
Neurological Manifestations and Outcomes in a Retrospective Cohort of Mexican Inpatients with SARS-CoV-2 Pneumonia: Design of a Risk Profile

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Demographic Characteristics
3.2. Medical History and Neurological Symptoms
3.3. Outcomes
3.4. Neurological Symptoms and Outcomes
3.5. Clinical Non-Neurological Conditions and Outcomes
4. Discussion
4.1. Non-Specific Neurological Symptoms in COVID-19
4.2. Neurological Complications
4.3. Development of Neurological Non-Specific Symptoms and Complications
4.4. Development of Comorbidities and Neurological Symptoms
4.5. Outcomes
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harapan, B.N.; Yoo, H.J. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef] [PubMed]
- Mapa en tiemp real de casos de coronavirus por Johns Hopkins School—CVOED—centro virtual de operaciones en emergencias y desastres. Available online: http://cvoed.imss.gob.mx/mapa_coronavirus/ (accessed on 27 August 2021).
- Tsatsakis, A.; Calina, D.; Falzone, L.; Petrakis, D.; Mitrut, R.; Siokas, V.; Pennisi, M.; Lanza, G.; Libra, M.; Doukas, S.G.; et al. SARS-CoV-2 pathophysiology and its clinical implications: An integrative overview of the pharmacotherapeutic management of COVID-19. Food Chem. Toxicol. 2020, 146, 111769. [Google Scholar] [CrossRef]
- Meppiel, E.; Peiffer-Smadja, N.; Maury, A.; Bekri, I.; Delorme, C.; Desestret, V.; Gorza, L.; Hautecloque-Raysz, G.; Landre, S.; Lannuzel, A.; et al. Neurologic manifestations associated with COVID-19: A multicentre registry. Clin Microbiol Infect. 2021, 27, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J. Neurological complications of coronavirus and COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar] [CrossRef]
- Zaffina, S.; Lanteri, P.; Gilardi, F.; Garbarino, S.; Santoro, A.; Vinci, M.R.; Carsetti, R.; Scorpecci, A.; Raponi, M.; Magnavita, N.; et al. Recurrence, Reactivation, or Inflammatory Rebound of SARS-CoV-2 Infection with Acute Vestibular Symptoms: A Case Report and Revision of Literature. Front. Hum. Neurosci. 2021, 15, 666468. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Beghi, E.; Helbok, R.; Moro, E.; Sampson, J.; Altamirano, V.; Mainali, S.; Bassetti, C.; Suarez, J.I.; McNett, M.; et al. Global incidence of neurological manifestations among patients hospitalized with COVID-19-A report for the GCS-NeuroCOVID Consortium and the ENERGY Consortium. JAMA Netw. Open 2021, 4, e2112131. [Google Scholar] [CrossRef]
- Inciarte, A.; Cardozo, C.; Chumbita, M.; Alcubilla, P.; Torres, B.; González Cordón, A.; Rico, V.; Aguero, D.; García-Pouton, N.; Hernández-Meneses, M.; et al. Gustatory and olfactory dysfunctions in hospitalised patients with COVID-19 pneumonia: A prospective study. BMJ 2021, 11, e040775. [Google Scholar] [CrossRef]
- Keyhanian, K.; Umeton, R.P.; Mohit, B.; Davoudi, V.; Hajighasemi, F.; Ghasemi, M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J. Neuroimmunol. 2020, 350, 577436. [Google Scholar] [CrossRef] [PubMed]
- Nersesjan, V.; Amiri, M.; Lebech, A.M.; Roed, C.; Mens, H.; Russell, L.; Fonsmark, L.; Berntsen, M.; Sigurdsson, S.T.; Carlsen, J.; et al. Central and peripheral nervous system complications of COVID-19: A prospective tertiary center cohort with 3-month follow-up. J. Neurol. 2021, 268, 3086–3104. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Neurological manifestations of COVID-19: A comprehensive literature review and discussion of mechanisms. J. Neuroimmunol. 2021, 358, 577658. [Google Scholar] [CrossRef]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in Health Care Workers during the COVID-19 Epidemic. A Cross-Sectional Survey. Int J Environ Res Public Health. 2020, 17, 5218. [Google Scholar] [CrossRef]
- Chirakkal, P.; Al Hail, A.N.; Zada, N.; Vijayakumar, D.S. COVID-19 and Tinnitus. Ear Nose Throat J. 2021, 100 (Suppl. 2), 160S–162S. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.; Qureshi, A.S.; Mohamed, S.A. Neurological Manifestations of COVID-19 in Absence of Respiratory Symptoms or Fever. Cureus. 2021, 13, e13887. [Google Scholar] [CrossRef]
