
Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (Mean ± Standard deviation) |
|---|---|
| Total sample number | 20 |
| Sex | Male |
| Age (years) | 58.0 ± 10.6 |
| Height (cm) | 167.9 ± 6.2 |
| Weight (kg) | 66.1 ± 10.6 |
| BMI (kg/m2) | 23.4 ± 3.3 |
| SBP (mmHg) | 151.2 ± 17.9 |
| DBP (mmHg) | 90.7 ± 5.0 |
2.2. Experimental Sites
2.3. Physiological Indices
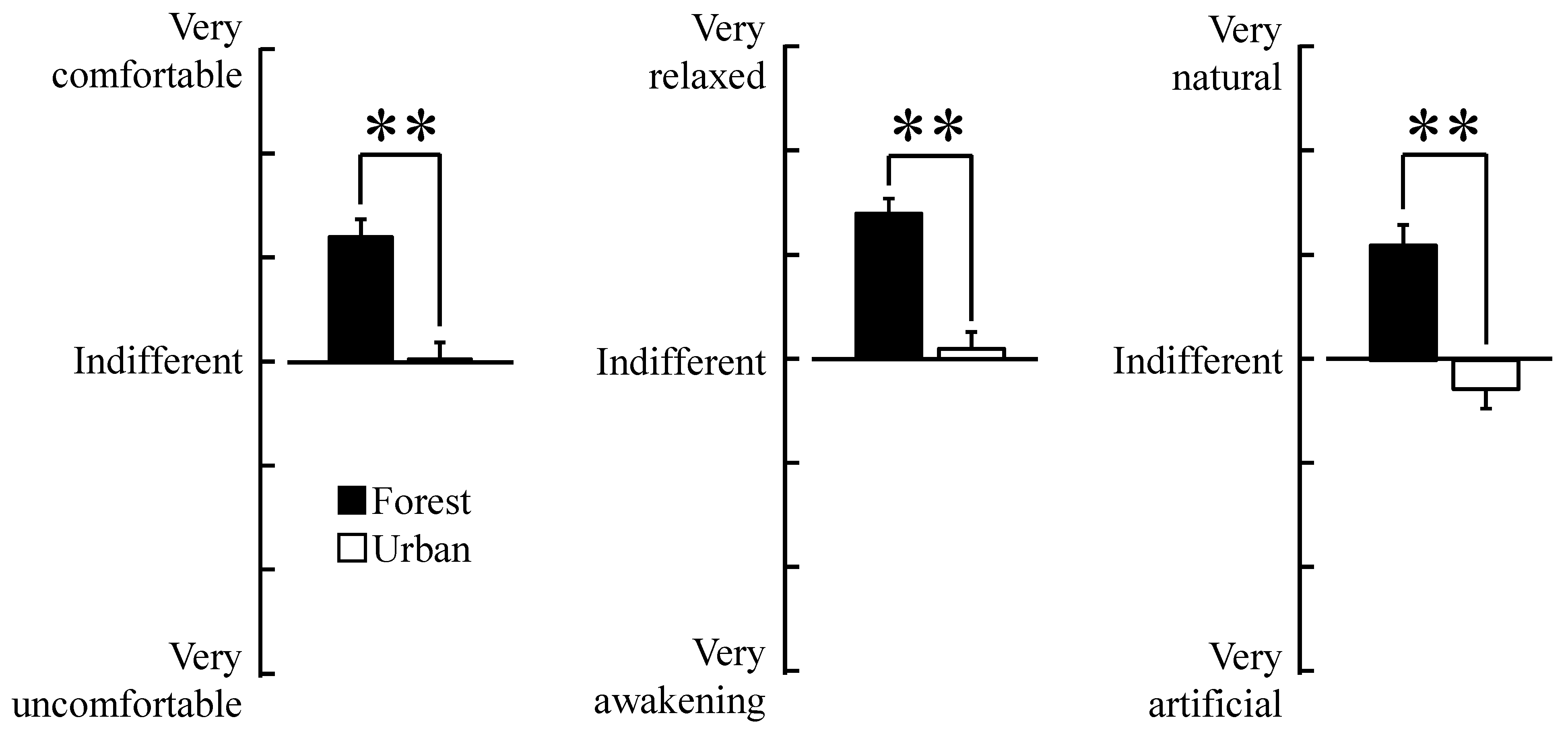
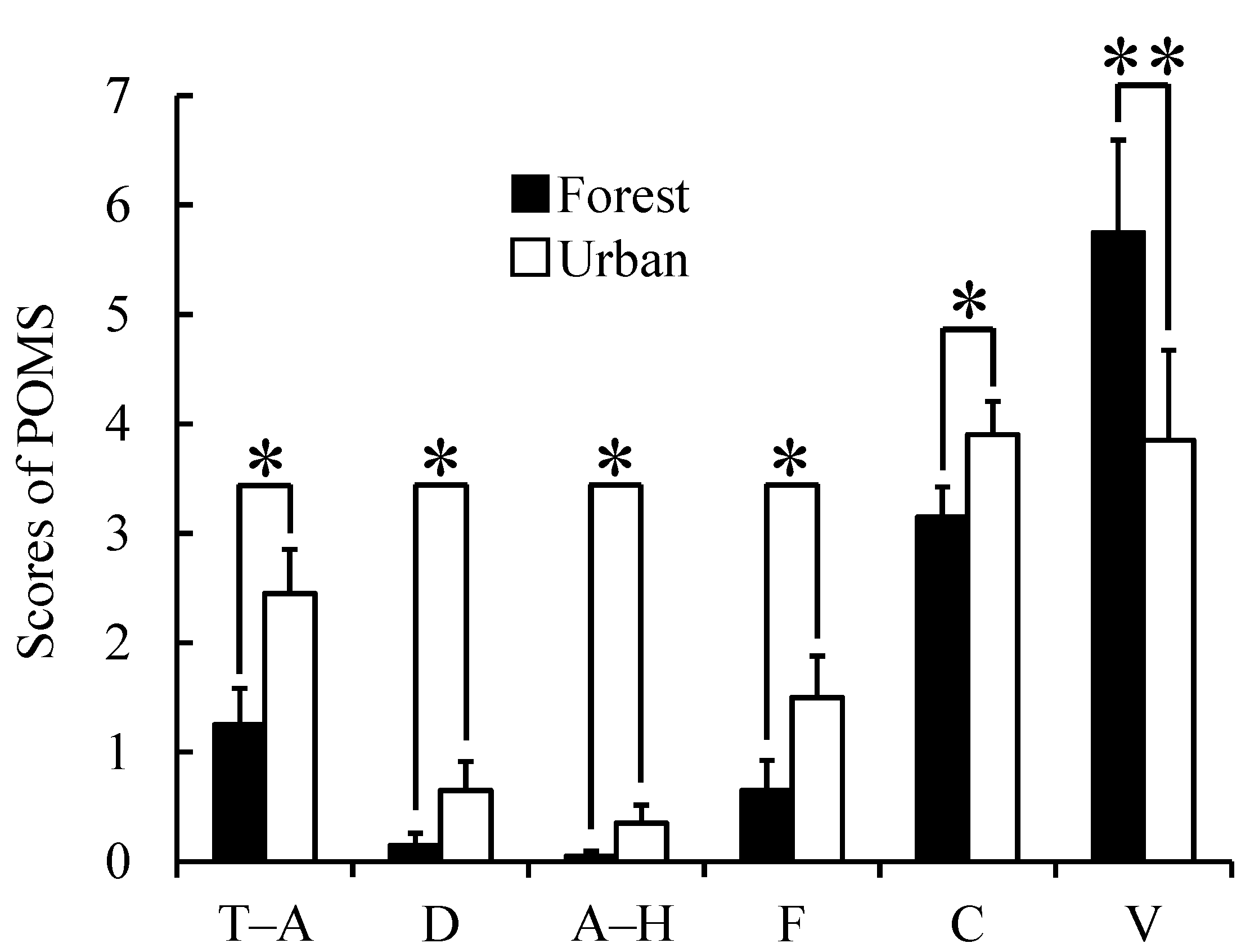
2.4. Psychological Indices
2.5. Experimental Design

2.6. Statistical Analyses
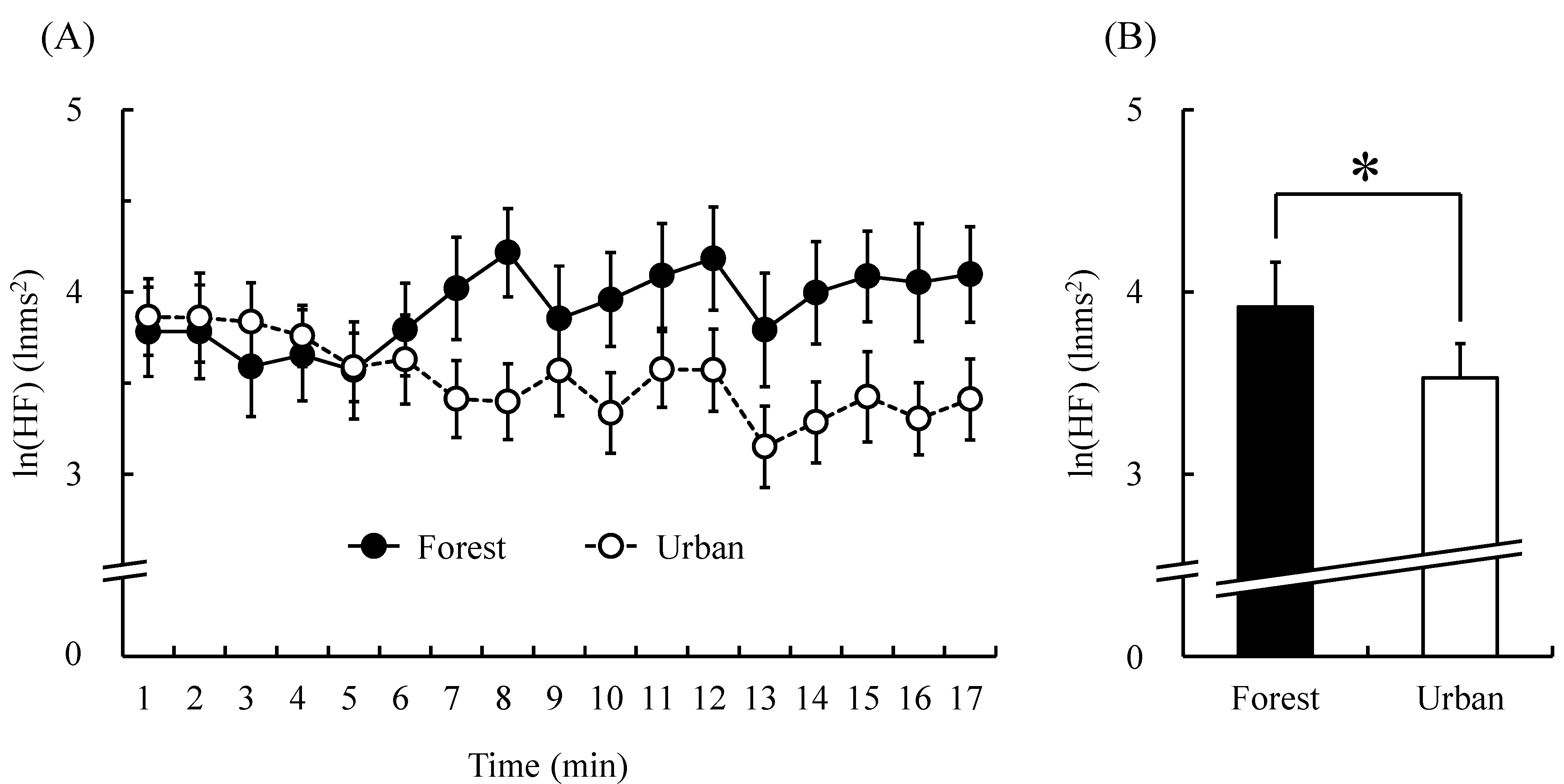
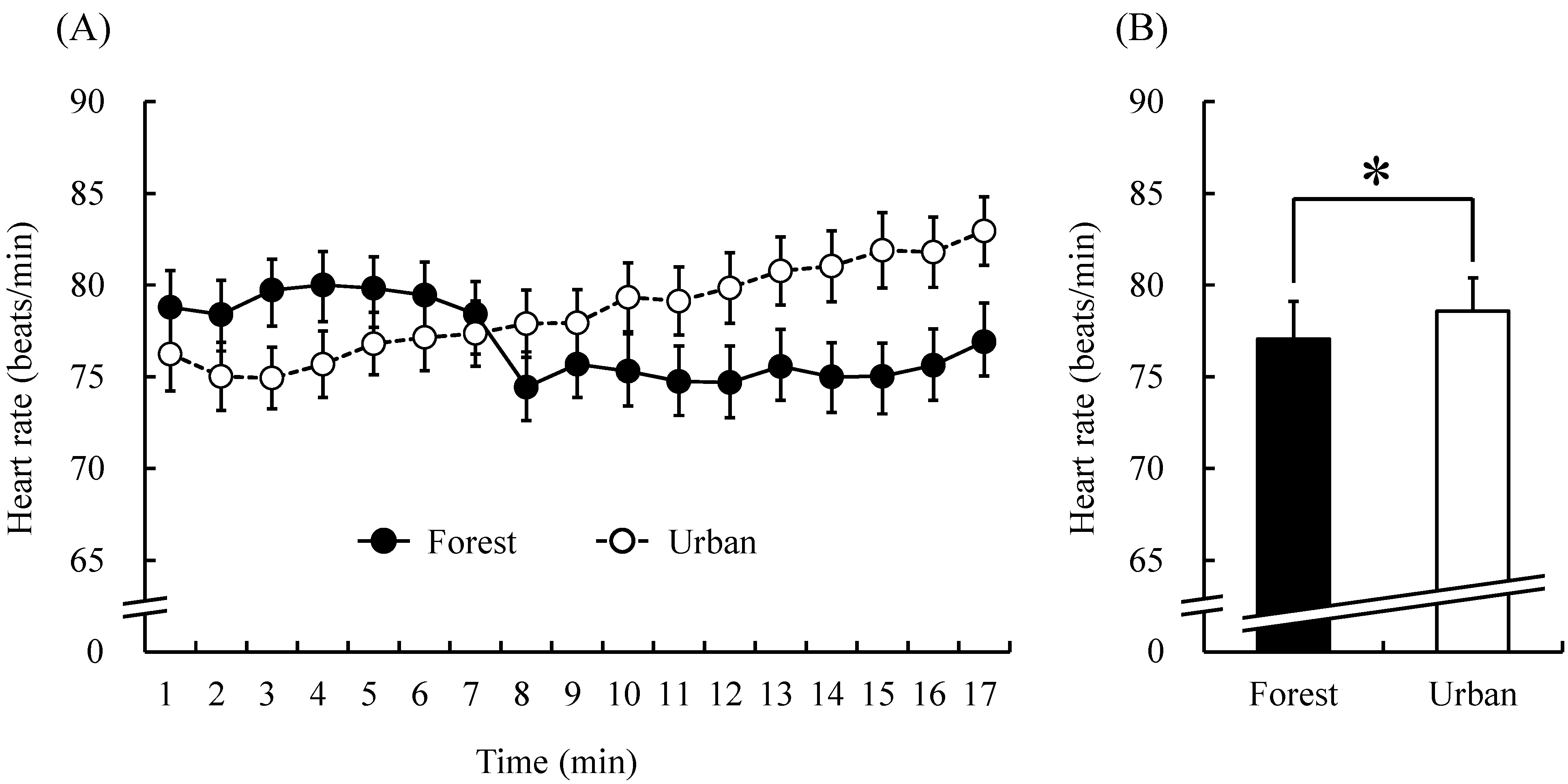
3. Results




4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brunet, M.; Guy, F.; Pilbeam, D.; Mackaye, H.T.; Likius, A.; Ahounta, D.; Beauvilain, A.; Blondel, C.; Bocherens, H.; Boisserie, J.R.; et al. A new hominid from the Upper Miocene of Chad, Central Africa. Nature 2002, 418, 141–151. [Google Scholar]
- Pronczuka, J.; Surdub, S. Children’s environmental health in the twenty-first century. N. Y. Acad. Sci. 2008, 1140, 143–154. [Google Scholar]
- Patz, J.A.; Campbell, L.D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar]
