
Respiratory Syncytial Virus Infections in Recipients of Bone Marrow Transplants: A Systematic Review and Meta-Analysis

 , and
, and 
Abstract
:1. Introduction
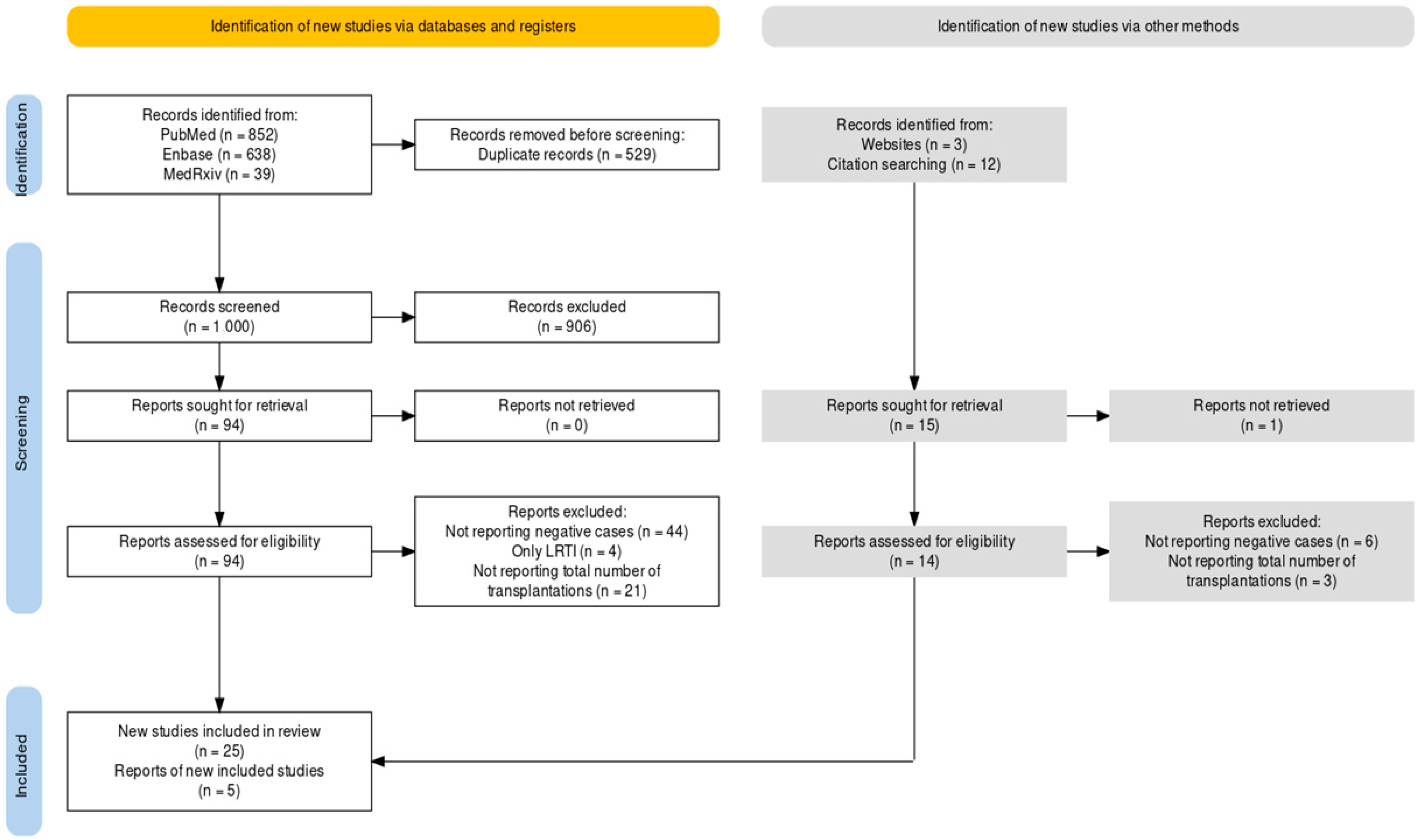
2. Materials and Methods
2.1. Research Concept
2.2. Research Strategy
- (a)
- PubMed (through Medical Subject Heading [MeSH] terms): (“RSV” OR “respiratory syncytial virus, human [Mesh]” OR “bronchiolitis [Mesh]”) AND (“bone marrow transplantation [Mesh]” OR “hematopoietic stem cell transplantation [Mesh]” OR “mesenchymal stem cell transplantation [Mesh]”).
- (b)
- EMBASE: (“bone marrow transplantation”/exp OR “bone marrow transplantation” OR “hematopoietic stem cell transplantation”) AND (“human respiratory syncytial virus” OR “respiratory syncytial virus infection” OR “respiratory syncytial virus pneumonia”).
- (c)
- medRxiv: (“RSV” OR “respiratory syncytial virus, human” OR “bronchiolitis”) AND (“bone marrow transplantation” OR “hematopoietic stem cell transplantation” OR “mesenchymal stem cell transplantation”).
2.3. Screening
- (1)
- Full text not available through online repositories or through inter-library loan;
