
Allogeneic Stem Cell Transplantation for MDS


1
Hematology Department, Clinica Universidad de Navarra, 31008 Pamplona, Spain
2
Hématologie-Greffe, Hôpital Saint-Louis, APHP, 75010 Paris, France
*
Author to whom correspondence should be addressed.
Hemato 2021, 2(3), 545-555; https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2030034
Submission received: 31 May 2021
/
Revised: 4 August 2021
/
Accepted: 10 August 2021
/
Published: 25 August 2021
(This article belongs to the Special Issue Challenges in the Treatment of Myelodysplastic Syndrome)
{kind=link}
{kind=link}
Abstract
:Myelodysplastic syndromes are clonal disorders with morphological dysplasia, a variable degree of cytopenia and a risk of transformation to acute myeloid leukemia. Prognosis is very variable and is defined by blast count, cytopenia, cytogenetics and more recently by somatic mutations, with IPSS or revised IPSS score being the most widely used to assess disease risk. HSCT remains the only curative treatment to date, with high-risk patients obtaining the biggest benefit. However, NRM should be carefully assessed before indicating the transplant in this usually old population, where organ toxicity and comorbid conditions are to be considered. Multi-domain assessment tools, such as CGA (comprehensive geriatric assessment) and EBMT score, are useful in this context and might guide physician decisions regarding the transplant. Indeed, with the development of reduced intensity conditioning regimens, the number of patient candidates for an HSCT has increased. Regarding pre-transplant treatment, patients with a blast excess > 10% might be treated with HMAs or chemotherapy, although there are no randomized trials confirming the benefit of this approach, even when achieving a complete response. Concerning donor choice, matched sibling donors continue to be the first option, although matched unrelated donors, and more recently haploidentical donors, have proven to be valid options and should be offered in the absence of a related donor. Relapse remains the main cause of transplantation failure. MRD assessment and pre-emptive or prophylactic use of HMA or other targeted inhibitors with or without DLI are accepted strategies to reduce relapse risk, but the prognosis in this context remains dismal, and is the subject for several ongoing clinical protocols.
1. Introduction
Myelodysplastic syndromes (MDS) are characterized by dysplastic morphology of hematopoietic cells associated with clonal hematopoiesis, peripheral blood cytopenia, and a propensity to progress to acute myeloid leukemia. The disease course is variable, mainly conditioned by molecular alterations, marrow blast count, and cytopenia [1,2,3,4,5]. Transformation into acute leukemia is the main cause of death in patients with higher risk MDS. Hematopoietic stem cell transplantation (HSCT) remains, to date, the only potentially curative therapy, albeit with a treatment-related mortality between 15 and 50%, according to specific risk factors [6,7,8]. Furthermore, only young and fit patients can be candidates for HSCT, due to higher mortality in the elderly and in patients with major comorbidities. The optimal timing of HSCT should take into account life expectancy without HSCT and quality of life. Some low-risk patients with persistent disease might live for years with supportive therapy and a relatively good quality of life. Hypomethylating agents (HMAs) have been reported to increase median survival and decrease transformation into leukemia in higher risk patients, and should be balanced with the potential effect of transplantation [9]. On the other hand, the development of less toxic conditioning regimens has expanded the indication to HSCT to older or more fragile patients previously not eligible for transplantation. Pre-transplant therapy remains a matter of debate. Indeed, marrow blast percentage is a risk factor for disease progression, but there is no randomized trial demonstrating a benefit for pre-transplant cytoreduction. This review will detail the current evidence for transplant strategies in MDS patients.
2. Patient Consideration
Chronological age alone is not reliable enough to consider HSCT eligibility. Some relatively old patients have a relatively good outcome after HSCT, and some authors have reported that this is not an obstacle to transplantation [8,10]. As MDS patients are usually older than 60 years, the probability of non-relapse mortality (NRM) in this fragile population should be precisely estimated. In the EBMT study including 1245 MDS patients [8], older age and a higher number of comorbidities were associated with higher mortality. Comorbidity index has shown to impact the outcome in all categories of age, including the elderly [11,12]. Recently, multi-domain assessment tools have also been tested, especially in patients older than 50 or 60 years, to better estimate the risk of post-transplant morbidity and mortality [13]. Domains usually assessed include physical fitness, auto-nomy and dependence, cognitive performance, social and professional insertion, moods and psychological well-being, nutrition, and inflammation. This multi-domain assessment has been regularly tested in the geriatric setting and is called “comprehensive geriatric assessment” (CGA). CGA has been reported to be associated with mortality in cancer patients and, more recently, in transplanted patients, and could guide physicians in their decisions regarding invasive treatments. This CGA is also applied to younger patients in the setting of transplantation, thus CGA may be useful to determinate a physiological age and help the physician take the decision for transplantation.
