
Geographic Prevalence Patterns and Modifiable Risk Factors for Monoclonal Gammopathy of Undetermined Significance

1
Department of Medicine, Boston University Chobanian and Avedisian School of Medicine, Boston, MA 02118, USA
2
Boston University Medical Campus, Boston University Chobanian and Avedisian School of Medicine, Boston, MA 02118, USA
3
Section of Hematology and Oncology, Department of Medicine, Boston Medical Center, Boston, MA 02118, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Hemato 2023, 4(4), 331-349; https://0-doi-org.brum.beds.ac.uk/10.3390/hemato4040027
Submission received: 20 September 2023
/
Revised: 17 October 2023
/
Accepted: 24 October 2023
/
Published: 1 November 2023
(This article belongs to the Section Plasma Cell Disorders)
Abstract
:Monoclonal gammopathy of undetermined significance (MGUS) is a pre-malignant plasma cell disorder with an etiology that is incompletely understood. Modifiable risk factors and genetic predispositions likely interact to increase MGUS risk in specific individuals and populations. Identifying geographic prevalence patterns and modifiable risk factors is critical for understanding the etiology of MGUS. The aim of this review was to outline original research on MGUS prevalence across geographic locations and modifiable risk factors. We conducted a systematic review of 39 eligible studies from PubMed®, Embase®, and Web of Science® written in English and published by February 2023. Our protocol was registered in accordance with PROSPERO guidelines. Studies were synthesized using Research Electronic Data Capture and appraised using the National Heart, Lung, and Blood Institute study quality assessment tools. The prevalence of MGUS ranged from 0.24% to 9% across geographic locations. Modifiable risk factors for MGUS include infections, autoimmune diseases, chronic inflammatory conditions, lifestyle factors, environmental exposures, and ionizing radiation. Therefore, the development of MGUS may be related to chronic antigenic stimulation and genetic aberrations that promote clonal proliferation of plasma cells. Prospective studies assessing gene–environment interactions are needed to further define risk factors for MGUS and inform screening and preventative strategies.
1. Introduction
Monoclonal gammopathy of undetermined significance (MGUS) is a plasma cell disorder that universally precedes multiple myeloma (MM), which accounts for approximately 10% of all hematologic malignancies [1,2,3,4]. The diagnosis of MGUS is often incidental and relies on a serum monoclonal protein (M protein) level of <3 g/dL, <10% clonal plasma cells in the bone marrow, and the absence of myeloma-defining events. MGUS is also associated with other life-threatening disorders, including light chain amyloidosis, light chain deposition disease, lymphoma, and lymphoproliferative diseases such as Waldenström macroglobulinemia [5,6]. Even without progression to MM and other disorders, MGUS can lead to clinical sequelae with long-term morbidity, such as osteoporosis, bone fractures, peripheral neuropathy, arterial and venous thrombosis, and cardiovascular morbidities, even without underlying risk factors for cardiovascular disease [7,8,9].
In the United States, MGUS affects 3% of the population above age 50 and carries an annual 1% risk of progression to MM [10]. Meanwhile, less is known about global geographic patterns in the prevalence of MGUS. The prevalence of MGUS is likely population-specific and highly dependent on the composition and interaction of the modifiable (medical, socioeconomic, and environmental) and non-modifiable (demographic) risk factors affecting the individuals in each population [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25]. Specifically, race, ethnicity, and increasing age are major non-modifiable risk factors for MGUS [26]. In Black as compared to White US patients, MGUS is two to three times more common and has an earlier age of onset [27,28]. Although studying the role of genetic ancestry and self-identified race and ethnicity improved our understanding of MGUS development, genetics alone may not provide an explanation that fully addresses the racial and ethnic differences in the prevalence of MGUS. Genome-wide association studies have failed to identify loci that explain the increased MM risk in patients of African ancestry, suggesting more complex mechanisms could be at play [29]. Race and ethnicity are dynamic sociocultural constructs, so disparities are likely heavily influenced by modifiable risk factors, including geographic, cultural, and social factors, in addition to genetic predispositions. Finally, given that MGUS prevalence increases with age, there is potential for the aging process to contribute to the development of the disease. The environment and behavioral factors play a crucial role in modifying biological determinants of human health, including the epigenetic changes that occur during aging [30,31]. Therefore, it is paramount to assess possible modifiable factors that may contribute to the association between increasing age and the development of MGUS.
While recent advances have improved our understanding of the complex genetic and non-genetic factors that cause MGUS progression to MM, the development of MGUS and potentially modifiable risk factors for MGUS are less understood. As a result, screening and prevention strategies for MGUS are largely understudied. Some studies suggest that chronic exposure of the B-cell receptor to persistent exogenous or endogenous antigens may lead to clonal B cell proliferation, antigen-driven selection of B cell clones, and the subsequent development of MGUS [13,14,15,32,33,34]. Nonetheless, descriptive epidemiologic studies and a thorough assessment of risk factors are paramount to understanding the development of MGUS, developing screening guidelines, and implementing public health policies for MGUS prevention.
Since MGUS prevalence is a function of the demographic composition of each group and risk factors for MGUS may be population-specific, large population studies at various geographic sites are needed. Poor knowledge of global geographic patterns in MGUS prevalence limits the generalizability of any suggested screening or preventive interventions. Population-based screening for MGUS could also identify candidates for early treatment or help guide optimal clinical management [35]. Using this lens, we discuss the geographic prevalence patterns of MGUS and recent advances in knowledge of risk factors for MGUS to assess the potential influence of non-modifiable versus modifiable risk factors associated with MGUS. Then, using existing knowledge of risk factors, racial disparities in MGUS prevalence, and the impact of non-genetic factors on plasma cell biology, we propose a framework for viewing gene-environment interactions and explore future directions for research.
2. Materials and Methods
2.1. Data Sources and Searches
This review was conducted between 11 November 2021 and 31 March 2023 and performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [36,37]. (Table S1) The protocol for this study was registered on the PROSPERO registry for systematic reviews (CRD42022312662; https://www.crd.york.ac.uk/Prospero/display_record.php?RecordID=312662 accessed 12 March, 2022). In collaboration with a librarian, we developed a search strategy and search terms to query various databases. Searches on PubMed®, Embase®, and Web of Science® were performed from December 2021 to February 2023 to identify relevant articles. Text headings and medical subject heading (MeSH) terms used included MGUS, monoclonal gammopathy, monoclonal gammopathy of undetermined significance, incidence, prevalence, and risk. We also reviewed the references of the identified papers to look for studies relevant to our topic.
2.2. Study Selection
Abstracts with available full-text articles were reviewed by K.V. and R.S. to determine which articles examined the prevalence and risk factors for MGUS. We included studies that (1) reported the prevalence of MGUS across various geographic locations; (2) investigated non-genetic risk factors for developing MGUS; (3) were published before 28 February 2023; and (4) were available in English. Studies on prevalence were limited to case–control studies and cohort studies. However, to include all relevant data, we also reviewed case series on risk factors for MGUS. We excluded case reports and abstracts without available full text.
2.3. Data Extraction, Synthesis, and Quality Assessment
K.V. and R.S. reviewed all publication titles and abstracts and eliminated articles that were not relevant to the review. K.V., R.S., and C.V.E. reviewed the full text of all articles included. Data were then extracted by K.V. and R.S. from the articles that met the inclusion criteria. A standardized data collection form was used and included the study title, authors, year of publication, source of participants, sample size, mean age and sex composition of the sample, race and ethnicity composition of the sample, country in which the study was conducted, method used to diagnose MGUS, prevalence, risk factor(s) evaluated if applicable, and effect estimates with 95% confidence intervals (CI). The standardized data collection form and all related study data were managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Boston University, CTSI 1UL1TR001430 [38,39,40]. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. C.V.E. reviewed all data extracted and resolved any discordance in article inclusion and data extraction. For the quality assessment of individual studies, we used questions adapted from the screening study quality assessment tools developed by the National Heart, Lung, and Blood Institute (NHLBI) and available at https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 19 February 2022). (Table S2 and S3) For studies included, data synthesis involved a (1) description of the study; (2) description of the findings related to prevalence and risk factors; and (3) statistical summary of the findings of each study. The statistical summary included percentages for prevalence and calculated risk ratios or odds ratios (whichever was applicable) with 95% confidence interval (CI) and two-sided p values. At the data analysis stage, we gave preference to studies that defined prevalence according to country and/or geographic location and studies that had information available on key demographic criteria such as age, sex, race, or ethnicity. Due to the marked heterogeneity of the included studies, we were only able to provide a descriptive summary and could not conduct a meta-analysis with pooled statistical testing.
3. Results
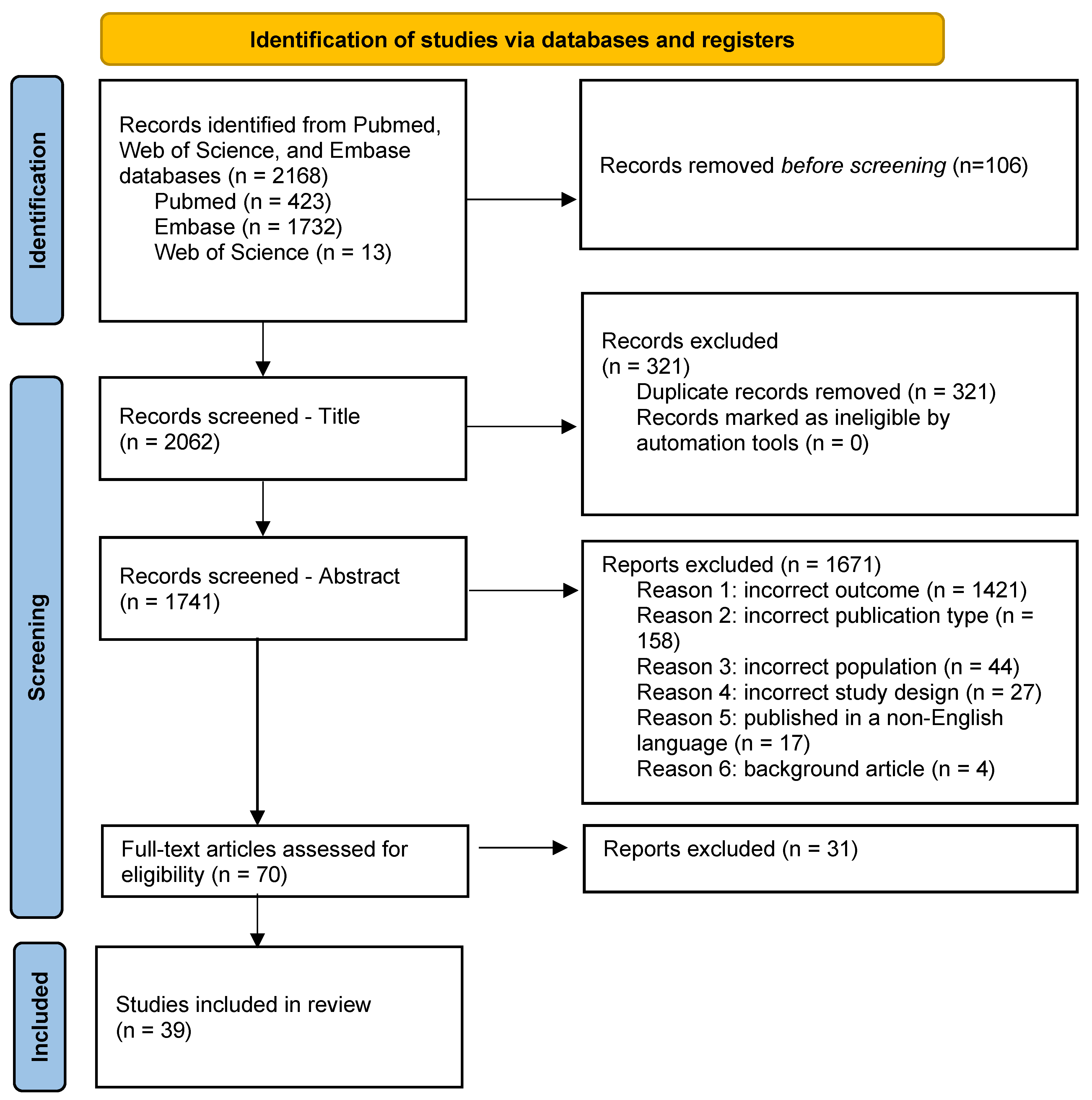
We identified 2168 articles from MESH term searches of PubMed (n = 423), Embase (n = 1732), and Web of Science (n = 12) (Figure 1). After excluding the 106 articles that did not evaluate MGUS or investigated non-modifiable risk factors for developing MGUS, we screened titles using Rayaan to eliminate duplicates (n = 321) [41]. We then screened the abstracts of the remaining 1741 articles and further excluded articles assessing the incorrect outcome (n = 1421), incorrect publication type (n = 158), incorrect population (n = 44), and incorrect study design (n = 27). We further excluded four background articles and 17 articles published in a non-English language. Thirty-one additional studies were excluded after a full-text review. Therefore, a total of 39 articles were available for review.