- (2)
- Reports lacking appropriate or only vaguely defined geographical settings and corresponding timeframes;
- (3)
- Diagnosis for RSV infection provided by means of diagnostic tests other than Real Time quantitative Polymerase Chain Reaction (RT-qPCR) or by means of clinical features of the patient(s);
- (4)
- Reports lacking the total number of RSV infections and only providing the amount of either URTI or LRTI;
- (5)
- Studies not including the total number (i.e., the denominator) of BMT cases from the parent institution(s) for that timeframe.
2.4. Summary of Retrieved Data
- (a)
- Setting of the study: country, region, year (timeframe);
- (b)
- Amount of BMT included in the estimates (autologous vs. allogenic);
- (c)
- Number of cases with patients aged <18 y.o. at the time of the study (i.e., children/adolescents) vs. cases ≥ 18 y.o. (adults);
- (d)
- Characteristics of RSV cases: total cases, number of LRTI, number of URTI, and number of RSV-related deaths;
- (e)
- Where available, other respiratory tract viral infections (i.e., influenza, HAdV, hMPV, and SARS-CoV-2) and total number of reported cases;
- (f)
- Total number of cases treated with palivizumab (if available).
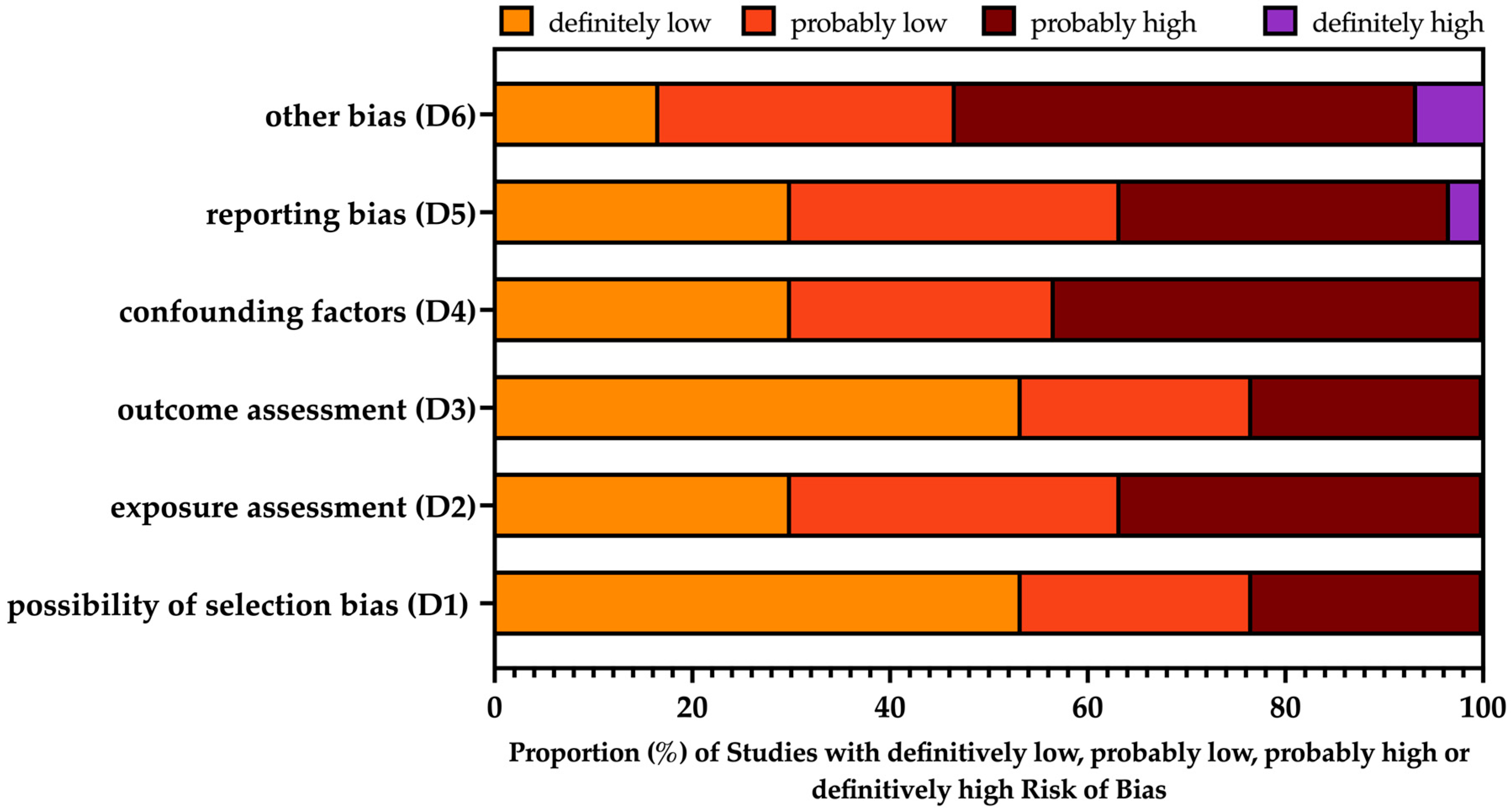
2.5. Risk of Bias Analysis
2.6. Data Analysis
3. Results
3.1. Descriptive Analysis
3.2. Risk of Bias
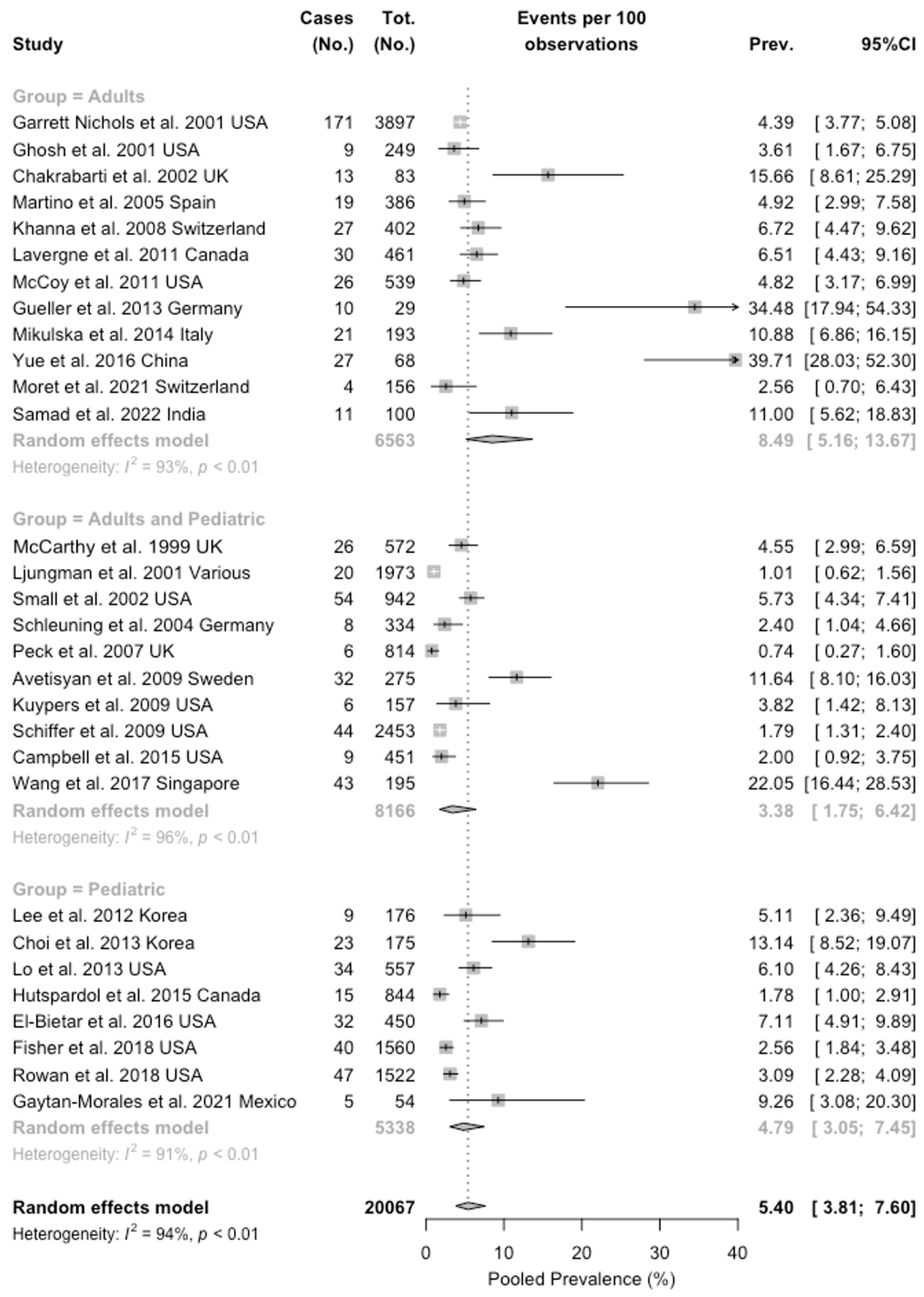
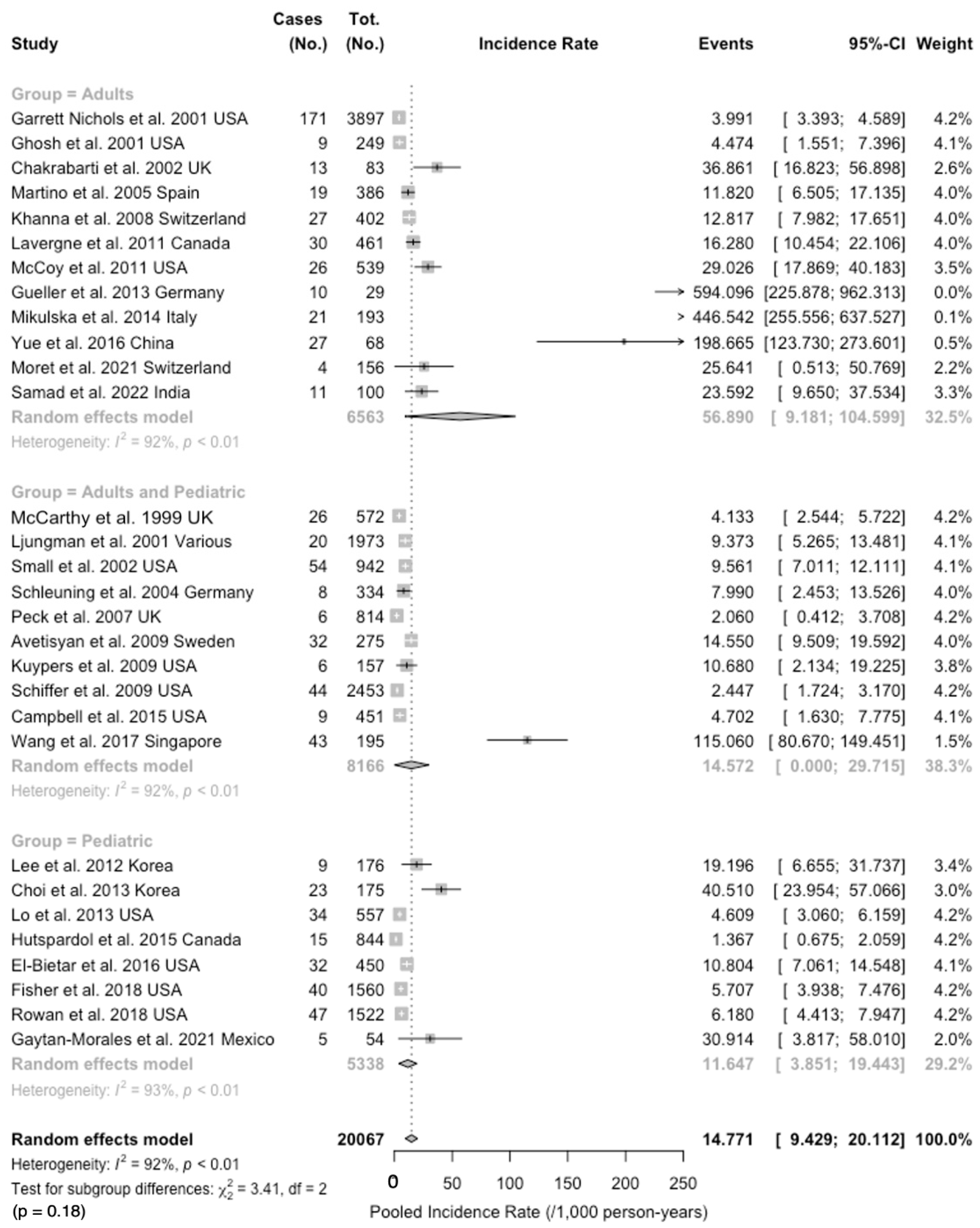
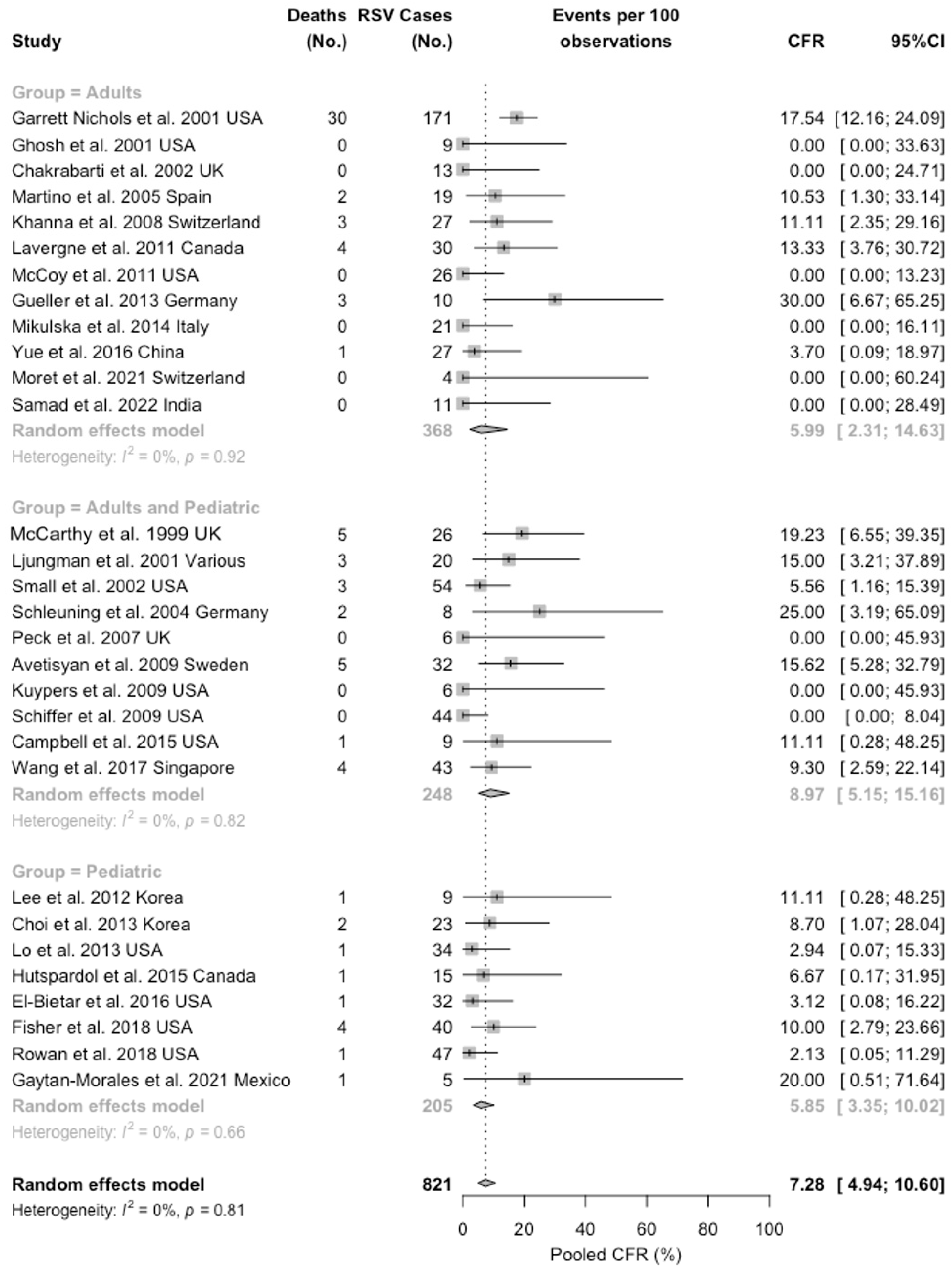
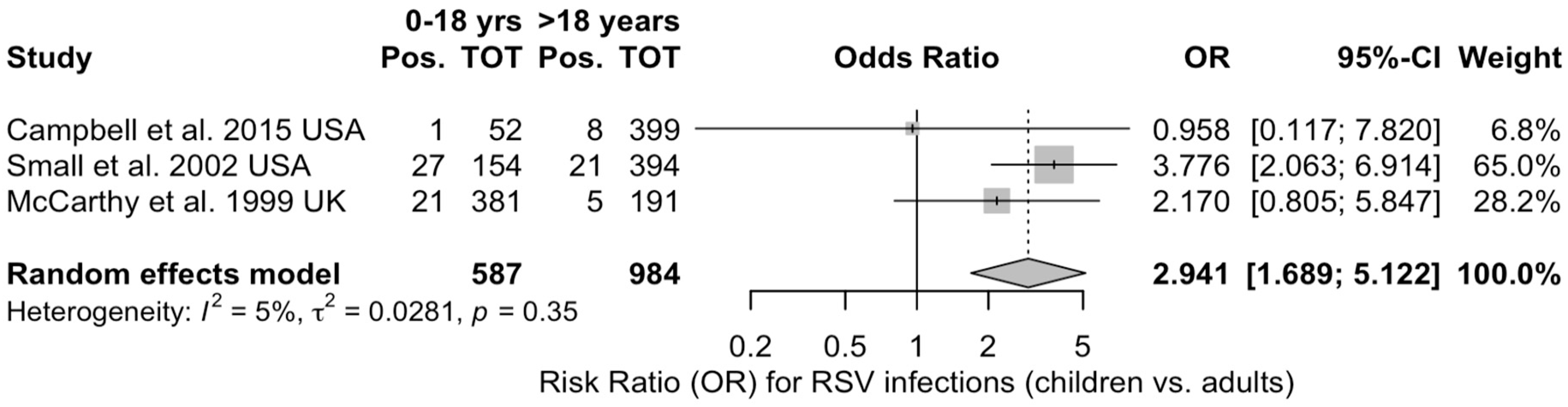
3.3. Meta-Analysis
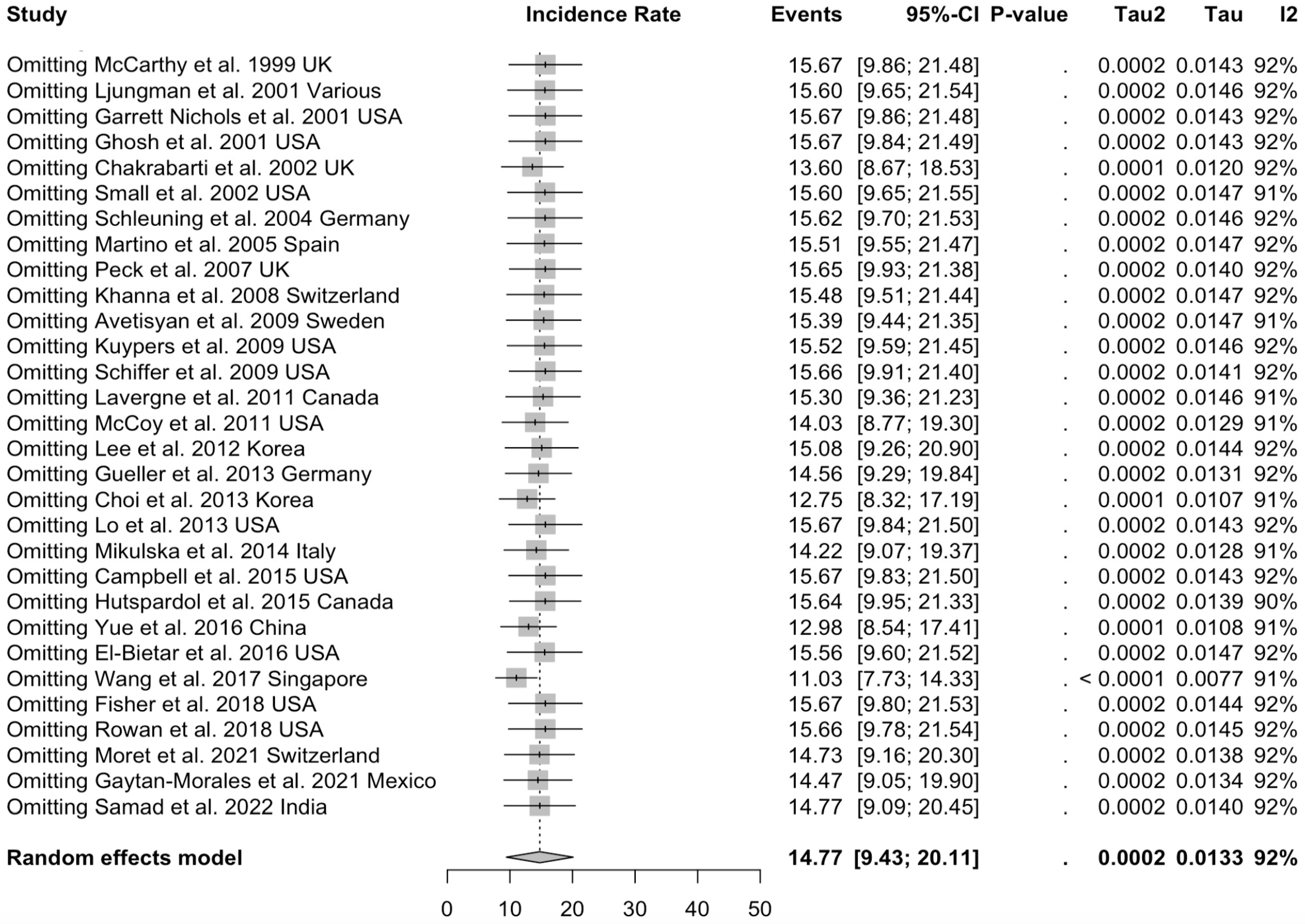
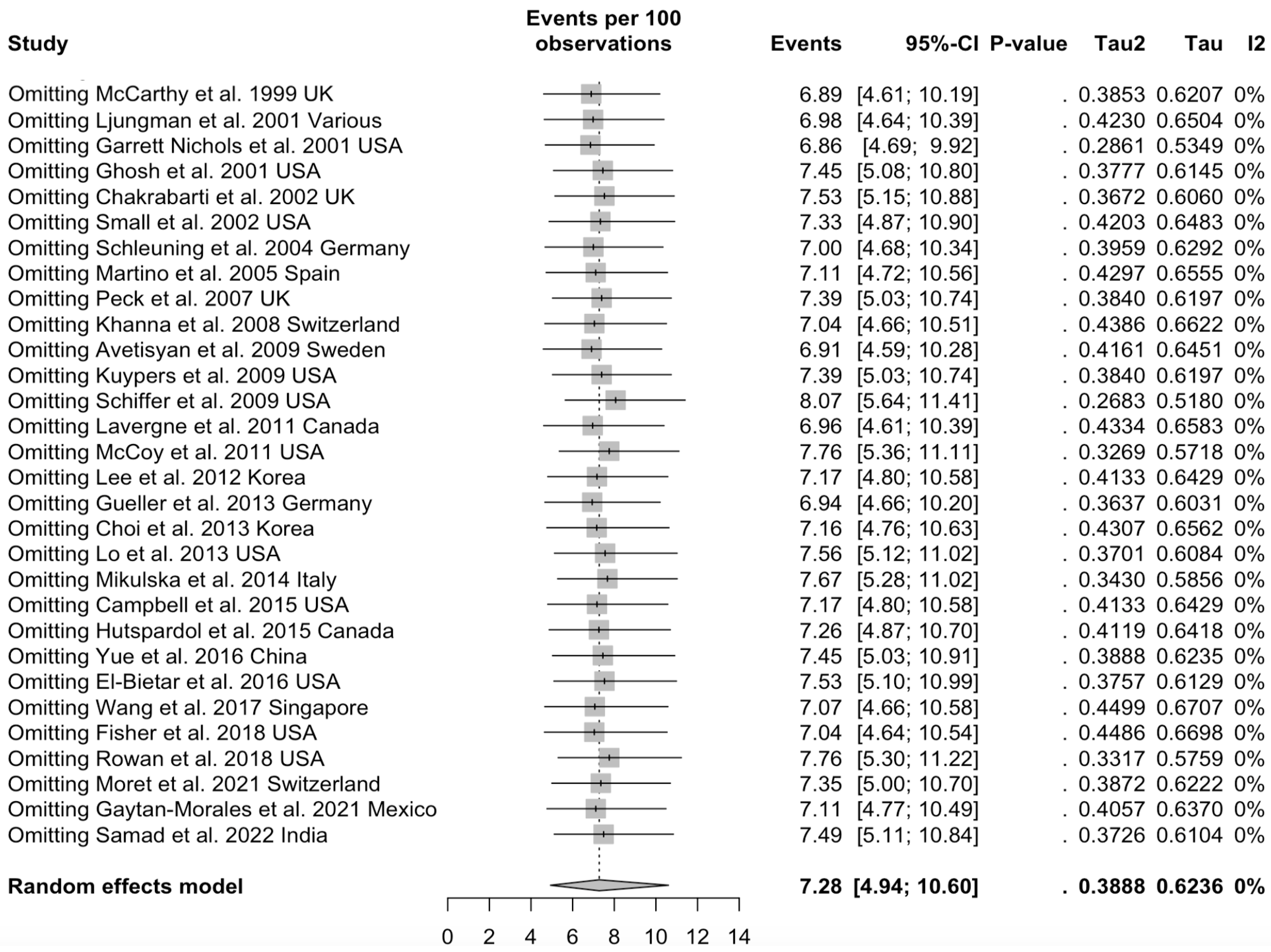
3.4. Sensitivity Analysis
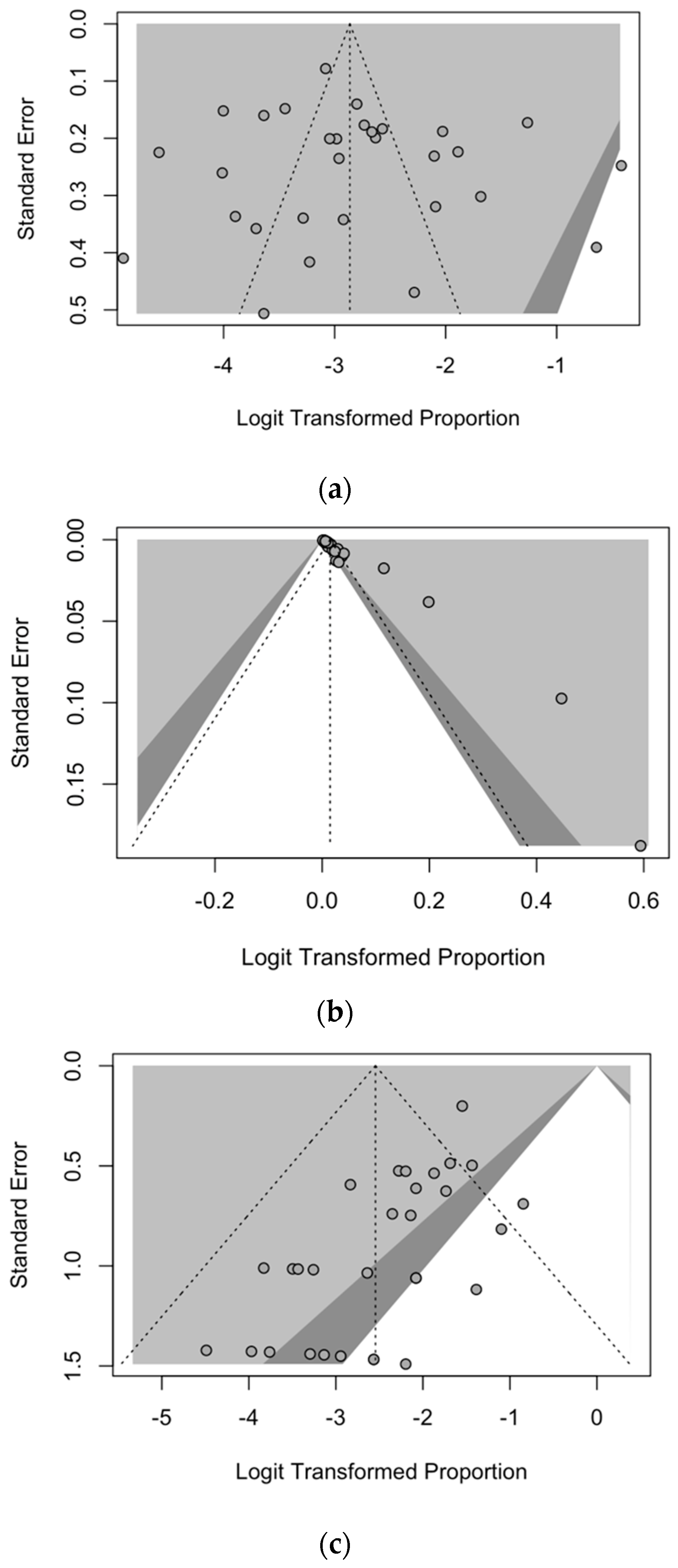
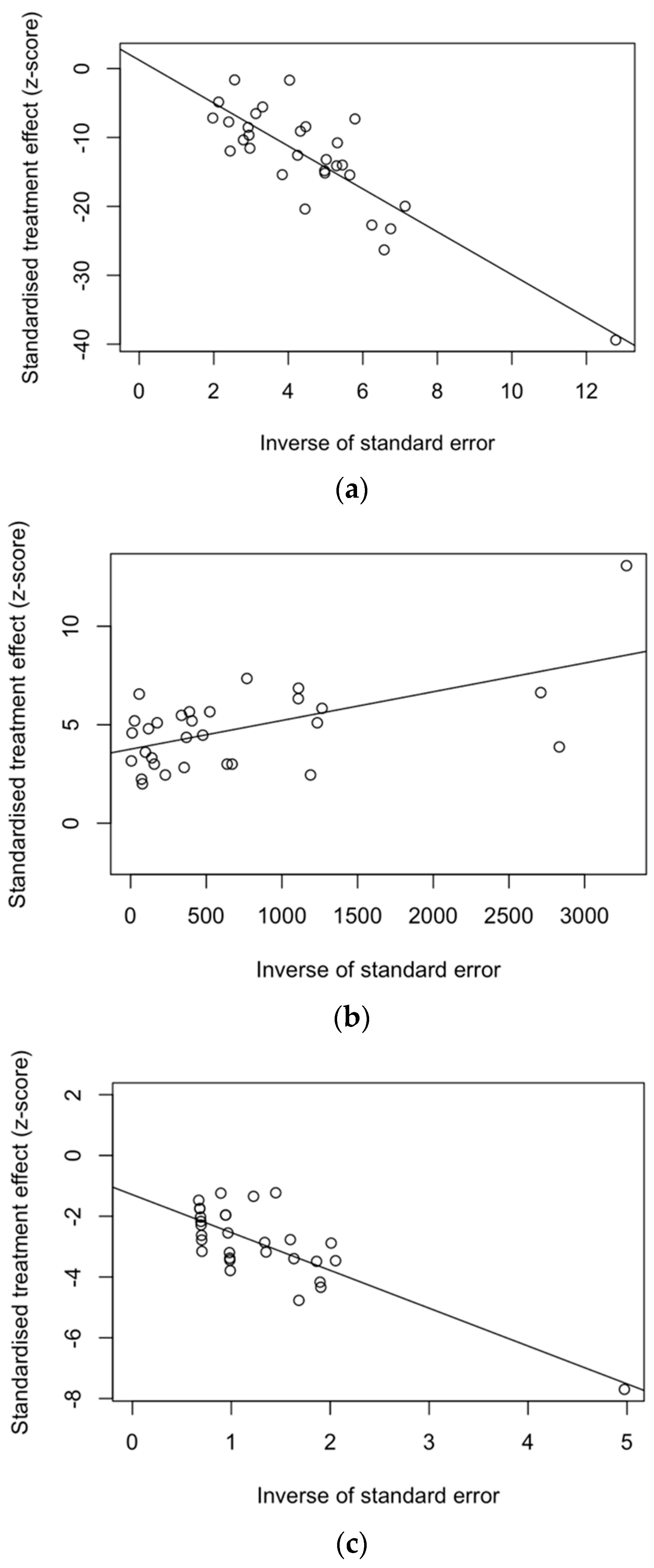
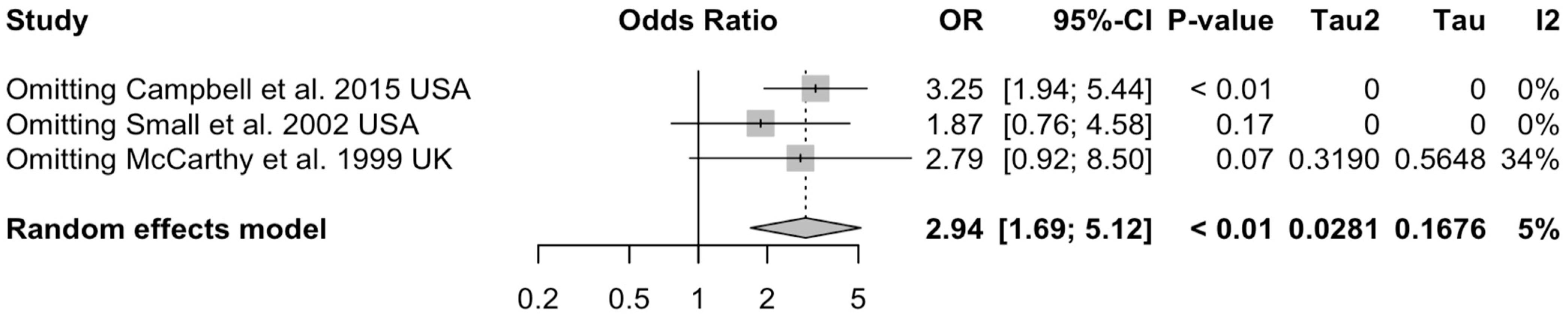
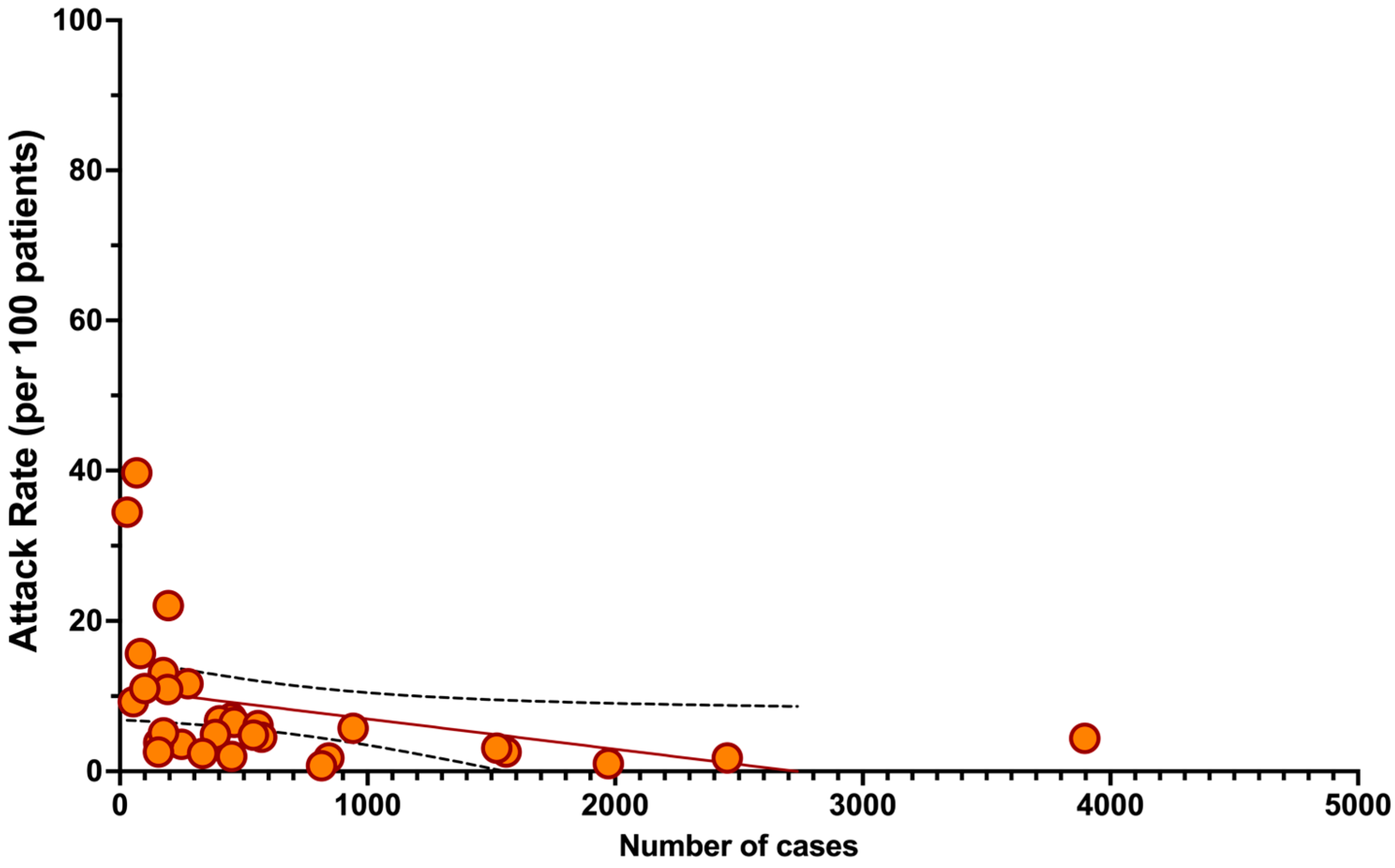
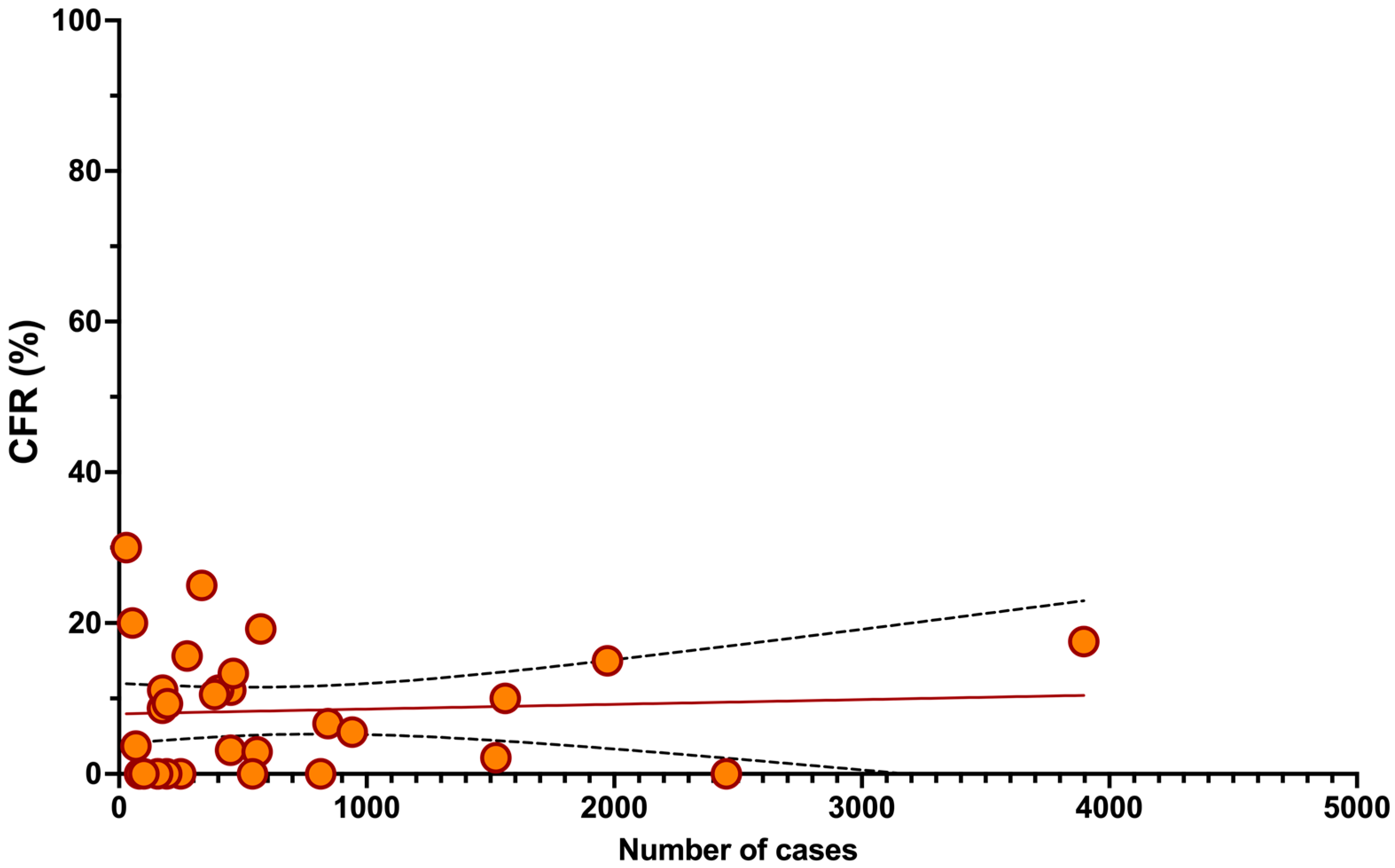
3.5. Analysis of Publication Bias and Small Study Bias
4. Discussion
4.1. Summary of the Main Findings
4.2. Interpretation of Key Results
4.3. Generalizability
4.4. Limits and Implications for Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

 : definitively high; : probably high;
: definitively high; : probably high;  : probably low; : definitively low.