3. MDS Consideration
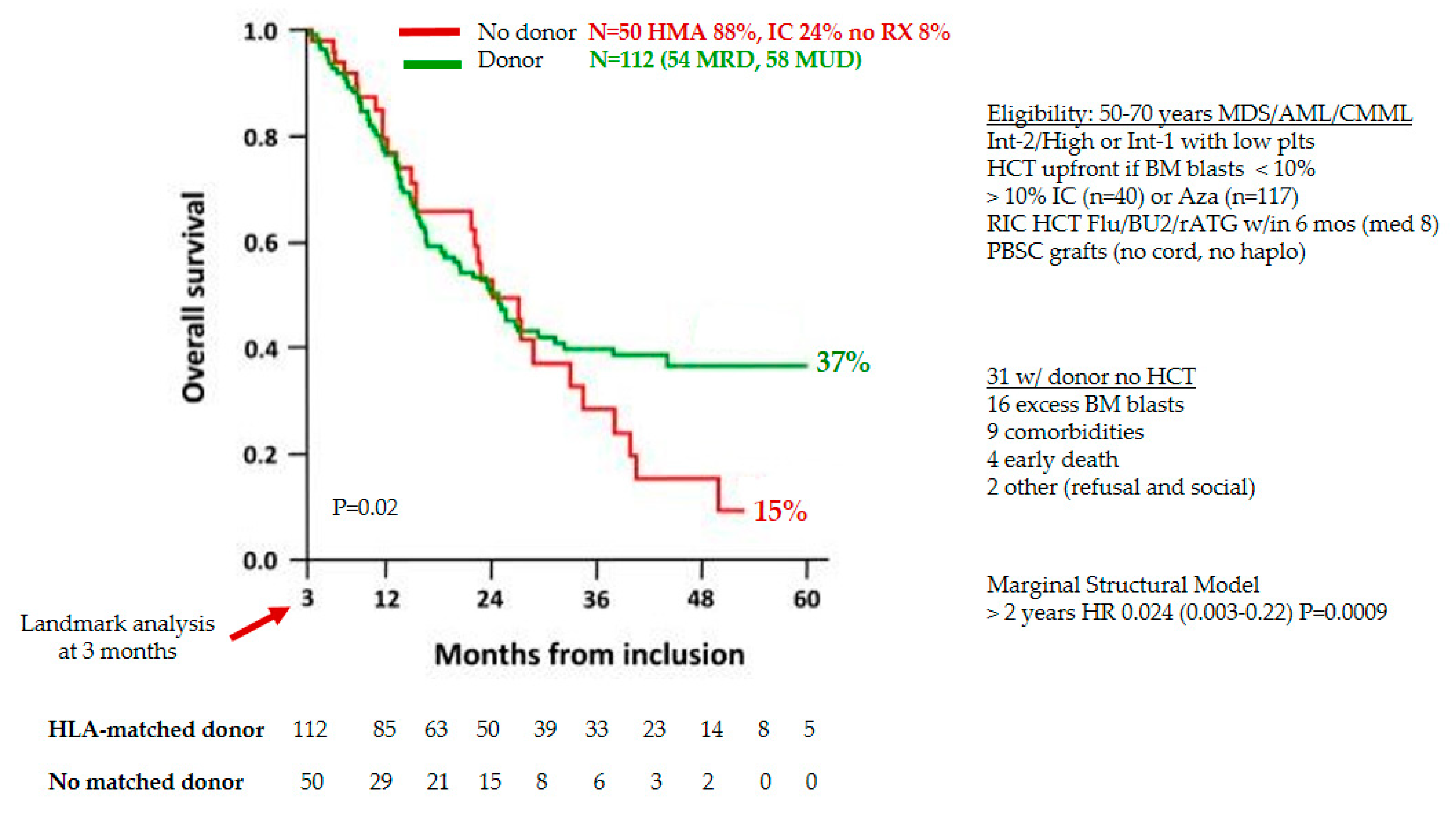
HSCT is an established curative treatment in MDS patients. However, the risk of disease progression without such a treatment and the NRM after transplantation should be carefully balanced before indicating this procedure. According to standard or revised international prognostic scoring system (IPSS), different categories distinguished patients from low risk, with median survival longer than 10 years, to very high risk, with median survival of a few months [1,2]. The indication for transplantation relies on the estimation of mortality with or without HSCT. The NRM post-transplantation is usually greater than 15% in the best series and mortality mainly occurs within the first 2 years post-transplantation. Higher risk MDS patients (intermediate-2 and high) have an estimated mortality much higher than 15% at 2 years, suggesting that they may have a better outcome with HSCT. Registry studies raised the question of the potential benefit of transplantation comparing transplant and non-transplant cohorts. Specific statistics have been carried out to overcome all bias due to registry studies. Of note, transplant cohorts include patients who received transplantation only, meaning that patients had to be alive between diagnosis and transplantation, which is a major bias. Patients who are transplanted usually have a higher risk, but a better general performance status, than non-transplanted patients. Furthermore, the disease risk in main comparative studies is usually assessed by IPSS, but does not take into account other risk factors such as somatic mutations, marrow fibrosis, heavy transfusion requirement, previous infections, or complications, which have an impact on prognosis. The first comparative study published in 2004 by Cutler et al. included relatively young patients, transplanted from HLA matched sibling donors after a myeloablative conditioning regimen. It was shown that there was a survival benefit in higher risk patients (intermediate-2 and high risk according to classical IPSS) when transplantation was performed upfront, while there was a detrimental effect in lower risk patients (low and intermediate-1) [14]. It has been reported later that this was also true for older patients receiving a reduced intensity conditioning regimen in comparison to patients who received HMA [15,16]. In addition, a national prospective study including patients at the time of transplantation indication has reported a significant advantage of survival in higher risk patients who received transplantation, especially after 2 years of follow up (Figure 1) [17].
The role of somatic mutations in these comparative studies has not been evaluated, while their prognostic value has recently taken more and more room [5,18,19,20,21]. Somatic mutations have an impact in all categories of disease risk, especially for TP53, RUNX1, ASXL1, DNMT3A, TET2, and RAS-pathway mutations. Indeed, it has been reported that lower risk patients who harbored some poor risk mutations have superimposable survivals to higher risk patients. Some prognostic classifications have integrated somatic mutations in order to better assess patients risk, but had not been widely reproduced yet [22,23]. In higher risk patients, it has been reported that patients harboring very poor cytogenetics (complex or monosomal karyotype) or TP53 mutations have a very high probability of relapse after transplantation, leading to a poor survival rate of less than 15% at long-term [20,21,24,25]. That is an additional issue to think about when considering transplantation strategies in these patients to improve their outcome.
Transplantation in Lower Risk MDS
In lower risk patients, allogeneic transplantation indication is still controversial, as there are no prospective studies regarding this issue [26]. In this group of patients, NRM remains the main cause of treatment failure [27]. However, in young patients with pejorative factors, HSCT might be indicated. These factors are mainly somatic mutations (TP53, ASXL1, and RUNX1), marrow fibrosis (grade 2 or more), very poor cytogenetics, relapse or refractoriness to standard therapies, therapy related MDS, and profound or symptomatic cytopenia [26]. Nevertheless, more studies are needed to explore the role of HSCT in these patients.
4. The Role of Pre-Graft MDS Therapy
International recommendations, based on registry studies, have highlighted that marrow blast count, especially if higher than 10%, is a risk factor of post-transplant relapse and mortality [28]. Many efforts have been made to reduce this marrow blastosis with chemotherapy or HMA. Nevertheless, there is no randomized trial showing that pre-graft therapy reduces relapse risk in MDS patients. One can argue this is because patients do not frequently achieve complete remission (CR), but even when patients are in CR, the prognosis is not improved [29,30]. The role of pre-transplant remission in acute myeloblastic leukemia (AML) has been largely demonstrated, as well as molecular remission, but this is not the case in MDS [31,32]. Minimal residual disease in MDS patients is unfrequently measurable and unfrequently negative when measured, even in patients in CR, as shown by the persistence of somatic mutations detection before HSCT, including patients in CR [20,21,25]. One hypothesis may be that the persistence of molecular disease is associated with an increased relapse risk in patients, whatever the disease status before transplantation. Of note, the HSCT procedure often takes several weeks to organize, especially when an unrelated donor is recruited, so a therapy to reduce the risk of AML transformation before HSCT may be justified in higher risk patients. Indeed, HSCT in overt AML is followed by a very poor outcome with high risk of relapse [33]. The issue appears similar using intensive chemotherapy (IC) or HMA [29,30,34].