3.1. Geographic Prevalence
The prevalence of MGUS in studies representing 18 geographic locations ranged from 0.24% to 9.0%. (Table 1) Sociodemographic characteristics, study setting, and methods of MGUS detection varied across studies, and patient characteristics were not uniformly reported. Among population-based studies using the agarose gel electrophoresis method for MGUS diagnosis, the highest prevalence was reported in Black US women aged 50–79 at 9.0% (95% CI, 7.6–10.4) [42]. In a comparative study of Black Ghanaian males versus White US males from Olmsted County, Minnesota (Midwest USA), aged 50–74, the prevalence of MGUS was 5.84% (95% CI, 4.27–7.40) in Black Ghanaian males [43]. Additionally, both the Iceland Age, Gene/Environment Susceptibility–Reykjavik (AGES) and the recent Iceland Screens, Treats, or Prevents Multiple Myeloma (iSTOP-MM) population-based studies report an approximate 5% prevalence of MGUS among patients aged > 50 in Iceland (AGES: 5.2%; iSTOP-MM: 5%; 95% CI 4.9–5.2%) [44,45]. In a population-based study by Kyle et al. involving predominantly White residents of Olmsted County, Minnesota, USA, MGUS prevalence was 3.2% (95% CI 3.0–3.5) in individuals > 50 years [46]. A population-based study of Korean individuals > 65 years reported an MGUS prevalence of 3.3% (95% CI, 2.0–4.6), which is comparatively lower than the prevalence in Western countries for the age range studied [47]. Furthermore, in a large Japanese population of atomic bomb survivors in Nagasaki aged > 50 years diagnosed by the cellulose acetate method, the prevalence of MGUS was 2.4% (95% CI, 2.0–2.6), which is similar to the prevalence reported in a small cohort of 146 Japanese patients aged 63–95 years diagnosed by the agarose gel electrophoresis method in Yokohama, Japan (2.7%; 95% CI not reported) [48,49]. Meanwhile, MGUS prevalence in a French study using the cellulose acetate method for diagnosis was 1.10% (95% CI, not reported) [50]. An MGUS prevalence of 0.8 (95% CI, 0.3–1.4) was reported in a population-based study from China [51]. Notably, some studies also included patients < 50 years of age, for which the prevalence of MGUS was lower overall. For example, Landgren et al. evaluated 12,372 patients aged 10–49 years and reported a prevalence of 0.34% (95% CI 0.11–0.45) [28]. In Nigeria, the prevalence of MGUS was reported in a population study of 410 healthy subjects aged 20–80 at 0.24% (95% CI 0.01–1.38) [52]. Age-specific MGUS prevalence was not evaluated in this study.
Several large hospital-based studies using the agarose gel method for the diagnosis of MGUS also provide important data regarding geographic prevalence estimates. An MGUS prevalence of 6.3% was reported in a study of 6624 patients at King Fahad National Guard Hospital in Riyadh, Saudi Arabia [53]. In a North Indian hospital, the prevalence of MGUS was reported as 1.43% (95% CI not reported) in a cohort of 3429 patients [54]. A hospital-based study of 154,597 patients over the age of 50 at Peking Union Medical College in Beijing, China, reported an MGUS prevalence of 1.11% (95% CI, 1.02–1.18) [51,55]. Among hospital-based studies utilizing higher sensitivity capillary zone electrophoresis techniques, the highest prevalence of MGUS was reported at 8.19% (95% CI, not reported) in a Taiwanese hospital-based study of patients aged > 50 years [56]. Similarly, one hospital-based study of Black South African males aged > 30 years reported an MGUS prevalence of approximately 8% (age > 30 years: 8.03%; 95% CI, 5.32–10.74, age > 50 years—8.11; 5.63–11.54) [57]. In an older population (>51 to >90), an Italian study by Vernocchi et al. found an MGUS prevalence of 6.0% (95% CI, 5.7–6.3) [58]. Studies from Australia and Germany reported MGUS prevalence of 4.6% (95% CI 3.8–5.3%) and 3.5% (95% CI 3.0–4.1) in participants approximately 50 years and older, respectively [59,60].

Table 1.
Geographic prevalence of MGUS in various studies.
| Reference | Geographic Location | Age | Setting | Diagnostic Method | Diagnostic Criteria | Sample Size | Prevalence % (95% CI) | Notes |
|---|---|---|---|---|---|---|---|---|
| Bertrand et al. [42] | United States | 39 to 89 | population-based | agarose gel | M protein < 3 g/dL | 13,030 | 9.0 (7.6–10.4) | Included only Black females |
| Landgren et al. [43] | Ghana | 50 to 74 | population-based | agarose gel | M protein < 3 g/dL | 917 | 5.84 (4.27–7.40) | Included only Black males |
| Thordardottir [44] | Iceland | 66 to 98 | Population-based | agarose gel | M protein < 3 g/dL | 5764 | 5% (4.9–5.2) | Excluded patients diagnosed with multiple myeloma via review of the national cancer registry data |
| Love et al. [45] | Iceland | 41 to >80 | population-based | agarose gel | M protein < 3 g/dL, FLC ratio < 100, no end-organ damage | 75,422 | All ages: 3.9 (3.8–4.0) Age > 50: 5.0 (4.9–5.2) | |
| Kyle et al. [46] | USA | >50 | population-based | agarose gel | M protein < 3 g/dL | 16,485 | 3.2 (3.0–3.5) | |
| Bowden et al. [49] | Japan | 63 to 95 | population-based | agarose gel | M protein < 3 g/dL | 146 | 2.7 (not reported) | Compared prevalence of MGUS in Japan to prevalence in the US in the same age group |
| Wu et al. [51] | China | 50 to 65 | population-based | agarose gel | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage | 1000 | 0.8 (0.3–1.4) | |
| Landgren et al. [28] | USA | 10 to 49 | population-based | agarose gel | M protein < 3 g/dL | 12,372 | 0.34 (0.11–0.45) | |
| Onwah et al. [52] | Nigeria | 20 to 84 | population-based | agarose gel | M protein < 3 g/dL | 410 | 0.24 (0.01–1.38) | |
| Iwanaga et al. [48] | Japan | 42 to >80 | population-based | cellulose acetate | M protein < 3 g/dL | 52,781 | 2.1 (1.9–2.2) | |
| Saleun et al. [50] | France | 30 to >80 | population-based | cellulose acetate | M protein < 3 g/dL | 30,279 | 1.10 (not reported) | |
| Axelsson et al. [61] | Sweden | >70 | population-based | paper electrophoresis | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage | 6995 | 0.9 (not reported) | |
| Park et al. [47] | Korea | 65 to 97 | population-based | not reported | M protein < 3 g/dL | 945 | 3.3 (2.0–4.6) | |
| Suan et al. [59] | Australia | >50 | population-based | capillary zone | M protein < 3 g/dL, no end-organ damage | 2993 | 4.6 (3.8–5.3)) | |
| Eisele et al. [60] | Germany | 47 to 75 | population-based | capillary zone | M protein < 3 g/dL, no end-organ damage | 4702 | 3.5 (3.0–4.1) | |
| Tamimi et al. [53] | Saudi Arabia | Not reported | hospital-based | agarose gel | M protein < 3 g/dL, no end-organ damage | 6624 | 6.3 (not reported) | |
| Chang et al. [56] | Taiwan | 58 to 85 | hospital-based | capillary zone | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage | 327 | 8.19 (not reported) | |
| Cicero et al. [57] | South Africa | 35 to >85 | hospital-based | capillary zone | M protein < 3 g/dL | 386 | All ages: 8.03 (5.32–10.74)Age > 50: 8.11; 5.63–11.54 | Included only Black males |
| Veronicchi et al. [31] | Italy | <50 to >90 | hospital-based | capillary zone | M protein < 3 g/dL | 44,474 | 6.0 (5.7–6.3) | Prevalence reported for subjects > 50 years |
| Ma et al. [48] | China | >40 | hospital-based | capillary zone | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage | 1797 | 2.73 (not reported) | |
| Han et al. [55] | China | 25 to 96 | hospital-based | capillary zone | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage | 154,597 | All ages: 0.53 (0.49–0.57)Age ≥ 50: 1.11 (1.02–1.18) | |
| Gupta et al. [54] | North India | 40–88 | hospital-based | not reported | M protein < 3 g/dL, bone marrow < 10%, no end-organ damage, no amyloidosis attributed to plasma cell disorder | 3429 | 1.43 (not reported) |
3.2. Risk Factors for MGUS Development
3.2.1. Population-Specific Risk Factor Assessment
Few prevalence studies have also reported on risk factors associated with MGUS in specific populations. In a study of 2933 Australian participants, there was no statistically significant difference in smoking history, body mass index, and self-reported medical illnesses in patients with or without MGUS [59]. Age and male sex were the sole risk factors associated with the increased prevalence of MGUS in the Australian population [59]. Chang et al. evaluated environmental risk factors for MGUS and found that there was no association between living environment (urban or suburban) and MGUS in the Taiwanese population (0.77; 95% CI, 0.40–1.50) [56].