: definitively high; : probably high; : probably low; : definitively low.
: probably low; : definitively low.
: definitively high; : probably high; : probably low; : definitively low.| Study | RISK OF BIAS | |||||
|---|---|---|---|---|---|---|
| D1 | D2 | D3 | D4 | D5 | D6 | |
| Avetysian et al., 2009 [80] | | | | | | |
| Campbell et al., 2015 [81] | | | | | | |
| Chakrabarti et al., 2002 [51] | | | | | | |
| Choi et al., 2013 [82] | | | | | | |
| El-Bietar et al., 2016 [61] | | | | | | |
| Fisher et al., 2018 [83] | | | | | | |
| Garrett Nichols et al., 2001 [84] | | | | | | |
| Gaytan Morales et al., 2021 [85] | | | | | | |
| Ghosh et al., 2001 [86] | | | | | | |
| Gueller et al., 2013 [68] | | | | | | |
| Hutspardol et al., 2015 [87] | | | | | | |
| Khanna et al., 2008 [88] | | | | | | |
| Kuypers et al., 2009 [89] | | | | | | |
| Lavergne et al., 2011 [46] | | | | | | |
| Lee et al., 2012 [90] | | | | | | |
| Ljungman et al., 2001 [91] | | | | | | |
| Lo et al., 2013 [92] | | | | | | |
| Martino et al., 2005 [93] | | | | | | |
| McCarthy et al., 1999 [94] | | | | | | |
| McCoy et al., 2011 [104] | | | | | | |
| Mikulska et al., 2014 [95] | | | | | | |
| Moret et al., 2021 [96] | | | | | | |
| Peck et al., 2007 [97] | | | | | | |
| Rowan et al., 2018 [98] | | | | | | |
| Samad et al., 2022 [99] | | | | | | |
| Schiffer et al., 2009 [100] | | | | | | |
| Schleuning et al., 2004 [70] | | | | | | |
| Small et al., 2002 [101] | | | | | | |
| Wang et al., 2017 [102] | | | | | | |
| Yue et al., 2016 [103] | | | | | | |
| Study | Limits of the Study |
|---|---|
| Avetysian et al., 2009 [80] | report lacking data on non-RSV cases unclear reporting of demographic data |
| Campbell et al., 2015 [81] | did not report palivizumab delivery unclear reporting of demographic data by groups |
| Chakrabarti et al., 2002 [51] | unclear selection strategy (all participants from this single institution?) |
| Choi et al., 2013 [82] | did not report palivizumab delivery unclear reporting of demographic data by groups |
| El-Bietar et al., 2016 [61] | report lacking data on non-RSV cases unclear reporting of demographic data |
| Fisher et al., 2018 [83] | high-quality report |
| Garrett Nichols et al., 2001 [84] | report lacking data on non-RSV cases unclear reporting of demographic data unclear and confusing report about the eventual outcome |
| Gaytan Morales et al., 2021 [85] | unclear reporting of demographic data |
| Ghosh et al., 2001 [86] | only female patients unclear reporting of clinical and demographic data unclear and confusing report about the eventual outcome |
| Gueller et al., 2013 [68] | very small sample size (single outbreak) did not report palivizumab delivery unclear reporting of demographic data by groups |
| Hutspardol et al., 2015 [87] | high-quality report |
| Khanna et al., 2008 [88] | report lacking data on non-RSV cases other than influenza and para-influenza unclear reporting of demographic data |
| Kuypers et al., 2009 [89] | unclear reporting of clinical and demographic data |
| Lavergne et al., 2011 [46] | report lacking data on non-RSV cases unclear reporting of demographic data |
| Lee et al., 2012 [90] | did not report palivizumab delivery unclear reporting of demographic data by groups did not report the share of upper vs. lower respiratory tract |
| Ljungman et al., 2001 [91] | unclear reporting of clinical and demographic data unclear and confusing report about the eventual outcome |
| Lo et al., 2013 [92] | unclear reporting of demographic data by groups |
| Martino et al., 2005 [93] | high-quality report |
| McCarthy et al., 1999 [94] | high-quality report |
| McCoy et al., 2011 [104] | report lacking data on non-RSV cases unclear reporting of demographic data |
| Mikulska et al., 2014 [95] | outpatients doubtful reporting of main clinical features and demographic data |
| Moret et al., 2021 [96] | unclear reporting of demographic data |
| Peck et al., 2007 [97] | unclear reporting of clinical and demographic data |
| Rowan et al., 2018 [98] | report lacking data on non-RSV cases |
| Samad et al., 2022 [99] | unclear definition of the sample size unclear reporting of autologous vs. allogenic transplants |
| Schiffer et al., 2009 [100] | report lacking data on non-RSV cases other than influenza and para-influenza unclear reporting of demographic data |
| Schleuning et al., 2004 [70] | report lacking data on non-RSV cases other than influenza and para-influenza unclear reporting of demographic data |
| Small et al., 2002 [101] | report lacking data on non-RSV cases other than influenza and para-influenza unclear reporting of demographic data, particularly on autologous transplant |
| Wang et al., 2017 [102] | did not report palivizumab delivery |
| Yue et al., 2016 [103] | did not report palivizumab delivery unclear reporting of demographic data |








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



References
- Langedijk, A.C.; Harding, E.R.; Konya, B.; Vrancken, B.; Lebbink, R.J.; Evers, A.; Willemsen, J.; Lemey, P.; Bont, L.J. A Systematic Review on Global RSV Genetic Data: Identification of Knowledge Gaps. Rev. Med. Virol. 2021, 32, e2284. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.H.; Ison, M.G. Respiratory Syncytial Virus Infection in Adults. BMJ 2019, 366, l5021. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef]
- Nair, H.; Theodoratou, E.; Rudan, I.; Nokes, D.J.; Ngama HND, M.; Munywoki, P.K.; Dherani, M.; Nair, H.; James Nokes, D.; Gessner, B.D.; et al. Global Burden of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children: A Systematic Review and Meta-Analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Liu, Q.; Zhou, Y.; Ran, Y.; Liu, Z.; Hou, W.; Pei, S.; Lai, S. Spatiotemporal Variations of “Triple-Demic” Outbreaks of Respiratory Infections in the United States in the Post-COVID-19 Era. BMC Public Health 2023, 23, 2452. [Google Scholar] [CrossRef]
- Patel, T.A.; Jain, B.; Raifman, J. Revamping Public Health Systems: Lessons Learned From the Tripledemic. Am. J. Prev. Med. 2023, 66, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2021, 222, S577–S583. [Google Scholar] [CrossRef] [PubMed]
- Regassa, B.T.; Gebrewold, L.A.; Mekuria, W.T.; Kassa, N.A. Molecular Epidemiology of Respiratory Syncytial Virus in Children with Acute Respiratory Illnesses in Africa: A Systematic Review and Meta-Analysis. J. Glob. Health 2023, 13, 04001. [Google Scholar] [CrossRef]
- Youssef, Y.; Chmaisse, A.; Boutros, C.; Chamseddine, S.; Fayad, D.; Zaraket, H.; Dbaibo, G. The Burden of Respiratory Syncytial Virus (RSV) Infection in the Middle East and North Africa (MENA) Region across Age Groups: A Systematic Review. Vaccine 2021, 39, 3803–3813. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Children Younger than 5 Years in 2019: A Systematic Analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Du, Y.; Yan, R.; Wu, X.; Zhang, X.; Chen, C.; Jiang, D.; Yang, M.; Cao, K.; Chen, M.; You, Y.; et al. Global Burden and Trends of Respiratory Syncytial Virus Infection across Different Age Groups from 1990 to 2019: A Systematic Analysis of the Global Burden of Disease 2019 Study. Int. J. Infect. Dis. 2023, 135, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Van-tam, J.S.; O’leary, M.; Martin, E.T.; Heijnen, E.; Callendret, B.; Fleischhackl, R.; Comeaux, C.; Tran, T.M.P.; Weber, K. Burden of Respiratory Syncytial Virus Infection in Older and High-Risk Adults: A Systematic Review and Meta-Analysis of the Evidence from Developed Countries. Eur. Respir. Rev. 2022, 31, 220105. [Google Scholar] [PubMed]
- Weigl, J.A.I.; Puppe, W.; Schmitt, H.J. Incidence of Respiratory Syncytial Virus-Positive Hospitalizations in Germany. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Scarselli, E.; Lelii, M.; Scala, A.; Vitelli, A.; Capone, S.; Fornili, M.; Biganzoli, E.; Orenti, A.; Nicosia, A.; et al. Antibody Response to Respiratory Syncytial Virus Infection in Children <18 Months Old. Hum. Vaccin. Immunother. 2016, 12, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Tabatabai, J.; Ihling, C.M.; Rehbein, R.M.; Schnee, S.V.; Hoos, J.; Pfeil, J.; Grulich-Henn, J.; Schnitzler, P. Molecular Epidemiology of Respiratory Syncytial Virus in Hospitalised Children in Heidelberg, Southern Germany, 2014–2017. Infect. Genet. Evol. 2022, 98, 105209. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Poehling, K.A.; Szilagyi, P.G.; Griffin, M.R.; Williams, J.V.; et al. Respiratory Syncytial Virus-Associated Hospitalizations among Children Less Than 24 Months of Age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef]
- Abbas, S.; Raybould, J.E.; Sastry, S.; de la Cruz, O. Respiratory Viruses in Transplant Recipients: More than Just a Cold. Clinical Syndromes and Infection Prevention Principles. Int. J. Infect. Dis. 2017, 62, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Bozzola, E.; Ciarlitto, C.; Guolo, S.; Brusco, C.; Cerone, G.; Antilici, L.; Schettini, L.; Piscitelli, A.L.; Chiara Vittucci, A.; Cutrera, R.; et al. Respiratory Syncytial Virus Bronchiolitis in Infancy: The Acute Hospitalization Cost. Front. Pediatr. 2021, 8, 594898. [Google Scholar] [CrossRef]
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory Syncytial Virus-Associated Hospitalizations among Young Children: 2015–2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef]
- Leader, S.; Kohlhase, K. Respiratory Syncytial Virus-Coded Pediatric Hospitalizations, 1997 to 1999. Pediatr. Infect. Dis. J. 2002, 21, 629–661. [Google Scholar] [CrossRef] [PubMed]
- Leader, S.; Kohlhase, K.; Pearlman, M.H.; Williams, J.V.; Engle, W.A. Recent Trends in Severe Respiratory Syncytial Virus (RSV) among US Infants, 1997 to 2000. J. Pediatr. 2003, 143, S127–S132. [Google Scholar] [CrossRef] [PubMed]
- Hammitt, L.L.; Dagan, R.; Yuan, Y.; Baca Cots, M.; Bosheva, M.; Madhi, S.A.; Muller, W.J.; Zar, H.J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N. Engl. J. Med. 2022, 386, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Aliprantis, A.O.; Shaw, C.A.; Griffin, P.; Farinola, N.; Railkar, R.A.; Cao, X.; Liu, W.; Sachs, J.R.; Swenson, C.J.; Lee, H.; et al. A Phase 1, Randomized, Placebo-Controlled Study to Evaluate the Safety and Immunogenicity of an MRNA-Based RSV Prefusion F Protein Vaccine in Healthy Younger and Older Adults. Hum. Vaccin. Immunother. 2021, 17, 1248–1261. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Pérez Marc, G.; Zareba, A.M.; Falsey, A.R.; Jiang, Q.; Patton, M.; Polack, F.P.; Llapur, C.; Doreski, P.A.; Ilangovan, K.; et al. Efficacy and Safety of a Bivalent RSV Prefusion F Vaccine in Older Adults. N. Engl. J. Med. 2023, 388, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Chatzis, O.; Darbre, S.; Pasquier, J.; Meylan, P.; Manuel, O.; Aubert, J.D.; Beck-Popovic, M.; Masouridi-Levrat, S.; Ansari, M.; Kaiser, L.; et al. Burden of Severe RSV Disease among Immunocompromised Children and Adults: A 10 Year Retrospective Study. BMC Infect. Dis. 2018, 18, 111. [Google Scholar] [CrossRef] [PubMed]
- Boattini, M.; Almeida, A.; Christaki, E.; Marques, T.M.; Tosatto, V.; Bianco, G.; Iannaccone, M.; Tsiolakkis, G.; Karagiannis, C.; Maikanti, P.; et al. Severity of RSV Infection in Southern European Elderly Patients during Two Consecutive Winter Seasons (2017–2018). J. Med. Virol. 2021, 93, 5152–5157. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Koval, C.; DeVincenzo, J.P.; Walsh, E.E. Compassionate Use Experience with High-Titer Respiratory Syncytical Virus (RSV) Immunoglobulin in RSV-Infected Immunocompromised Persons. Transpl. Infect. Dis. 2017, 19, e12657. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory Syncytial Virus Infection in Elderly and High-Risk Adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef]
- Ali, A.; Lopardo, G.; Scarpellini, B.; Stein, R.T.; Ribeiro, D. Systematic Review on Respiratory Syncytial Virus Epidemiology in Adults and the Elderly in Latin America. Int. J. Infect. Dis. 2020, 90, 170–180. [Google Scholar] [CrossRef]