5. The Role of Conditioning Regimen
The intensity of the conditioning regimen has been guided by patient’s age for a long-time, meaning that young patients received myeloablative conditioning (MAC) while older or young patients with comorbidities received reduced intensity regimen (RIC). RIC was developed to reduce NRM, but is followed by an increased progression/relapse risk. An EBMT phase 3 prospective trial has compared MAC and RIC in MDS patients [35]. There was no significant difference between the two arms, relapse risk being balanced by NRM risk. It was not confirmed in an American phase 3 trial including MDS and a majority of AML, which showed worse results with RIC. The minority of MDS patients in the American trial can explain why the results were different from the EBMT study [36]. Schmid and colleagues reported a new regimen combining two sequences of chemotherapy (SEQ): one AML targeted chemotherapy with Fludarabine, Amsacrine and Cytarabine (FLAMSA) followed by one RIC (4 Gy Total Body Irradiation and Cyclophosphamide) developed for high risk patients, especially not eligible for MAC [37,38]. Prophylactic donor lymphocyte infusions (DLI) were planned. All patients (total n = 75) included in the phase 2 trial were either progressive or refractory to chemotherapy, in second remission after early relapse, or in first remission with poor cytogenetics. The 2-year OS was 42% and 62.5% in primary chemotherapy refractory patients. However, a recent phase 3 randomized trial from United Kingdom (UK) has compared SEQ to RIC in 255 patients with AML (n = 164) or MDS (n = 80), and there was no advantage with SEQ on overall survival, event-free survival, NRM, or cumulative incidence of relapse [39]. Of note, disease characteristics from the phase 3 UK trial are very far from the original trial published by Schmid et al., with a majority of patients in remission at time of HSCT, and a minority of MDS at high risk. The exact room for SEQ remains debated and is a source of comparative studies.
In the last years, conditioning regimens with new drugs such as treosulfan [40] in the RIC setting have shown better results regarding NRM. These new approaches might offer better results and enlarge the number of patients who might be candidates for HSCT, such as more lower risk patients, or patients with comorbidities.
6. The Type of Donor
Apart from conditioning regimen, the donor type is potentially modulated by physician’s choice. It is established that an HLA matched sibling donor (MSib), may be the first choice. However, the preference of a younger HLA matched unrelated donor has been questioned [41]. Indeed, an EBMT study reported that the outcome of MDS patients receiving transplant from a young unrelated donor (<30 years) may be better than patients receiving a transplant from an older HLA matched sibling donor. This issue is not specific to MDS, but it is particularly relevant in MDS where both recipients and donors are typically older [42].
Regarding the donor choice between MSib and unrelated (MUD), a CIBMT registry study reported that treatment failure (death or relapse) is similar among MDS patients who received a transplant from MSib as compared to MUD [43]. However, NRM remains significantly higher with MUD. Unfortunately, not all patients have an HLA matched donor, and in these cases, several alternative HLA mismatched donors are possible: unrelated cord blood, unrelated donor, or related haplo-identical (HAPLO) donor. CIMBTR and EBMT have reported that an HLA mismatched unrelated donor gives an inferior outcome as compared to an HLA matched donor [43,44,45]. HAPLO donors are being increa- singly used, mainly because new procedures, including intensive GVHD prophylaxis with post-transplant cyclophosphamide have considerably improved post-transplantation outcome. The EBMT registry study reported that outcome was better using HAPLO donor than unrelated cord blood [44,46], and it has been confirmed in a large meta-analysis [47]. Others have reported that outcome after HAPLO is close to outcome after matched related donor, and several meta-analyses have compiled this HAPLO effect, however they did not only include MDS. A meta-analysis including 1919 patients (publications searched until February 2017) has compared engraftment, GVHD, relapse, DFS, NRM, and OS after HAPLO or HLA matched sibling donor [48]. The authors found that outcomes were all better with MSib, except for NRM, which was similar. Another large meta-analysis including 11,359 patients (publications research until June 2017) confirmed that HAPLO gives similar acute and chronic GVHD, NRM, and relapse incidence than HLA matched donors [49]. However, patients who received a RIC-HAPLO, had higher risk of acute GVHD and NRM. Another more recent meta-analysis including 7806 patients (publications searched until June 2019) compared HAPLO to MSib. HAPLO lowered chronic GVHD risk but increased NRM. Relapse, OS, and DFS were similar. From these meta-analyses, not focused on MDS and sometimes overlapping, we conclude that HAPLO is a valid alternative donor, and gives close results as compared to HLA matched donor transplantation. Randomized trials are still ongoing to determine if HAPLO do better than HLA matched or HLA mismatched donor transplantation.
7. Outcome after Transplantation
Outcome after transplantation depends on patient characteristics; disease characteristics; transplantation-related factors including GVHD prophylaxis, type of donor, infectious prophylaxis; and the occurrence of post-transplant complications such as acute or chronic GVHD, infection, organ failure, comorbidities, or therapy side effects. Recent studies showed 3-year overall survival from 20% to 82% according to disease risk, age, and type of MDS (de novo vs. therapy-related) [25]. The majority of currently transplanted patients have intermediate/high risk, and 3-year OS in this category of patients ranges from 35 to 50% [50,51,52]. NRM, estimated in a large MDS EBMT cohort, ranges between 13% to 60% according to age, comorbidity, disease risk, and type of donor, and for the whole cohort is 28% at 2 years [8]. Relapse incidence ranges from 5 to 80%, mainly related to cytogenetics and somatic mutations prognosis [24,51]. Other risk factors for relapse are high blast count, marrow fibrosis, and refractoriness to pre-graft therapy. Scores taking into account potential risk factors have been developed and used to estimate outcome of transplanted MDS patients [50,51,53]. The optimized EBMT score considers CMV serostatus of the recipient, Karnofsky score, and age for patient characteristics, cytogenetics, platelet count and blood blast count as disease risk, and donor type as transplant procedure. This score is able to distinguish four groups of patients from lower to higher proportion of survival (Figure 2).
8. Post-Transplant Relapse
Relapse remains the first cause of failure after HSCT. An EBMT study showed, in 698 patients relapsing after HSCT, that median OS is only 4.7 months after relapse. Poor risk factors in these patients were shorter remission after HSCT, MDS with blast excess before HSCT, older age, the use of an unrelated donor, and acute GVHD occurrence before relapse [54]. This study also analyzed the outcome after therapy. Using a 6-month landmark post relapse, 2-year OS was 29.7% after second HSCT, and 27% after donor lymphocyte infusion (DLI). The German cooperative transplant group reported the outcome in 152 relapsing patients treated by AZA and DLI [55]. Two-year OS was 29%, and predictors for response were low percentage of marrow blast or molecular relapse. Recently, the SFGM-TC has reported 147 MDS patients relapsing after transplant. Only patients who received “cellular therapy” (DLI or second SCT) could achieve long-term survival (32% vs. 6% for chemotherapy alone) [56]. These results were not confirmed by another European study, showing that relapsing patients who responded to AZA had better OS, with or without DLI [57]. More recently, the addition of Venetoclax to DLI has shown to be feasible in a small retrospective trial [58], with ORR of 50%. Regarding AZA + Venetoclax combinations, a study of the German Cooperative group concludes that toxicity remains high, and responses might be better in molecular relapse and as first salvage therapy [59]. However, larger and prospective studies are needed in this setting [60].
