
The Impact of Ambient Temperature on Childhood HFMD Incidence in Inland and Coastal Area: A Two-City Study in Shandong Province, China

Abstract
:1. Introduction

2. Materials and Methods
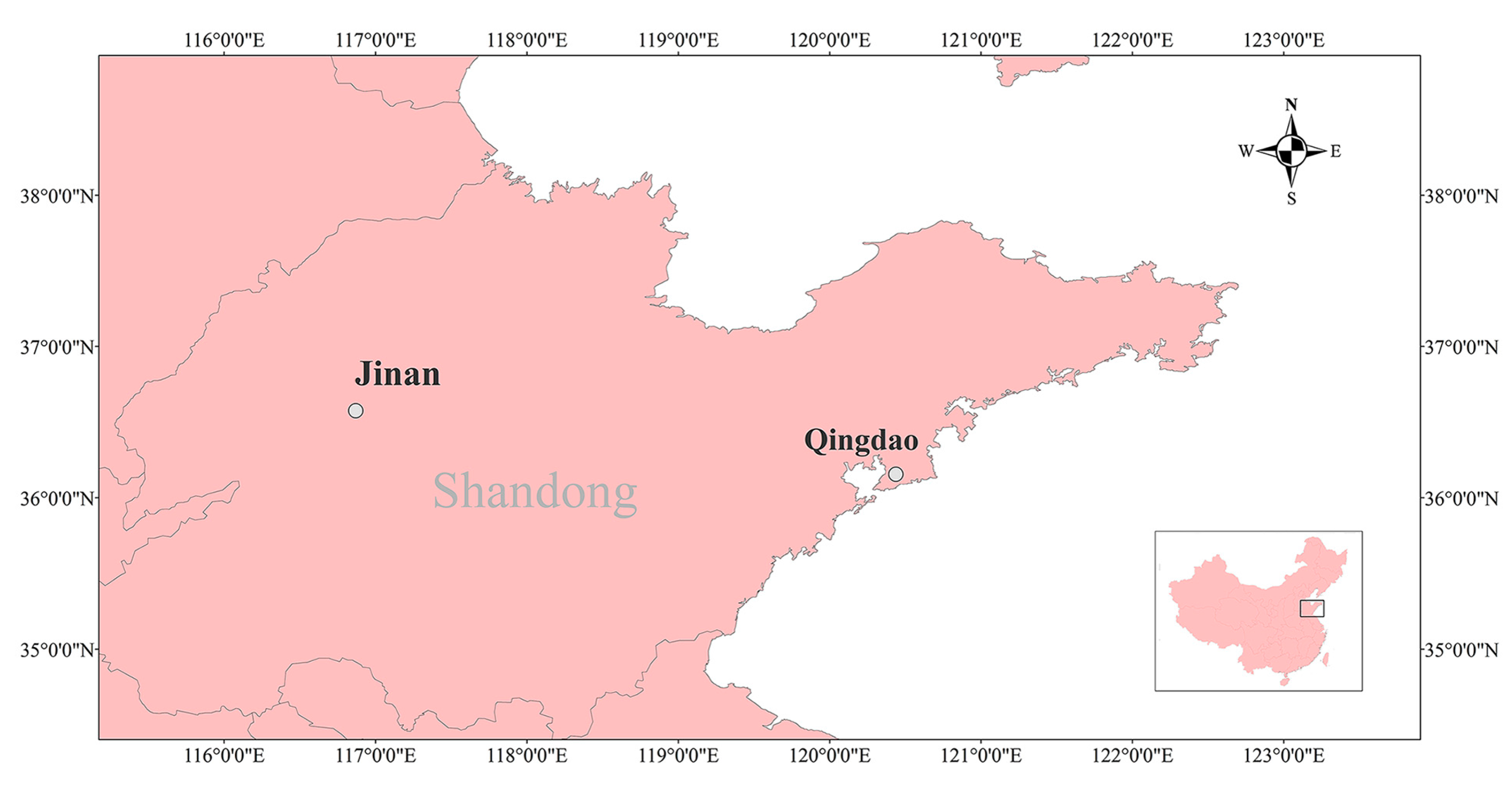
2.1. Data Collection
2.2. Statistical Analysis
NS(Time,7/year) + γDowt + vHolidayt ,
3. Results
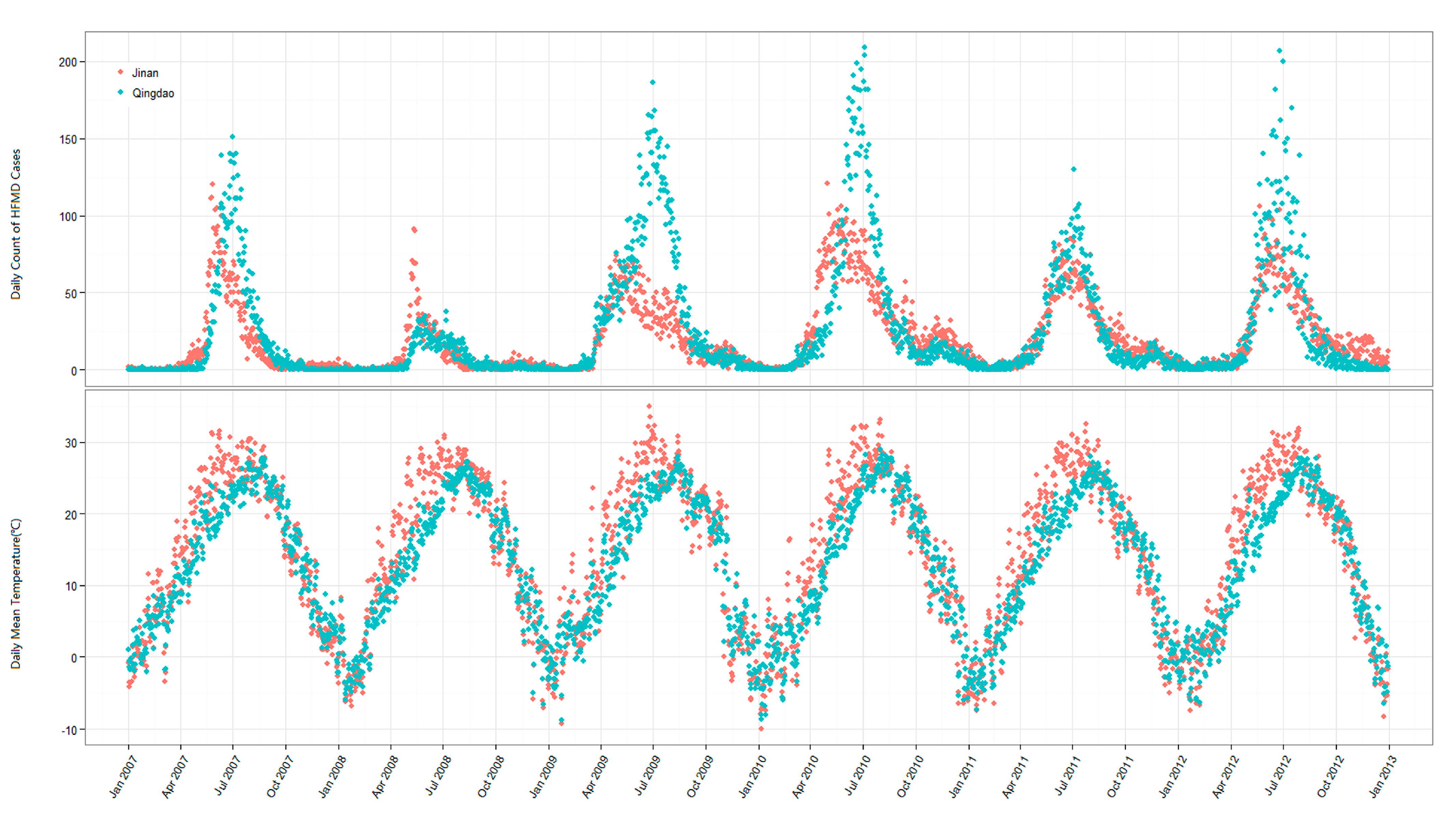
3.1. Descriptive Statistics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Cases | Jinan | Qingdao |
| 47,705 | 60,672 | |
| Age | ||
| 0–5 years | 44,573 (93.4%) | 55,176 (91.0%) |
| >5 years | 3132 (6.6%) | 5496 (9.0%) |
| Sex (0–5 years) | ||
| Male | 26,967 (60.5%) | 33,989 (61.6%) |
| Female | 17,606 (39.5%) | 21,187 (38.4%) |
| Pathogen (0–5 years) | ||
| Cox A16 | 699 (36.6%) | 330 (27.4%) |
| EV71 | 830 (43.5%) | 375 (31.1%) |