- Schult-Montoya, S.C.; Pichilingue-Torres, P.R.; Vásquez-Vidal, W.L.; Rodríguez-Mujica, E.O.; Juárez-Luna, M. Manifestaciones neurológicas en pacientes pediátricos con COVID-19: Reporte de casos (Neurological manifestations in pediatric patients with COVID-19: Case report). Rev Peru Med Exp Salud Publica. 2021, 38, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Melegari, G.; Rivi, V.; Zelent, G.; Nasillo, V.; De Santis, E.; Melegari, A.; Bevilacqua, C.; Zoli, M.; Meletti, S.; Barbieri, A. Mild to Severe Neurological Manifestations of COVID-19: Cases Reports. Int J Environ Res Public Health. 2021, 18, 3673. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, M.; Lanza, G.; Falzone, L.; Fisicaro, F.; Ferri, R.; Bella, R. SARS-CoV-2 and the nervous system: From clinical features to molecular mechanisms. Int. J. Mol. Sci. 2020, 21, 5475. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Xiong, W.; Mu, J.; Guo, J.; Lu, L.; Liu, D.; Luo, J.; Li, N.; Liu, J.; Yang, D.; Gao, H.; et al. New onset neurologic events in people with COVID-19 in 3 regions in China. Neurology 2020, 95, e1479–e1487. [Google Scholar] [CrossRef]
- Karadaş, Ö.; Öztürk, B.; Sonkaya, A.R. A prospective clinical study of detailed neurological manifestations in patients with COVID-19. Neurol. Sci. 2020, 41, 1991–1995. [Google Scholar] [CrossRef] [PubMed]
- Kacem, I.; Gharbi, A.; Harizi, C.; Souissi, E.; Safer, M.; Nasri, A.; Letaief, H.; Akkari, M.; Hechaichi, A.; Mrabet, S.; et al. Characteristics, onset, and evolution of neurological symptoms in patients with COVID-19. Neurol. Sci. 2021, 42, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Travi, G.; Rossotti, R.; Merli, M.; D’Amico, F.; Chiappetta, S.; Giussani, G.; Panariello, A.; Corradin, M.; Vecchi, M.; Raimondi, A.; et al. Neurological manifestations in patients hospitalized with COVID-19: A retrospective analysis from a large cohort in Northern Italy. Eur. J. Neurosci. 2021, 53, 2912–2922. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.; Ou, C.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Benussi, A.; Pilotto, A.; Premi, E.; Libri, I.; Giunta, M.; Agosti, C.; Alberici, A.; Baldelli, E.; Benini, M.; Bonacina, S.; et al. Clinical characteristics and outcomes of inpatients with neurologic disease and COVID-19 in Brescia, Lombardy, Italy. Neurology 2020, 95, e910–e920. [Google Scholar] [CrossRef]
- Mahammedi, A.; Saba, L.; Vagal, A.; Leali, M.; Rossi, A.; Gaskill, M.; Sengupta, S.; Zhang, B.; Carriero, A.; Bachir, S.; et al. Imaging of neurologic disease in hospitalized patients with COVID-19: An Italian multicenter retrospective observational study. Radiology 2020, 297, E270–E273. [Google Scholar] [CrossRef]
- Khedr, E.M.; Abo-Elfetoh, N.; Deaf, E.; Hassan, H.M.; Amin, M.T.; Soliman, R.K.; Attia, A.A.; Zarzour, A.A.; Zain, M.; Mohamed-Hussein, A.; et al. Surveillance Study of Acute Neurological Manifestations among 439 Egyptian Patients with COVID-19 in Assiut and Aswan University Hospitals. Neuroepidemiology. 2021, 55, 109–118. [Google Scholar] [CrossRef]
- Altunisik, E.; Sayiner, H.S.; Aksoz, S.; Cil, E.; Ozgenc, G. Neurological symptoms in COVID-19 patien. Bratisl. Lek. Listy 2001, 122, 39–44. [Google Scholar] [CrossRef]
- Romero-Sánchez, C.M.; Díaz-Maroto, I.; Fernández-Díaz, E.; Sánchez-Larsen, Á.; Layos-Romero, A.; García-García, J.; González, E.; Redondo-Peñas, I.; Perona-Moratalla, A.B.; Del Valle-Pérez, J.A.; et al. Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry. Neurology 2020, 95, e1060–e1070. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef] [PubMed]
- Radmanesh, A.; Raz, E.; Zan, E.; Derman, A.; Kaminetzky, M. Brain imaging use and findings in COVID-19: A single academic center experience in the epicenter of disease in the United States. AJNR Am. J. Neuroradiol. 2020, 41, 1179–1183. [Google Scholar] [CrossRef]
- Liguori, C.; Pierantozzi, M.; Spanetta, M.; Sarmati, L.; Cesta, N.; Iannetta, M.; Ora, J.; Mina, G.G.; Puxeddu, E.; Balbi, O.; et al. Subjective neurological symptoms frequently occur in patients with SARS-CoV2 infection. Brain Behav. Immun. 2020, 88, 11–16. [Google Scholar] [CrossRef]