Patients with lower disease burden respond better to post-transplant therapy. This observation led to the development of preemptive therapy. In MDS, there is no standardized method to monitor minimal residual disease (MRD) in all patients. Platzbecker et al. have conducted two prospective phase 2 trials based on preemptive AZA therapy [61,62]. In these two studies, markers of minimal disease were flow sorted CD34 positive donor cells, NPM1, or leukemia specific fusion genes. In the most recent study, 60 patients among 198 had MRD detection during follow-up, and 53 were eligible for the treatment. Among the 138 patients who stayed MRD negative, only five patients relapsed. After MRD-guided treatment, relapse-free survival was 46% at one year, which is very encouraging in patients with imminent relapse.
Preventive therapy is another option which has proven its efficiency in acute myeloblastic leukemia for FLT3 inhibitors in phase 3 trials [63,64]. In MDS, phase 2 studies have reported that reduced dose AZA or decitabine are feasible from day 40 after transplantation [59,65,66,67]. These preventive therapies are especially indicated in patients at very high risk of post-HSCT relapse.
9. Conclusions
HSCT is a curative therapy for MDS, but NRM remains a major obstacle to the success of this treatment. The risk of disease related mortality without the transplant should be balanced with the NRM. Higher risk patients have short life expectancy with chemotherapy, and will generally benefit from the HSCT. Risk for NRM should be carefully eva-luated, and relies on functional age assessment related to general performance status and comorbidities. When a patient has an indication of HSCT, a donor can be found either in the family (MSib or HAPLO) or in registry (matched unrelated or mismatched unrelated). The use of a mismatched donor increases the risk of NRM, but there is also evidence to suggest that an HAPLO donor is a valid choice, as general outcome appears to be at least similar to MUD. Outcome after HSCT is still disappointing in some situations, such as in patients harboring TP53 mutations or very poor cytogenetics. Protocols are ongoing to test new strategies in these patients, enabling us to overcome this poor prognosis and to prevent post-transplant relapse.
Author Contributions
S.V. and M.R. wrote the manuscript. Both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Greenberg, P.; Cox, C.; LeBeau, M.M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997, 89, 2079–2088. [Google Scholar] [CrossRef]
- Greenberg, P.L.; Tuechler, H.; Schanz, J.; Sanz, G.; Garcia-Manero, G.; Sole, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood 2012, 120, 2454–2465. [Google Scholar] [CrossRef]
- Nagata, Y.; Zhao, R.; Awada, H.; Kerr, C.M.; Mirzaev, I.; Kongkiatkamon, S.; Nazha, A.; Makishima, H.; Radivoyevitch, T.; Scott, J.G.; et al. Machine learning demonstrates that somatic mutations imprint invariant morphologic features in myelodysplastic syndromes. Blood 2020, 136, 2249–2262. [Google Scholar] [CrossRef] [PubMed]
- Malcovati, L.; Papaemmanuil, E.; Ambaglio, I.; Elena, C.; Gallì, A.; Della Porta, M.G.; Travaglino, E.; Pietra, D.; Pascutto, C.; Ubezio, M.; et al. Driver somatic mutations identify distinct disease entities within myeloid neoplasms with myelodysplasia. Blood 2014, 124, 1513–1521. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Malcovati, L.; Tauro, S.; Gundem, G.; Van Loo, P.; Yoon, C.J.; Ellis, P.; Wedge, D.C.; Pellagatti, A.; et al. Clinical and biological implications of driver mutations in myelodysplastic syndromes. Blood 2013, 122, 3616–3627. [Google Scholar] [CrossRef] [PubMed]
- Onida, F.; Brand, R.; van Biezen, A.; Schaap, M.; von dem Borne, P.A.; Maertens, J.; Beelen, D.W.; Carreras, E.; Alessandrino, E.P.; Volin, L.; et al. Impact of the International Prognostic Scoring System cytogenetic risk groups on the outcome of patients with primary myelodysplastic syndromes undergoing allogeneic stem cell transplantation from human leukocyte antigen-identical siblings: A retrospective analysis of the European Society for Blood and Marrow Transplantation-Chronic Malignancies Working Party. Haematologica 2014, 99, 1582–1590. [Google Scholar]
- Deeg, H.J.; Scott, B.L.; Fang, M.; Shulman, H.M.; Gyurkocza, B.; Myerson, D.; Pagel, J.M.; Platzbecker, U.; Ramakrishnan, A.; Radich, J.P.; et al. Five-group cytogenetic risk classification, monosomal karyotype, and outcome after hematopoietic cell transplantation for MDS or acute leukemia evolving from MDS. Blood 2012, 120, 1398–1408. [Google Scholar] [CrossRef] [PubMed]
- Carré, M.; Porcher, R.; Finke, J.; Ehninger, G.; Koster, L.; Beelen, D.; Ganser, A.; Volin, L.; Lozano, S.; Friis, L.; et al. Role of age and hematopoietic cell transplantation-specific comorbidity index in myelodysplastic patients undergoing an allotransplant. A retrospective study from the CMWP (Chronic Malignancies Working Party) of the EBMT. Biol. Blood Marrow Transplant. 2020, 2020, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Finelli, C.; Giagounidis, A.; Schoch, R.; Gattermann, N.; Sanz, G.; List, A.; et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: A randomised, open-label, phase III study. Lancet Oncol. 2009, 10, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Muffly, L.; Pasquini, M.C.; Martens, M.; Brazauskas, R.; Zhu, X.; Adekola, K.; Aljurf, M.; Ballen, K.K.; Bajel, A.; Baron, F.; et al. Increasing use of allogeneic hematopoietic cell transplantation in patients aged 70 years and older in the United States. Blood 2017, 130, 1156–1164. [Google Scholar] [CrossRef]