- McMichael, A.J.; Woodruff, R.E.; Hales, S. Climate change and human health: present and future risks. Lancet 2006, 367, 859–869. [Google Scholar]
- Kinney, P.L. Climate change, air quality, and human health. Amer. J. Prev. Med. 2008, 35, 459–467. [Google Scholar]
- Craig, B. Technostress: The Human Cost of the COMPUTER revolution; Addison Wesley Press: Boston, MA, USA, 1984. [Google Scholar]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar]
- Song, C.; Ikei, H.; Tsunetsugu, Y.; Lee, J.; Kagawa, T.; Miyazaki, Y. Physiological and psychological impacts of walking stress in an urban environment on young males. J. Geogr. Nat. Disast. 2013, 32. [Google Scholar] [CrossRef]
- Tanaka, A.; Takano, T.; Nakamura, K.; Takeuchi, S. Health levels influenced by urban residential conditions in a megacity—Tokyo. Urban Stud. 1996, 33, 879–894. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-Yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar]
- Tsunetsugu, Y.; Park, B.J.; Ishi, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-Yoku (taking in the atmosphere of the forest) in an oldgrowth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. Forest Res. 2009, 24, 227–234. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological effects of forest recreation in a young conifer forest in Hinokage Town, Japan. Silva Fenn. 2009, 43, 291–301. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrinyoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Ishi, H.; Furuhashi, S.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in a mixed forest in Shinano Town, Japan. Scand. J. Forest Res. 2008, 23, 278–283. [Google Scholar]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar]
- Tsunetsugu, Y.; Lee, J.; Park, B.J.; Tyrvainen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing urban forest landscapes assessed by multiple measurement. Landsc. Urban Plan. 2013, 11, 390–393. [Google Scholar]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Compl. Altern. Med. 2014, 2014. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazaki, Y.; et al. Forest bathing enhances human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2007, 20, 3–8. [Google Scholar]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.; Wakayama, Y.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regulat. Homeost. Agent. 2008, 22, 45–55. [Google Scholar]