3.2.2. Autoimmune and Inflammatory Conditions
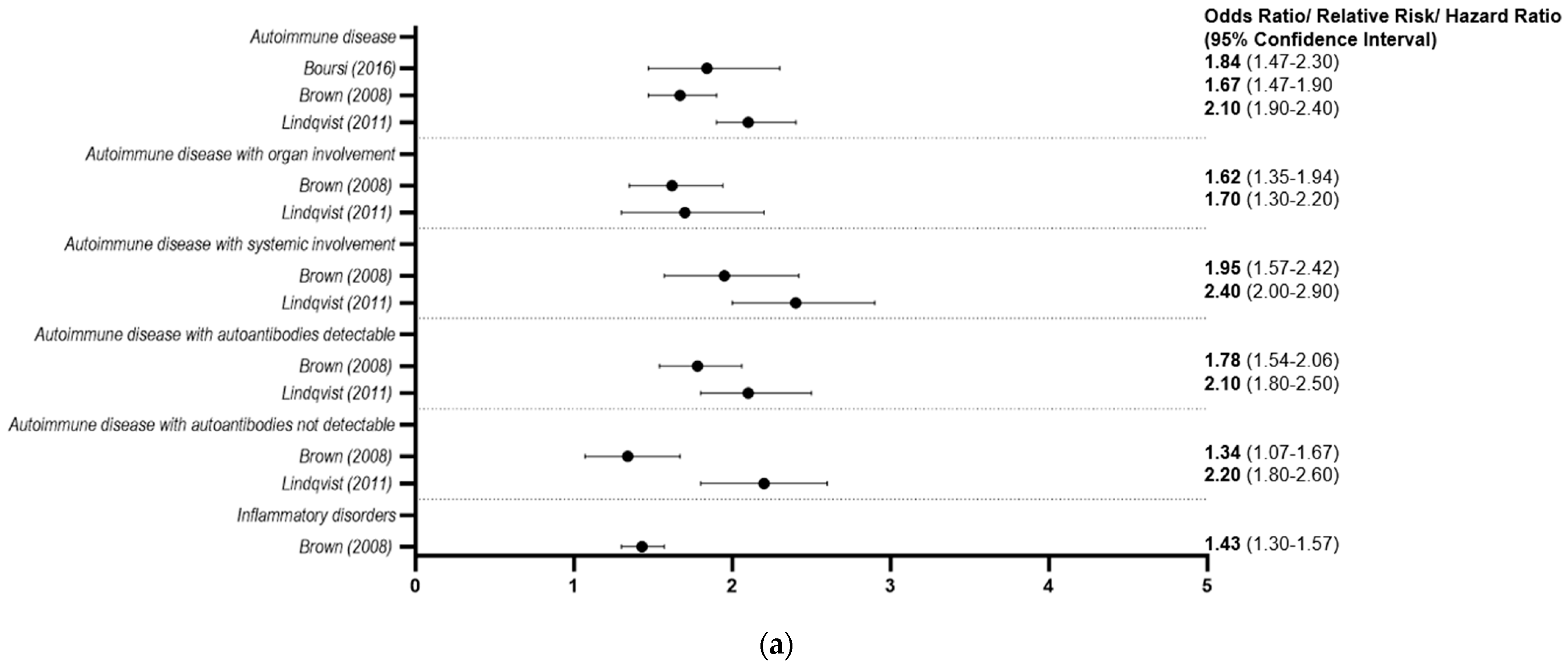
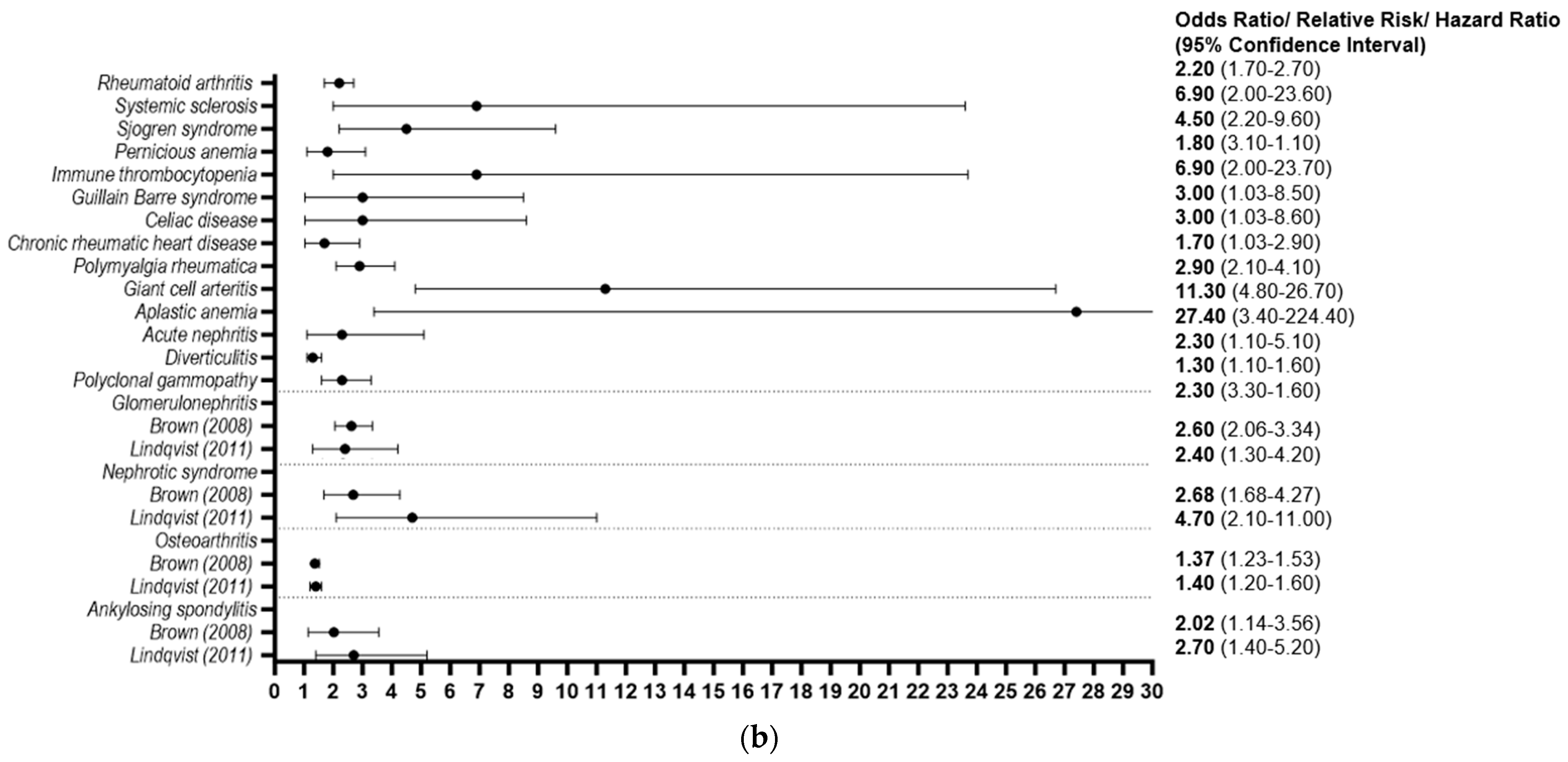
Autoimmune disease and chronic inflammation have been explored as potential risk factors for MGUS development (Figure 2). In a case–control study in the United Kingdom examining the primary care electronic medical records of 2363 MGUS patients and 9193 matched controls, a personal history of autoimmune disease was identified as a risk factor for MGUS (odds ratio [OR] = 1.84, 95% CI 1.47–2.30) [62]. Furthermore, in a retrospective cohort of four million Black and White US male veterans, there was an increased risk of MGUS in patients with autoimmune disease (relative risk [RR] = 1.67, 95% CI 1.47–1.90) [63]. Specific autoimmune diseases which portended an increased risk of MGUS included systemic sclerosis (RR = 4.21, 95% CI 1.89–9.38), autoimmune hemolytic anemia (RR = 2.58, 95% CI 1.07–6.20), pernicious anemia (RR = 1.97, 95% CI 1.16–3.34), and ankylosing spondylitis (RR = 2.02, 95% CI 1.14–3.56) [64]. Similarly, a history of autoimmune disease was associated with a significantly increased risk of MGUS in a large population-based study in Sweden (OR = 2.1, 95% CI 1.9–2.4) [64]. This relationship was particularly strong in patients with rheumatoid arthritis (RR = 2.2, 95% CI 1.7–2.7), Sjogren syndrome (RR = 4.5, 95% CI 2.2–9.6), pernicious anemia (RR = 1.8, 95% CI 1.1–3.1), Guillain–Barre (RR = 3.0, 95% CI (1.03–8.5), celiac disease (RR = 3.0, 95% CI 1.03–8.6), chronic rheumatic heart disease (RR = 1.7, 95% CI 1.03–2.9), ankylosing spondylitis (RR = 2.7, 95% CI 1.4–5.2), and polymyalgia rheumatica (RR = 2.9, 95% CI 2.1–4.1) [64].
An increased risk of MGUS was also identified in patients with chronic inflammatory conditions (RR = 1.43, 95% CI 1.30–1.57) such as glomerulonephritis (RR = 2.62, 95% CI 2.06–3.34), osteoarthritis (RR = 1.37, 95% CI 1.23–1.53), and nephrotic syndrome (RR = 2.68, 95% CI 1.68–4.27) [63].
3.2.3. Environmental Exposures
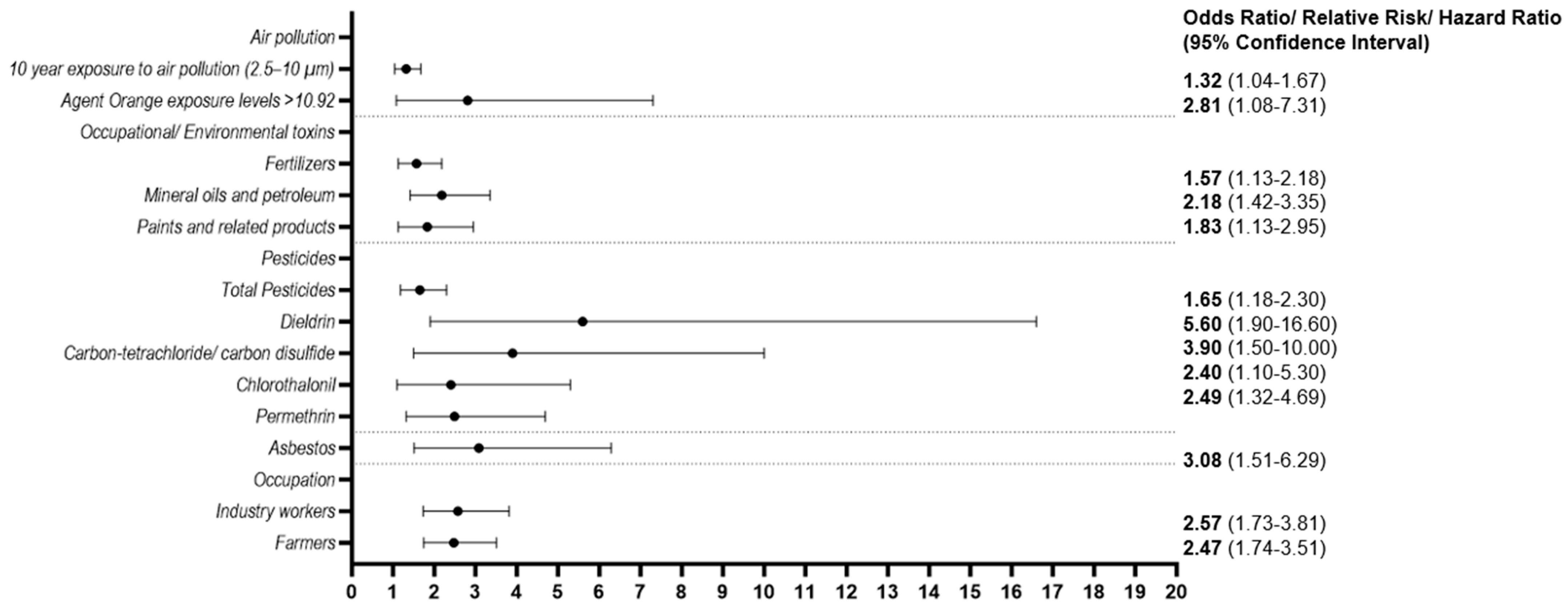
Environmental exposures, including air pollution, radiation, and occupational toxins, have also been implicated as risk factors for MGUS (Figure 3). A prospective study by Orban et al. evaluated the association between MGUS and long-term exposure to air pollution (at least 10 years). After adjusting for sociodemographic factors (age, sex, and socioeconomic status (SES)) and lifestyle factors (smoking status, physical activity, and body mass index (BMI)), the study found that there was a significant association between MGUS and long-term exposure to particulate matter with an aerodynamic diameter of 2.5–10 μm (OR: 1.32, 95% CI 1.04–1.67) [65].