- Sorror, M.L.; Maris, M.B.; Storb, R.; Baron, F.; Sandmaier, B.M.; Maloney, D.G.; Storer, B. Hematopoietic cell transplantation (HCT)-specific comorbidity index: A new tool for risk assessment before allogeneic HCT. Blood 2005, 106, 2912–2919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorror, M.L.; Giralt, S.; Sandmaier, B.M.; De Lima, M.; Shahjahan, M.; Maloney, D.G.; Deeg, H.J.; Appelbaum, F.R.; Storer, B.; Storb, R. Hematopoietic cell transplantation specific comorbidity index as an outcome predictor for patients with acute myeloid leukemia in first remission: Combined FHCRC and MDACC experiences. Blood 2007, 110, 4606–4613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muffly, L.S.; Kocherginsky, M.; Stock, W.; Chu, Q.; Bishop, M.R.; Godley, L.A.; Kline, J.; Liu, H.; Odenike, O.M.; Larson, R.A.; et al. Geriatric assessment to predict survival in older allogeneic hematopoietic cell transplantation recipients. Haematologica 2014, 99, 1373–1379. [Google Scholar] [CrossRef] [Green Version]
- Cutler, C.S.; Lee, S.J.; Greenberg, P.; Deeg, H.J.; Perez, W.S.; Anasetti, C.; Bolwell, B.J.; Cairo, M.S.; Gale, R.P.; Klein, J.P.; et al. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: Delayed transplantation for low-risk myelodysplasia is associated with improved outcome. Blood 2004, 104, 579–585. [Google Scholar] [CrossRef]
- Koreth, J.; Pidala, J.; Perez, W.S.; Deeg, H.J.; Garcia-Manero, G.; Malcovati, L.; Cazzola, M.; Park, S.; Itzykson, R.; Ades, L.; et al. Role of reduced-intensity conditioning allogeneic hematopoietic stem-cell transplantation in older patients with de novo myelodysplastic syndromes: An international collaborative decision analysis. J. Clin. Oncol. 2013, 31, 2662–2670. [Google Scholar] [CrossRef] [PubMed]
- Platzbecker, U.; Schetelig, J.; Finke, J.; Trenschel, R.; Scott, B.L.; Kobbe, G.; Schaefer-Eckart, K.; Bornhauser, M.; Itzykson, R.; Germing, U.; et al. Allogeneic hematopoietic cell transplantation in patients age 60–70 years with de novo high-risk myelodysplastic syndrome or secondary acute myelogenous leukemia: Comparison with patients lacking donors who received azacitidine. Biol. Blood Marrow Transplant. 2012, 18, 1415–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robin, M.; Porcher, R.; Adès, L.; Raffoux, E.; Michallet, M.; François, S.; Cahn, J.-Y.; Delmer, A.; Wattel, E.; Vigouroux, S.; et al. HLA-matched allogeneic stem cell transplantation improves outcome of higher risk myelodysplastic syndrome A prospective study on behalf of SFGM-TC and GFM. Leukemia 2015, 29, 1496–1501. [Google Scholar] [CrossRef]
- Bejar, R.; Stevenson, K.E.; Caughey, B.; Lindsley, R.C.; Mar, B.G.; Stojanov, P.; Getz, G.; Steensma, D.P.; Ritz, J.; Soiffer, R.; et al. Somatic mutations predict poor outcome in patients with myelodysplastic syndrome after hematopoietic stem-cell transplantation. J. Clin. Oncol. 2014, 32, 2691–2698. [Google Scholar] [CrossRef] [Green Version]
- Bejar, R.; Stevenson, K.; Abdel-Wahab, O.; Galili, N.; Nilsson, B.; Garcia-Manero, G.; Kantarjian, H.; Raza, A.; Levine, R.L.; Neuberg, D.; et al. Clinical effect of point mutations in myelodysplastic syndromes. N. Engl. J. Med. 2011, 364, 2496–2506. [Google Scholar] [CrossRef] [Green Version]
- Yoshizato, T.; Nannya, Y.; Atsuta, Y.; Shiozawa, Y.; Iijima-Yamashita, Y.; Yoshida, K.; Shiraishi, Y.; Suzuki, H.; Nagata, Y.; Sato, Y.; et al. Genetic abnormalities in myelodysplasia and secondary acute myeloid leukemia: Impact on outcome of stem cell transplantation. Blood 2017, 129, 2347–2358. [Google Scholar] [CrossRef]
- Della Porta, M.G.; Gallì, A.; Bacigalupo, A.; Zibellini, S.; Bernardi, M.; Rizzo, E.; Allione, B.; van Lint, M.T.; Pioltelli, P.; Marenco, P.; et al. Clinical Effects of Driver Somatic Mutations on the Outcomes of Patients with Myelodysplastic Syndromes Treated With Allogeneic Hematopoietic Stem-Cell Transplantation. J. Clin. Oncol. 2016, 34, 3627. [Google Scholar] [CrossRef]
- Gangat, N.; Mudireddy, M.; Lasho, T.L.; Finke, C.M.; Nicolosi, M.; Szuber, N.; Patnaik, M.M.; Pardanani, A.; Hanson, C.A.; Ketterling, R.P.; et al. Mutations and prognosis in myelodysplastic syndromes: Karyotype-adjusted analysis of targeted sequencing in 300 consecutive cases and development of a genetic risk model. Am. J. Hematol. 2018, 93, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Nazha, A.; Al-Issa, K.; Hamilton, B.K.; Radivoyevitch, T.; Gerds, A.T.; Mukherjee, S.; Adema, V.; Zarzour, A.; Abuhadra, N.; Patel, B.J.; et al. Adding molecular data to prognostic models can improve predictive power in treated patients with myelodysplastic syndromes. Leukemia 2017, 31, 2848–2850. [Google Scholar] [CrossRef]
- Koenecke, C.; Gohring, G.; de Wreede, L.C.; van Biezen, A.; Scheid, C.; Volin, L.; Maertens, J.; Finke, J.; Schaap, N.; Robin, M.; et al. Impact of the revised International Prognostic Scoring System cytogenetics and monosomal karyotype on outcome after allogeneic stem cell transplantation for myelodysplastic syndromes and secondary acute myeloid leukemia evolving from myelodysplastic syndromes: A retrospective multicenter study of the European Society of Blood and Marrow Transplantation. Haematologica 2014, 100, 400. [Google Scholar] [PubMed] [Green Version]
- Lindsley, R.C.; Saber, W.; Mar, B.G.; Redd, R.; Wang, T.; Haagenson, M.D.; Grauman, P.V.; Hu, Z.-H.; Spellman, S.R.; Lee, S.J.; et al. Prognostic Mutations in Myelodysplastic Syndrome after Stem-Cell Transplantation. N. Engl. J. Med. 2017, 376, 536–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robin, M.; Fenaux, P. Which lower risk myelodysplastic syndromes should be treated with allogeneic hematopoietic stem cell transplantation? Leukemia 2020, 34, 2552–2560. [Google Scholar] [CrossRef] [PubMed]