- Nowalk, M.P.; D’Agostino, H.; Dauer, K.; Stiegler, M.; Zimmerman, R.K.; Balasubramani, G.K. Estimating the Burden of Adult Hospitalized RSV Infection Including Special Populations. Vaccine 2022, 40, 4121–4127. [Google Scholar] [CrossRef] [PubMed]
- Narejos Pérez, S.; Ramón Torrell, J.M.; Põder, A.; Leroux-Roels, I.; Pérez-Breva, L.; Steenackers, K.; Vandermeulen, C.; Meisalu, S.; McNally, D.; Bowen, J.S.; et al. Respiratory Syncytial Virus Disease Burden in Community-Dwelling and Long-Term Care Facility Older Adults in Europe and the United States: A Prospective Study. Open Forum Infect. Dis. 2023, 10, ofad111. [Google Scholar] [CrossRef] [PubMed]
- Savic, M.; Penders, Y.; Shi, T.; Branche, A.; Pirçon, J.Y. Respiratory Syncytial Virus Disease Burden in Adults Aged 60 Years and Older in High-Income Countries: A Systematic Literature Review and Meta-Analysis. Influenza Other Respir. Viruses 2022, 17, e13031. [Google Scholar] [CrossRef] [PubMed]
- Chemaly, R.F.; Shah, D.P.; Boeckh, M.J. Management of Respiratory Viral Infections in Hematopoietic Cell Transplant Recipients and Patients with Hematologic Malignancies. Clin. Infect. Dis. 2014, 59, S344–S351. [Google Scholar] [CrossRef] [PubMed]
- El Saleeby, C.M.; Somes, G.W.; DeVincenzo, J.P.; Gaur, A.H. Risk Factors for Severe Respiratory Syncytial Virus Disease in Children with Cancer: The Importance of Lymphopenia and Young Age. Pediatrics 2008, 121, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.P.; Tapia, L.I.; Catalán, P.; De la Maza, V.; Mejías, A. Intravenous Palivizumab in Respiratory Syncytial Virus Infection after Hematopoietic Stem Cell Transplant in Children. Pediatr. Blood Cancer 2017, 64, e26667. [Google Scholar] [CrossRef] [PubMed]
- Permpalung, N.; Mahoney, M.V.; McCoy, C.; Atsawarungruangkit, A.; Gold, H.S.; Levine, J.D.; Wong, M.T.; LaSalvia, M.T.; Alonso, C.D. Clinical Characteristics and Treatment Outcomes among Respiratory Syncytial Virus (RSV)-Infected Hematologic Malignancy and Hematopoietic Stem Cell Transplant Recipients Receiving Palivizumab. Leuk. Lymphoma 2019, 60, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Cutland, C.L.; Downs, S.; Jones, S.; Van Niekerk, N.; Simoes, E.A.F.; Nunes, M.C. Burden of Respiratory Syncytial Virus Infection in South African Human Immunodeficiency Virus (HIV)-Infected and HIV-Uninfected Pregnant and Postpartum Women: A Longitudinal Cohort Study. Clin. Infect. Dis. 2018, 66, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yuan, L.; Zhang, Y.; Zhang, X.; Zheng, M.; Kyaw, M.H. Burden of Respiratory Syncytial Virus Infections in China: Systematic Review and Meta-Analysis. J. Glob. Health 2015, 5, 20417. [Google Scholar] [CrossRef]
- Palmer, L.; Hall, C.B.; Katkin, J.P.; Shi, N.; Masaquel, A.S.; McLaurin, K.K.; Mahadevia, P.J. Healthcare Costs within a Year of Respiratory Syncytial Virus among Medicaid Infants. Pediatr. Pulmonol. 2010, 45, 772–781. [Google Scholar] [CrossRef]
- McLaurin, K.K.; Farr, A.M.; Wade, S.W.; Diakun, D.R.; Stewart, D.L. Respiratory Syncytial Virus Hospitalization Outcomes and Costs of Full-Term and Preterm Infants. J. Perinatol. 2016, 36, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Mao, Z.; Li, X.; Dacosta-Urbieta, A.; Billard, M.N.; Wildenbeest, J.; Korsten, K.; Martinón-Torres, F.; Heikkinen, T.; Cunningham, S.; Snape, M.D.; et al. Economic Burden and Health-Related Quality-of-Life among Infants with Respiratory Syncytial Virus Infection: A Multi-Country Prospective Cohort Study in Europe. Vaccine 2023, 41, 2707–2715. [Google Scholar] [CrossRef] [PubMed]
- Neemann, K.; Freifeld, A. Respiratory Syncytial Virus in Hematopoietic Stem Cell Transplantation and Solid-Organ Transplantation. Curr. Infect. Dis. Rep. 2015, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, D.D.H.; Arcega, V.; Rao, M. Review of Respiratory Syncytial Virus Infection among Older Adults and Transplant Recipients. Ther. Adv. Infect. Dis. 2022, 9, 20499361221091413. [Google Scholar] [CrossRef] [PubMed]
- Manothummetha, K.; Mongkolkaew, T.; Tovichayathamrong, P.; Boonyawairote, R.; Meejun, T.; Srisurapanont, K.; Phongkhun, K.; Sanguankeo, A.; Torvorapanit, P.; Moonla, C.; et al. Ribavirin Treatment for Respiratory Syncytial Virus Infection in Patients with Haematologic Malignancy and Haematopoietic Stem Cell Transplant Recipients: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2023, 29, 1272–1279. [Google Scholar] [CrossRef] [PubMed]
- Lavergne, V.; Ghannoum, M.; Weiss, K.; Roy, J.; Béliveau, C. Successful Prevention of Respiratory Syncytial Virus Nosocomial Transmission Following an Enhanced Seasonal Infection Control Program. Bone Marrow Transplant. 2011, 46, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Anderson, N.W.; Binnicker, M.J.; Harris, D.M.; Chirila, R.M.; Brumble, L.; Mandrekar, J.; Hata, D.J. Morbidity and Mortality among Patients with Respiratory Syncytial Virus Infection: A 2-Year Retrospective Review. Diagn. Microbiol. Infect. Dis. 2016, 85, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Vakil, E.; Sheshadri, A.; Faiz, S.A.; Shah, D.P.; Zhu, Y.; Li, L.; Kmeid, J.; Azzi, J.; Balagani, A.; Bashoura, L.; et al. Risk Factors for Mortality after Respiratory Syncytial Virus Lower Respiratory Tract Infection in Adults with Hematologic Malignancies. Transpl. Infect. Dis. 2018, 20, e12994. [Google Scholar] [CrossRef] [PubMed]
- Sheshadri, A.; Chemaly, R.F.; Alousi, A.M.; Shah, P.K.; Rondon, G.; Bashoura, L.; Kmeid, J.; Azzi, J.; Blanco, D.W.; Kaous, M.; et al. Pulmonary Impairment after Respiratory Viral Infections Is Associated with High Mortality in Allogeneic Hematopoietic Cell Transplant Recipients. Biol. Blood Marrow Transplant. 2019, 25, 800–809. [Google Scholar] [CrossRef]
- Renaud, C.; Xie, H.; Seo, S.; Kuypers, J.; Cent, A.; Corey, L.; Leisenring, W.; Boeckh, M.; Englund, J.A. Mortality Rates of Human Metapneumovirus and Respiratory Syncytial Virus Lower Respiratory Tract Infections in Hematopoietic Cell Transplantation Recipients. Biol. Blood Marrow Transplant. 2013, 19, 1220–1226. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Avivi, I.; Mackinnon, S.; Ward, K.; Kottaridis, P.D.; Osman, H.; Waldmann, H.; Hale, G.; Fegan, C.D.; Yong, K.; et al. Respiratory Virus Infections in Transplant Recipients after Reduced-Intensity Conditioning with Campath-1H: High Incidence but Low Mortality. Br. J. Haematol. 2002, 119, 1125–1132. [Google Scholar] [CrossRef]
- Melgar, M.; Britton, A.; Roper, L.E.; Talbot, K.H.; Long, S.S.; Kotton, C.N.; Havers, F.P. Use of Respiratory Syncytial Virus Vaccines in Older Adults: Recommendations of the Advisory Committee on Immunization Practices—United States, 2023. Morb. Mortal. Wkly. Rep. 2023, 72, 793–801. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer Respiratory Syncytial Virus Vaccine During Pregnancy for the Prevention of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Disease in Infants: Recommendations of the Advisory Committee on Immunization Practices-United States, 2023. Morb. Mortal. Wkly. Rep. 2023, 72, 1115–1122. [Google Scholar]
- Kampmann, B.; Madhi, S.A.; Munjal, I.; Simões, E.A.F.; Pahud, B.A.; Llapur, C.; Baker, J.; Pérez Marc, G.; Radley, D.; Shittu, E.; et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N. Engl. J. Med. 2023, 388, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Papi, A.; Ison, M.G.; Langley, J.M.; Lee, D.-G.; Leroux-Roels, I.; Martinon-Torres, F.; Schwarz, T.F.; van Zyl-Smit, R.N.; Campora, L.; Dezutter, N.; et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine in Older Adults. N. Engl. J. Med. 2023, 388, 595–608. [Google Scholar] [CrossRef]
- Andabaka, T.; Nickerson, J.W.; Rojas-Reyes, M.X.; Rueda, J.D.; Bacic Vrca, V.; Barsic, B. Monoclonal Antibody for Reducing the Risk of Respiratory Syncytial Virus Infection in Children. Cochrane Database Syst. Rev. 2013, 4, CD006602. [Google Scholar] [CrossRef]
- Griffin, M.P.; Yuan, Y.; Takas, T.; Domachowske, J.B.; Madhi, S.A.; Manzoni, P.; Simões, E.A.F.; Esser, M.T.; Khan, A.A.; Dubovsky, F.; et al. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. N. Engl. J. Med. 2020, 383, 415–425. [Google Scholar] [CrossRef]
- Domachowske, J.B.; Chang, Y.; Atanasova, V.; Cabañas, F.; Furuno, K.; Nguyen, K.A.; Banu, I.; Kubiak, R.J.; Leach, A.; Mankad, V.S.; et al. Safety of Re-Dosing Nirsevimab Prior to RSV Season 2 in Children with Heart or Lung Disease. J. Pediatr. Infect. Dis. Soc. 2023, 12, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Domachowske, J.; Madhi, S.A.; Simões, E.A.F.; Atanasova, V.; Cabañas, F.; Furuno, K.; Garcia-Garcia, M.L.; Grantina, I.; Nguyen, K.A.; Brooks, D.; et al. Safety of Nirsevimab for RSV in Infants with Heart or Lung Disease or Prematurity. N. Engl. J. Med. 2022, 386, 892–894. [Google Scholar] [CrossRef] [PubMed]
- Committee on Infectious Diseases and Bronchiolitis Guidelines Committee; Brady, M.T.; Byington, C.L.; Dele Davies, H.; Edwards, K.M.; Jackson, M.A.; Maldonado, Y.A.; Murray, D.L.; Orenstein, W.A.; Rathore, M.H.; et al. Updated Guidance for Palivizumab Prophylaxis among Infants and Young Children at Increased Risk of Hospitalization for Respiratory Syncytial Virus Infection. Pediatrics 2014, 134, e620–e638. [Google Scholar] [CrossRef]
- El-Bietar, J.; Nelson, A.; Wallace, G.; Dandoy, C.; Jodele, S.; Myers, K.C.; Teusink, A.; Lane, A.; Davies, S.M.; Danziger-Isakov, L. RSV Infection without Ribavirin Treatment in Pediatric Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2016, 51, 1382–1384. [Google Scholar] [CrossRef]
- Molinos-Quintana, A.; Pérez-De Soto, C.; Gómez-Rosa, M.; Pérez-Simón, J.A.; Pérez-Hurtado, J.M. Intravenous Ribavirin for Respiratory Syncytial Viral Infections in Pediatric Hematopoietic SCT Recipients. Bone Marrow Transplant. 2013, 48, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Marcelin, J.R.; Wilson, J.W.; Razonable, R.R. Oral Ribavirin Therapy for Respiratory Syncytial Virus Infections in Moderately to Severely Immunocompromised Patients. Transpl. Infect. Dis. 2014, 16, 242–250. [Google Scholar] [CrossRef]
- Chávez-Bueno, S.; Mejías, A.; Merryman, R.A.; Ahmad, N.; Jafri, H.S.; Ramilo, O. Intravenous Palivizumab and Ribavirin Combination for Respiratory Syncytial Virus Disease in High-Risk Pediatric Patients. Pediatr. Infect. Dis. J. 2007, 26, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Gorcea, C.M.; Tholouli, E.; Turner, A.; Saif, M.; Davies, E.; Battersby, E.; Dignan, F.L. Effective Use of Oral Ribavirin for Respiratory Syncytial Viral Infections in Allogeneic Haematopoietic Stem Cell Transplant Recipients. J. Hosp. Infect. 2017, 95, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Foolad, F.; Aitken, S.L.; Shigle, T.L.; Prayag, A.; Ghantoji, S.; Ariza-Heredia, E.; Chemaly, R.F. Oral versus Aerosolized Ribavirin for the Treatment of Respiratory Syncytial Virus Infections in Hematopoietic Cell Transplant Recipients. Clin. Infect. Dis. 2019, 68, 1641–1649. [Google Scholar] [CrossRef] [PubMed]
- Stamouli, M.; Tsonis, I.; Gkirkas, K.; Economopoulou, C.; Siafakas, N.; Pournaras, S.; Antoniadou, A.; Chondropoulos, S.; Karagiannidi, A.; Meletiadis, J.; et al. Oral Ribavirin Is a Highly Effective Treatment for Lower Respiratory Tract Infections Due to Respiratory Syncytial Virus or Parainfluenza after Allogeneic Stem Cell Transplantation. Bone Marrow Transplant. 2021, 56, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Gueller, S.; Duenzinger, U.; Wolf, T.; Ajib, S.; Mousset, S.; Berger, A.; Martin, H.; Serve, H.; Bug, G. Successful Systemic High-Dose Ribavirin Treatment of Respiratory Syncytial Virus-Induced Infections Occurring Pre-Engraftment in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Transpl. Infect. Dis. 2013, 15, 435–440. [Google Scholar] [CrossRef]