Two studies examined the relationship between MGUS and radiation exposure in survivors of atomic bombings in Japan. In one study of 74,411 survivors who lived in Nagasaki city from 1988 to 2004, patients 30 years or older at the time of radiation exposure had an almost 3-fold higher risk of MGUS than those exposed at younger ages (prevalence ratio [PR] = 2.6, 95% CI 2.0–3.3, p < 0.001). Interestingly, in patients aged <20 years, there was a statistically significant increase in the prevalence of MGUS for those residing <1.5 km from the atomic bomb hypocenter (PR = 1.7, 95% CI 1.3–2.3) or for those exposed to >0.1 Gy radiation (PR = 2.02, 95% CI 1.09–3.76, p = 0.03) [48,66]. There was no significant association between MGUS and distance from the hypocenter or dose of radiation in patients 20 years and older. In another study of 38,602 atomic bomb survivors who lived in Hiroshima from 1989 to 2018, age at exposure was an independent risk factor for developing MGUS by age 70. The risk of developing MGUS was highest in survivors who were exposed to radiation at an age < 20 years old (exposed <10 years old adjusted OR = 1.72, 95% CI 1.24–2.37, p < 0.0001; exposed 10–19 years old adjusted OR = 1.40, 95% CI 1.07–1.85, p = 0.0153) [67]. In contrast to previous studies, there was no association between distance from the hypocenter at the time of bombing and MGUS risk.
In a case–control study of 285 MGUS cases in patients aged 40–89 years, asbestos, fertilizers, mineral oils, and petroleum, paints, pesticides, and radiation were all associated with a statistically significant increased risk of MGUS [68]. Radiation exposure had the highest association with MGUS (OR = 6.5, 95% CI 2.10–20.12, p < 0.0001), followed by exposure to asbestos (OR = 3.08, 95% CI 1.51–6.29, p < 0.001), and then exposure to mineral oils and petroleum (OR = 2.18, 95% CI 1.42–3.35, p < 0.025) [68]. Agent Orange and its contaminant 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) was also found to be associated with a 2.4-fold higher risk of MGUS in US Air Force personnel who were exposed to the herbicide spray compared to those who were not exposed, even after adjusting for age, race, and BMI [69]. Higher TCDD levels appeared to increase MGUS risk, with a TCDD level > 10.92 ppt conferring the highest risk for MGUS (crude OR = 2.81, 95% CI 1.08–7.31, p = 0.03). However, after adjusting OR for age, race, and BMI, there was no longer an association [69]. Moreover, a study of 678 male farmers in the Agricultural Health Study showed that there was an increased risk of MGUS with the use of specific pesticides, including dieldrin (5.6-fold, 95% CI, 1.9–16.6), carbon-tetrachloride/carbon disulfide (3.9-fold, 95% CI, 1.5–10.0), and chlorothalonil (2.4-fold, 95% CI, 1.1–5.3) [70]. A recent update to this study also found a significant association between MGUS risk and the continued use of permethrin, a widely used pesticide in the current era (OR = 2.49, 95% CI 1.32–4.69) [71].

3.2.4. Lifestyle
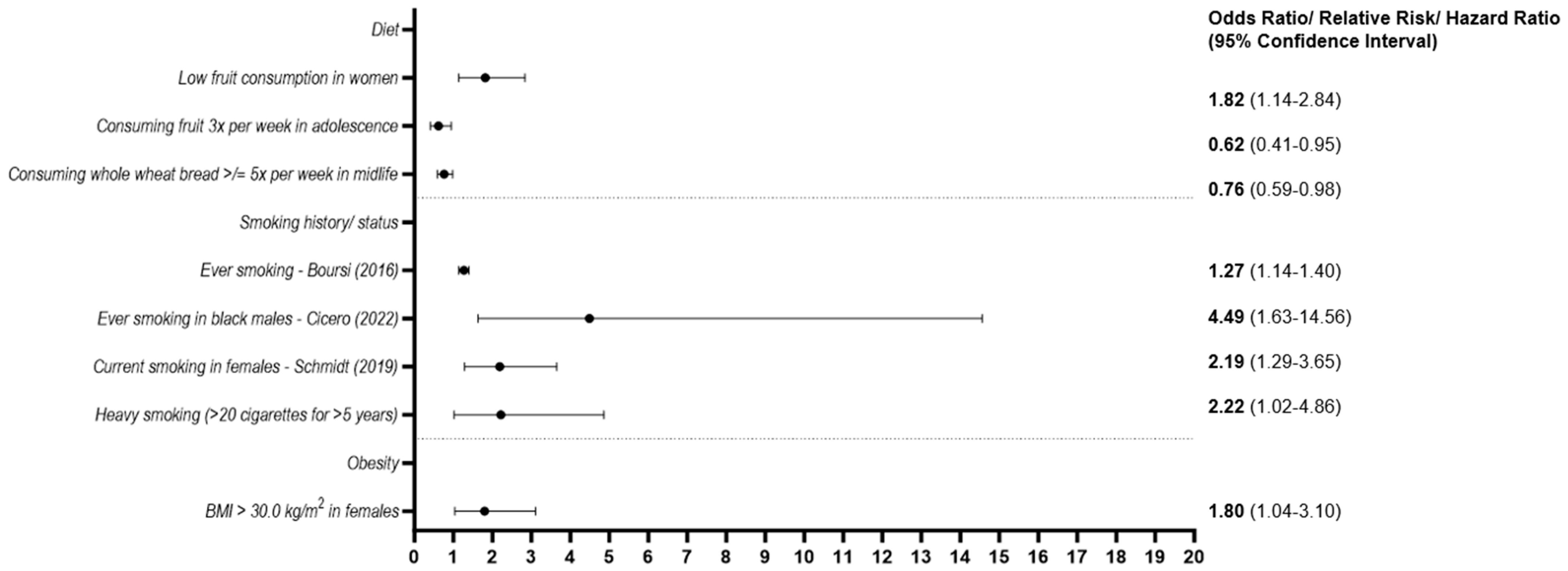
Several studies have also outlined modifiable lifestyle factors which increase the risk of developing MGUS (Figure 4). For example, a retrospective study by Pasqualetti et al. examined possible associations between substance use and occupational and environmental exposures in a cohort of 285 cases of MGUS. In this study, tobacco intake correlated with a higher risk of MGUS development (OR = 1.4, 95% CI 1.03–1.89), but the association was not statistically significant [68]. A later study by Pasqualetti et al. evaluated whether the duration and amount of tobacco smoking are significantly associated with MGUS. Notably, heavy smoking (>20 cigarettes for >5 years) was found to be significantly associated with the development of MGUS, while light smoking (<20 cigarettes/day for <5 years, <20 cigarettes/day for >5 years or >20 cigarettes/day for <5 years) did not show a significant positive association (OR = 2.22, 95% CI 1.02–4.86, p < 0.05; OR 1.31, 95% CI 0.95–2.28, p value not significant) [72]. Similarly, a nested case–control study by Boursi et al. using a primary care database found a positive association with ever-smoking history and MGUS development (OR = 1.27, 95% CI 1.14, 1.40) [62]. In a study of 4814 participants, current smoking, defined as smoking cigarettes within the past year, was positively associated with the development of MGUS in females after adjusting for age and education level (OR = 2.19, 95% CI 1.29–3.65, p = 0.003). However, current or past smoking history in males was not significantly associated with the development of MGUS in this particular study [73]. In contrast, a prospective cohort study of Black South African males highlighted that MGUS was 5.6-fold more common in those who actively smoked cigarettes compared with those who had never smoked in the univariable analysis (p = 0.001) and 4.5-fold more common when BMI and HIV status were taken into consideration (p = 0.006) [57].
Researchers have also examined the association between dietary habits and developing MGUS. In a study by Schmidt et al., low fruit consumption was found to be positively associated with the development of MGUS in women (OR = 1.82, 95% CI 1.14–2.84), with a trend toward this association in men [73]. Similarly, a population-based study in Iceland assessing dietary intake and MGUS risk found a lower risk of MGUS in participants who consumed fruit three times weekly in adolescence (14–19 years old) compared to those who did not (OR = 0.62, 95% CI 0.41–0.95). They also identified midlife consumption of whole wheat bread, greater than five times per week, as protective against MGUS (OR = 0.75, 95% CI 0.57–0.99) [44].
On the other hand, evidence has been conflicting regarding the association between obesity and MGUS depending on the measure of obesity being studied. Obesity, as measured by body mass index (BMI), was found to be significantly associated with MGUS risk in one population-based study of females aged 40–79. The study reported an increased risk of MGUS in obese females (OR = 1.80, 95% CI 1.04–3.14, p = 0.039) [74]. However, in a study assessing the association between 11 different obesity markers (weight, BMI, percent body fat, total body fat, visceral fat, subcutaneous fat, abdominal circumference, lifetime maximum weight, and measured midlife BMI) and MGUS, no association was found (ORs = 0.81 to 1.15) [75].