- Robin, M.; Porcher, R.; Zinke-Cerwenka, W.; van Biezen, A.; Volin, L.; Mufti, G.; Craddock, C.; Finke, J.; Richard, C.; Passweg, J.; et al. Allogeneic haematopoietic stem cell transplant in patients with lower risk myelodysplastic syndrome: A retrospective analysis on behalf of the Chronic Malignancy Working Party of the EBMT. Bone Marrow Transplant. 2017, 52, 209–215. [Google Scholar] [CrossRef]
- De Witte, T.; Bowen, D.; Robin, M.; Malcovati, L.; Niederwieser, D.; Yakoub-Agha, I.; Mufti, G.J.; Fenaux, P.; Sanz, G.; Martino, R.; et al. Allogeneic hematopoietic stem cell transplantation for MDS and CMML: Recommendations from an international expert panel. Blood 2017, 129, 1753–1762. [Google Scholar] [CrossRef]
- Potter, V.T.; Iacobelli, S.; van Biezen, A.; Maertens, J.; Bourhis, J.-H.; Passweg, J.R.; Yakhoub-Agha, I.; Tabrizi, R.; Bay, J.-O.; Chevallier, P.; et al. Comparison of Intensive Chemotherapy and Hypomethylating Agents before Allogeneic Stem Cell Transplantation for Advanced Myelodysplastic Syndromes: A Study of the Myelodysplastic Syndrome Subcommittee of the Chronic Malignancies Working Party of the European Society for Blood and Marrow Transplant Research. Biol. Blood Marrow Transplant. 2016, 22, 1615–1620. [Google Scholar] [PubMed] [Green Version]
- Damaj, G.; Duhamel, A.; Robin, M.; Beguin, Y.; Michallet, M.; Mohty, M.; Vigouroux, S.; Bories, P.; Garnier, A.; El Cheikh, J.; et al. Impact of azacitidine before allogeneic stem-cell transplantation for myelodysplastic syndromes: A study by the Societe Francaise de Greffe de Moelle et de Therapie-Cellulaire and the Groupe-Francophone des Myelodysplasies. J. Clin. Oncol. 2012, 30, 4533–4540. [Google Scholar] [CrossRef]
- Ivey, A.; Hills, R.K.; Simpson, M.A.; Jovanovic, J.V.; Gilkes, A.; Grech, A.; Patel, Y.; Bhudia, N.; Farah, H.; Mason, J.; et al. Assessment of Minimal Residual Disease in Standard-Risk AML. N. Engl. J. Med. 2016, 374, 422–433. [Google Scholar] [CrossRef] [Green Version]
- Balsat, M.; Renneville, A.; Thomas, X.; de Botton, S.; Caillot, D.; Marceau, A.; Lemasle, E.; Marolleau, J.-P.; Nibourel, O.; Berthon, C.; et al. Postinduction Minimal Residual Disease Predicts Outcome and Benefit from Allogeneic Stem Cell Transplantation in Acute Myeloid Leukemia with NPM1 Mutation: A Study by the Acute Leukemia French Association Group. J. Clin. Oncol. 2017, 35, 185–193. [Google Scholar] [CrossRef]
- Kröger, N.; Eikema, D.-J.; Köster, L.; Beelen, D.; de Wreede, L.C.; Finke, J.; Koenecke, C.; Niederwieser, D.; Bornhäuser, M.; Schoenland, S.; et al. Impact of primary disease on outcome after allogeneic stem cell transplantation for transformed secondary acute leukaemia. Br. J. Haematol. 2019, 185, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Alessandrino, E.P.; Della Porta, M.G.; Pascutto, C.; Bacigalupo, A.; Rambaldi, A. Should cytoreductive treatment be performed before transplantation in patients with high-risk myelodysplastic syndrome? J. Clin. Oncol. 2013, 31, 2761–2762. [Google Scholar] [CrossRef]
- Kröger, N. Reduced Intensity Vs. Standard Conditioning Followed by Allogeneic Stem Cell Transplantation for Patients with MDS or Secondary AML: A Prospective, Randomized Phase III Study of the Chronic Malignancies Working Party of the EBMT (RICMAC-Trial). Blood 2014, 124, 320. [Google Scholar] [CrossRef]
- Scott, B.L.; Pasquini, M.C.; Logan, B.R.; Wu, J.; Devine, S.M.; Porter, D.L.; Maziarz, R.T.; Warlick, E.D.; Fernandez, H.F.; Alyea, E.P.; et al. Myeloablative Versus Reduced-Intensity Hematopoietic Cell Transplantation for Acute Myeloid Leukemia and Myelodysplastic Syndromes. J. Clin. Oncol. 2017, 35, 1154–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, C.; Schleuning, M.; Ledderose, G.; Tischer, J.; Kolb, H.J. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J. Clin. Oncol. 2005, 23, 5675–5687. [Google Scholar] [CrossRef]
- Schmid, C.; Schleuning, M.; Schwerdtfeger, R.; Hertenstein, B.; Mischak-Weissinger, E.; Bunjes, D.; Harsdorf, S.V.; Scheid, C.; Holtick, U.; Greinix, H.; et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood 2006, 108, 1092–1099. [Google Scholar] [CrossRef]
- Craddock, C.; Jackson, A.; Loke, J.; Siddique, S.; Hodgkinson, A.; Mason, J.; Andrew, G.; Nagra, S.; Malladi, R.; Peniket, A.; et al. Augmented Reduced-Intensity Regimen does not Improve Postallogeneic Transplant Outcomes in Acute Myeloid Leukemia. J. Clin. Oncol. 2020, JCO2002308. [Google Scholar] [CrossRef]
- Beelen, D.W.; Trenschel, R.; Stelljes, M.; Groth, C.; Masszi, T.; Reményi, P.; Wagner-Drouet, E.-M.; Hauptrock, B.; Dreger, P.; Luft, T.; et al. Treosulfan or busulfan plus fludarabine as conditioning treatment before allogeneic haemopoietic stem cell transplantation for older patients with acute myeloid leukaemia or myelodysplastic syndrome (MC-FludT.14/L): A randomised, non-inferiority, phase 3 trial. Lancet Haematol. 2020, 7, e28–e39. [Google Scholar]
- Kröger, N.; Zabelina, T.; de Wreede, L.; Berger, J.; Alchalby, H.; van Biezen, A.; Milpied, N.; Volin, L.; Mohty, M.; Leblond, V.; et al. Allogeneic stem cell transplantation for older advanced MDS patients: Improved survival with young unrelated donor in comparison with HLA-identical siblings. Leukemia 2013, 27, 604–609. [Google Scholar] [CrossRef] [Green Version]
- Kollman, C.; Spellman, S.R.; Zhang, M.-J.; Hassebroek, A.; Anasetti, C.; Antin, J.H.; Champlin, R.E.; Confer, D.L.; DiPersio, J.F.; Fernandez-Viña, M.; et al. The effect of donor characteristics on survival after unrelated donor transplantation for hematologic malignancy. Blood 2016, 127, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Saber, W.; Opie, S.; Rizzo, J.D.; Zhang, M.J.; Horowitz, M.M.; Schriber, J. Outcomes after matched unrelated donor versus identical sibling hematopoietic cell transplantation in adults with acute myelogenous leukemia. Blood 2012, 119, 3908–3916. [Google Scholar] [CrossRef] [Green Version]