- Akhmedov, M.; Wais, V.; Sala, E.; Neagoie, A.; Nguyen, T.M.; Gantner, A.; von Harsdorf, S.; Kuchenbauer, F.; Schubert, A.; Michel, D.; et al. Respiratory Syncytial Virus and Human Metapneumovirus after Allogeneic Hematopoietic Stem Cell Transplantation: Impact of the Immunodeficiency Scoring Index, Viral Load, and Ribavirin Treatment on the Outcomes. Transpl. Infect. Dis. 2020, 22, e13276. [Google Scholar] [CrossRef]
- Schleuning, M.; Buxbaum-Conradi, H.; Jäger, G.; Kolb, H.J. Intravenous Ribavirin for Eradication of Respiratory Syncytial Virus (RSV) and Adenovirus Isolates from the Respiratory and/or Gastrointestinal Tract in Recipients of Allogeneic Hematopoietic Stem Cell Transplants. Hematol. J. 2004, 5, 135–144. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- NTP. OHAT Risk of Bias Rating Tool for Human and Animal Studies; NTP: Durham, NC, USA, 2015. [Google Scholar]
- National Toxicology Program. Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; March 4, 2019; NTP: Durham, NC, USA, 2019. [Google Scholar]
- Eick, S.M.; Goin, D.E.; Chartres, N.; Lam, J.; Woodruff, T.J. Assessing Risk of Bias in Human Environmental Epidemiology Studies Using Three Tools: Different Conclusions from Different Tools. Syst. Rev. 2020, 9, 249. [Google Scholar] [CrossRef]
- Von Hippel, P.T. The Heterogeneity Statistic I2 Can Be Biased in Small Meta-Analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Imrey, P.B. Limitations of Meta-Analyses of Studies with High Heterogeneity. JAMA Netw. Open 2020, 3, e1919325. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R a Language and Environment for Statistical Computing: Reference Index; R Foundation for Statistical Computing: Vienna, Austria, 2010; ISBN 3900051070. [Google Scholar]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R Package and Shiny App for Producing PRISMA 2020-Compliant Flow Diagrams, with Interactivity for Optimised Digital Transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef] [PubMed]
- Avetisyan, G.; Mattsson, J.; Sparrelid, E.; Ljungman, P. Respiratory Syncytial Virus Infection in Recipients of Allogeneic Stem-Cell Transplantation: A Retrospective Study of the Incidence, Clinical Features, and Outcome. Transplantation 2009, 88, 1222–1226. [Google Scholar] [CrossRef]
- Campbell, A.P.; Guthrie, K.A.; Englund, J.A.; Farney, R.M.; Minerich, E.L.; Kuypers, J.; Corey, L.; Boeckh, M. Clinical Outcomes Associated with Respiratory Virus Detection before Allogeneic Hematopoietic Stem Cell Transplant. Clin. Infect. Dis. 2015, 61, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Choi, E.H.; Kang, H.J.; Park, K.D.; Park, S.S.; Shin, H.Y.; Lee, H.J.; Ahn, H.S. Respiratory Viral Infections after Hematopoietic Stem Cell Transplantation in Children. J. Korean Med. Sci. 2013, 28, 36–41. [Google Scholar] [CrossRef]
- Fisher, B.T.; Danziger-Isakov, L.; Sweet, L.R.; Munoz, F.M.; Maron, G.; Tuomanen, E.; Murray, A.; Englund, J.A.; Dulek, D.; Halasa, N.; et al. A Multicenter Consortium to Define the Epidemiology and Outcomes of Inpatient Respiratory Viral Infections in Pediatric Hematopoietic Stem Cell Transplant Recipients. J. Pediatr. Infect. Dis. Soc. 2018, 7, 275–282. [Google Scholar] [CrossRef]
- Garrett Nichols, W.; Gooley, T.; Boeckh, M. Community-Acquired Respiratory Syncytial Virus and Parainfluenza Virus Infections after Hematopoietic Stem Cell Transplantation: The Fred Hutchinson Cancer Research Center Experience. Biol. Blood Marrow Transplanat. 2001, 7, 11S–15S. [Google Scholar] [CrossRef] [PubMed]
- Gaytán-Morales, J.F.; Castorena-Villa, I.; Cortés-Flores, D.C.; Avilés-Robles, M.J.; Sánchez-Huerta, J.L.; Ortiz-Navarrete, V.; Olvera-Gómez, I.; López-Martínez, B.; Parra-Ortega, I. Respiratory Viral Infections in Pediatric Patients with Hematopoietic Stem Cell Transplantation. Bol. Med. Hosp. Infant. Mex. 2021, 78, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Champlin, R.E.; Ueno, N.T.; Anderlini, P.; Rolston, K.; Raad, I.; Kontoyiannis, D.; Jacobson, K.; Luna, M.; Tarrand, J.; et al. Infections Post Transplant Respiratory Syncytial Virus Infections in Autologous Blood and Marrow Transplant Recipients with Breast Cancer: Combination Therapy with Aerosolized Ribavirin and Parenteral Immunoglobulins. Bone Marrow Transplant. 2001, 28, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Hutspardol, S.; Essa, M.; Richardson, S.; Schechter, T.; Ali, M.; Krueger, J.; Fujii, H.; Egeler, R.M.; Gassas, A. Significant Transplantation-Related Mortality from Respiratory Virus Infections within the First One Hundred Days in Children after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 1802–1807. [Google Scholar] [CrossRef] [PubMed]
- Khanna, N.; Widmer, A.F.; Decker, M.; Steffen, I.; Halter, J.; Heim, D.; Weisser, M.; Gratwohl, A.; Fluckiger, U.; Hirsch, H.H. Respiratory Syncytial Virus Infection in Patients with Hematological Diseases: Single-Center Study and Review of the Literature. Clin. Infect. Dis. 2008, 46, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, J.; Campbell, A.P.; Cent, A.; Corey, L.; Boeckh, M. Comparison of Conventional and Molecular Detection of Respiratory Viruses in Hematopoietic Cell Transplant Recipients. Transpl. Infect. Dis. 2009, 11, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jang, J.H.; Lee, S.H.; Kim, Y.J.; Yoo, K.H.; Sung, K.W.; Lee, N.Y.; Ki, C.S.; Koo, H.H. Respiratory Viral Infections during the First 28 Days after Transplantation in Pediatric Hematopoietic Stem Cell Transplant Recipients. Clin. Transplant. 2012, 26, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; Ward, K.N.; Crooks, B.; Parker, A.; Martino, R.; Shaw, P.J.; Brinch, L.; Brune, M.; De, R.; Camara, L.; et al. Viral Infections Respiratory Virus Infections after Stem Cell Transplantation: A Prospective Study from the Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2001, 28, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.S.; Lee, G.M.; Gunawardane, N.; Burchett, S.K.; Lachenauer, C.S.; Lehmann, L.E. The Impact of RSV, Adenovirus, Influenza, and Parainfluenza Infection in Pediatric Patients Receiving Stem Cell Transplant, Solid Organ Transplant, or Cancer Chemotherapy. Pediatr. Transplant. 2013, 17, 133–143. [Google Scholar] [CrossRef]
- Martino, R.; Porras, R.P.; Rabella, N.; Williams, J.V.; Rámila, E.; Margall, N.; Labeaga, R.; Crowe, J.E.; Coll, P.; Sierra, J. Prospective Study of the Incidence, Clinical Features, and Outcome of Symptomatic Upper and Lower Respiratory Tract Infections by Respiratory Viruses Is Adult Recipients of Hematopoietic Stem Cell Transplants for Hematologic Malignancies. Biol. Blood Marrow Transplant. 2005, 11, 781–796. [Google Scholar] [CrossRef]
- Mccarthy, A.J.; Kingman, H.M.; Kelly, C.; Taylor, G.S.; Caul, E.O.; Grier, D.; Moppett, J.; Foot, A.; Cornish, J.M.; Oakhill, A.; et al. The Outcome of 26 Patients with Respiratory Syncytial Virus Infection Following Allogeneic Stem Cell Transplantation. Bone Marrow Transplant. 1999, 24, 1315–1322. [Google Scholar] [CrossRef]
- Mikulska, M.; Del Bono, V.; Gandolfo, N.; Dini, S.; Dominietto, A.; Di Grazia, C.; Bregante, S.; Varaldo, R.; Orsi, A.; Ansaldi, F.; et al. Epidemiology of Viral Respiratory Tract Infections in an Outpatient Haematology Facility. Ann. Hematol. 2014, 93, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Moret, F.; Marschall, J.; Atkinson, A.; Farag, S.; Zimmerli, S.; Pabst, T.; Sommerstein, R. Characteristics of Respiratory Virus Infections in Autologous Hematopoietic Stem Cell Transplantation Patients, a Prospective Study, Bern, Switzerland, 2015–2017. Infect. Dis. 2021, 53, 274–280. [Google Scholar] [CrossRef]
- Peck, A.J.; Englund, J.A.; Kuypers, J.; Guthrie, K.A.; Corey, L.; Morrow, R.; Hackman, R.C.; Cent, A.; Boeckh, M. Respiratory Virus Infection among Hematopoietic Cell Transplant Recipients: Evidence for Asymptomatic Parainfluenza Virus Infection. Blood 2007, 110, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Rowan, C.M.; Gertz, S.J.; Zinter, M.S.; Moffet, J.; Bajwa, R.P.S.; Barnum, J.L.; Kong, M. A Multicenter Investigation of Respiratory Syncytial Viral Infection in Children with Hematopoietic Cell Transplantation. Transpl. Infect. Dis. 2018, 20, e12882. [Google Scholar] [CrossRef]
- Samad, S.A.; Jethani, J.; Kumar, L.; Choudhary, A.; Brijwal, M.; Dar, L. Respiratory Syncytial Virus Infection among Adults after Hematopoietic Stem Cell Transplantation. J. Glob. Infect. Dis. 2022, 14, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, J.T.; Kirby, K.; Sandmaier, B.; Storb, R.; Corey, L.; Boeckh, M. Timing and Severity of Community Acquired Respiratory Virus Infections after Myeloablative versus Non-Myeloablative Hematopoietic Stem Cell Transplantation. Haematologica 2009, 94, 1101–1108. [Google Scholar] [CrossRef]
- Small, T.N.; Casson, A.; Malak, S.F.; Boulad, F.; Kiehn, T.E.; Stiles, J.; Ushay, H.M.; Sepkowitz, K.A. Viral Infections Respiratory Syncytial Virus Infection Following Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2002, 29, 321–327. [Google Scholar] [CrossRef]
- Wang, L.; Allen, J.; Diong, C.; Goh, Y.T.; Gopalakrishnan, S.; Ho, A.; Hwang, W.; Lim, F.; Oon, L.; Tan, T.T.; et al. Respiratory Virus Infection after Allogeneic Hematopoietic Stem Cell Transplant in a Tropical Center: Predictive Value of the Immunodeficiency Scoring Index. Transpl. Infect. Dis. 2017, 19, e12693. [Google Scholar] [CrossRef]
- Yue, C.; Kang, Z.; Ai, K.; Xu, D.; Wu, J.; Pan, Y.; Yan, J.; Liu, M.; Liu, Q. Virus Infection Facilitates the Development of Severe Pneumonia in Transplant Patients with Hematologic Malignancies. Oncotarget 2016, 7, 53930–53940. [Google Scholar] [CrossRef]
- Mccoy, D.; Wong, E.; Kuyumjian, A.G.; Wynd, M.A.; Sebti, R.; Munk, G.B. Treatment of Respiratory Syncytial Virus Infection in Adult Patients with Hematologic Malignancies Based on an Institution-Specific Guideline. Transpl. Infect. Dis. 2011, 13, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Barton, T.D. Viral Respiratory Tract Infections in Transplant Patients Epidemiology, Recognition and Management. Drugs 2007, 67, 1411–1427. [Google Scholar] [CrossRef] [PubMed]
- Bylsma, L.C.; Suh, M.; Movva, N.; Fryzek, J.P.; Nelson, C.B. Mortality among US Infants and Children Under 5 Years of Age with Respiratory Syncytial Virus and Bronchiolitis: A Systematic Literature Review. J. Infect. Dis. 2022, 226, S267–S281. [Google Scholar] [CrossRef] [PubMed]
- Celante, H.; Oubaya, N.; Fourati, S.; Beaune, S.; Khellaf, M.; Casalino, E.; Ricard, J.D.; Vieillard-Baron, A.; Heming, N.; Mekontso Dessap, A.; et al. Prognosis of Hospitalised Adult Patients with Respiratory Syncytial Virus Infection: A Multicentre Retrospective Cohort Study. Clin. Microbiol. Infect. 2023, 29, 943.e1–943.e8. [Google Scholar] [CrossRef] [PubMed]
- Whimbey, E.; Champlin, R.E.; Couch, R.B.; Englund, J.A.; Goodrich, J.M.; Raad, I.; Przepiorka, D.; Lewis, V.A.; Mirza, N.; Yousuf, H.; et al. Community Respiratory Virus Infections among Hospitalized Adult Bone Marrow Transplant Recipients. Clin. Infect. Dis. 1996, 22, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Hertz, M.I.; Englung, J.A.; Snover, D.; Bitterman, P.B.; McGlave, P.B. Respiratory Syncytial Virus-Induced Acute Lung Injury in Adult Patients with Bone Marrow Transplant: A Clinical Approach and Review of the Literature. Medicine 1989, 68, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Waghmare, A.; Campbell, A.P.; Xie, H.; Seo, S.; Kuypers, J.; Leisenring, W.; Jerome, K.R.; Englund, J.A.; Boeckh, M. Respiratory Syncytial Virus Lower Respiratory Disease in Hematopoietic Cell Transplant Recipients: Viral RNA Detection in Blood, Antiviral Treatment, and Clinical Outcomes. Clin. Infect. Dis. 2013, 57, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Chemaly, R.F.; Ghosh, S.; Bodey, G.P.; Rohatgi, N.; Safdar, A.; Keating, M.J.; Champlin, R.E.; Aguilera, E.A.; Tarrand, J.J.; Raad, I.I. Respiratory Viral Infections in Adults with Hematologic Malignancies and Human Stem Cell Transplantation Recipients: A Retrospective Study at a Major Cancer Center. Medicine 2006, 85, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P. Respiratory Syncytial Virus in Hematopoietic Cell Transplant Recipients: Factors Determining Progression to Lower Respiratory Tract Disease. J. Infect. Dis. 2014, 209, 1151–1152. [Google Scholar] [CrossRef]