| Other EV | 380 (19.9%) | 501 (43.2%) |
| Meteorological Variables | ||
| Mean Temp (°C) | ||
| Mean ± SD | 14.5 ± 10.6 | 13.0 ± 9.3 |
| Min. | −10.0 | −8.8 |
| Median | 16.3 | 13.1 |
| Max. | 35.0 | 29.0 |
| Mean Relative Humidity (%) | ||
| Mean ± SD | 56.0 ± 20.7 | 69.9 ± 17.3 |
| Min. | 13.0 | 22.0 |
| Median | 55.0 | 71 |
| Max. | 100.0 | 100 |
| Rainfall (mm) | ||
| Mean ± SD | 2.0 ± 8.1 | 2.3 ± 10.7 |
| Min. | 0 | 0 |
| Median | 0 | 0 |
| Max. | 143.8 | 241.2 |
| Sunshine Duration (h) | ||
| Mean ± SD | 5.7 ± 3.9 | 5.9 ± 3.9 |
| Min. | 0 | 0 |
| Median | 6.5 | 6.9 |
| Max. | 13.5 | 12.8 |

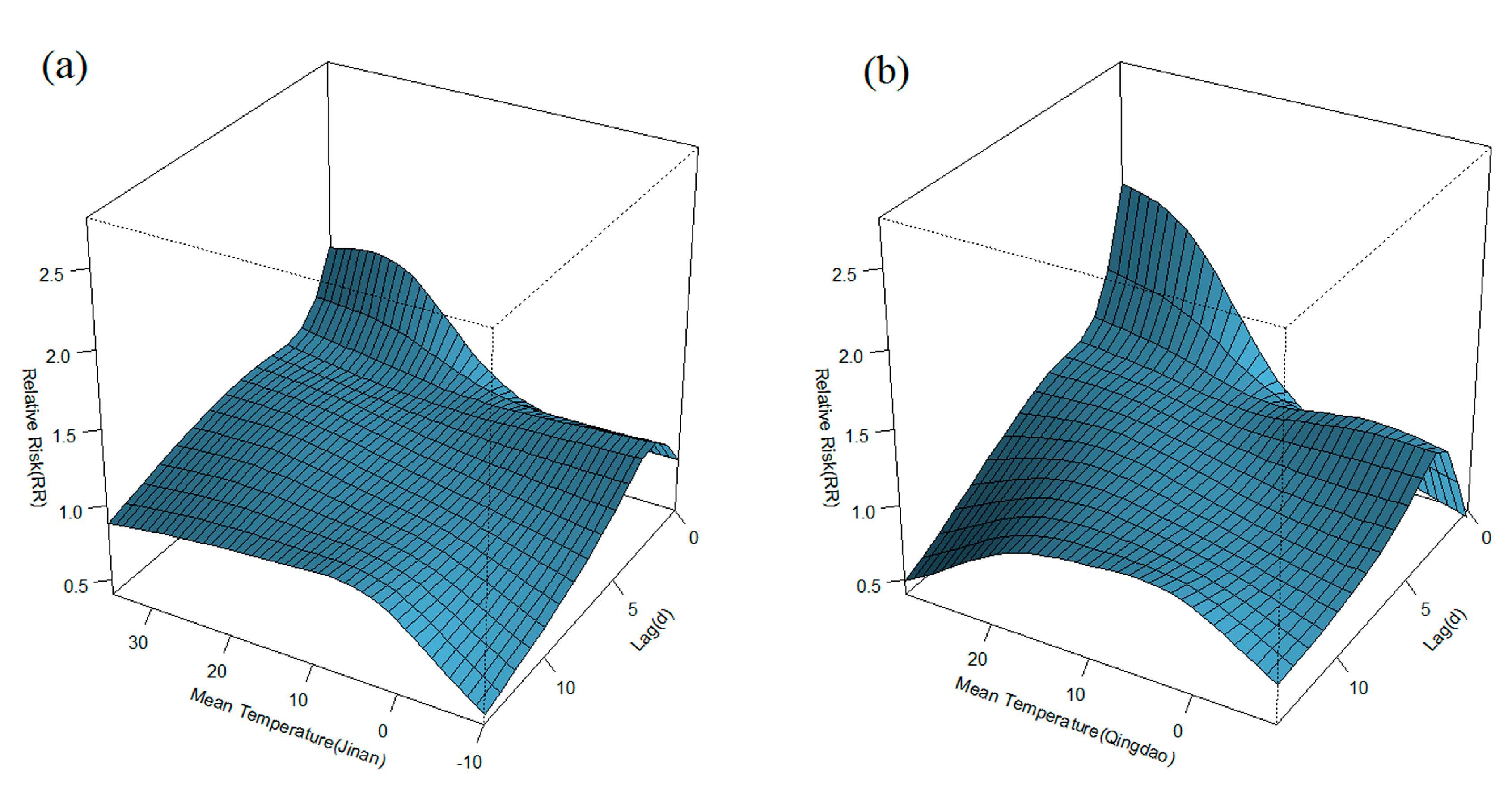
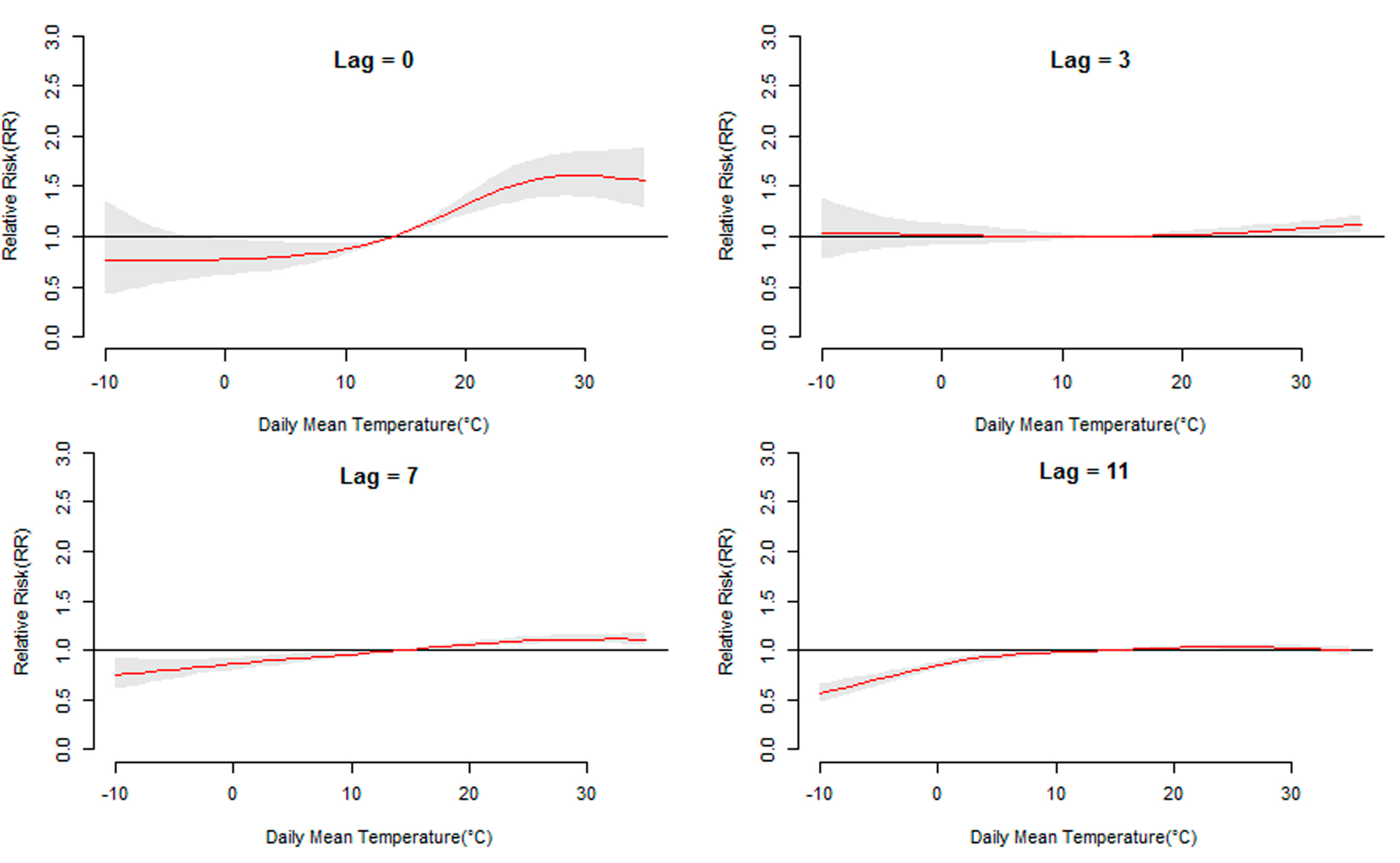
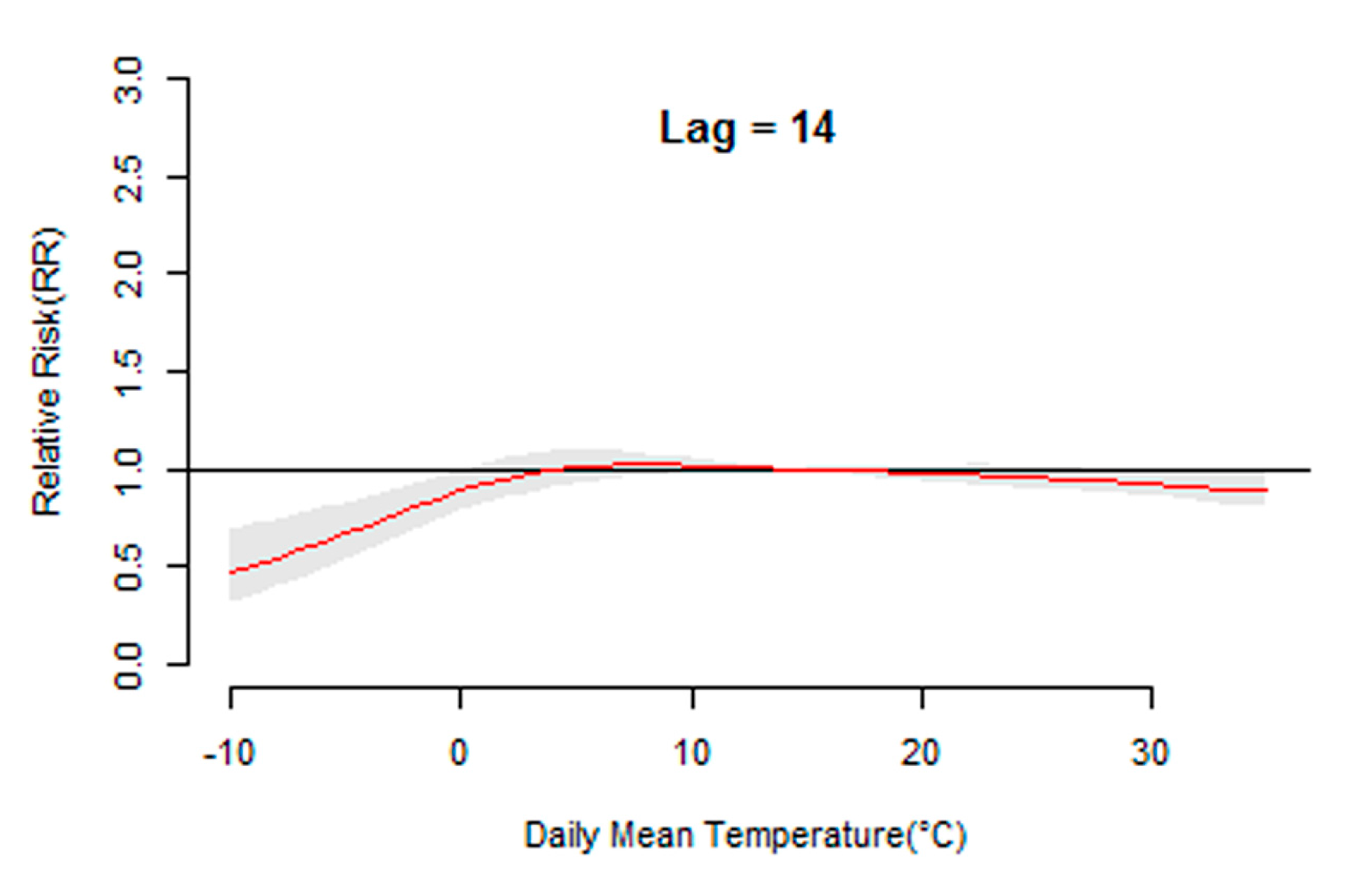
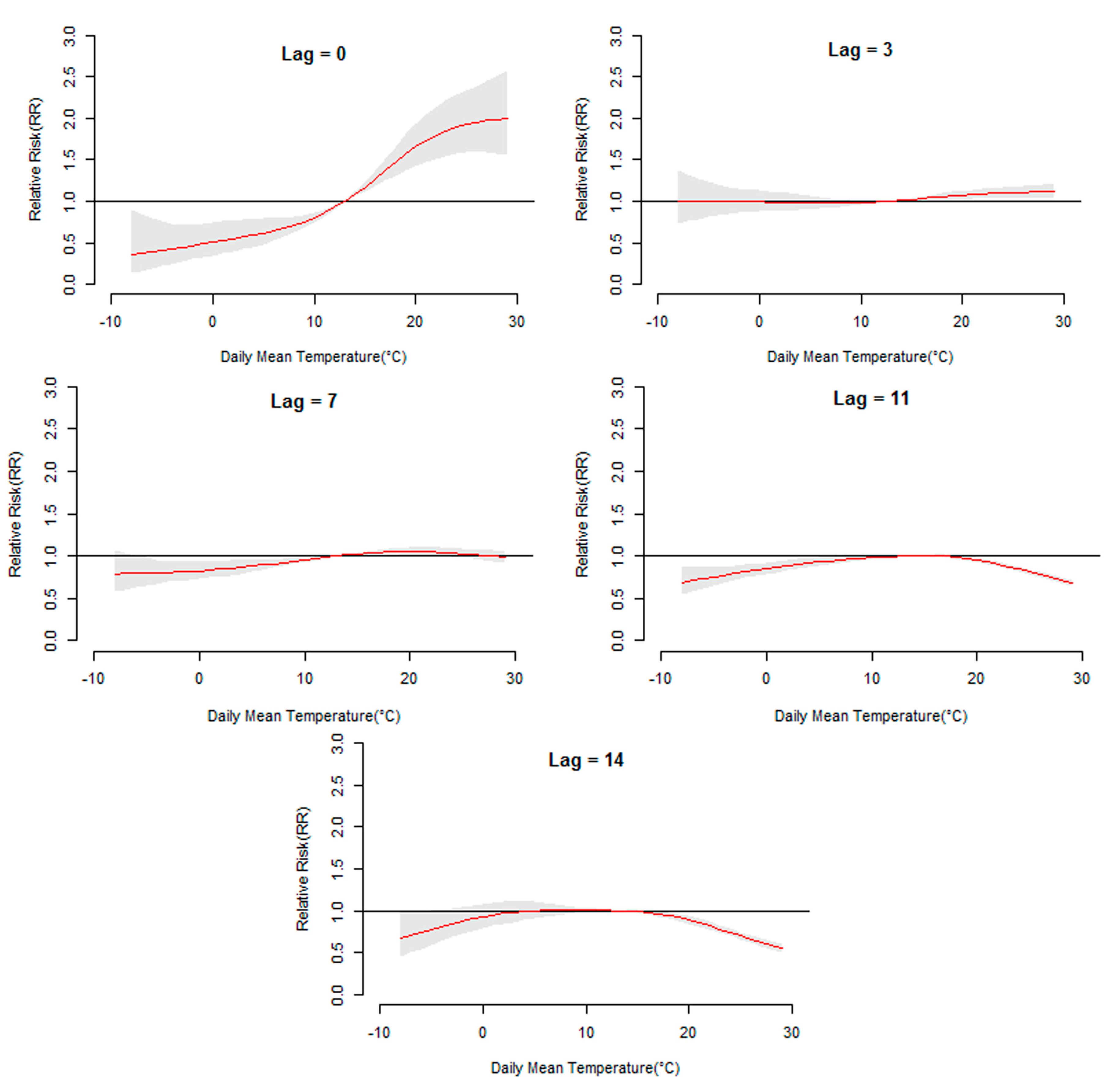
3.2. Temperature Lag–HFMD Incidence Association




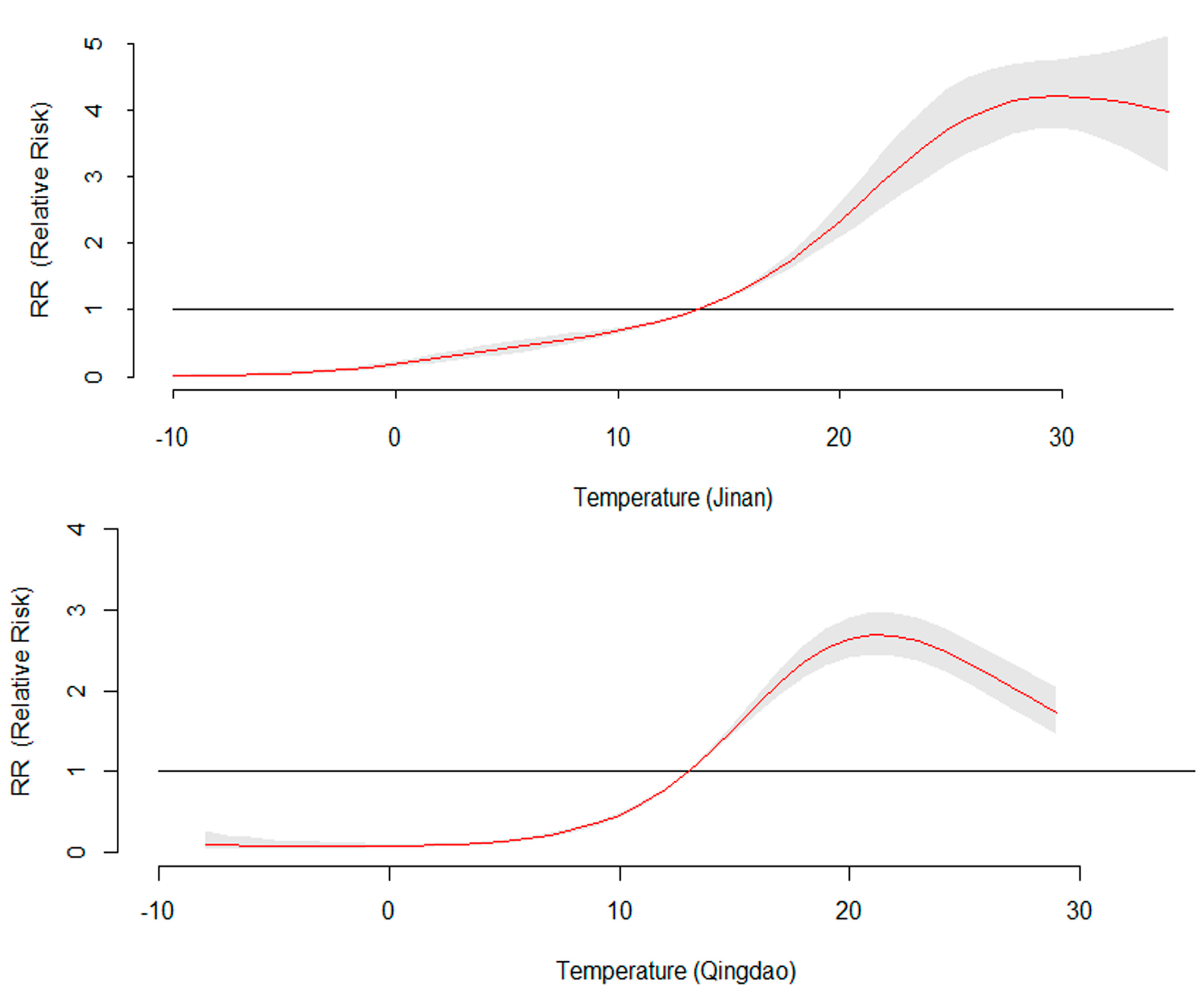