- Favas, T.T.; Dev, P.; Chaurasia, R.N.; Chakravarty, K.; Mishra, R.; Joshi, D.; Mishra, V.N.; Kumar, A.; Singh, V.K.; Pandey, M.; et al. Neurological manifestations of COVID-19: A systematic review and meta-analysis of proportions. Neurol. Sci. 2020, 41, 3437–3470. [Google Scholar] [CrossRef] [PubMed]
- Ahrenfeldt, L.J.; Otavova, M.; Christensen, K.; Lindahl-Jacobsen, R. Sex and age differences in COVID-19 mortality in Europe. Wiener klinische Wochenschrift. 2021, 133, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef]
- Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Sex differences in COVID-19: The role of androgens in disease severity and progression. Endocrine 2021, 71, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nature Comm. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; et al. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, W.S.; Kang, C.I.; Kim, Y.; Choi, J.P.; Joh, J.S.; Shin, H.S.; Kim, G.; Peck, K.R.; Chung, D.R.; Kim, H.; et al. Clinical presentation and outcomes of middle east respiratory syndrome in the Republic of Korea. Infect. Chemother. 2016, 48, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Chin, B.S.; Kang, C.K.; Kim, N.J.; Kang, Y.M.; Choi, J.P.; Oh, D.H.; Kim, J.H.; Koh, B.; Kim, S.E.; et al. Clinical course and outcomes of patients with severe acute respiratory syndrome coronavirus 2 infection: A preliminary report of the first 28 patients from the Korean cohort study on COVID-19. J. Korean Med. Sci. 2020, 35, e142. [Google Scholar] [CrossRef] [Green Version]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhong, Z.; Ji, P.; Li, H.; Li, B.; Pang, J.; Zhang, J.; Zhao, C. Clinicopathological characteristics of 8697 patients with COVID-19 in China: A meta-analysis. Fam. Med. Commun. Health 2020, 8, e000406. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; De Riu, G. Potential pathogenesis of ageusia and anosmia in COVID-19 patients. Int. Forum Allergy Rhinol. 2020, 10, 1103–1104. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in patients with severe acute respiratory coronavirus 2 infection: A cross-sectional study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [Green Version]
- Vaira, L.A.; Salzano, G.; Deiana, G.; De Riu, G. Anosmia and ageusia: Common findings in COVID-19 patients. Laryngoscope 2020, 130, 1787. [Google Scholar] [CrossRef] [Green Version]
- Saussez, S.; Lechien, J.R.; Hopkins, C. Anosmia: An evolution of our understanding of its importance in COVID-19 and what questions remain to be answered. Eur. Arch. Otorhinolaryngol. 2021, 278, 2187–2191. [Google Scholar] [CrossRef] [PubMed]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van Den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.J.; Fletcher, R.B.; et al. Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Tsuruoka, S.; Wakaumi, M.; Araki, N.; Ioka, T.; Sugimoto, K.; Fujimura, A. Comparative study of taste disturbance by losartan and perindopril in healthy volunteers. J. Clin. Pharmacol. 2005, 45, 1319–1323. [Google Scholar] [CrossRef]
- Suliburska, J.; Duda, G.; Pupek-Musialik, D. The influence of hypotensive drugs on the taste sensitivity in patients with primary hypertension. Acta Pol. Pharm. 2012, 69, 121–741. [Google Scholar]
- Aghagoli, G.; Gallo Marin, B.; Katchur, N.J.; Chaves-Sell, F.; Asaad, W.F.; Murphy, S.A. Neurological Involvement in COVID-19 and Potential Mechanisms: A Review. Neurocrit. Care 2021, 34, 1062–1071. [Google Scholar] [CrossRef]
- Park, Y.J.; Walls, A.C.; Wang, Z.; Sauer, M.M.; Li, W.; Tortorici, M.A.; Bosch, B.J.; DiMaio, F.; Veesler, D. Structures of MERS-CoV spike glycoprotein in complex with sialoside attachment receptors. Nat. Struct. Mol. Biol. 2019, 26, 1151–1157. [Google Scholar] [CrossRef] [Green Version]
- Milanetti, E.; Miotto, M.; Di Rienzo, L.; Monti, M.; Gosti, G.; Ruocco, G. In-Silico Evidence for Two Receptors Based Strategy of SARS-CoV-2. bioRxiv [Preprint] (2020). Available online: http://arxiv.org/abs/2003.11107 (accessed on 20 March 2021).