- Shah, D.P.; Ghantoji, S.S.; Mulanovich, V.E.; Ariza-Heredia, E.J.; Chemaly, R.F. Review Article Management of Respiratory Viral Infections in Hematopoietic Cell Transplant Recipients. Am. J. Blood Res. 2012, 2, 203–218. [Google Scholar]
- Fontana, L.; Strasfeld, L. Respiratory Virus Infections of the Stem Cell Transplant Recipient and the Hematologic Malignancy Patient. Infect. Dis. Clin. N. Am. 2019, 33, 523–544. [Google Scholar] [CrossRef] [PubMed]
- Manuel, O.; Estabrook, M. RNA Respiratory Viral Infections in Solid Organ Transplant Recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13511. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Lenzi, N.; Valette, M.; Foulongne, V.; Krivine, A.; Houhou, N.; Lagathu, G.; Rogez, S.; Alain, S.; Duval, X.; et al. Clinical Characteristics and Outcome of Respiratory Syncytial Virus Infection among Adults Hospitalized with Influenza-like Illness in France. Clin. Microbiol. Infect. 2017, 23, 253–259. [Google Scholar] [CrossRef]
- Paulsen, G.C.; Danziger-Isakov, L. Respiratory Viral Infections in Solid Organ and Hematopoietic Stem Cell Transplantation. Clin. Chest Med. 2017, 38, 707–726. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Guthrie, K.A.; Waghmare, A.; Walsh, E.E.; Falsey, A.R.; Kuypers, J.; Cent, A.; Englund, J.A.; Boeckh, M. Respiratory Syncytial Virus in Hematopoietic Cell Transplant Recipients: Factors Determining Progression to Lower Respiratory Tract Disease. J. Infect. Dis. 2014, 209, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Harrington, R.D.; Hooton, T.M.; Hackman, R.C.; Storch, G.A.; Osborne, B.; Gleaves, C.A.; Benson, A.; Meyers, J.D. An Outbreak of Respiratory Syncytial Virus in a Bone Marrow Transplant Center. J. Infect. Dis. 1992, 165, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.G.; Metzger, K.; Bolon, M.K.; Silkaitis, C.; Mielnicki, M.; Cullen, J.; Rooney, M.; Blanke, T.; Tahboub, A.E.; Noskin, G.A.; et al. Respiratory Syncytial Virus Outbreak on an Adult Stem Cell Transplant Unit. Am. J. Infect. Control 2016, 44, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Mendes, E.T.; Ramos, J.; Peixoto, D.; Dulley, F.; Alves, T.; Vilas Boas, L.S.; Batista, M.V.; Da Silva, D.P.; Levin, A.S.; Shikanai-Yasuda, M.A.; et al. An Outbreak of Respiratory Syncytial Virus Infection in Hematopoietic Stem Cell Transplantation Outpatients: Good Outcome without Specific Antiviral Treatment. Transpl. Infect. Dis. 2013, 15, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Kassis, C.; Champlin, R.E.; Hachem, R.Y.; Hosing, C.; Tarrand, J.J.; Perego, C.A.; Neumann, J.L.; Raad, I.I.; Chemaly, R.F. Detection and Control of a Nosocomial Respiratory Syncytial Virus Outbreak in a Stem Cell Transplantation Unit: The Role of Palivizumab. Biol. Blood Marrow Transplant. 2010, 16, 1265–1271. [Google Scholar] [CrossRef]
- Lehners, N.; Tabatabai, J.; Prifert, C.; Wedde, M.; Puthenparambil, J.; Weissbrich, B.; Biere, B.; Schweiger, B.; Egerer, G.; Schnitzler, P. Long-Term Shedding of Influenza Virus, Parainfluenza Virus, Respiratory Syncytial Virus and Nosocomial Epidemiology in Patients with Hematological Disorders. PLoS ONE 2016, 11, e0148258. [Google Scholar] [CrossRef]
- Weigt, S.S.; Gregson, A.L.; Deng, J.C.; Lynch, J.P.; Belperio, J.A. Respiratory Viral Infections in Hematopoietic Stem Cell and Solid Organ Transplant Recipients. Semin. Respir. Crit. Care Med. 2011, 32, 471–493. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Corrado, S.; Palmieri, S.; Marchesi, F. Respiratory Syncytial Virus: A Systematic Review and Meta-Analysis of Tomographic Findings (2000–2022). Children 2023, 10, 1169. [Google Scholar] [CrossRef] [PubMed]
- Auvinen, R.; Syrjänen, R.; Ollgren, J.; Nohynek, H.; Skogberg, K. Clinical Characteristics and Population-Based Attack Rates of Respiratory Syncytial Virus versus Influenza Hospitalizations among Adults—An Observational Study. Influenza Other Respir. Viruses 2022, 16, 276–288. [Google Scholar] [CrossRef]
- Baraldi, E.; Checcucci Lisi, G.; Costantino, C.; Heinrichs, J.H.; Manzoni, P.; Riccò, M.; Roberts, M.; Vassilouthis, N. RSV Disease in Infants and Young Children: Can We See a Brighter Future? Hum. Vaccin. Immunother. 2022, 18, 2079322. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Ranzieri, S. Respiratory Syncytial Virus: Knowledge, Attitudes and Beliefs of General Practitioners from North-Eastern Italy (2021). Pediatr. Rep. 2022, 14, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B. Respiratory Syncytial Virus and Parainfluenza Virus. N. Engl. J. Med. 2001, 344, 1917–1926. [Google Scholar] [CrossRef]
- Hall, C.B.; Long, C.E.; Schnabel, K.C. Respiratory Syncytial Virus Infections in Previously Healthy Working Adults. Clin. Infect. Dis. 2001, 33, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.; Dazzi, F. Bone Marrow Transplantation 1957–2019. Front. Immunol. 2019, 10, 1246. [Google Scholar] [CrossRef]
- Granot, N.; Storb, R. History of Hematopoietic Cell Transplantation: Challenges and Progress. Haematologica 2020, 105, 2716–2729. [Google Scholar] [CrossRef]
- Karhana, S.; Hussain, K.; Bint-E-attar, G.; Bhurani, D.; Khan, M.A. Risk of Mortality in Bone Marrow Transplant Patients During SARS-CoV-2 Infection: A Systematic Review. Exp. Clin. Transplant. 2023, 21, 1–11. [Google Scholar] [CrossRef]
- Müller, O.; Razum, O.; Jahn, A. Effects of Non-Pharmaceutical Interventions against COVID-19 on the Incidence of Other Diseases. Lancet Reg. Health-Eur. 2021, 6, 100139. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the Effects of Non-Pharmaceutical Interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Peruzzi, S.; Balzarini, F. Public Perceptions on Non-Pharmaceutical Interventions for West Nile Virus Infections: A Survey from an Endemic Area in Northern Italy. Trop. Med. Infect. Dis. 2021, 6, 116. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Satta, E.; Ranzieri, S. Excess Mortality on Italian Small Islands during the SARS-CoV-2 Pandemic: An Ecological Study. Infect. Dis. Rep. 2022, 14, 391–412. [Google Scholar] [CrossRef] [PubMed]
- Weiner, J.H. Respiratory Syncytial Virus Infection and Palivizumab: Are Families Receiving Accurate Information? Am. J. Perinatol. 2010, 27, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, I.; Li, A.; Bjornson, C.L.; Lanctot, K.L.; Paes, B.A. Respiratory Syncytial Virus Immunoprophylaxis with Palivizumab: 12-Year Observational Study of Usage and Outcomes in Canada. Am. J. Perinatol. 2022, 39, 1668–1677. [Google Scholar] [CrossRef] [PubMed]
- Frogel, M.P.; Stewart, D.L.; Hoopes, M.; Fernandes, A.W.; Mahadevia, P.J. A Systematic Review of Compliance with Palivizumab Administration for RSV Immunoprophylaxis. J. Manag. Care Pharm. 2010, 16, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Boeckh, M.; Berrey, M.M.; Bowden, R.A.; Crawford, S.W.; Balsley, J.; Corey, L. Phase 1 Evaluation of the Respiratory Syncytial Virus-Specific Monoclonal Antibody Palivizumab in Recipients of Hematopoietic Stem Cell Transplants Downloaded From. J. Infect. Dis. 1998, 184, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.L.; Agwan, S.; Hassan, M.; van Driel, M.L.; Del Mar, C.B. Immunoglobulin Treatment for Hospitalised Infants and Young Children with Respiratory Syncytial Virus Infection. Cochrane Database Syst. Rev. 2019, 8, CD009417. [Google Scholar] [CrossRef]
- Olchanski, N.; Hansen, R.N.; Pope, E.; D’Cruz, B.; Fergie, J.; Goldstein, M.; Krilov, L.R.; McLaurin, K.K.; Nabrit-Stephens, B.; Oster, G.; et al. Palivizumab Prophylaxis for Respiratory Syncytial Virus: Examining the Evidence around Value. Open Forum Infect. Dis. 2018, 5, ofy031. [Google Scholar] [CrossRef]
- Sánchez Luna, M.; Manzoni, P.; Paes, B.; Baraldi, E.; Cossey, V.; Kugelman, A.; Chawla, R.; Dotta, A.; Rodríguez Fernández, R.; Resch, B.; et al. Expert Consensus on Palivizumab Use for Respiratory Syncytial Virus in Developed Countries. Paediatr. Respir. Rev. 2020, 33, 35–44. [Google Scholar] [CrossRef]
- Mac, S.; Sumner, A.; Duchesne-Belanger, S. Cost-Effectiveness of Palivizumab for Respiratory Syncytial Virus: A Systematic Review. Pediatrics 2019, 143, 20184064. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Abu Raya, B.; Baraldi, E.; Flanagan, K.; Martinon Torres, F.; Tsolia, M.; Zielen, S. RSV Prevention in All Infants: Which Is the Most Preferable Strategy? Front. Immunol. 2022, 13, 880368. [Google Scholar] [CrossRef] [PubMed]
- Voirin, N.; Virlogeux, V.; Demont, C.; Kieffer, A. Potential Impact of Nirsevimab on RSV Transmission and Medically Attended Lower Respiratory Tract Illness Caused by RSV: A Disease Transmission Model. Infect. Dis. Ther. 2021, 11, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M.; Fleming-Dutra, K.E.; Prill, M.M.; Roper, L.E.; Brooks, O.; Sánchez, P.J.; Kotton, C.N.; Mahon, B.E.; Meyer, S.; Long, S.S.; et al. Use of Nirsevimab for the Prevention of Respiratory Syncytial Virus Disease among Infants and Young Children: Recommendations of the Advisory Committee on Immunization Practices-United States, 2023. Morb. Mortal. Wkly. Rep. 2023, 72, 920–925. [Google Scholar] [CrossRef]
- Francisco, L.; Cruz-Cañete, M.; Pérez, C.; Couceiro, J.A.; Otheo, E.; Launes, C.; Rodrigo, C.; Jiménez, A.B.; Llorente, M.; Montesdeoca, A.; et al. Nirsevimab for the Prevention of Respiratory Syncytial Virus Disease in Children: Statement of the Spanish Society of Paediatric Infectious Disease (SEIP). An. Pediatría (Engl. Ed.) 2023, 99, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Domachowske, J.B.; Anderson, E.J.; Goldstein, M. The Future of Respiratory Syncytial Virus Disease Prevention and Treatment. Infect. Dis. Ther. 2021, 10, 47–60. [Google Scholar] [CrossRef]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Checcucci Lisi, G.; et al. Epidemiology and Prevention of Respiratory Syncytial Virus Infections in Children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef]
- Verwey, C.; Madhi, S.A. Review and Update of Active and Passive Immunization Against Respiratory Syncytial Virus. BioDrugs 2023, 37, 295–309. [Google Scholar] [CrossRef]
- Bouzid, D.; Visseaux, B.; Ferré, V.M.; Peiffer-Smadja, N.; Le Hingrat, Q.; Loubet, P. Respiratory Syncytial Virus in Adults with Comorbidities: An Update on Epidemiology, Vaccines, and Treatments. Clin. Microbiol. Infect. 2023, 29, 1538–1550. [Google Scholar] [CrossRef]
- Cunningham, C.K.; Karron, R.A.; Muresan, P.; Kelly, M.S.; McFarland, E.J.; Perlowski, C.; Libous, J.; Oliva, J.; Jean-Philippe, P.; Moye, J.; et al. Evaluation of Recombinant Live-Attenuated Respiratory Syncytial Virus (RSV) Vaccines RSV/ΔNS2/Δ1313/I1314L and RSV/276 in RSV-Seronegative Children. J. Infect. Dis. 2022, 226, 2069–2078. [Google Scholar] [CrossRef] [PubMed]
- Vidal Valero, M. “A Good Day”: FDA Approves World’s First RSV Vaccine. Nature 2023, 617, 234–235. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D.E.; Patel, S.R.; Skinner, R.; Dignan, F.; Richter, A.; Jeffery, K.; Khan, A.; Heath, P.T.; Clark, A.; Orchard, K.; et al. Joint Consensus Statement on the Vaccination of Adult and Paediatric Haematopoietic Stem Cell Transplant Recipients: Prepared on Behalf of the British Society of Blood and Marrow Transplantation and Cellular Therapy (BSBMTCT), the Children’s Cancer and Leukaemia Group (CCLG), and British Infection Association (BIA). J. Infect. 2023, 86, 1–8. [Google Scholar] [PubMed]








| Item | Definition |
|---|---|
| Population of interest | Individuals having received bone marrow transplant |
| Exposure | The occurrence of Respiratory Syncytial Virus (RSV) infection |
| Control/comparator | in children and adults Comparison to other respiratory pathogens (influenza, adenovirus, and human metapneumovirus) |