3.2.5. Infectious Diseases
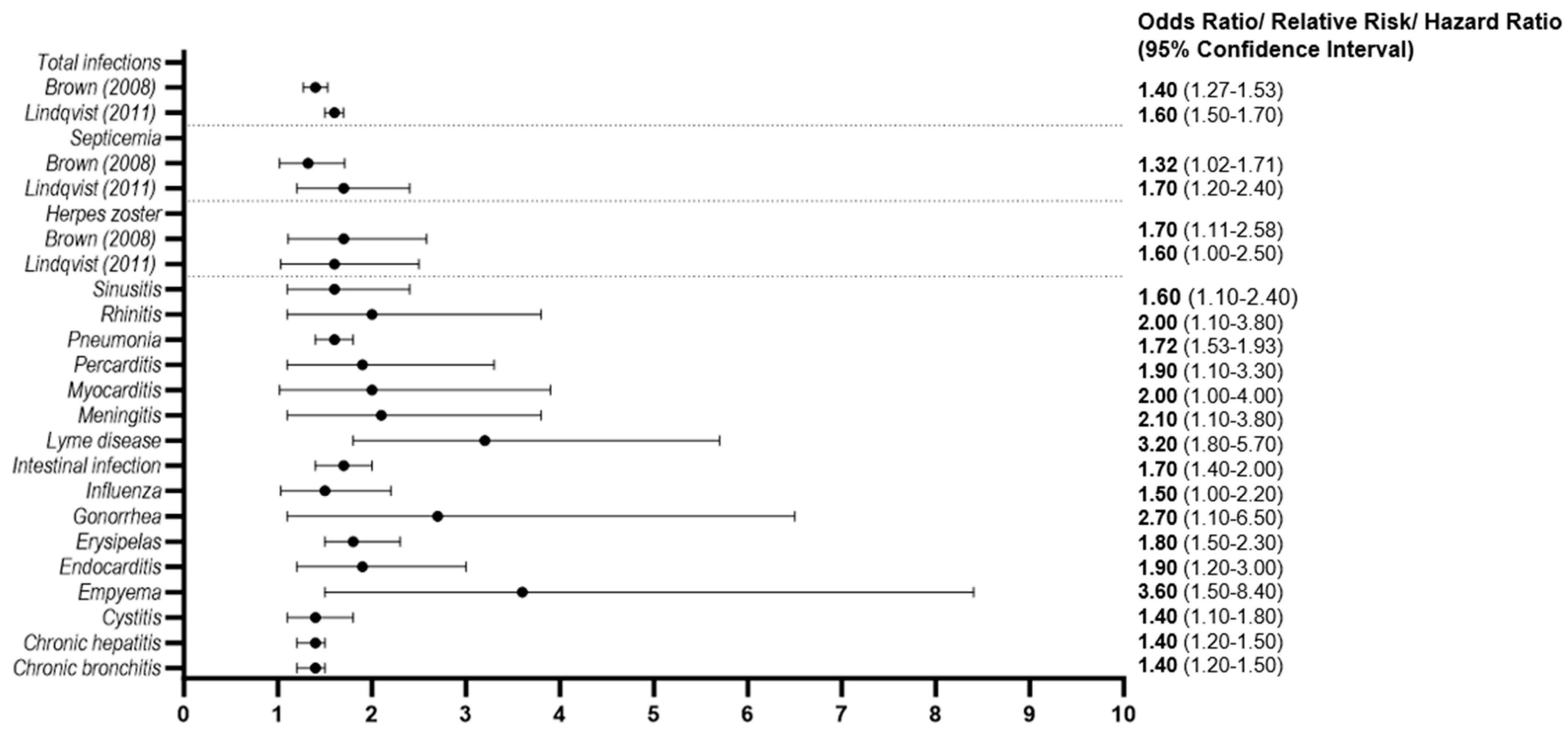
Moreover, a history of infections has also been reported as a risk factor for MGUS. Several infectious diseases have been implicated (Figure 5). Specifically, two large population-based studies in the US and Sweden confirmed that a history of infection was associated with a significantly elevated risk of MGUS (RR = 1.40, 95% CI 1.27–1.53; OR = 1.6, 95% CI 1.5–1.7), respectively [63,64]. Both studies highlighted an increased risk for MGUS in those with a history of herpes zoster (RR = 1.70, 95% CI 1.11–2.58; OR = 1.6, 95% CI 1.03–2.5), pneumonia (RR = 1.72, 95% CI 1.53–1.93; OR = 1.6, 95% CI 1.4–1.8), and prior sepsis (RR = 1.32, 95% CI 1.02–1.71; OR = 1.7, 95% CI 1.2–2.4) [63,64]. A history of empyema (OR = 3.6; 95% CI, 1.5–8.4), Lyme disease (OR = 3.2; 95% CI, 1.8–5.7), and gonorrhea (OR = 2.7; 95% CI, 1.1–6.5) conferred the highest risk for MGUS in the Swedish population-based study [64].
3.2.6. Socioeconomic Status
Socioeconomic status (SES) has also been explored as a potential risk factor for MGUS. However, results have been conflicting. An Italian study by Pasqualetti revealed that low SES was associated with a higher risk of MGUS (OR = 1.61, 95% CI 1.18–2.19), although the results were not statistically significant [68]. On the other hand, a randomized controlled trial conducted in Germany by Schmidt et al. showed that low socioeconomic status, as measured by education level or income, conferred a lower risk of MGUS independent of age, BMI, smoking status, presence of diabetes, and dietary factors [73].
4. Discussion
In this systematic review, we outline original research on the prevalence and risk factors for MGUS across geographic locations to gain further insight into the potential potency of sociocultural influences, lifestyle factors, medical conditions, and environmental exposures as risk factors for MGUS. We updated a similar systematic review conducted by Castaneda-Avila et al. in 2021, which looked at modifiable risk factors for MGUS since several landmark population-based studies have been performed since that review [76]. To ascertain the true prevalence of MGUS, we identified 22 unique studies reporting on the prevalence of MGUS across 18 geographic locations. We noted that the prevalence of MGUS is highly varied. Population-based screening studies provide the most accurate geographic prevalence estimates, while studies from hospital and outpatient settings tend to overestimate MGUS prevalence. Moreover, despite uniform criteria for MGUS diagnosis, a lack of standardization of MGUS detection methods, inconsistent use of standard diagnostic criteria for study inclusion, and variations in study design limited our ability to directly compare prevalence estimates across all studies. Nonetheless, we note that the influence of race and age on MGUS prevalence remains apparent in population-based screening studies. The highest prevalence of MGUS from population-based studies utilizing the agarose gel electrophoresis method and similar diagnostic criteria was seen in Black US women (9.0%) and Black Ghanaian men (5.84%). Meanwhile, a much lower prevalence of MGUS was reported in several countries across South and East Asia, highlighting the significance of self-identified race on the prevalence of MGUS [42,43,48,51,55]. On the other hand, an MGUS prevalence of approximately 5% was reported in both Icelanders (predominantly White population) and Black Ghanaian men of similar ages, which could suggest sociocultural and environmental factors are also at play [43,44,45]. Interestingly, in comparing two studies of similar design and inclusion criteria, there was a higher prevalence of MGUS in French (predominantly White) versus Nigerian (predominantly Black) individuals of similar age, further solidifying a potentially significant influence of sociocultural and environmental factors on MGUS prevalence in specific populations [50,52]. Additionally, population-based studies including younger patients (ages 10–20) diagnosed by the agarose gel electrophoresis method reported the lowest prevalence of MGUS regardless of the racial composition of the cohort [28,52]. Furthermore, studies from the same geographic location reported similar MGUS prevalence despite the method of diagnosis (particularly the cellulose acetate versus agarose gel methods) [48,49]. Therefore, particularly with older techniques, the method of MGUS detection is unlikely to significantly influence the geographic prevalence estimates and patterns reported. Based on our review of geographic prevalence studies, we propose that MGUS prevalence is likely highly dependent on the demographic composition of each group (particularly age and race) and population-specific sociocultural and environmental risk factors.
We further identified large cohort studies evaluating modifiable risk factors for MGUS and identified prior infections, autoimmune diseases, chronic inflammatory conditions, lifestyle factors such as tobacco use and low fruit consumption, environmental exposures, and ionizing radiation as potential risk factors. Studies are conflicting regarding the association between the development of MGUS and obesity, but evidence for the role of obesity in myelomagenesis is increasing [75,77,78]. Meanwhile, the association between MGUS and SES remains unclear as studies are conflicting. The discrepancy may, in part, be explained by varying methods used to measure SES across studies. However, it is also plausible that the relationship is population-specific and dependent on other modifiable risk factors associated with SES in various geographic locations. More studies are needed in this area.
Overall, the relationship between MGUS and the aforementioned risk factors is still poorly understood. However, the data summarized in this review support the notion that the etiology of MGUS and progressive clonal proliferation of plasma cells may be linked to chronic antigen stimulation and genomic aberrations triggered by infectious organisms, chronic inflammation, autoantigens, lifestyle factors, and environmental exposures [79]. Specifically, chronic infectious antigen exposure or chronic inflammation could trigger genetic translocations that lead to the clonal proliferation of plasma cells [80,81,82]. Furthermore, there may be a common susceptibility (such as immune dysregulation and augmented immune response) for developing plasma cell dyscrasias and autoimmune diseases [81]. In addition, obesity may lead to chronic antigen stimulation by increasing circulating leptin levels, which can cause a chronic inflammatory state via activation of both innate and acquired immune pathways [83]. Likewise, certain lifestyle conditions such as tobacco use and low fruit consumption may lead to increased inflammation via increased free radical production and decreased free radical clearance, respectively [84,85]. In particular, dietary antioxidants in fruits have anti-carcinogenic effects by trapping free radicals and protecting against oxidative stress [86,87,88]. With regard to environmental exposures, toxins, and radiation could induce DNA damage via oxidative stress, which likely increases the risk of translocations that eventually trigger monoclonal plasma cell proliferation [89]. Several studies have also shown that particulate matter exposure via pollution may cause persistent inflammation or stimulate the adaptive immune system [90,91,92]. For example, Toll-like receptors may recognize particulate matter, which then leads to antigen presentation and subsequent activation of plasma cells [90].
Our study has several limitations. First, our study did not include articles not published in English. Our selection process may have also missed eligible studies if they were not available in the databases searched. Moreover, differences in MGUS detection methods, study design, selection of patients, sample size and study power, and sociodemographic characteristics may explain inconsistencies among prevalence studies and across certain risk factors. Thus, it was difficult to understand the potential potency of modifiable risk factors versus well-known demographic risk factors such as age, sex, and race across different populations. In studies of MGUS prevalence, MGUS detection methods were heterogeneous, and in some studies, myeloma-defining events (MDEs) were not assessed. Studies that reported prevalence using more sensitive techniques could have reported slightly higher MGUS prevalence. Studies not assessing MDEs may have also reported higher MGUS prevalence by including patients with MM. Furthermore, the demographics (age, race, ethnicity, and sex) of study populations varied widely, and in some prevalence studies, race was not reported. Race and ethnicity could have been excluded from the reports because of the homogeneity of the respective populations being studied. While studies of homogenous populations could still provide clues about population-specific risk factors, data may not be generalizable. Prevalence studies also reported data from various sites, including outpatient clinics and inpatient hospital settings, as opposed to entire populations. This could have resulted in selection bias as there may be an increased likelihood of detecting MGUS in hospitalized patients or outpatient hematology clinics testing symptomatic patients. Studies that included patients admitted to the hospital are at a higher risk for detection bias due to medical comorbidities that may increase the risk of MGUS compared to the general population. Interestingly, only one study from our data set revealed an increased risk for MGUS among obese females [74]. The data on obesity and MGUS are limited by the lack of a standardized quantifiable measure of BMI since most of the data were obtained via self-reporting. Additionally, BMI alone does not account for adipose content or fat–muscle ratio, so the data are difficult to interpret. BMI also does not take into consideration other lifestyle factors, including diet and exercise, which may predispose to MGUS risk. Finally, there are likely differences in sociocultural, lifestyle, and environmental factors between populations in different geographic locations. However, it is difficult to draw strong conclusions about this based on the large variability in populations and studies assessed.