- Pushpass, R.G.; Pellicciotta, N.; Kelly, C.; Proctor, G.; Carpenter, G.H. Reduced salivary mucin binding and glycosylation in older adults influences taste in an in vitro cell model. Nutrients 2019, 11, 2280. [Google Scholar] [CrossRef] [Green Version]
- Dogra, S.; Jain, R.; Cao, M.; Bilaloglu, S.; Zagzag, D.; Hochman, S.; Lewis, A.; Melmed, K.; Hochman, K.; Horwitz, L.; et al. Hemorrhagic stroke and anticoagulation in COVID-19. J. Stroke Cerebrovasc. Dis. 2020, 29, 104984. [Google Scholar] [CrossRef]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5, 279–284. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, H.; Shen, H.; Li, Z.; Geng, J.; Han, H.; Cai, J.; Li, X.; Kang, W.; Weng, D.; et al. The clinical pathology of severe acute respiratory syndrome (SARS): A report from China. J. Pathol. 2003, 200, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Nannoni, S.; de Groot, R.; Bell, S.; Markus, H.S. Stroke in COVID-19: A systematic review and meta-analysis. J. Stroke 2021, 16, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-vessel stroke as a presenting feature of Covid-19 in the young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Zhang, J.; Wang, B.; Zhu, X.; Wang, Q.; Qiu, S. Analysis of clinical characteristics and laboratory findings of 95 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A retrospective analysis. Respir. Res. 2020, 21, 74. [Google Scholar] [CrossRef]
- Manousakis, G.; Jensen, M.B.; Chacon, M.R.; Sattin, J.A.; Levine, R.L. The interface between stroke and infectious disease: Infectious diseases leading to stroke and infections complicating stroke. Curr. Neurol. Neurosci. Rep. 2009, 9, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A. COVID-19: Current understanding of its pathophysiology, clinical presentation and treatment. Postgrad. Med. J. 2021, 97, 312–320. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.Y.; Xu, X.X.; Yin, H.S.; Hu, Q.M.; Xiong, T.; Tang, Y.Y.; Yang, A.Y.; Yu, B.P.; Huang, Z.P. Clinical characteristics of patients with 2019 coronavirus disease in a non-Wuhan area of Hubei Province, China: A retrospective study. BMC Infect. Dis. 2020, 20, 311. [Google Scholar] [CrossRef] [PubMed]
- Beach, S.R.; Praschan, N.C.; Hogan, C.; Dotson, S.; Merideth, F.; Kontos, N.; Fricchione, G.L.; Smith, F.A. Delirium in COVID-19: A case series and exploration of potential mechanisms for central nervous system involvement. Gen. Hosp. Psychiatry 2020, 65, 47–53. [Google Scholar] [CrossRef]
- Alkeridy, W.A.; Almaghlouth, I.; Alrashed, R.; Alayed, K.; Binkhamis, K.; Alsharidi, A.; Liu-Ambrose, T. A unique presentation of delirium in a patient with otherwise asymptomatic COVID-19. J. Am. Geriatr. Soc. 2020, 68, 1382–1384. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Paliwal, V.K.; Gupta, A. Encephalopathy in patients with COVID-19: A review. J. Med. Virol. 2021, 93, 206–222. [Google Scholar] [CrossRef]
