery 2017, 52, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Linde-Arias, A.R.; Roura, M.; Siqueira, E. Solidarity, vulnerability and mistrust: How context, information and government affect the lives of women in times of Zika. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Lori, J.R.; Munro-Kramer, M.L.; Shifman, J.; Amarah, N.; Williams, G. Patient satisfaction with maternity waiting homes in Liberia: A case study during the Ebola outbreak. J. Midwifery Women’s Health 2017, 62, 163–171. [Google Scholar] [CrossRef]
- Lusambili, A.M.; Martini, M.; Abdirahman, F.; Asante, A.; Ochieng, S.; Guni, J.N.; Maina, R.; Luchters, S. “We have a lot of home deliveries” A qualitative study on the impact of COVID-19 on access to and utilization of reproductive, maternal, newborn and child health care among refugee women in urban Eastleigh, Kenya. J. Migr. Health 2020, 1, 100025. [Google Scholar] [CrossRef]
- Miller, N.P.; Milsom, P.; Johnson, G.; Bedford, J.; Kapeu, A.S.; Diallo, A.O.; Hassen, K.; Rafique, N.; Islam, K.; Camara, R. Community health workers during the Ebola outbreak in Guinea, Liberia, and Sierra Leone. J. Glob. Health 2018, 8. [Google Scholar] [CrossRef]
- Nidzvetska, S.; Rodriguez-Llanes, J.M.; Aujoulat, I.; Gil Cuesta, J.; Tappis, H.; Van Loenhout, J.A.; Guha-Sapir, D. Maternal and child health of internally displaced persons in Ukraine: A qualitative study. Int. J. Environ. Res. Public Health 2017, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- Pieterse, P.; Lodge, T. When free healthcare is not free. Corruption and mistrust in Sierra Leone’s primary healthcare system immediately prior to the Ebola outbreak. Int. Health 2015, 7, 400–404. [Google Scholar] [CrossRef]
- Saso, A.; Skirrow, H.; Kampmann, B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines 2020, 8, 556. [Google Scholar] [CrossRef]
- Sato, M.; Nakamura, Y.; Atogami, F.; Horiguchi, R.; Tamaki, R.; Yoshizawa, T.; Oshitani, H. Immediate needs and concerns among pregnant women during and after Typhoon Haiyan (Yolanda). PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- Semaan, A.; Audet, C.; Huysmans, E.; Afolabi, B.; Assarag, B.; Banke-Thomas, A.; Blencowe, H.; Caluwaerts, S.; Campbell, O.M.R.; Cavallaro, F.L.; et al. Voices from the frontline: Findings from a thematic analysis of a rapid online global survey of maternal and newborn health professionals facing the COVID-19 pandemic. BMJ Glob. Health 2020, 5, e002967. [Google Scholar] [CrossRef]
- Sohrabizadeh, S.; Jahangiri, K.; Jazani, R.K. Reproductive health in the recent disasters of Iran: A management perspective. BMC Public Health 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Theuring, S.; Koroma, A.P.; Harms, G. “In the hospital, there will be nobody to pamper me”: A qualitative assessment on barriers to facility-based delivery in post-Ebola Sierra Leone. Reprod. Health 2018, 15, 1–9. [Google Scholar] [CrossRef]
- Brolin Ribacke, K.J.; Saulnier, D.D.; Eriksson, A.; Von Schreeb, J. Effects of the West Africa Ebola virus disease on health-care utilization–a systematic review. Front. Public Health 2016, 4, 222. [Google Scholar] [CrossRef]
- Datar, A.; Liu, J.; Linnemayr, S.; Stecher, C. The impact of natural disasters on child health and investments in rural India. Soc. Sci. Med. 2013, 76, 83–91. [Google Scholar] [CrossRef]
- Nour, N.N. Maternal health considerations during disaster relief. Rev. Obstet. Gynecol. 2011, 4, 22. [Google Scholar] [PubMed]
- Quaglio, G.; Pizzol, D.; Bome, D.; Kebbie, A.; Bangura, Z.; Massaquoi, V.; Frasson, C.; Dalla Riva, D.; Putoto, G. Maintaining maternal and child health services during the Ebola outbreak: Experience from Pujehun, Sierra Leone. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- Harville, E.W.; Xiong, X.; Buekens, P. Disasters and perinatal health: A systematic review. Obstet. Gynecol. Surv. 2010, 65, 713. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author | Setting | Pandemic/Disaster | Study Participants | Data Collection Method | Analysis Method | Major Topic Discussed |
|---|---|---|---|---|---|---|
| Abdullah et al., 2019 [16] | Bangladesh | Flood | Healthcare Providers, Pregnant and postnatal women | Focus group discussions (n = 3), In-depth interviews (n = 8) | Content analysis | Maternal care |
| Aridi et al., 2020 [17] | Kenya | COVID-19 | Postnatal women | Telephonic interviews (n = 71) | Thematic analysis | Access to MCH services |
| Bakouei et al., 2020 [18] | Iran | COVID-19 | Pregnant women | Telephonic interviews (n = 12) | Content analysis | Pregnancy experience |
