
Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
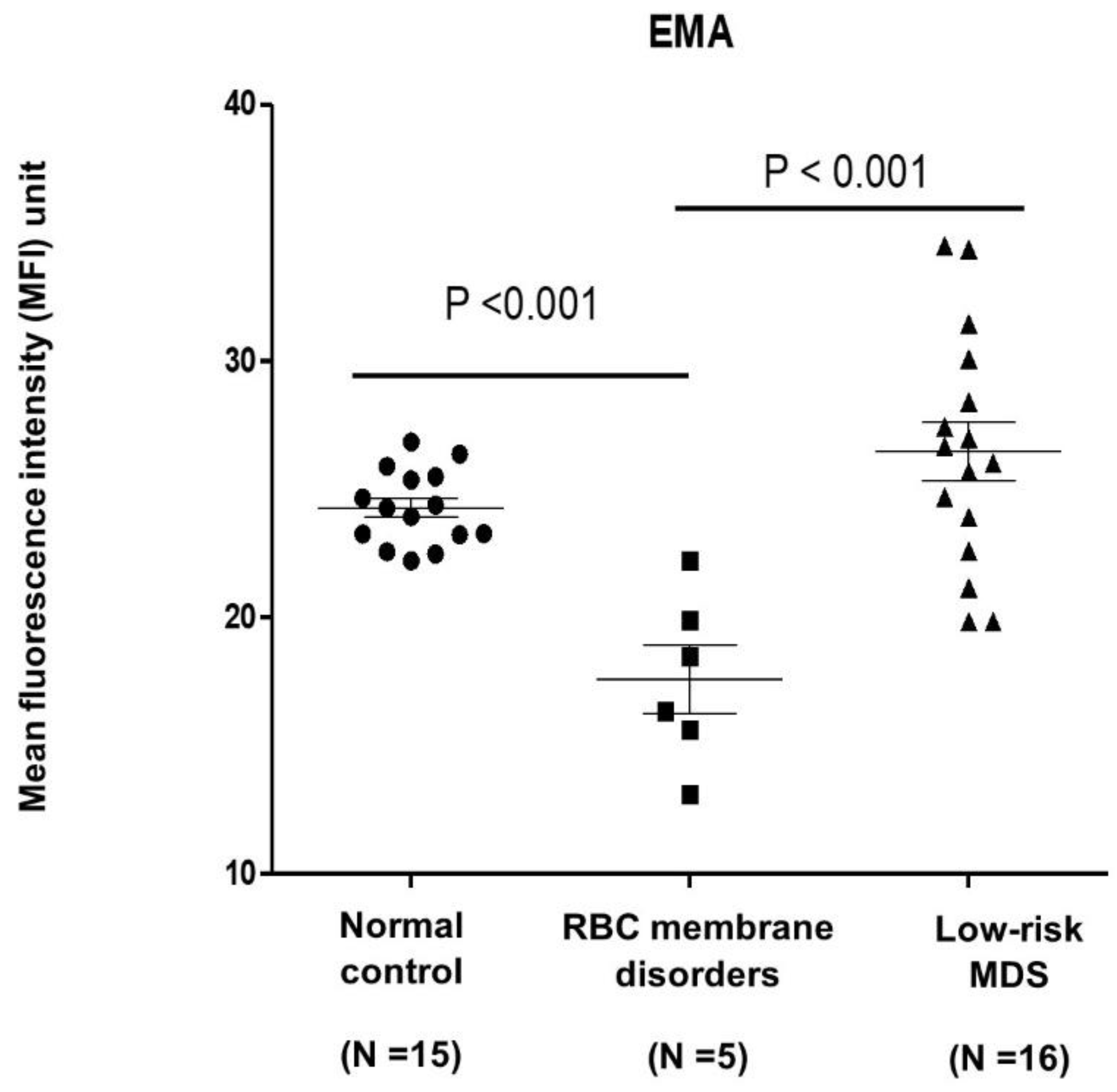
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Castelli, R.; Schiavon, R.; Rossi, V.; Deliliers, G.L. Management of anemia in low-risk myelodysplastic syndromes treated with erythropoiesis-stimulating agents newer and older agents. Med Oncol. 2018, 35, 76. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Barosi, G.; Berzuini, C.; Dacco, M.; Orlandi, E.; Stefanelli, M.; Ascari, E. Quantitative evaluation of erythropoietic activity in dysmyelopoietic syndromes. Br. J. Haematol. 1982, 50, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Liu, J.; Xue, F.; Halverson, G.; Reid, M.; Guo, A.; Chen, L.; Raza, A.; Galili, N.; Jaffray, J.; et al. Isolation and functional characterization of human erythroblasts at distinct stages: Implications for understanding of normal and disordered erythropoiesis in vivo. Blood 2013, 121, 3246–3253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komrokji, R.S.; Al Ali, M.N.; Hussaini, M.O.; Sallman, D.A.; Rollison, D.E.; Padron, E. U2AF1 and EZH2 Mutations Are Associated with Non-Immune Hemolytic Anemia in Myelodysplastic Syndromes. Blood 2020, 136, 35–36. [Google Scholar] [CrossRef]
- Glenthøj, A.; Sharfo, A.; Brieghel, C.; Nardo-Marino, A.; Birgens, H.; Petersen, J.B. Improving the EMA Binding Test by Using Commercially Available Fluorescent Beads. Front. Physiol. 2020, 11, 569289. [Google Scholar] [CrossRef]
- Picard, V.; Proust, A.; Eveillard, M.; Flatt, J.F.; Couec, M.-L.; Caillaux, G.; Feneant-Thibault, M.; Finkelstein, A.; Raphael, M.; Delaunay, J.; et al. Homozygous Southeast Asian ovalocytosis is a severe dyserythropoietic anemia associated with distal renal tubular acidosis. Blood 2014, 123, 1963–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, M.-J.; Smythe, J.S.; Mushens, R. Eosin-5-maleimide binding to band 3 and Rh-related proteins forms the basis of a screening test for hereditary spherocytosis. Br. J. Haematol. 2004, 124, 106–113. [Google Scholar] [CrossRef]