- Zubair, A.S.; McAlpine, L.S.; Gardin, T.; Farhadian, S.; Kuruvilla, D.E.; Spudich, S. Neuropathogenesis and neurologic manifestations of the coronaviruses in the age of coronavirus disease 2019: A review. JAMA Neurol. 2020, 77, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, G.; Danti, S.; Nuti, A.; Carlesi, C.; Lucetti, C.; Di Fiorino, M. A complication of coronavirus disease 2019: Delirium. Acta Neurol. Belg. 2020, 120, 927–932. [Google Scholar] [CrossRef]
- Bagnato, S.; Boccagni, C.; Marino, G.; Prestandrea, C.; D’Agostino, T.; Rubino, F. Critical illness myopathy after COVID-19. Int. J. Infect. Dis. 2020, 99, 276–278. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, C.; Sun, Y.; Huang, W.; Ye, K. Cognitive disorders associated with hospitalization of COVID-19: Results from an observational cohort study. Brain Behav. Immun. 2021, 91, 383–392. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Q.; Zhang, P.; Sun, R.; Jiang, H.; Wan, J.; Wu, F.; Wang, X.; Tao, X. Prevalence and risk factors for intensive care unit acquired weakness: A protocol for a systematic review and meta-analysis. Medicine 2020, 99, e22013. [Google Scholar] [CrossRef]
- Yachou, Y.; El Idrissi, A.; Belapasov, V.; Ait Benali, S. Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2: Understanding the neurological manifestations in COVID-19 patients. Neurol. Sci. 2020, 41, 2657–2669. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Deeb, A.M.; Al-Hameed, F.; Mandourah, Y.; Almekhlafi, G.A.; Sindi, A.A.; Al-Omari, A.; Shalhoub, S.; Mady, A.; Alraddadi, B.; et al. Macrolides in critically ill patients with Middle East respiratory syndrome. Int. J. Infect. Dis. 2019, 81, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algahtani, H.; Subahi, A.; Shirah, B. Neurological complications of Middle East respiratory syndrome coronavirus: A report of two cases and review of the literature. Case Rep. Neurol. Med. 2016, 2016, 3502683. [Google Scholar] [CrossRef] [Green Version]
- Guidon, A.C.; Amato, A.A. COVID-19 and neuromuscular disorders. Neurology 2020, 94, 959–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N.; et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Lyons, S.; O’Kelly, B.; Woods, S.; Rowan, C.; Brady, D.; Sheehan, G.; Smyth, S. Seizure with CSF lymphocytosis as a presenting feature of COVID-19 in an otherwise healthy young man. Seizure 2020, 80, 113–114. [Google Scholar] [CrossRef]
- Elgamasy, S.; Kamel, M.G.; Ghozy, S.; Khalil, A.; Morra, M.E.; Islam, S.M. First case of focal epilepsy associated with SARS-coronavirus-2. J. Med. Virol. 2020, 92, 2238–2242. [Google Scholar] [CrossRef]
- Sohal, S.; Mansur, M. COVID-19 presenting with seizures. IDCases 2020, 20, e00782. [Google Scholar] [CrossRef]
- Somani, S.; Pati, S.; Gaston, T.; Chitlangia, A.; Agnihotri, S. De novo status epilepticus in patients with COVID-19. Ann. Clin. Transl. Neurol. 2020, 7, 1240–1244. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Simani, L.; Shahisavandi, M.; Barzegar, Z. ( COVID-19, de novo seizures, and epilepsy: A systematic review. Neurol. Sci. 2021, 42, 415–431. [Google Scholar] [CrossRef] [PubMed]
- Iaconetta, G.; De Luca, P.; Scarpa, A.; Cassandro, C.; Cassandro, E. Meningoencephalitis associated with SARS-Coronavirus-2. Transl, Med, UniSa. 2020, 23, 42–47. [Google Scholar] [CrossRef]