5. Conclusions
In summary, while age and race are broadly studied risk factors for MGUS, modifiable risk factors and potential geographic patterns in prevalence are less well studied. Here, we report that the geographic prevalence of MGUS is highly varied. Importantly, population-based screening studies provide the most accurate geographic prevalence estimates, but there are few of these studies in the current literature. Geographic prevalence patterns are heavily influenced by the demographic composition of each cohort (particularly age and race) and other population-specific risk factors such as sociocultural and environmental factors. Other modifiable risk factors related to chronic antigen stimulation from certain disorders, lifestyle factors, or environmental exposures appear to play a role, but large prospective population-based studies are needed to confirm causality. It remains unclear whether the association between MGUS and demographic risk factors such as age and race and ethnicity are confounded by modifiable sociocultural, lifestyle, and environmental factors. A full appraisal of causal risk factors for the development of MGUS will require further research into the complex interactions between ancestry, individual genetics, sociodemographic factors, and environmental factors. Therefore, future research should involve large prospective population-based studies across geographic sites that employ new computational methods to evaluate complex gene-environment interactions [35,45,93]. Deciphering the underlying causes of MGUS is paramount to addressing screening and prevention strategies.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/hemato4040027/s1, Table S1: Prisma checklist; Table S2: Quality of observational cohort and cross-sectional studies included in the systematic review—Risk Factors. Table S3. Quality of case-control studies included in the systematic review-Risk Factors.
Author Contributions
C.V.E. designed the study, devised the analytic plan, and analyzed data. K.P.V. and R.S. analyzed data and wrote the manuscript. All authors provided feedback and assisted in writing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The REDCap software through Boston University Clinical & Translational Science Institute was funded by the National Institutes of Health/National Center for Advancing Translational Research grant number 1UL1TR001430.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We extend our gratitude to Nadine Edwards, for providing editorial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Landgren, O.; Kyle, R.A.; Pfeiffer, R.M.; Katzmann, J.A.; Caporaso, N.E.; Hayes, R.B.; Dispenzieri, A.; Kumar, S.; Clark, R.J.; Baris, D.; et al. Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: A prospective study. Blood 2009, 113, 5412–5417. [Google Scholar] [CrossRef]
- Weiss, B.M.; Abadie, J.; Verma, P.; Howard, R.S.; Kuehl, W.M. A monoclonal gammopathy precedes multiple myeloma in most patients. Blood 2009, 113, 5418–5422. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Kumar, S. Multiple myeloma current treatment algorithms. Blood Cancer J. 2020, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Kyle, R.A.; Buadi, F.K. Advances in the Diagnosis, Classification, Risk Stratification, and Management of Monoclonal Gammopathy of Undetermined Significance: Implications for Recategorizing Disease Entities in the Presence of Evolving Scientific Evidence. Mayo Clin. Proc. 2010, 85, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R.; Plevak, M.F.; Melton, L.J. A Long-Term Study of Prognosis in Monoclonal Gammopathy of Undetermined Significance. N. Engl. J. Med. 2002, 346, 564–569. [Google Scholar] [CrossRef]
- Bida, J.P.; Kyle, R.A.; Therneau, T.M.; Melton, L.J., 3rd; Plevak, M.F.; Larson, D.R.; Dispenzieri, A.; Katzmann, J.A.; Rajkumar, S.V. Disease associations with monoclonal gammopathy of undetermined significance: A population-based study of 17,398 patients. Mayo Clin. Proc. 2009, 84, 685–693. [Google Scholar] [CrossRef]
- Schwartz, B.; Schou, M.; Ruberg, F.L.; Rucker, D.; Choi, J.; Siddiqi, O.; Monahan, K.; Køber, L.; Gislason, G.; Torp-Pedersen, C.; et al. Cardiovascular Morbidity in Monoclonal Gammopathy of Undetermined Significance. JACC CardioOncology 2022, 4, 313–322. [Google Scholar] [CrossRef]
- Kristinsson, S.Y.; Pfeiffer, R.M.; Björkholm, M.; Goldin, L.R.; Schulman, S.; Blimark, C.; Mellqvist, U.-H.; Wahlin, A.; Turesson, I.; Landgren, O. Arterial and venous thrombosis in monoclonal gammopathy of undetermined significance and multiple myeloma: A population-based study. Blood 2010, 115, 4991–4998. [Google Scholar] [CrossRef] [PubMed]
- Mouhieddine, T.H.; Weeks, L.D.; Ghobrial, I.M. Monoclonal gammopathy of undetermined significance. Blood 2019, 133, 2484–2494. [Google Scholar] [CrossRef]
- Belouni, R.; Allam, I.; Cherguelaine, K.; Berkani, L.; Belaid, B.; Berkouk, Y.; Nekkal, S.; Saidani, M.; Belhani, M.; Ghaffor, M.; et al. Epidemiological and immunochemical parameters of monoclonal plasma cell dyscrasias of 2121 cases in Algeria. Curr. Res. Transl. Med. 2020, 68, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Abell, K.; Chadwell, S.E.; Burrow, T.A.; Becker, A.P.P.; Bailey, L.; Steele, P.; Zhang, X.; Islas-Ohlmayer, M.; Bittencourt, R.; Schwartz, I.V.D.; et al. Outcomes of screening for gammopathies in children and adults with Gaucher disease type 1 in a cohort from Brazil and the United States. Am. J. Med. Genet. C Semin. Med. Genet. 2020, 184, 1052–1059. [Google Scholar] [CrossRef]
- Babel, N.; Schwarzmann, F.; Pruss, A.; Volk, H.-D.; Reinke, P. Monoclonal gammopathy of undetermined significance (MGUS) is associated with an increased frequency of Epstein-Barr Virus (EBV) latently infected B lymphocytes in long-term renal transplant patients. Transplant. Proc. 2004, 36, 2679–2682. [Google Scholar] [CrossRef]
- Bigot-Corbel, E.; Gassin, M.; Corre, I.; Le Carrer, D.; Delaroche, O.; Hermouet, S. Hepatitis C virus (HCV) infection, monoclonal immunoglobulin specific for HCV core protein, and plasma-cell malignancy. Blood 2008, 112, 4357–4358. [Google Scholar] [CrossRef]
- Hermouet, S.; Corre, I.; Gassin, M.; Bigot-Corbel, E.; Sutton, C.A.; Casey, J.W. Hepatitis C virus, human herpesvirus 8, and the development of plasma-cell leukemia. N. Engl. J. Med. 2003, 348, 178–179. [Google Scholar] [CrossRef]
- Ali, Y.M.; Urowitz, M.B.; Ibanez, D.; Gladman, D.D. Monoclonal gammopathy in systemic lupus erythematosus. Lupus 2007, 16, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Amara, S.; Dezube, B.J.; Cooley, T.P.; Pantanowitz, L.; Aboulafia, D.M. HIV-associated monoclonal gammopathy: A retrospective analysis of 25 patients. Clin. Infect. Dis. 2006, 43, 1198–1205. [Google Scholar] [CrossRef]
- Arnulf, B.; Bengoufa, D.; Sarfati, E.; Toubert, M.E.; Meignin, V.; Brouet, J.C.; Fermand, J.P. Prevalence of monoclonal gammopathy in patients with primary hyperparathyroidism: A prospective study. Arch. Intern. Med. 2002, 162, 464–467. [Google Scholar] [CrossRef]
- Eder, L.; Thavaneswaran, A.; Pereira, D.; Sussman, G.; Gladman, D.D. Prevalence of Monoclonal Gammopathy Among Patients with Psoriatic Arthritis. J. Rheumatol. 2012, 39, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Garton, M.J.; Keir, G.; Dickie, A.; Steven, M.; Rennie, J.A. Prevalence and long-term significance of paraproteinaemia in rheumatoid arthritis. Rheumatol. Oxf. 2006, 45, 355–356. [Google Scholar] [CrossRef]
- Geller, H.I.; Singh, A.; Mirto, T.M.; Padera, R.; Mitchell, R.; Laubach, J.P.; Falk, R.H. Prevalence of Monoclonal Gammopathy in Wild-Type Transthyretin Amyloidosis. Mayo Clin. Proc. 2017, 92, 1800–1805. [Google Scholar] [CrossRef]
- Heer, M.; Joller-Jemelka, H.; Fontana, A.; Seefeld, U.; Schmid, M.; Ammann, R. Monoclonal gammopathy in chronic active hepatitis. Liver 1984, 4, 255–263. [Google Scholar] [CrossRef]
- Papadaki, H.A.; Eliopoulos, D.G.; Ponticoglou, C.; Eliopoulos, G.D. Increased frequency of monoclonal gammopathy of undetermined significance in patients with nonimmune chronic idiopathic neutropenia syndrome. Int. J. Hematol. 2001, 73, 339–345. [Google Scholar] [CrossRef]
- Phull, P.; Sanchorawala, V.; Connors, L.H.; Doros, G.; Ruberg, F.L.; Berk, J.L.; Sarosiek, S. Monoclonal gammopathy of undetermined significance in systemic transthyretin amyloidosis (ATTR). Amyloid 2018, 25, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, N.M.; El Deeb, M.; Nasr, A.S. Monoclonal gammopathy among patients with chronic hepatitis C virus infection. Am. J. Med. Sci. 2013, 345, 366–368. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Rajkumar, S.V. Prevalence of Monoclonal Gammopathy of Undetermined Significance: A Systematic Review. Mayo Clin. Proc. 2010, 85, 933–942. [Google Scholar] [CrossRef]
- Waxman, A.J.; Mink, P.J.; Devesa, S.S.; Anderson, W.F.; Weiss, B.M.; Kristinsson, S.Y.; McGlynn, K.A.; Landgren, O. Racial disparities in incidence and outcome in multiple myeloma: A population-based study. Blood 2010, 116, 5501–5506. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Graubard, B.I.; Kumar, S.; Kyle, R.A.; Katzmann, J.A.; Murata, K.; Costello, R.; Dispenzieri, A.; Caporaso, N.; Mailankody, S.; et al. Prevalence of myeloma precursor state monoclonal gammopathy of undetermined significance in 12372 individuals 10–49 years old: A population-based study from the National Health and Nutrition Examination Survey. Blood Cancer J. 2017, 7, e618. [Google Scholar] [CrossRef]