| Brunson, 2017 [19] | Nepal | Earthquake | Women | In-depth interviews (n = 14) | Thematic analysis | Maternal and Child Health |
| Dynes et al., 2015 [20] | Sierra Leone | Ebola | Healthcare workers, pregnant and lactating women | Focus group discussions (n = 9) | Content analysis | Antenatal care, Postnatal care and Immunization |
| Elston et al., 2015 [21] | Sierra Leone | Ebola outbreak | Local stakeholders, Community Health Workers, and Social mobilizers | Focus group discussions (n = 7), In-depth interviews (n = 60) | Thematic analysis | Maternal and Child Health |
| Fredricks et al., 2017 [22] | Nepal | Earthquake | Key Informants, Community Health Workers | Focus group discussions (n = 2), In-depth interviews (n = 17) | Thematic analysis | Maternal and Child Health |
| Gomez et al., 2020 [23] | Colombia | Zika virus | Women | In-depth interviews (n = 6) | Thematic analysis | Prenatal services |
| Jones et al., 2017 [24] | Sierra Leone | Ebola | Midwives, Medical staffs and Program Managers | In-depth interviews (n = 66) | Framework analysis | Maternal and Child Health |
| Linde-Arias et al., 2020 [25] | Brazil, Puerto Rico | Zika virus | Women | In-depth interviews (n = 24) | Thematic analysis | Social effects of pandemic on Maternal health |
| Lori et al., 2017 [26] | Liberia | Ebola | Traditional Birth Attendants, Certified midwives, Women | In-depth interviews (n = 21) | Content analysis | Maternal and Child Health |
| Lusambili et al., 2020 [27] | Kenya | COVID-19 | Healthcare staff, antenatal and postnatal refugees women | In-depth interviews (n = 25) | Thematic analysis | Barriers of MCH services utilization |
| Miller et al., 2018 [28] | Liberia | Ebola outbreak | Stakeholders | Focus group discussions (n = 16), in-depth interviews (n = 44) | Thematic analysis | Maternal and Child Health |
| Nidzvetska et al., 2017 [29] | Ukraine | Conflict | Mothers | In-depth interviews (n = 9) | Thematic analysis | Maternal and Child Health |
| Pieterse and Lodge, 2018 [30] | Sierra Leone | Ebola | Healthcare Providers | Focus group discussions (n = 3), In-depth interviews (n = 25) | Thematic analysis | Maternal and Child Health |
| Saso et al., 2020 [31] | Multi-countries | COVID-19 | Members of IMPRINT | Online survey (n = 48) | Thematic analysis | Immunization |
| Sato et al., 2016 [32] | Yolanda | Typhoon | Women | Focus group discussions (n = 4) | Content analysis | Maternal and Child Health |
| Semaaan et al., 2020 [33] | Global | COVID-19 | Healthcare professionals | Online survey (n = 714) | Thematic analysis | Maternity care |
| Sohrabizadeh et al., 2018 [34] | Iran | Disasters | Health workers and Experts | In-depth interviews (n = 22) | Content analysis | Maternal and Child Health |
| Theuring et al., 2018 [35] | Sierra Leone | Ebola | Providers, pregnant and postnatal women | Focus group discussions (n = 6) | Content analysis | Maternal and Child Health |
| Maternal Health Services | Emergency Situation | |
|---|---|---|
| Pandemic | Disaster | |
| Antenatal check-up |
|
|
| Delivery and Post Natal Care |
|
|
| Child Health Services | ||
| Immunization services for child |
|
|
| Management of sick infants |
|
|
| MCH Services | Pandemic (n = 14) | Disaster (n = 6) | ||||||
|---|---|---|---|---|---|---|---|---|
| Accessibility | Availability | Affordability | Acceptability | Accessibility | Availability | Affordability | Acceptability | |
| Maternal Health services | ||||||||
| Diagnostic services | SC | SC | SC | VC | VC | SC | NR | NR |
| Doctor consultation | SC | SC | SC | VC | VC | SC | VC | NC |
| Transportation | SC | SC | SC | VC | VC | VC | SC | NR |
| Drugs and consumables | SC | SC | SC | VC | SC | SC | SC | NC |
| Labor room/intra-natal | NR | NC | SC | VC | SC | SC | NR | NR |
| Hospital stay | NR | NC | SC | VC | SC | SC | SC | NR |
| Child health services | ||||||||
| Immunization | NR | SC | SC | VC | SC | NR | NR | NR |
| Doctor consultation | NR | NR | SC | VC | SC | VC | NR | NR |
| Transportation | NR | NR | NR | SC | SC | VC | NR | NR |
| Drugs and consumables | NR | SC | SC | SC | SC | VC | NR | NC |
| Diagnostic services | NR | NR | NR | SC | SC | SC | SC | NR |
| Hospital stay | NR | NR | NR | VC | SC | SC | NR | NR |