- Choudhary, S.; Sharma, K.; Silakari, O. The interplay between inflammatory pathways and COVID-19: A critical review on pathogenesis and therapeutic options. Microb. Pathog. 2021, 150, 104673. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; Pesce, M.; Seguella, L.; Sanseverino, W.; Lu, J.; Sarnelli, G. Can the enteric nervous system be an alternative entrance door in SARS-CoV2 neuroinvasion? Brain Behav. Immun. 2020, 87, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Pinho, M.; Raj, K.; Yu, F.F.; Bathla, G.; Achilleos, M.; ONeill, T.; Still, M.; Maldjian, J. Neurological emergencies associated with COVID-19: Stroke and beyond. Emerg. Radiol. 2020, 27, 747–754. [Google Scholar] [CrossRef]
- Belvis, R. Headaches during COVID-19: My clinical case and review of the literature. Headache 2020, 60, 1422–1426. [Google Scholar] [CrossRef]
- He, Y.; Bai, X.; Zhu, T.; Huang, J.; Zhang, H. What can the neurological manifestations of COVID-19 tell us: A meta-analysis. J. Transl. Med. 2021, 19, 363. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its impact on patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1–8. [Google Scholar] [CrossRef]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.; Ahmed, Z.; Younas, S. COVID-19 and comorbidities: Deleterious impact on infected patients. J. Infect. Public Health. 2020, 13, 1833–1839. [Google Scholar] [CrossRef]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef]
- Abu-Rumeileh, S.; Abdelhak, A.; Foschi, M.; Tumani, H.; Otto, M. Guillain–Barré syndrome spectrum associated with COVID-19: An up-to-date systematic review of 73 cases. J. Neurol. 2021, 268, 1133–1370. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Comorbidity | Total | n (%) | Neurological Symptoms n (%) | p Value | OR | 95% CI |
|---|---|---|---|---|---|---|
| Arterial hypertension | 1040 | 440 (42.30) | 388 (88.81) | 0.81 | 0.99 | 0.932–1.057 |
| Diabetes mellitus | 1040 | 403 (38.74) | 323 (80.14) | 0.69 | 1.015 | 0.953–1.081 |
| Obesity | 1039 | 638 (61.34) | 507 (79.46) | 1 | 1.001 | 0.94–1.067 |
| Grade 1 | 634 | 209 (32.96) | 173 (82.77) | 0.90 | -- | -- |
| Grade 2 | 634 | 273 (43.05) | 206 (75.45) | -- | -- | |
| Grade 3 | 634 | 152 (23.97) | 125 (82.83) | -- | -- | |
| COPD | 1040 | 33 (3.17) | 32 (96.96) | 0.007 | 1.23 | 1.149–1.317 |
| Asthma | 1040 | 21 (2.01) | 19 (90.47) | 0.2 | 1.142 | 0.991–1.317 |
| Neurological Symptoms | Total | Male/Female | p Value | OR | 95% CI |
|---|---|---|---|---|---|
| All neurological symptoms | 826 | 512/314 | 0.621 | 0.621 | 0.446–0.864 |
| One neurological symptom | 359 | 208/151 | 0.003 | 0.666 | 0.512–0.867 |
| Two neurological symptoms | 257 | 165/92 | 1 | 1.004 | 0.748–1.347 |
| Three or more neurological symptoms | 210 | 140/72 | 0.522 | 1.113 | 0.810–1.529 |
| Headache | 666 | 399/267 | 0.001 | 0.591 | 0.450–0.777 |
| Anosmia | 266 | 172/94 | 0.882 | 1.031 | 0.771–1.380 |
| Ageusia | 264 | 182/82 | 0.063 | 1.332 | 0.998–1.795 |
| Myopathy | 232 | 162/70 | 0.043 | 1.389 | 1.014–1.902 |