- Du, Z.; Weinhold, N.; Song, G.C.; Rand, K.A.; Van Den Berg, D.J.; Hwang, A.E.; Sheng, X.; Hom, V.; Ailawadhi, S.; Nooka, A.K.; et al. A meta-analysis of genome-wide association studies of multiple myeloma among men and women of African ancestry. Blood Adv. 2020, 4, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.; Tyler, J.K. Epigenetics and aging. Sci. Adv. 2016, 2, e1600584. [Google Scholar] [CrossRef] [PubMed]
- Steves, C.J.; Spector, T.D.; Jackson, S.H.D. Ageing, genes, environment and epigenetics: What twin studies tell us now, and in the future. Age Ageing 2012, 41, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Bosseboeuf, A.; Feron, D.; Tallet, A.; Rossi, C.; Charlier, C.; Garderet, L.; Caillot, D.; Moreau, P.; Cardó-Vila, M.; Pasqualini, R.; et al. Monoclonal IgG in MGUS and multiple myeloma targets infectious pathogens. JCI Insight 2017, 2, e95367. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Kyle, R.A.; Plevak, M.F.; Murray, J.A.; Therneau, T.M. Helicobacter pylori infection and monoclonal gammopathy of undetermined significance. Br. J. Haematol. 2002, 119, 706–708. [Google Scholar] [CrossRef]
- Nair, S.; Branagan, A.R.; Liu, J.; Boddupalli, C.S.; Mistry, P.K.; Dhodapkar, M.V. Clonal Immunoglobulin against Lysolipids in the Origin of Myeloma. N. Engl. J. Med. 2016, 374, 555–561. [Google Scholar] [CrossRef]
- Rögnvaldsson, S.; Love, T.J.; Thorsteinsdottir, S.; Reed, E.R.; Óskarsson, J.Þ.; Pétursdóttir, Í.; Sigurðardóttir, G.Á.; Viðarsson, B.; Önundarson, P.T.; Agnarsson, B.A.; et al. Iceland screens, treats, or prevents multiple myeloma (iStopMM): A population-based screening study for monoclonal gammopathy of undetermined significance and randomized controlled trial of follow-up strategies. Blood Cancer J. 2021, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, i4086. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Obeid, J.S.; McGraw, C.A.; Minor, B.L.; Conde, J.G.; Pawluk, R.; Lin, M.; Wang, J.; Banks, S.R.; Hemphill, S.A.; Taylor, R.; et al. Procurement of shared data instruments for Research Electronic Data Capture (REDCap). J. Biomed. Inform. 2013, 46, 259–265. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Bertrand, K.A.; Zirpoli, G.; Niharika Pillalamarri, B.; Szalat, R.; Palmer, J.R.; Kataria, Y. Prevalence of monoclonal gammopathy of undetermined significance in US black women. Am. J. Hematol. 2022, 97, E341. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Katzmann, J.A.; Hsing, A.W.; Pfeiffer, R.M.; Kyle, R.A.; Yeboah, E.D.; Biritwum, R.B.; Tettey, Y.; Adjei, A.A.; Larson, D.R.; et al. Prevalence of monoclonal gammopathy of undetermined significance among men in Ghana. Mayo Clin. Proc. 2007, 82, 1468–1473. [Google Scholar] [CrossRef] [PubMed]
- Thordardottir, M.; Lindqvist, E.K.; Lund, S.H.; Costello, R.; Burton, D.; Steingrimsdottir, L.; Korde, N.; Mailankody, S.; Eiriksdottir, G.; Launer, L.J.; et al. Dietary intake is associated with risk of multiple myeloma and its precursor disease. PLoS ONE 2018, 13, e0206047. [Google Scholar] [CrossRef]
- Love, T.J.; Rögnvaldsson, S.; Thorsteinsdottir, S.; Aspelund, T.; Reed, E.R.; Vidarsson, B.; Onundarson, P.T.; Agnarsson, B.A.; Sigurdardottir, M.; Thorsteinsdottir, I.; et al. Prevalence of MGUS Is High in the Istopmm Study but the Prevalence of IgA MGUS Does Not Increase with Age in the Way Other Immunoglobulin Subtypes Do. Blood 2022, 140, 256–258. [Google Scholar] [CrossRef]
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Larson, D.R.; Plevak, M.F.; Offord, J.R.; Dispenzieri, A.; Katzmann, J.A.; Melton, L.J., III. Prevalence of monoclonal gammopathy of undetermined significance. N. Engl. J. Med. 2006, 354, 1362–1369. [Google Scholar] [CrossRef]
- Park, H.K.; Lee, K.R.; Kim, Y.J.; Cho, H.I.; Kim, J.E.; Kim, K.W.; Kim, Y.J.; Lee, K.W.; Kim, J.H.; Bang, S.M.; et al. Prevalence of monoclonal gammopathy of undetermined significance in an elderly urban Korean population. Am. J. Hematol. 2011, 86, 752–755. [Google Scholar] [CrossRef]
- Iwanaga, M.; Tagawa, M.; Tsukasaki, K.; Kamihira, S.; Tomonaga, M. Prevalence of monoclonal gammopathy of undetermined significance: Study of 52,802 persons in Nagasaki City, Japan. Mayo Clin. Proc. 2007, 82, 1474–1479. [Google Scholar] [CrossRef]
- Bowden, M.; Crawford, J.; Cohen, H.J.; Noyama, O. A comparative study of monoclonal gammopathies and immunoglobulin levels in Japanese and United States elderly. J. Am. Geriatr. Soc. 1993, 41, 11–14. [Google Scholar] [CrossRef]
- Saleun, J.P.; Vicariot, M.; Deroff, P.; Morin, J.F. Monoclonal gammopathies in the adult population of Finistere, France. J. Clin. Pathol. 1982, 35, 63–68. [Google Scholar] [CrossRef]
- Wu, S.P.; Minter, A.; Costello, R.; Zingone, A.; Lee, C.K.; Au, W.Y.; Landgren, O. MGUS prevalence in an ethnically Chinese population in Hong Kong. Blood 2013, 121, 2363–2364. [Google Scholar] [CrossRef]
- Onwah, A.L.; Adeyemo, T.A.; Adediran, A.; Ajibola, S.O.; Akanmu, A.S. Prevalence and type of monoclonal gammopathy of undetermined significance in an apparently healthy Nigerian population: A cross sectional study. BMC Blood Disord. 2012, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, W.; Alaskar, A.; Alassiri, M.; Alsaeed, W.; Alarifi, S.A.; Alenzi, F.Q.; Jawdat, D. Monoclonal gammopathy in a tertiary referral hospital. Clin. Biochem. 2010, 43, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Dahiya, M.; Kumar, L.; Shekhar, V.; Sharma, A.; Ramakrishnan, L.; Sharma, O.D.; Begum, A. Prevalence of Monoclonal Gammopathy of Undetermined Significance in India-A Hospital-based Study. Clin. Lymphoma Myeloma Leuk. 2018, 18, e345–e350. [Google Scholar] [CrossRef]
- Han, J.H.; Wang, J.N.; Zhang, Y.L.; Cao, X.X.; Zhou, D.B.; Xu, T.D.; Su, W.; Li, J. Prevalence of monoclonal gammopathy of undetermined significance in a large population with annual medical check-ups in China. Blood Cancer J. 2020, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Su, M.J.; Lee, S.J.; Tsai, Y.H.; Kuo, L.Y.; Lin, I.H.; Huang, H.L.; Yen, T.H.; Chu, F.Y. The Immunotyping Distribution of Serum Monoclonal Paraprotein and Environmental Impact on Multiple Myeloma (MM) and Monoclonal Gammopathy of Uncertain Significance (MGUS) in Taiwan: A Medical Center-Based Experience. Asian Pac. J. Cancer Prev. 2016, 17, 395–399. [Google Scholar] [CrossRef]
- Cicero, K.I.; Joffe, M.; Patel, M.; Chiuzan, C.; Pentz, A.; Ruff, P.; Lentzsch, S.; Leng, S.; Jacobson, J.S.; Rebbeck, T.R.; et al. Prevalence of Monoclonal Gammopathy of Undetermined Significance in Black South African Men. Cancer Epidemiol. Biomark. Prev. 2022, 31, 2192–2198. [Google Scholar] [CrossRef]
- Vernocchi, A.; Longhi, E.; Lippi, G.; Gelsumini, S. Increased Monoclonal Components: Prevalence in an Italian Population of 44 474 Outpatients Detected by Capillary Electrophoresis. J. Med. Biochem. 2016, 35, 50–54. [Google Scholar] [CrossRef]
- Suan, D.; Hughan, M.; Bates, S.; Rochtchina, E.; Empson, M.; Mitchell, P.; Fulcher, D.A. Prevalence of paraproteinaemia in older Australians. Intern. Med. J. 2012, 42, 165–169. [Google Scholar] [CrossRef]
- Eisele, L.; Dürig, J.; Hüttmann, A.; Dührsen, U.; Assert, R.; Bokhof, B.; Erbel, R.; Mann, K.; Jöckel, K.H.; Moebus, S. Prevalence and progression of monoclonal gammopathy of undetermined significance and light-chain MGUS in Germany. Ann. Hematol. 2012, 91, 243–248. [Google Scholar] [CrossRef]
- Axelsson, U.; Bachmann, R.; Hällén, J. Frequency of Pathological Proteins (M-components) in 6,995 Sera from an Adult Population. Acta Med. Scand. 2009, 179, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Boursi, B.; Weiss, B.M.; Haynes, K.; Mamtani, R.; Yang, Y.X. Reappraisal of risk factors for monoclonal gammopathy of undetermined significance. Am. J. Hematol. 2016, 91, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.M.; Gridley, G.; Check, D.; Landgren, O. Risk of multiple myeloma and monoclonal gammopathy of undetermined significance among white and black male United States veterans with prior autoimmune, infectious, inflammatory, and allergic disorders. Blood 2008, 111, 3388–3394. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, E.K.; Goldin, L.R.; Landgren, O.; Blimark, C.; Mellqvist, U.H.; Turesson, I.; Wahlin, A.; Bjorkholm, M.; Kristinsson, S.Y. Personal and family history of immune-related conditions increase the risk of plasma cell disorders: A population-based study. Blood 2011, 118, 6284–6291. [Google Scholar] [CrossRef]
- Orban, E.; Arendt, M.; Hennig, F.; Lucht, S.; Eisele, L.; Jakobs, H.; Durig, J.; Hoffmann, B.; Jockel, K.H.; Moebus, S. Is long-term particulate matter and nitrogen dioxide air pollution associated with incident monoclonal gammopathy of undetermined significance (MGUS)? An analysis of the Heinz Nixdorf Recall study. Environ. Int. 2017, 108, 237–245. [Google Scholar] [CrossRef]
- Iwanaga, M.; Tagawa, M.; Tsukasaki, K.; Matsuo, T.; Yokota, K.; Miyazaki, Y.; Fukushima, T.; Hata, T.; Imaizumi, Y.; Imanishi, D.; et al. Relationship between monoclonal gammopathy of undetermined significance and radiation exposure in Nagasaki atomic bomb survivors. Blood 2009, 113, 1639–1650. [Google Scholar] [CrossRef]
- Fujimura, K.; Sugiyama, A.; Akita, T.; Ohisa, M.; Nagashima, S.; Katayama, K.; Maeda, R.; Tanaka, J. Screening for M-proteinemia consisting of monoclonal gammopathy of undetermined significance and multiple myeloma for 30 years among atomic bomb survivors in Hiroshima. Int. J. Hematol. 2021, 113, 576–585. [Google Scholar] [CrossRef]
- Pasqualetti, P.; Collacciani, A.; Casale, R. Risk of monoclonal gammopathy of undetermined significance: A case-referent study. Am. J. Hematol. 1996, 52, 217–220. [Google Scholar] [CrossRef]