| Domains | Abdullah et al., 2019 [16] | Aridi et al., 2020 [17] | Bakouei et al., 2020 [18] | Brunson, 2017 [19] | Dynes et al., 2015 [20] | Elston et al., 2015 [21] | Fredricks et al., 2017 [22] | Gomez et al., 2020 [23] | Jones et al., 2017 [24] | Linde-Arias et al., 2020 [25] | Lori et al., 2017 [26] | Lusambili et al., 2020 [27] | Miller et al., 2018 [28] | Nidzvetska et al., 2017 [29] | Pieterse and Lodge, 2018 [30] | Saso et al., 2020 [31] | Sato et al., 2016 [32] | Semaan et al., 2020 [33] | Sohrabizadeh et al., 2018 [34] | Theuring et al., 2018 [35] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Research team and reflexivity | ||||||||||||||||||||
| Personal characteristics | ||||||||||||||||||||
| Interviewer | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Credentials | ● | ● | ● | ● | ● | ● | ● | ● | ● | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Occupation | × | ● | ● | × | × | ● | × | × | ● | × | ● | ● | × | × | × | ● | ● | ● | × | × |
| Gender | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | ● | × | × | ● |
| Experience and training | × | ● | ● | × | × | × | × | × | × | × | × | ● | ● | × | × | ● | ● | × | × | ● |
| Relationship with participants | ||||||||||||||||||||
| Relationship established | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Participant knowledge of the interviewer | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Interviewer characteristics | ● | ● | ● | ● | ● | ● | ● | ● | × | ● | ● | ● | ● | ● | ● | × | ● | ● | ● | ● |
| Study design | ||||||||||||||||||||
| Theoretical Framework | ||||||||||||||||||||
| Methodological orientation | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Participant selection | ||||||||||||||||||||
| Sampling | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Method of approach | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Sample size | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Non-participation | × | ● | × | × | × | × | × | ● | × | × | × | ● | × | ● | × | ● | × | ● | × | × |
| Setting | ||||||||||||||||||||
| Setting of data collection | ● | ● | ● | ● | ● | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Presence of non-participants | × | × | × | × | × | × | × | ● | × | × | × | ● | × | × | × | × | × | × | × | × |
| Description of sample | ● | ● | ● | × | ● | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Data collection | ||||||||||||||||||||
| Interview guide | ● | ● | ● | ● | ● | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Repeat interviews | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × |
| Audio/visual recording | ● | ● | ● | ● | × | × | ● | ● | ● | ● | ● | ● | ● | ● | × | × | ● | × | ● | ● |
| Field notes | ● | × | × | × | ● | × | × | ● | × | × | × | ● | ● | × | × | × | × | × | × | ● |
| Duration | ● | × | ● | ● | × | × | × | ● | ● | ● | × | × | × | ● | × | ● | ● | × | ● | ● |
| Data saturation | × | ● | ● | × | × | × | × | × | × | × | ● | ● | × | ● | × | × | ● | × | ● | ● |
| Transcripts returned | × | ● | ● | × | × | × | × | × | × | × | × | × | × | × | × | ● | ● | × | ● | × |
| Analysis and findings | ||||||||||||||||||||
| Number of data coders | ● | ● | × | × | × | × | ● | × | ● | ● | ● | ● | ● | × | × | ● | × | ● | × | ● |
| Descriptions of the coding | × | ● | ● | × | × | × | × | ● | × | ● | × | ● | × | × | × | ● | × | ● | × | × |
| Derivation of themes | ● | ● | ● | × | ● | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Software | × | ● | × | ● | × | × | ● | ● | ● | ● | × | ● | × | × | ● | × | × | × | × | × |
| Participant checking | × | ● | ● | × | × | × | × | × | × | × | × | × | × | × | × | × | × | × | ● | × |
| Reporting | ||||||||||||||||||||
| Quotations presented | ● | ● | ● | × | × | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Data and findings consistent | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Clarity of major themes | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Clarity of minor themes | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sahoo, K.C.; Negi, S.; Patel, K.; Mishra, B.K.; Palo, S.K.; Pati, S. Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review. Healthcare 2021, 9, 828. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070828
Sahoo KC, Negi S, Patel K, Mishra BK, Palo SK, Pati S. Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review. Healthcare. 2021; 9(7):828. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070828
Chicago/Turabian StyleSahoo, Krushna Chandra, Sapna Negi, Kripalini Patel, Bijaya Kumar Mishra, Subrata Kumar Palo, and Sanghamitra Pati. 2021. "Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review" Healthcare 9, no. 7: 828. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070828