- Park, B.J.; Furuya, K.; Kasetani, T.; Takayama, N.; Kagawa, T.; Miyazaki, Y. Relationship between psychological responses and physical environments in forest settings. Landsc. Urban Plan. 2011, 102, 24–32. [Google Scholar]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-Yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar]
- Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest experience and psychological health benefits: the state of the art and future prospect in Korea. Environ. Health Prev. Med. 2010, 15, 38–47. [Google Scholar]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S.; Kim, J.J. The influence of interaction with forest on cognitive function. Scan. J. Forest Res. 2011, 26, 595–598. [Google Scholar]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar]
- Lee, J.; Li, Q.; Tyrväinen, L.; Tsunetsugu, Y.; Park, B.J.; Kagawa, T.; Miyazaki, Y. Nature therapy and preventive medicine. In Public Health-Social and Behavioral Health; Maddock, J.R., Ed.; InTech: Rijeka, Croatia, 2012; pp. 325–350. [Google Scholar]
- Frumkin, H. Beyond toxicity: human health and the natural environment. Amer. J. Prev. Med. 2001, 20, 234–240. [Google Scholar]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar]
- Ohtsuka, Y.; Yabunaka, N.; Takayama, S. Shinrin-Yoku (forest-air bathing and walking) effectively decreases blood glucose levels in diabetic patients. Int. J. Biometeorol. 1998, 41, 125–127. [Google Scholar]
- Kim, W.; Lim, S.K.; Chung, E.J.; Woo, J.M. The effect of cognitive behavior therapy-based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiat. Investig. 2009, 6, 245–254. [Google Scholar]
- Mao, G.X.; Cao, Y.B.; Lan, X.G.; He, Z.H.; Chen, Z.M.; Wang, Y.Z.; Hu, X.L.; Lv, Y.D.; Wang, G.F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar]
- Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “Forest Therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar]
- Task force of the European society of cardiology and the north american society of pacing and electrophysiology: Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065.