- Robin, M.; Porcher, R.; Ruggeri, A.; Blaise, D.; Wolschke, C.; Koster, L.; Angelucci, E.; Stölzel, F.; Potter, V.; Yakoub-Agha, I.; et al. HLA-Mismatched Donors in Patients with Myelodysplastic Syndrome: An EBMT Registry Analysis. Biol. Blood Marrow Transplant. 2019, 25, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Robin, M.; Ruggeri, A.; Labopin, M.; Niederwieser, D.; Tabrizi, R.; Sanz, G.; Bourhis, J.H.; van Biezen, A.; Koenecke, C.; Blaise, D.; et al. Comparison of Unrelated Cord Blood and Peripheral Blood Stem Cell Transplantation in Adults with Myelodysplastic Syndrome after Reduced-Intensity Conditioning Regimen: A Collaborative Study from Eurocord (Cord blood Committee of Cellular Therapy & Immunobiology Working Party of EBMT) and Chronic Malignancies Working Party. Biol. Blood Marrow Transplant. 2014, 21, 489–495. [Google Scholar] [PubMed] [Green Version]
- Robin, M.; Porcher, R.; Ciceri, F.; van Lint, M.T.; Santarone, S.; Ehninger, G.; Blaise, D.; Güllbas, Z.; Gonzáles Muñiz, S.; Michallet, M.; et al. Haploidentical transplant in patients with myelodysplastic syndrome. Blood Adv. 2017, 1, 1876–1883. [Google Scholar] [CrossRef]
- Poonsombudlert, K.; Kewcharoen, J.; Prueksapraopong, C.; Limpruttidham, N. Post transplant cyclophosphamide based haplo-identical transplant versus umbilical cord blood transplant; a meta-analysis. Jpn. J. Clin. Oncol. 2019, 49, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Zhou, D.; Guo, D.; Xu, P.; Chen, B. Comparison of outcomes in hematological malignancies treated with haploidentical or HLA-identical sibling hematopoietic stem cell transplantation following myeloablative conditioning: A meta-analysis. PLoS ONE 2018, 13, e0191955. [Google Scholar] [CrossRef]
- Yang, B.; Yu, R.; Cai, L.; Guo, B.; Chen, H.; Zhang, H.; He, P.; Lu, X. Haploidentical versus matched donor stem cell transplantation for patients with hematological malignancies: A systemic review and meta-analysis. Bone Marrow Transplant. 2019, 54, 99–122. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, B.C.; Ahn, K.W.; Hu, Z.-H.; Nishihori, T.; Malone, A.K.; Valcárcel, D.; Grunwald, M.R.; Bacher, U.; Hamilton, B.; Kharfan-Dabaja, M.A.; et al. Scoring System Prognostic of Outcome in Patients Undergoing Allogeneic Hematopoietic Cell Transplantation for Myelodysplastic Syndrome. J. Clin. Oncol. 2016, 34, 1864–1871. [Google Scholar] [CrossRef] [PubMed]
- Della Porta, M.G.; Alessandrino, E.P.; Bacigalupo, A.; van Lint, M.T.; Malcovati, L.; Pascutto, C.; Falda, M.; Bernardi, M.; Onida, F.; Guidi, S.; et al. Predictive factors for the outcome of allogeneic transplantation in patients with MDS stratified according to the revised IPSS-R. Blood 2014, 123, 2333–2342. [Google Scholar] [CrossRef]
- Scheid, C.; de Wreede, L.; van Biezen, A.; Koenecke, C.; Göhring, G.; Volin, L.; Maertens, J.; Finke, J.; Passweg, J.; Beelen, D.; et al. Validation of the revised IPSS at transplant in patients with myelodysplastic syndrome/transformed acute myelogenous leukemia receiving allogeneic stem cell transplantation: A retrospective analysis of the EBMT chronic malignancies working party. Bone Marrow Transplant. 2017, 52, 1519–1525. [Google Scholar] [CrossRef] [Green Version]
- Gagelmann, N.; Eikema, D.-J.; Stelljes, M.; Beelen, D.; de Wreede, L.; Mufti, G.; Knelange, N.S.; Niederwieser, D.; Friis, L.S.; Ehninger, G.; et al. Optimized EBMT transplant-specific risk score in myelodysplastic syndromes after allogeneic stem-cell transplantation. Haematologica 2019, 104, 929–936. [Google Scholar] [CrossRef]
- Schmid, C.; de Wreede, L.C.; van Biezen, A.; Finke, J.; Ehninger, G.; Ganser, A.; Volin, L.; Niederwieser, D.; Beelen, D.; Alessandrino, P.; et al. Outcome after relapse of myelodysplastic syndrome and secondary acute myeloid leukemia following allogeneic stem cell transplantation: A retrospective registry analysis on 698 patients by the Chronic Malignancies Working Party of the European Society of Blood and Marrow Transplantation. Haematologica 2018, 103, 237–245. [Google Scholar] [PubMed]
- Schroeder, T.; Rachlis, E.; Bug, G.; Stelljes, M.; Klein, S.; Steckel, N.K.; Wolf, D.; Ringhoffer, M.; Czibere, A.; Nachtkamp, K.; et al. Treatment of acute myeloid leukemia or myelodysplastic syndrome relapse after allogeneic stem cell transplantation with azacitidine and donor lymphocyte infusions—A retrospective multicenter analysis from the German Cooperative Transplant Study Group. Biol Blood Marrow Transplant. 2015, 21, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Guièze, R.; Damaj, G.; Pereira, B.; Robin, M.; Chevallier, P.; Michallet, M.; Vigouroux, S.; Beguin, Y.; Blaise, D.; El Cheikh, J.; et al. Management of Myelodysplastic Syndrome Relapsing after Allogeneic Hematopoietic Stem Cell Transplantation: A Study by the French Society of Bone Marrow Transplantation and Cell Therapies. Biol. Blood Marrow Transplant. 2016, 22, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craddock, C.; Labopin, M.; Robin, M.; Finke, J.; Chevallier, P.; Yakoub-Agha, I.; Bourhis, J.H.; Sengelov, H.; Blaise, D.; Luft, T.; et al. Clinical activity of azacitidine in patients who relapse after allogeneic stem cell transplantation for acute myeloid leukemia. Haematologica 2016, 101, 879–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, O.; On, Y.B.; Perez, G.; Shargian-Alon, L.; Yeshurun, M.; Ram, R. Venetoclax and donor lymphocyte infusion for early relapsed acute myeloid leukemia after allogeneic hematopoietic cell transplantation. A retrospective multicenter trial. Ann. Hematol. 2021, 100, 817–824. [Google Scholar] [CrossRef]