- Landgren, O.; Shim, Y.K.; Michalek, J.; Costello, R.; Burton, D.; Ketchum, N.; Calvo, K.R.; Caporaso, N.; Raveche, E.; Middleton, D.; et al. Agent Orange Exposure and Monoclonal Gammopathy of Undetermined Significance: An Operation Ranch Hand Veteran Cohort Study. JAMA Oncol. 2015, 1, 1061–1068. [Google Scholar] [CrossRef]
- Landgren, O.; Kyle, R.A.; Hoppin, J.A.; Beane Freeman, L.E.; Cerhan, J.R.; Katzmann, J.A.; Rajkumar, S.V.; Alavanja, M.C. Pesticide exposure and risk of monoclonal gammopathy of undetermined significance in the Agricultural Health Study. Blood 2009, 113, 6386–6391. [Google Scholar] [CrossRef]
- Hofmann, J.N.; Beane Freeman, L.E.; Murata, K.; Andreotti, G.; Shearer, J.J.; Thoren, K.; Ramanathan, L.; Parks, C.G.; Koutros, S.; Lerro, C.C.; et al. Lifetime Pesticide Use and Monoclonal Gammopathy of Undetermined Significance in a Prospective Cohort of Male Farmers. Env. Health Perspect. 2021, 129, 17003. [Google Scholar] [CrossRef]
- Pasqualetti, P.; Festuccia, V.; Acitelli, P.; Collacciani, A.; Giusti, A.; Casale, R. Tobacco smoking and risk of haematological malignancies in adults: A case-control study. Br. J. Haematol. 1997, 97, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Debold, E.; Frank, M.; Arendt, M.; Dragano, N.; Durig, J.; Duhrsen, U.; Moebus, S.; Erbel, R.; Jockel, K.H.; et al. Socioeconomic Position is Positively Associated with Monoclonal Gammopathy of Undetermined Significance in a Population-based Cohort Study. Ann. Hematol. 2019, 98, 2761–2767. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Rajkumar, S.V.; Pfeiffer, R.M.; Kyle, R.A.; Katzmann, J.A.; Dispenzieri, A.; Cai, Q.; Goldin, L.R.; Caporaso, N.E.; Fraumeni, J.F.; et al. Obesity is associated with an increased risk of monoclonal gammopathy of undetermined significance among black and white women. Blood 2010, 116, 1056–1059. [Google Scholar] [CrossRef] [PubMed]
- Thordardottir, M.; Lindqvist, E.K.; Lund, S.H.; Costello, R.; Burton, D.; Korde, N.; Mailankody, S.; Eiriksdottir, G.; Launer, L.J.; Gudnason, V.; et al. Obesity and risk of monoclonal gammopathy of undetermined significance and progression to multiple myeloma: A population-based study. Blood Adv. 2017, 1, 2186–2192. [Google Scholar] [CrossRef]
- Castaneda-Avila, M.A.; Ulbricht, C.M.; Epstein, M.M. Risk factors for monoclonal gammopathy of undetermined significance: A systematic review. Ann. Hematol. 2021, 100, 855–863. [Google Scholar] [CrossRef]
- Chang, S.-H.; Luo, S.; Thomas, T.S.; O’Brian, K.K.; Colditz, G.A.; Carlsson, N.P.; Carson, K.R. Obesity and the Transformation of Monoclonal Gammopathy of Undetermined Significance to Multiple Myeloma: A Population-Based Cohort Study. J. Natl. Cancer Inst. 2017, 109, djw264. [Google Scholar] [CrossRef]
- Parikh, R.; Tariq, S.M.; Marinac, C.R.; Shah, U.A. A comprehensive review of the impact of obesity on plasma cell disorders. Leukemia 2022, 36, 301–314. [Google Scholar] [CrossRef]
- Sanoja-Flores, L.; Flores-Montero, J.; Garcés, J.J.; Paiva, B.; Puig, N.; García-Mateo, A.; García-Sánchez, O.; Corral-Mateos, A.; Burgos, L.; Blanco, E.; et al. Next generation flow for minimally-invasive blood characterization of MGUS and multiple myeloma at diagnosis based on circulating tumor plasma cells (CTPC). Blood Cancer J. 2018, 8, 117. [Google Scholar] [CrossRef]
- Fonseca, R.; Barlogie, B.; Bataille, R.; Bastard, C.; Bergsagel, P.L.; Chesi, M.; Davies, F.E.; Drach, J.; Greipp, P.R.; Kirsch, I.R.; et al. Genetics and cytogenetics of multiple myeloma: A workshop report. Cancer Res. 2004, 64, 1546–1558. [Google Scholar] [CrossRef]
- Shimanovsky, A.; Alvarez Argote, J.; Murali, S.; Dasanu, C.A. Autoimmune manifestations in patients with multiple myeloma and monoclonal gammopathy of undetermined significance. BBA Clin. 2016, 6, 12–18. [Google Scholar] [CrossRef]
- Fonseca, R.; Bailey, R.J.; Ahmann, G.J.; Rajkumar, S.V.; Hoyer, J.D.; Lust, J.A.; Kyle, R.A.; Gertz, M.A.; Greipp, P.R.; Dewald, G.W. Genomic abnormalities in monoclonal gammopathy of undetermined significance. Blood 2002, 100, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pérez, A.; Vilariño-García, T.; Fernández-Riejos, P.; Martín-González, J.; Segura-Egea, J.J.; Sánchez-Margalet, V. Role of leptin as a link between metabolism and the immune system. Cytokine Growth Factor. Rev. 2017, 35, 71–84. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.S.; Saedisomeolia, A.; Starkey, M.R.; Collison, A.; Wark, P.A.B.; Wood, L.G. Effects of fruit and vegetable consumption on inflammatory biomarkers and immune cell populations: A systematic literature review and meta-analysis. Am. J. Clin. Nutr. 2018, 108, 136–155. [Google Scholar] [CrossRef]
- Martín de Diego, C.E.; Gómez de Terreros Sánchez, F.J.; Caro de Miguel, M.C.; Medina Font, J.; Matesanz Ruiz, C.; Gómez de Terreros Caro, J. C-reactive protein value related to a smoking history and composition of nicotine and tobacco tar. An. Med. Interna Madr. Spain 1984 2006, 23, 3–10. [Google Scholar] [CrossRef]
- Diplock, A.T.; Charleux, J.L.; Crozier-Willi, G.; Kok, F.J.; Rice-Evans, C.; Roberfroid, M.; Stahl, W.; Viña-Ribes, J. Functional food science and defence against reactive oxidative species. Br. J. Nutr. 1998, 80 (Suppl. S1), S77–S112. [Google Scholar] [CrossRef]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef]
- Bouayed, J.; Bohn, T. Exogenous antioxidants—Double-edged swords in cellular redox state: Health beneficial effects at physiologic doses versus deleterious effects at high doses. Oxid. Med. Cell. Longev. 2010, 3, 228–237. [Google Scholar] [CrossRef]
- Møller, P.; Danielsen, P.H.; Karottki, D.G.; Jantzen, K.; Roursgaard, M.; Klingberg, H.; Jensen, D.M.; Christophersen, D.V.; Hemmingsen, J.G.; Cao, Y.; et al. Oxidative stress and inflammation generated DNA damage by exposure to air pollution particles. Mutat. Res. Mutat. Res. 2014, 762, 133–166. [Google Scholar] [CrossRef] [PubMed]
- Miyata, R.; Van Eeden, S.F. The innate and adaptive immune response induced by alveolar macrophages exposed to ambient particulate matter. Toxicol. Appl. Pharmacol. 2011, 257, 209–226. [Google Scholar] [CrossRef]
- Viehmann, A.; Hertel, S.; Fuks, K.; Eisele, L.; Moebus, S.; Möhlenkamp, S.; Nonnemacher, M.; Jakobs, H.; Erbel, R.; Jöckel, K.-H.; et al. Long-term residential exposure to urban air pollution, and repeated measures of systemic blood markers of inflammation and coagulation. Occup. Environ. Med. 2015, 72, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Hennig, F.; Fuks, K.; Moebus, S.; Weinmayr, G.; Memmesheimer, M.; Jakobs, H.; Bröcker-Preuss, M.; Führer-Sakel, D.; Möhlenkamp, S.; Erbel, R.; et al. Association between Source-Specific Particulate Matter Air Pollution and hs-CRP: Local Traffic and Industrial Emissions. Environ. Health Perspect. 2014, 122, 703–710. [Google Scholar] [CrossRef] [PubMed]
- El-Khoury, H.; Lee, D.J.; Alberge, J.-B.; Redd, R.; Cea-Curry, C.J.; Perry, J.; Barr, H.; Murphy, C.; Sakrikar, D.; Barnidge, D.; et al. Prevalence of monoclonal gammopathies and clinical outcomes in a high-risk US population screened by mass spectrometry: A multicentre cohort study. Lancet Haematol. 2022, 9, e340–e349. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram. We screened article titles using Rayaan to exclude 321 duplicates, 106 articles that did not evaluate MGUS or non-modifiable risk factors, and articles assessing the wrong outcome, publication type, population, and study design [41]. We further excluded (four) background articles, 17 articles published in a non-English language, and 31 articles after a full-text review. Thirty-nine articles were reviewed.
Figure 1.
PRISMA flow diagram. We screened article titles using Rayaan to exclude 321 duplicates, 106 articles that did not evaluate MGUS or non-modifiable risk factors, and articles assessing the wrong outcome, publication type, population, and study design [41]. We further excluded (four) background articles, 17 articles published in a non-English language, and 31 articles after a full-text review. Thirty-nine articles were reviewed.

Figure 2.
Forest plots of autoimmune and inflammatory disorders reported to significantly increase risk of MGUS: (a) overall autoimmune and inflammatory states associated with a significantly increased risk of MGUS [62,63,64]; (b) specific autoimmune and inflammatory disorders associated with a significantly increased risk of MGUS [63,64].
Figure 2.
Forest plots of autoimmune and inflammatory disorders reported to significantly increase risk of MGUS: (a) overall autoimmune and inflammatory states associated with a significantly increased risk of MGUS [62,63,64]; (b) specific autoimmune and inflammatory disorders associated with a significantly increased risk of MGUS [63,64].


Figure 4.
Forest plot of lifestyle factors reported in the literature to be associated with MGUS risk [44,57,62,6872,73,74,75].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Verma, K.P.; Steuer, R.; Edwards, C.V. Geographic Prevalence Patterns and Modifiable Risk Factors for Monoclonal Gammopathy of Undetermined Significance. Hemato 2023, 4, 331-349. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato4040027
AMA Style
Verma KP, Steuer R, Edwards CV. Geographic Prevalence Patterns and Modifiable Risk Factors for Monoclonal Gammopathy of Undetermined Significance. Hemato. 2023; 4(4):331-349. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato4040027
Chicago/Turabian StyleVerma, Karina P., Rebecca Steuer, and Camille V. Edwards. 2023. "Geographic Prevalence Patterns and Modifiable Risk Factors for Monoclonal Gammopathy of Undetermined Significance" Hemato 4, no. 4: 331-349. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato4040027