| Outcome | Occurrence of RSV infections, RSV-related lower respiratory tract infections and RSV-related deaths |
| Study | Country | Timeframe (Month–Year) | Design | BMT (N.) | Pediatric Cases (N., %) | Allogenic BMT (N., %) | RSV Cases | Flu (N.) | HAdV (N.) | hMPV (N.) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases (N.) | Attack Rate (%) | LRTI (N., %) | Deaths (N.) | CFR (%) | ||||||||||
| Avetysian et al., 2009 [80] | Sweden | 01/2000–12/2007 | S, R | 275 | NA | 275, 100% | 32 | 11.64% | 14, 43.75% | 5 | 15.63% | - | - | - |
| Campbell et al., 2015 [81] | USA | 12/2005–02/2010 | S, R | 451 | 52, 11.53% | 451, 100% | 9 | 2.00% | 0, - | 1 | 11.11% | 10 | 5 | 4 |
| Chakrabarti et al., 2002 [51] | UK | 06/1997–08/2001 | S, R | 83 | 0, - | 83, 100% | 13 | 15.66% | 6, 46.15% | 0 | - | 5 | - | - |
| Choi et al., 2013 [82] | Korea | 01/2007–03/2010 | S, R | 175 | 175, 100% | 96, 54.86% | 23 | 13.14% | 12, 52.17% | 2 | 8.70% | 4 | 12 | 1 |
| El-Bietar et al., 2016 [61] | USA | 06/2008–12/2014 | S, R | 450 | 450, 100% | 450, 100% | 32 | 7.11% | 6, 18.75% | 1 | 3.13% | - | - | - |
| Fisher et al., 2018 [83] | USA | 01/2010–06/2013 | M, R | 1560 | 1560, 100% | 1144, 73.33% | 40 | 2.56% | 13, 32.50% | 4 | 10.00% | 29 | - | 17 |
| Garrett Nichols et al., 2001 [84] | USA | 1989–1999 | S, R | 3897 | NA | NA | 171 | 4.39% | 68, 39.77% | 30 | 17.54% | - | - | - |
| Gaytan Morales et al., 2021 [85] | Mexico | 01/2017–12/2019 | S, P | 54 | 54, 100% | 11, 20.37% | 5 | 9.26% | 5, 100% | 1 | 20.00% | 7 | 4 | 4 |
| Ghosh et al., 2001 [86] | USA | 11/1992–11/2000 | S, R | 249 | 0, - | 249, 100% | 9 | 3.61% | 5, 55.56% | 0 | - | - | - | - |
| Gueller et al., 2013 [68] | Germany | 10/2011–04/2012 | S, R | 29 | 0, - | 29, 100% | 10 | 34.48% | 5, 50.00% | 3 | 30.00% | - | - | - |
| Hutspardol et al., 2015 [87] | Canada | 01/2000–12/2012 | S, R | 844 | 844, 100% | 491, 58.18% | 15 | 1.78% | 8, 53.33% | 1 | 6.67% | 12 | 4 | 2 |
| Khanna et al., 2008 [88] | Switzerland | 02/2002–04/2007 | S, R | 402 | NA | 283, 70.40% | 27 | 6.72% | 7, 25.93% | 3 | 11.11% | - | - | - |
| Kuypers et al., 2009 [89] | USA | 12/2000–06/2004 | S, P | 157 | NA | NA | 6 | 3.82% | NA | 0 | 0.00% | 3 | 0 | 8 |
| Lavergne et al., 2011 [46] | Canada | 07/1999–06/2003 | S, R | 461 | 0, - | 293, 63.56% | 30 | 6.51% | 16, 53.33% | 4 | 13.33% | - | - | - |
| Lee et al., 2012 [90] | Korea | 01/2007–08/2009 | S, R | 176 | 176, 100% | 82, 46.59% | 9 | 5.11% | NA | 1 | 11.11% | - | 1 | - |
| Ljungman et al., 2001 [91] | Various | 10/1997–10/1998 | M, R | 1973 | NA | 819, 41.51% | 20 | 1.01% | 14, 70.00% | 3 | 15.00% | 16 | - | - |
| Lo et al., 2013 [92] | USA | 01/1993–03/2006 | S, R | 557 | 557, 100% | NA | 34 | 6.10% | 14, 41.18% | 1 | 2.94% | 6 | 24 | - |
| Martino et al., 2005 [93] | Spain | 09/1999–10/2003 | S, R | 386 | 0, - | 172, 44.56% | 19 | 4.92% | 11, 57.89% | 2 | 10.53% | 39 | 11 | 16 |
| McCarthy et al., 1999 [94] | UK | 09/1987–08/1998 | S, R | 572 | 381, 66.61% | 474, 82.87% | 26 | 4.55% | 15, 57.69% | 5 | 19.23% | - | - | - |
| McCoy et al., 2011 [104] | USA | 09/2006–04/2009 | S, R | 539 | 0, - | 196, 36.36% | 26 | 4.82% | 13, 50.00% | 0 | - | - | - | - |
| Mikulska et al., 2014 [95] | Italy | 01/2011–03/2011 | S, P | 193 | 0, - | 127, 65.80% | 21 | 10.88% | 2, 9.52% | 0 | - | 20 | 3 | - |
| Moret et al., 2021 [96] | Switzerland | 11/2015–04/2016 11/2016–04/2017 | S, P | 156 | 0, - | 0, - | 4 | 2.56% | 0, - | 0 | - | 3 | 1 | 1 |
| Peck et al., 2007 [97] | UK | 12/2000–06/2004 | S, R | 814 | NA | NA | 6 | 0.74% | 1, 16.67% | 0 | - | 4 | - | 6 |
| Rowan et al., 2018 [98] | USA | 01/2010–12/2014 | M, R | 1522 | 1522, 100% | NA | 47 | 3.09% | 9, 19.15% | 1 | 2.13% | - | - | - |
| Samad et al., 2022 [99] | India | 01/2017–08/2021 | S, P | 100 | 0, - | NA | 11 | 11.00% | 2, 18.18% | 0 | - | - | - | - |
| Schiffer et al., 2009 [100] | USA | 12/1997–03/2005 | S, R | 2453 | NA | 1620, 66.04% | 44 | 1.79% | 12, 27.27% | 0 | - | 30 | - | - |
| Schleuning et al., 2004 [70] | Germany | 07/1998–06/2001 | S, R | 334 | NA | 334, 100% | 8 | 2.40% | 4, 50.00% | 2 | 25.00% | - | 16 | - |
| Small et al., 2002 [101] | USA | 01/1994–12/1999 | S, R | 942 | 154, 16.35% | 548, 58.17% | 54 | 5.73% | 25, 46.30% | 3 | 5.56% | - | - | - |
| Wang et al., 2017 [102] | Singapore | 12/2010–10/2012 | S, R | 195 | 11, 5.64% | 195, 100% | 43 | 22.05% | 12, 27.91% | 4 | 9.30% | 25 | 21 | 46 |
| Yue et al., 2016 [103] | China | 03/2011–02/2013 | S, R | 68 | 0 | 68, 100% | 27 | 39.71% | 16, 59.26% | 1 | 3.70% | - | - | - |
| Collected Studies | N. | 30 |
| Collected cases of BMT | N. | 20,067 |
| Cases < 18 years of age | N. (% of total cases) | 5936 (29.58%) |
| Cases ≥ 18 years of age | 3826 (19.07%) | |
| Undefined | 9762 (48.65%) | |
| Cases of allogenic transplantation | N. (% of total cases) | 8490 (42.31%) |
| Cases of autologous transplantation | 4530 (22.57%) | |
| Undefined | 7047 (35.12%) | |
| Observation | person-years | 130,622.81 |
| Collected RSV cases | N. (% of total cases) | 821 (4.09%) |
| LRTI cases | N. (% of RSV cases) | 351 (42.75%) |
| RSV-related deaths | N. (% of RSV cases) | 78 (9.5%) |
| Treatment with Palivizumab | N. (% of RSV cases) | 30 (3.65%) |
| Cases sampled for Influenza | N. | 10,051 |
| Collected Influenza cases | N. (% of sampled cases) | 213 (2.12%) |
| Cases sampled for Adenovirus | N. | 3678 |
| Collected Adenovirus cases | N. (%of sampled cases) | 102 (2.77%) |
| Cases sampled for hMPV | N. | 4792 |
| Collected hMPV cases | N. (%of sampled cases) | 105 (2.19%) |
| Total (No./20,067, %) | Positive (No./821, %) | Crude Attack Rate (%) | Risk Ratio | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Country | |||||
| Canada | 1305, 6.50% | 45, 5.48% | 3.45% | 0.933 | 0.691; 1.261 |
| China | 68, 0.34% | 27, 3.29% | 39.71% | 10.784 | 7.915; 14.596 |
| Germany | 363, 1.81% | 18, 2.19% | 4.96% | 1.342 | 0.848; 2.124 |
| India | 100, 0.50% | 11, 1.34% | 11.00% | 2.978 | 1.693; 5.236 |
| Italy | 193, 0.96% | 21, 2.56% | 10.88% | 2.945 | 1.948; 4.453 |
| South Korea | 175, 0.87% | 23, 2.80% | 13.14% | 3.558 | 2.406; 5.260 |
| Mexico | 54, 0.27% | 5, 0.61% | 9.26% | 2.506 | 1.082; 5.804 |
| Singapore | 195, 0.97% | 43, 5.24% | 22.05% | 5.969 | 4.520; 7.885 |
| Spain | 386, 1.92% | 19, 2.31% | 4.92% | 1.332 | 0.852; 2.084 |
| Sweden | 275, 1.37% | 32, 3.90% | 11.64% | 3.150 | 2.248; 4.414 |
| Switzerland | 558, 2.78% | 31, 3.78% | 5.56% | 1.504 | 1.056; 2.141 |
| United Kingdom | 1469, 7.32% | 45, 5.48% | 3.06% | 0.829 | 0.614; 1.120 |
| United States | 12,777, 63.67% | 472, 57.49% | 3.69% | 1.000 | REFERENCE |
| Various (Europe) | 1973, 9.78483% | 20, 2.44% | 1.01% | 0.274 | 0.176; 0.428 |
| Timeframe | |||||
| Before 2005 | 8050, 40.12% | 301, 36.66% | 3.74% | 0.867 | 0.733; 1.025 |
| 2005–2009 | 4487, 22.36% | 134, 16.32% | 2.99% | 0.682 | 0.553; 0.841 |
| 2010–2014 | 2130, 10.61% | 153, 18.64% | 7.18% | 1.665 | 1.366; 2.029 |
| 2015 onwards | 5400, 26.91% | 233, 28.38% | 4.31% | 1.000 | REFERENCE |
| Patients | |||||
| Adults and Pediatric | 8166, 40.69% | 248, 30.21% | 3.04% | 1.000 | REFERENCE |
| Adults only | 6563, 32.71% | 368, 44.82% | 5.61% | 1.846 | 1.580; 2.162 |
| Pediatric only | 5338, 26.60% | 205, 24.97% | 3.84% | 1.264 | 1.054; 1.517 |
| Study Design | |||||
| Multi-center | 5055, 25.19% | 107, 13.03% | 2.12% | 0.445 | 0.364; 0.544 |
| Single center | 15,012, 74.81% | 714, 86.97% | 4.76% | 1.000 | REFERENCE |
| Total (No./821, %) | Deaths (No./78, %) | Case Fatality Ratio (%) | Risk Ratio | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Country | |||||
| Canada | 45, 5.48% | 5, 6.41% | 11.11% | 1.279 | 0.532; 3.073 |
| China | 27, 3.29% | 1, 1.28% | 3.70% | 0.426 | 0.061; 2.983 |
| Germany | 18, 2.19% | 5, 6.41% | 27.78% | 3.198 | 1.436; 7.119 |
| India | 11, 1.34% | 0, - | 0 | 0.523 | 0.034; 7.974 |
| Italy | 21, 2.56% | 0, - | 0 | 0.274 | 0.017; 4.306 |
| Korea | 23, 2.80% | 3, 3.85% | 9.38% | 1.502 | 0.502; 4.885 |
| Mexico | 5, 0.61% | 1, 1.28% | 20.00% | 2.302 | 0.389; 13.616 |
| Singapore | 43, 5.24% | 4, 5.13% | 9.30% | 1.071 | 0.403; 2.848 |
| Spain | 19, 2.31% | 2, 2.56% | 10.53% | 1.212 | 0.316; 4.642 |
| Sweden | 32, 3.90% | 5, 6.41% | 15.63% | 1.799 | 0.763; 4.236 |
| Switzerland | 31, 3.78% | 3, 3.85% | 9.68% | 1.114 | 0.366; 3.396 |
| United Kingdom | 45, 5.48% | 5, 6.41% | 11.11% | 1.279 | 0.532; 3.073 |
| United States | 472, 57.49% | 41, 52.56% | 8.69% | 1.000 | REFERENCE |
| Various (Europe) | 20, 2.44% | 3, 3.85% | 15.00% | 1.727 | 0.584; 5.103 |
| Timeframe | |||||
| Before 2005 | 301, 36.66% | 43, 55.13% | 14.29% | 2.378 | 1.333; 4.239 |
| 2005–2009 | 134, 16.32% | 10, 12.82% | 7.46% | 1.242 | 0.567; 2.718 |
| 2010–2014 | 153, 18.64% | 11, 14.10% | 7.19% | 1.197 | 0.558; 2.566 |
| 2015 onwards | 233, 28.38% | 14, 17.95% | 6.01% | 1.000 | REFERENCE |
| Patients | |||||
| Adults and Pediatric | 248, 30.21% | 23, 29.49% | 9.27% | 1.000 | REFERENCE |
| Adults only | 368, 44.82% | 43, 55.13% | 11.68% | 1.260 | 0.780; 2.036 |
| Pediatric only | 205, 24.97% | 12, 15.38% | 5.85% | 0.631 | 0.322; 1.237 |
| Study Design | |||||
| Multicenter | 107, 13.03% | 8, 10.26% | 7.48% | 0.763 | 0.378; 1.540 |
| Single center | 714, 86.97% | 70, 89.74% | 9.40% | 1.000 | REFERENCE |
| RSV Attack Rate | RSV Incidence Rate | Proportion of LRTI | CFR | |
|---|---|---|---|---|
| Proportion of allogenic BMT cases | rho = 0.311 (95%CI −0.118 to 0.643) p = 0.139 | rho = −0.042 (95%CI −0.448 to 0.379) p = 0.846 | rho = −0.235 (95%CI −0.599 to 0.208) p = 0.280 | rho = 0.085 (95%CI −0.341 to 0.482) p = 0.693 |
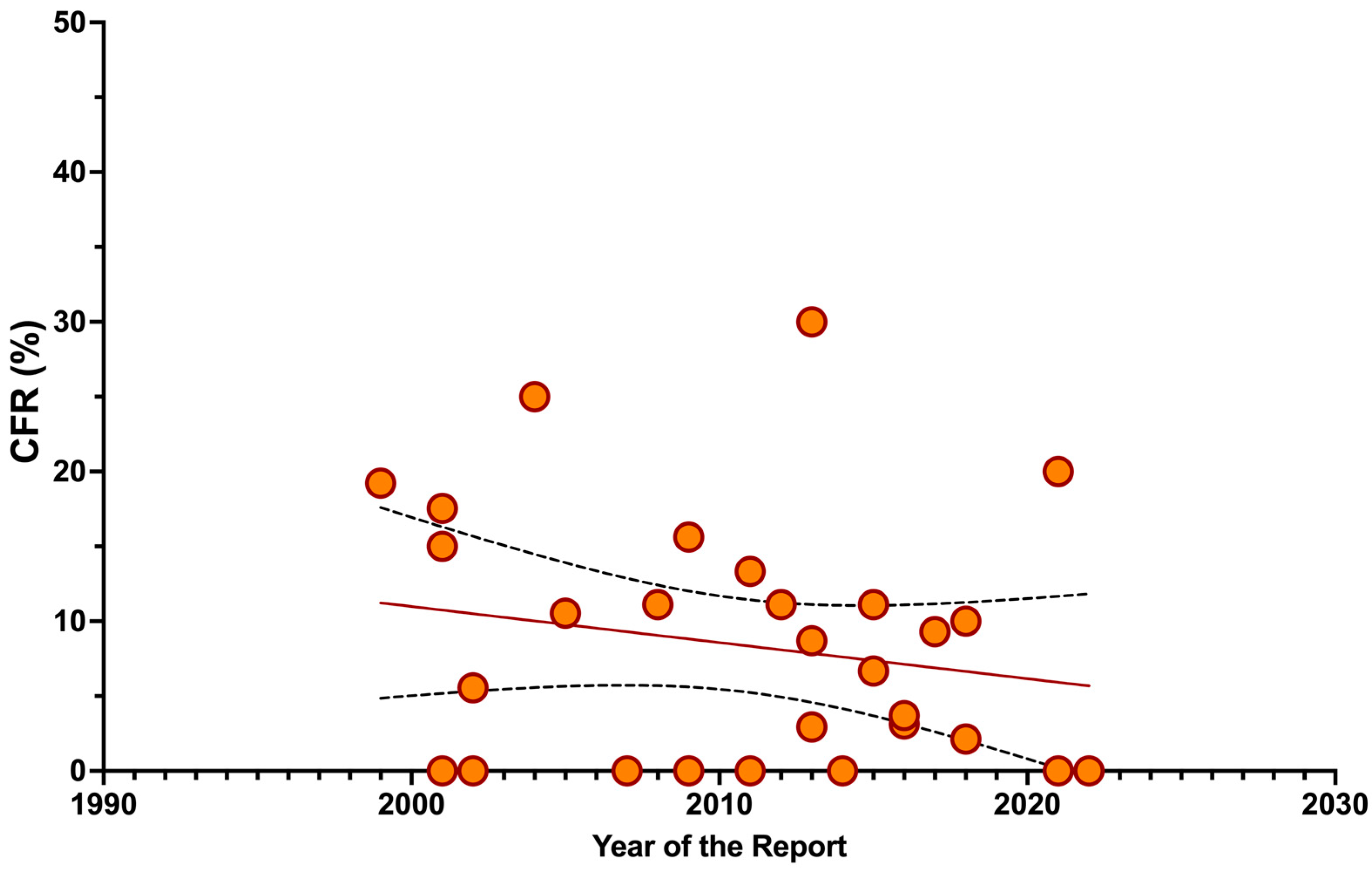
| Proportion of pediatric cases | rho = −0.283 (95%CI −0.638 to 0.170) p = 0.201 | rho = −0.433 (95%CI −0.729 to −0.001) p = 0.044 | rho = −0.008 (95%CI −0.449 to 0.437) p = 0.974 | rho = 0.317 (95%CI −0.134 to 0.659) p = 0.150 |
| Pooled Attack Rate per 100 Patients (95%CI) | τ2 | I2 (95%CI) | Q | p | ||
|---|---|---|---|---|---|---|
| RSV | 5.40 | 3.81; 7.60 | 0.966 | 94.4% (93.0; 95.6) | 519.16 | <0.001 |
| RSV (URTI) | 3.09 | 1.84; 5.15 | 1.894 | 93.0% (91.0; 94.6) | 385.45 | <0.001 |
| RSV (LRTI) | 1.90 | 1.20; 2.99 | 1.369 | 89.7% (86.4; 92.3) | 263.38 | <0.001 |
| Influenza | 2.65 | 1.53; 4.54 | 1.082 | 94.3% (92.1; 95.9) | 246.14 | <0.001 |
| AdV | 2.10 | 1.06; 4.14 | 1.188 | 83.1% (71.9; 89.9) | 65.17 | <0.001 |
| hMTP | 1.77 | 0.70; 4.49 | 1.986 | 95.8% (93.9; 97.1) | 215.75 | <0.001 |
| Pooled Incidence per 1000 Person-Years (95%CI) | τ2 | I2 (95%CI) | Q | p | ||
|---|---|---|---|---|---|---|
| RSV | 14.77 | 9.43; 20.12 | 0.001 | 91.6% (89.1; 93.5) | 345.84 | <0.001 |
| RSV (URTI) | 5.31 | 3.62; 6.99 | 0.001 | 88.4% (84.4; 91.4) | 232.55 | <0.001 |
| RSV (LRTI) | 3.99 | 2.40; 5.58 | 0.001 | 83.1% (76.5; 87.8) | 159.27 | <0.001 |
| Influenza | 10.45 | 4.04; 16.86 | 0.001 | 89.1% (83.7; 92.7) | 128.42 | <0.001 |
| HAdV | 9.64 | 2.95; 16.32 | 0.001 | 86.9% (78.9; 91.9) | 83.98 | <0.001 |
| hMPV | 15.56 | 0.00; 33.93 | 0.001 | 90.5% (84.6; 94.1) | 94.57 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Parisi, S.; Corrado, S.; Marchesi, F.; Bottazzoli, M.; Gori, D. Respiratory Syncytial Virus Infections in Recipients of Bone Marrow Transplants: A Systematic Review and Meta-Analysis. Infect. Dis. Rep. 2024, 16, 317-355. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020026
Riccò M, Parisi S, Corrado S, Marchesi F, Bottazzoli M, Gori D. Respiratory Syncytial Virus Infections in Recipients of Bone Marrow Transplants: A Systematic Review and Meta-Analysis. Infectious Disease Reports. 2024; 16(2):317-355. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020026
Chicago/Turabian StyleRiccò, Matteo, Salvatore Parisi, Silvia Corrado, Federico Marchesi, Marco Bottazzoli, and Davide Gori. 2024. "Respiratory Syncytial Virus Infections in Recipients of Bone Marrow Transplants: A Systematic Review and Meta-Analysis" Infectious Disease Reports 16, no. 2: 317-355. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020026