- Adan, A.; Alizada, G.; Kiraz, Y.; Baran, Y.; Nalbant, A. Flow cytometry: Basic principles and applications. Crit. Rev. Biotechnol. 2016, 37, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Park, C.-J.; Lee, B.-R.; Cho, Y.-U.; Jang, S.; Kim, N.; Koh, K.-N.; Im, H.-J.; Seo, J.-J.; Park, E.S.; et al. Comparison Study of the Eosin-5′-Maleimide Binding Test, Flow Cytometric Osmotic Fragility Test, and Cryohemolysis Test in the Diagnosis of Hereditary Spherocytosis. Am. J. Clin. Pathol. 2014, 142, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Huang, Y.; Pinheiro, R.F.; Xue, F.; Hu, J.; Iverson, N.; Hoehn, D.; Coutinho, D.; Kayani, J.; Chernak, B.; et al. Severely impaired terminal erythroid differentiation as an independent prognostic marker in myelodysplastic syndromes. Blood Adv. 2018, 2, 1393–1402. [Google Scholar] [CrossRef]
- Ciepiela, O.; Adamowicz-Salach, A.; Bystrzycka, W.; Łukasik, J.; Kotuła, I. Mean corpuscular volume of control red blood cells determines the interpretation of eosin-5′-maleimide (EMA) test result in infants aged less than 6 months. Ann. Hematol. 2015, 94, 1277–1283. [Google Scholar] [CrossRef] [Green Version]
- Falay, M.; Ulusan, G.E.; Şenes, M.; Acar, İ.O. Are the Reference Ranges and Cutoff Values of Eosin-5′-Maleimide (EMA) Binding Test for Hereditary Spherocytosis Specific for Each Age Group? Clin. Lab. 2018, 64, 1101–1103. [Google Scholar] [CrossRef]


{kind=link}
| Control (N = 16) | MDS (N = 15) | RBC Membrane Disorders (N = 6) | p-Value | |
|---|---|---|---|---|
| Median (IQR) age (years) | 28 (27–30) | 76 (67–82) | 36 (27–45) | <0.001 |
| Gender, N (%) | 0.07 | |||
| Female | 11 (73.3) | 5 (31.3) | 4(66.7) | |
| Male | 4 (26.7) | 11 (68.7) | 2 (33.3) | |
| Hemoglobin (g/dL) | 13 (1.0) | 8.6 (1.8) | 10.3 (3.2) | <0.001 |
| MCV (fL) | 86.2 (5.7) | 92.5 (17.1) | 85.2 (6.8) | 0.62 |
| MCH (pg) | 28.7 (2.3) | 29.5 (5.6) | 29.6 (2.6) | 0.77 |
| MCHC (g/dl) | 33.2 (0.7) | 31.9 (1.3) | 34.2 (1.4) | <0.001 |