| Disorientation | 123 | 90/33 | 0.028 | 1.607 | 1.055–2.448 |
| Encephalopathy | 101 | 76/25 | 0.016 | 1.790 | 1.118–2.867 |
| Neuropathy | 45 | 34/11 | 0.114 | 1.768 | 0.885–3.531 |
| Stroke | 11 | 5/6 | 0.216 | 0.462 | 0.140–1.524 |
| Seizures | 11 | 5/6 | 0.218 | 0.467 | 0.141–1.540 |
| Cerebral hemorrhage | 9 | 6/3 | 1 | 1.120 | 0.278–4.502 |
| Encephalitis | 7 | 4/3 | 0.706 | 0.744 | 0.166–3.343 |
| Cerebral venous thrombosis | 3 | 0/3 | 0.46 | -- | -- |
| Subarachnoid hemorrhage | 2 | 2/0 | 0.540 | -- | -- |
| With Neurological Symptoms (n = 826) | Without Neurological Symptoms (n = 214) | p Value | |
|---|---|---|---|
| O2 saturation at admission (%) | 83.3 ± 13.17 | 84.51 ± 11.73 | 0.122 |
| Symptoms duration before admission (hours) | 179.08 ± 125.112 | 162.07 ± 114.597 | 0.381 |
| Hospital stay (days) | 13.06 ± 11.391 | 10.37 ± 6.718 | 0.001 |
| Data at admission Leukocytes (cells per mm2) Lymphocytes (cells per mm2) Platelets (cells per mm2) Plasma glucose (mg/dL) Plasma sodium (mEq/L) Plasma creatinine (mg/dL) BUN (mg/dL) Plasma C-reactive protein (mg/dL) Plasma D-dimer (μg/mL) Plasma ferritin (ng/mL) Plasma fibrinogen (mg/dL) | 9109.547 ± 4795.254 1202.938 ± 1149.151 233369.829 ± 100659.543 135.724 ± 75.294 138.08 ± 4.778 1.213 ± 1.541 23.799 ± 20.041 113.039 ± 95.982 4.584 ± 22.327 1078.132 ± 1219.426 510.623 ± 169.637 | 9053.545 ± 4244.95 1098.591 ± 614.295 250575 ± 98015.044 130.121 ± 66.693 137.234 ± 10.202 1.13 ± 1.392 22.402 ± 19.407 118.202 ± 101.831 2.699 ± 5.447 1209.628 ± 1780.672 550.259 ± 376.028 | 0.091 0.144 0.497 0.165 0.138 0.254 0.256 0.408 0.074 0.215 0.508 |
| Wost data during hospitalization Plasma creatinine (mg/dL) BUN (mg/dL) Plasma C-reactive protein (mg/dL) Plasma D-dimer (μg/mL) Plasma ferritin (ng/mL) Plasma fibrinogen (mg/dL) | 1.488 ± 1.973 30.298 ± 31.362 99.389 ± 99.746 6.392 ± 25.452 1548.107 ± 3796.142 493.983 ± 170.579 | 1.374 ± 1.555 30.949 ± 37.025 97.915 ± 102.012 8.889 ± 32.111 1241.529 ± 1159.54 505.096 ± 117.984 | 0.105 0.410 0.766 0.130 0.408 0.026 |
| Type of Clinical Outcome at Hospital Discharge | ||||||
|---|---|---|---|---|---|---|
| Asymptomatic | Only Respiratory Symptoms | Only Neurological Symptoms | Neurological and Respiratory Symptoms | Death | p Value | |
| Neurological Symptoms during hospitalization Headache | 166 | 242 | 5 | 43 | 210 | 0.108 |
| Encephalopathy | 9 | 16 | 3 | 24 | 49 | <0.001 |
| Ageusia | 53 | 92 | 4 | 29 | 86 | <0.001 |
| Anosmia | 61 | 92 | 4 | 27 | 82 | 0.001 |
| Disorientation | 11 | 18 | 3 | 26 | 65 | <0.001 |
| Neuropathy | 0 | 5 | 2 | 17 | 21 | <0.001 |
| Myopathy | 7 | 104 | 5 | 36 | 80 | <0.001 |
| Stroke | 1 | 4 | 1 | 1 | 4 | 0.039 |
| Seizures | 2 | 5 | 0 | 1 | 3 | 0.953 |
| Comorbidity | N (%) | 1 | 2 | 3 | 4 | 5 | p Value |
|---|---|---|---|---|---|---|---|
| Arterial hypertension | 440 (42.30) | 73 | 164 | 3 | 25 | 175 | <0.001 |
| Diabetes mellitus | 403 (38.74) | 66 | 149 | 1 | 28 | 159 | <0.001 |
| Obesity | 638 (61.34) | 131 | 273 | 2 | 33 | 200 | 0.001 |
| Grade 1 | 209 (32.96) | 58 | 78 | 1 | 13 | 59 | 0.026 |