3.3. The 14-Day Cumulative RR for Daily Mean Temperature

3.4. Heterogeneity Analysis
| Coefficients | Jinan | Qingdao | p |
|---|---|---|---|
| constant | −0.0613 | −0.2727 | 0.0826 |
| linear term | 0.0336 | 0.0271 | 0.6777 |
| quadratic term | 0.0066 | 0.0149 | <0.0001 * |
| cubic term | −0.0001 | −0.0004 | <0.0001 * |
| R2 | 96.89% | 93.41% |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Xing, W.; Liao, Q.; Viboud, C.; Zhang, J.; Sun, J.; Wu, J.T.; Chang, Z.; Liu, F.; Fang, V.J.; Zheng, Y.; Cowling, B.J.; Varma, J.K.; Farrar, J.J.; Leung, G.M.; Yu, H. Hand, foot, and mouth disease in China, 2008–12: An epidemiological study. Lancet Infect. Dis. 2014, 14, 308–318. [Google Scholar] [CrossRef]
- Gopalkrishna, V.; Patil, P.R.; Patil, G.P.; Chitambar, S.D. Circulation of multiple enterovirus serotypes causing hand, foot and mouth disease in India. J. Med. Microbiol. 2012, 61, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Goksugur, N.; Goksugur, S. Hand, Foot, and Mouth Disease. New Engl. J. Med. 2010, 362. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.H.; Wong, S.C.; Lewthwaite, P.; Cardosa, M.J.; Solomon, T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010, 9, 1097–1105. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.; Liu, Y.; Sun, D.; Ding, S.; Zhang, B.; Du, Z.; Xue, F. Detecting spatial-temporal clusters of HFMD from 2007 to 2011 in Shandong Province, China. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Chan, K.C.; Cheng, P.; Wong, C.; Chuang, S.K. The enterovirus 71 epidemic in 2008—Public health implications for Hong Kong. Int. J. Infect. Dis. 2010, 14, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, K.; Lye, M.S.; Norlijah, O.; Ong, F.; Looi, L.M.; Khuzaiah, R.; Marzuki, I.; Hussein, I.; Wong, S.L.; Mohan, J.; Sinniah, M.; Abu Bakar, S. Deaths in children during an outbreak of hand, foot and mouth disease in Peninsular Malaysia—Clinical and pathological characteristics. Med. J. Malaysia 2005, 60, 297–304. [Google Scholar] [PubMed]
- Taniguchi, K.; Hashimoto, S.; Kawado, M.; Murakami, Y.; Izumida, M.; Ohta, A.; Tada, Y.; Shigematsu, M.; Yasui, Y.; Nagai, M. Overview of infectious disease surveillance system in Japan, 1999–2005. J. Epidemiol. 2007, 17, 3–13. [Google Scholar] [CrossRef]
- Ho, M.; Chen, E.R.; Hsu, K.H.; Twu, S.J.; Chen, K.T.; Tsai, S.F.; Wang, J.R.; Shih, S.R. An epidemic of enterovirus 71 infection in Taiwan. Taiwan Enterovirus Epidemic Working Group. New Engl. J. Med. 1999, 341, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, P.E.; Landrigan, P.J. Global climate change and children’s health: Threats and strategies for prevention. Environ. Health Persp. 2011, 119, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Loughnan, M.; Nicholls, N.; Tapper, N. Mortality-temperature thresholds for ten major population centres in rural Victoria, Australia. Health Place 2010, 16, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Rao, Y.; Wu, X.; Zhao, H.; Chen, J. A Method for Screening Climate Change-Sensitive Infectious Diseases. Int. J. Environ. Res. Public Health 2015, 12, 767–783. [Google Scholar] [CrossRef] [PubMed]
- Onozuka, D.; Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. 