| RDW (%) | 12.8 (0.7) | 18.5 (3.9) | 18.6 (4.3) | <0.001 |
| Unadjusted | Adjusted * | |||
|---|---|---|---|---|
| Mean Difference (95%CI) | p-Value | Mean Difference (95%CI) | p-Value | |
| Group | ||||
| Normal | Ref. | Ref. | Ref. | Ref. |
| MDS | 2.2 (−0.18 to 4.58) | 0.08 | 1.5 (−6.07 to 9.17) | 0.68 |
| HS | −6.7 (−10.03 to −3.34) | <0.001 | −6.87 (−10.48 to −3.26) | 0.001 |
| ณNo. | 1 | 2 | 3 | 4 | 5 | Mean (SD) | 6 |
|---|---|---|---|---|---|---|---|
| Group | HS | HS | HS | HS | HS | - | SAO |
| Age | 26 | 47 | 27 | 32 | 40 | 34.4 (8.9) | 45 |
| Gender | Female | Female | Female | Male | Male | - | Female |
| Hb (g/dL) | 9.2 | 10.4 | 10.2 | 8.8 | 16.4 | 11 (3.1) | 7 |
| MCV (fL) | 81 | 87.6 | 73.3 | 90.4 | 89 | 84.3 (7.1) | 90 |
| MCH (pg) | 27.8 | 29.7 | 25.7 | 29.9 | 32.7 | 29.2 (2.6) | 32 |
| MCHC (g/dl) | 33.1 | 33.9 | 35.1 | 33 | 36.8 | 34.4 (1.6) | 33 |
| RDW (%) | 21.1 | 19.6 | 23.4 | 20.7 | 12.5 | 19.5 (4.1) | 14 |
| PLT | 250 | 237 | 211 | 286 | 328 | 262 (45.5) | 160.2 |
| (×103 cell/mm3) | |||||||
| WBC (cell/mm3) | 11,300 | 8320 | 9820 | 7010 | 6590 | 8608 (1.9) | 9600 |
| EMA | 22.23 | 16.35 | 18.48 | 19.88 | 13.09 | 18.01 (3.5) | 15.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uman, N.; Kobbuaklee, S.; Kansuwan, P.; Watanaboonyongcharoen, P.; Polprasert, C. Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry. Hematol. Rep. 2022, 14, 13-18. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010003
Uman N, Kobbuaklee S, Kansuwan P, Watanaboonyongcharoen P, Polprasert C. Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry. Hematology Reports. 2022; 14(1):13-18. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010003
Chicago/Turabian StyleUman, Navavee, Sirorat Kobbuaklee, Patsita Kansuwan, Phandee Watanaboonyongcharoen, and Chantana Polprasert. 2022. "Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry" Hematology Reports 14, no. 1: 13-18. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010003