- Pusic, I.; Choi, J.; Fiala, M.A.; Gao, F.; Holt, M.; Cashen, A.F.; Vij, R.; Abboud, C.N.; Stockerl-Goldstein, K.E.; Jacoby, M.A.; et al. Maintenance Therapy with Decitabine after Allogeneic Stem Cell Transplantation for Acute Myelogenous Leukemia and Myelodysplastic Syndrome. Biol. Blood Marrow Transplant. 2015, 21, 1761–1769. [Google Scholar] [CrossRef] [Green Version]
- Schuler, E.; Wagner-Drouet, E.-M.; Ajib, S.; Bug, G.; Crysandt, M.; Dressler, S.; Hausmann, A.; Heidenreich, D.; Hirschbühl, K.; Hoepting, M.; et al. Treatment of myeloid malignancies relapsing after allogeneic hematopoietic stem cell transplantation with venetoclax and hypomethylating agents-a retrospective multicenter analysis on behalf of the German Cooperative Transplant Study Group. Ann. Hematol. 2021, 100, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Platzbecker, U.; Wermke, M.; Radke, J.; Oelschlaegel, U.; Seltmann, F.; Kiani, A.; Klut, I.M.; Knoth, H.; Rollig, C.; Schetelig, J.; et al. Azacitidine for treatment of imminent relapse in MDS or AML patients after allogeneic HSCT: Results of the RELAZA trial. Leukemia 2012, 26, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Platzbecker, U.; Middeke, J.M.; Sockel, K.; Herbst, R.; Wolf, D.; Baldus, C.D.; Oelschlägel, U.; Mütherig, A.; Fransecky, L.; Noppeney, R.; et al. Measurable residual disease-guided treatment with azacitidine to prevent haematological relapse in patients with myelodysplastic syndrome and acute myeloid leukaemia (RELAZA2): An open-label, multicentre, phase 2 trial. Lancet Oncol. 2018, 19, 1668–1679. [Google Scholar] [CrossRef]
- Burchert, A.; Bug, G.; Fritz, L.V.; Finke, J.; Stelljes, M.; Röllig, C.; Wollmer, E.; Wäsch, R.; Bornhäuser, M.; Berg, T.; et al. Sorafenib Maintenance After Allogeneic Hematopoietic Stem Cell Transplantation for Acute Myeloid Leukemia with FLT3-Internal Tandem Duplication Mutation (SORMAIN). J. Clin. Oncol. 2020, 38, 2993–3002. [Google Scholar] [CrossRef] [PubMed]
- Xuan, L.; Wang, Y.; Huang, F.; Fan, Z.; Xu, Y.; Sun, J.; Xu, N.; Deng, L.; Li, X.; Liang, X.; et al. Sorafenib maintenance in patients with FLT3-ITD acute myeloid leukaemia undergoing allogeneic haematopoietic stem-cell transplantation: An open-label, multicentre, randomised phase 3 trial. Lancet Oncol. 2020, 21, 1201–1212. [Google Scholar] [CrossRef]
- Craddock, C.; Jilani, N.; Siddique, S.; Yap, C.; Khan, J.; Nagra, S.; Ward, J.; Ferguson, P.; Hazlewood, P.; Buka, R.; et al. Tolerability and Clinical Activity of Post-Transplantation Azacitidine in Patients Allografted for Acute Myeloid Leukemia Treated on the RICAZA Trial. Biol. Blood Marrow Transplant. 2016, 22, 385–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lima, M.; Giralt, S.; Thall, P.F.; de Padua Silva, L.; Jones, R.B.; Komanduri, K.; Braun, T.M.; Nguyen, H.Q.; Champlin, R.; Garcia-Manero, G. Maintenance therapy with low-dose azacitidine after allogeneic hematopoietic stem cell transplantation for recurrent acute myelogenous leukemia or myelodysplastic syndrome: A dose and schedule finding study. Cancer 2010, 116, 5420–5431. [Google Scholar] [CrossRef]
- Guillaume, T.; Malard, F.; Magro, L.; Labopin, M.; Tabrizi, R.; Borel, C.; Chevallier, P.; Vigouroux, S.; Peterlin, P.; Garnier, A.; et al. Prospective phase II study of prophylactic low-dose azacitidine and donor lymphocyte infusions following allogeneic hematopoietic stem cell transplantation for high-risk acute myeloid leukemia and myelodysplastic syndrome. Bone Marrow Transplant. 2019, 54, 1815–1826. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overall survival in higher risk MDS patients with or without a donor. This is a prospective French study showing an advantage of survival in patients with a donor (Leukemia 2015. Robin et al.).
Figure 1.
Overall survival in higher risk MDS patients with or without a donor. This is a prospective French study showing an advantage of survival in patients with a donor (Leukemia 2015. Robin et al.).

Figure 2.
Outcome of MDS transplanted patients according to EBMT adapted score. This is a registry study from EBMT reporting a new score based on CMV serostatus recipient, Karnofsky score, and age for patient characteristics, cytogenetics, platelet count and blood blast count as disease risk, and donor type (Haematologica 2019, Gagelman [53]). The figure shows overall survival (A), relapse-free survival (B), relapse incidence (C), and non-relapse mortality (D) according to the EBMT adapted score.
Figure 2.
Outcome of MDS transplanted patients according to EBMT adapted score. This is a registry study from EBMT reporting a new score based on CMV serostatus recipient, Karnofsky score, and age for patient characteristics, cytogenetics, platelet count and blood blast count as disease risk, and donor type (Haematologica 2019, Gagelman [53]). The figure shows overall survival (A), relapse-free survival (B), relapse incidence (C), and non-relapse mortality (D) according to the EBMT adapted score.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Villar, S.; Robin, M. Allogeneic Stem Cell Transplantation for MDS. Hemato 2021, 2, 545-555. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2030034
AMA Style
Villar S, Robin M. Allogeneic Stem Cell Transplantation for MDS. Hemato. 2021; 2(3):545-555. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2030034
Chicago/Turabian StyleVillar, Sara, and Marie Robin. 2021. "Allogeneic Stem Cell Transplantation for MDS" Hemato 2, no. 3: 545-555. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2030034