| Grade 2 | 273 (43.05) | 48 | 130 | 1 | 13 | 81 | |
| Grade 3 | 152 (23.97) | 23 | 63 | 0 | 6 | 60 | |
| Chronic obstructive pulmonary disease | 33 (3.17) | 3 | 4 | 0 | 2 | 24 | <0.001 |
| Asthma | 21 (2.01) | 7 | 7 | 1 | 1 | 5 | 0.270 |
| Factors Associated with Neurological Symptoms | p Value | Analysis |
|---|---|---|
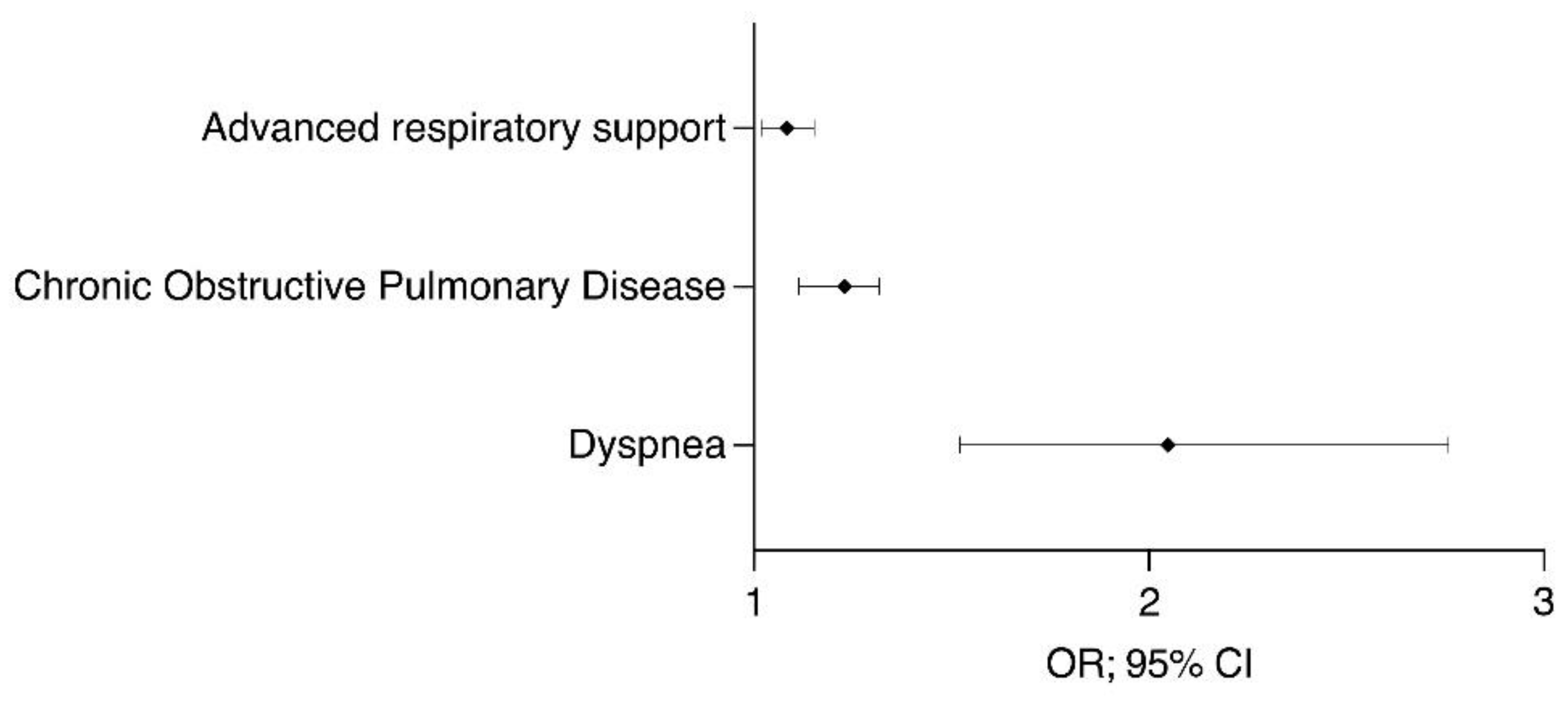
| Dyspnea | 0.0001 | OR; 95% CI 2.048; (1.522–2.7579) |
| Chronic obstructive pulmonary disease | 0.0070 | 1.23; (1.114–1.317) |
| Advanced respiratory support | 0.0200 | 1.084; (1.018–1.153) |
| Mean Difference | ||
| * Prolonged hospitalization | 0.0001 | 13.18 ± 12.69 vs. 10.37 ± 6.72 |
| * Worst fibrinogen level (mg/dL) | 0.0260 | 493.981 ± 70.58 vs. 505.10 ± 17.98 |
| Factors associated with death | ||
| OR; 95% CI | ||
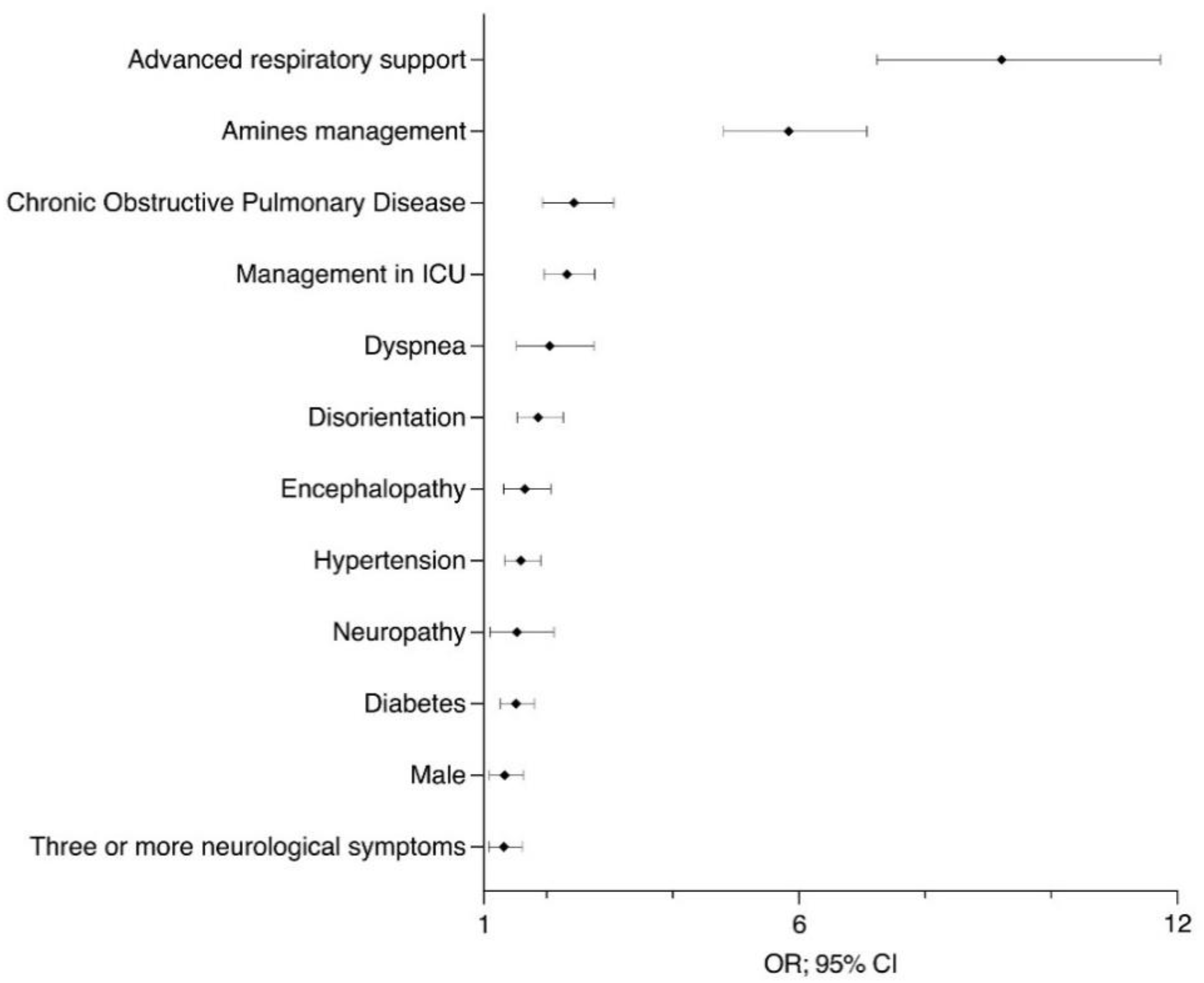
| Advanced respiratory support | 0.0001 | 9.212; (7.234–11.730) |
| Amine management | 0.0001 | 5.835; (4.804–7.087) |
| Chronic obstructive pulmonary disease | 0.0001 | 2.433; (1.934–3.060) |
| Management in intensive care unit | 0.0001 | 2.322; (1.952–2.761) |
| Dyspnea | 0.0001 | 2.048; (1.522–2.757) |
| Disorientation | 0.0001 | 1.864; (1.532–2.268) |
| Encephalopathy | 0.0001 | 1.651; (1.319–2.065) |
| Hypertension | 0.0001 | 1.591; (1.329–1.905) |
| Neuropathy | 0.0300 | 1.527; (1.102–2.116) |
| Diabetes | 0.0001 | 1.514; (1.267–1.809) |
| Male sex | 0.0040 | 1.334; (1.090- 1.632) |
| Three or more neurological symptoms | 0.0100 | 1.322; (1.082–1.614) |
| Obesity grade 3 | 0.0231 | 1.533; (1.074–2.188) |
| Mean Difference | ||
| * Older age | 0.0001 | 61.63 ± 12.57 vs. 52.68 ± 14.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, S.; Cuatepotzo-Burgos, F.M.; Toledo-Lozano, C.G.; Balderrama-Soto, A.; Alcaraz-Estrada, S.L.; Montiel-López, L.; De la Vega-Bravo, A.H.; Mondragón-Terán, P.; Santosbeña-Lagunes, M.; Escarela-Serrano, M.; et al. Neurological Manifestations and Outcomes in a Retrospective Cohort of Mexican Inpatients with SARS-CoV-2 Pneumonia: Design of a Risk Profile. Healthcare 2021, 9, 1501. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111501
García S, Cuatepotzo-Burgos FM, Toledo-Lozano CG, Balderrama-Soto A, Alcaraz-Estrada SL, Montiel-López L, De la Vega-Bravo AH, Mondragón-Terán P, Santosbeña-Lagunes M, Escarela-Serrano M, et al. Neurological Manifestations and Outcomes in a Retrospective Cohort of Mexican Inpatients with SARS-CoV-2 Pneumonia: Design of a Risk Profile. Healthcare. 2021; 9(11):1501. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111501
Chicago/Turabian StyleGarcía, Silvia, Francisco Manuel Cuatepotzo-Burgos, Christian Gabriel Toledo-Lozano, Adriana Balderrama-Soto, Sofía Lizeth Alcaraz-Estrada, Luis Montiel-López, Alberto Hilarión De la Vega-Bravo, Paul Mondragón-Terán, Maribel Santosbeña-Lagunes, Maricela Escarela-Serrano, and et al. 2021. "Neurological Manifestations and Outcomes in a Retrospective Cohort of Mexican Inpatients with SARS-CoV-2 Pneumonia: Design of a Risk Profile" Healthcare 9, no. 11: 1501. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9111501