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar]
- Kanaya, N.; Hirata, N.; Kurosawa, S.; Nakayama, M.; Namiki, A. Differential effects of propofol and sevoflurane on heart rate variability. Anesthesiology 2003, 98, 34–40. [Google Scholar]
- Kobayashi, H.; Park, B.J.; Miyazaki, Y. Normative references of heart rate variability and salivary alpha-amylase in a healthy young male population. J. Physiol. Anthropol. 2012, 31. [Google Scholar] [CrossRef]
- Osgood, C.E.; Suci, G.J.; Tannenbaum, P. The Measurement of Meaning; University of Illinois Press: Urbana, IL, USA, 1957. [Google Scholar]
- McNair, D.; Lorr, M. An analysis of mood in neurotics. J. Abnorm. Soc. Psych. 1964, 69, 620–627. [Google Scholar]
- McNair, D.; Lorr, M.; Droppleman, L. Profile of Mood States Manual; Educational and Industrial Testing Services: San Diego, CA, USA, 1992. [Google Scholar]
- Yokoyama, K. POMS Shortened Version-Manual and Commentary on Cases; Kaneko Syoboh: Tokyo, Japan, 2005. [Google Scholar]
- Delaney, J.P.; Leong, K.S.; Watkins, A.; Brodie, D. The short-term effects of myofascial trigger point massage therapy on cardiac autonomic tone in healthy subjects. J. Adv. Nurs. 2002, 3, 7364–7371. [Google Scholar]
- Buttagat, V.; Eungpinichpong, W.; Chatchawan, U.; Kharmwan, S. The immediate effects of traditional Thai massage on heart rate variability and stress-related parameters in patients with back pain associated with myofascial trigger points. J. Bodyw. Mov. Ther. 2011, 15, 15–23. [Google Scholar]
- Shapiro, D.; Cook, I.A.; Davydov, D.M.; Ottaviani, C.; Leuchter, A.F.; Abrams, M. Yoga as complementary of depression: Effects of traits and moods on treatment outcome. Evid. Based Compl. Alternat. Med. 2007, 4, 493–502. [Google Scholar]
- Perrey, S.; Fabre, N. Exertion during uphill, level and downhill walking with and without hiking poles. J. Sports Sci. Med. 2008, 7, 32–38. [Google Scholar]
- Minetti, A.E.; Moia, C.; Roi, G.S.; Susta, D.; Ferretti, G. Energy cost of walking and running at extreme uphill and downhill slopes. J. Appl. Physiol. 1985, 93, 1039–1046. [Google Scholar]
- Padulo, J.; Annino, G.; Tihanyi, J.; Calcagno, G.; Vando, S.; Smith, L.; Vernillo, G.; La Torre, A.; Dʼottavio, S. Uphill racewalking at iso-efficiency speed. J. Strength Cond. Res. 2013, 27, 1964–1973. [Google Scholar]
- Murray, C.J.L.; Lopez, A.D. Evidence-based health policy—Lessons from the global burden of disease study. Science 1996, 274, 740–743. [Google Scholar]
- Iwane, M.; Arita, M.; Tomimoto, S.; Satani, O.; Matsumoto, M.; Miyashita, K.; Nishio, I. Walking 10,000 steps/day or more reduces blood pressure and sympathetic nerve activity in mild essential hypertension. Hypertens. Res. 2000, 23, 573–580. [Google Scholar]
- Williams, P.T.; Thompson, P.D. Walking versus running for hypertension, cholesterol, and diabetes mellitus risk reduction. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1085–1091. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study. Int. J. Environ. Res. Public Health 2015, 12, 2687-2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120302687
Song C, Ikei H, Kobayashi M, Miura T, Taue M, Kagawa T, Li Q, Kumeda S, Imai M, Miyazaki Y. Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study. International Journal of Environmental Research and Public Health. 2015; 12(3):2687-2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120302687
Chicago/Turabian StyleSong, Chorong, Harumi Ikei, Maiko Kobayashi, Takashi Miura, Masao Taue, Takahide Kagawa, Qing Li, Shigeyoshi Kumeda, Michiko Imai, and Yoshifumi Miyazaki. 2015. "Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study" International Journal of Environmental Research and Public Health 12, no. 3: 2687-2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120302687