2011, 410, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Shindo, N.; Okabe, N. Seasonal models of herpangina and hand-foot-mouth disease to simulate annual fluctuations in urban warming in Tokyo. Jpn. J. Infect. Dis. 2003, 56, 48–53. [Google Scholar] [PubMed]
- Ma, E.; Lam, T.; Wong, C.; Chuang, S.K. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol. Infect. 2010, 138, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Deng, T.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: A time-series analysis in Guangzhou, China. BMC Infect. Dis. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Hii, Y.L.; Rocklöv, J.; Ng, N. Short term effects of weather on Hand, foot and mouth disease. PLoS ONE 2011, 6, 1435–1439. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Hansen, A.; Liu, Q.; Sun, Y.; Weinstein, P.; Bi, P. The Effect of Meteorological Variables on the Transmission of Hand, Foot and Mouth Disease in Four Major Cities of Shanxi Province, China: A Time Series Data Analysis (2009–2013). PLoS Neglect. Trop Dis. 2015, 9. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Yu, W.; Tong, S.; Jia, L.; Liang, F.; Pan, X. Non-Linear Association between Exposure to Ambient Temperature and Children’s Hand-Foot-and-Mouth Disease in Beijing, China. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Chinese Ministry of Health Hand, Foot and Mouth Disease Control. and Prevention Guide, 2009. Available online: http://www.chinacdc.cn/jkzt/crb/szkb/jszl_2275/200906/t20090612_24707.htm (accessed on 21 June 2015).
- Gasparrini, A. Modeling exposure-lag-response associations with distributed lag non-linear models. Stat. Med. 2014, 33, 881–899. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Multivariate meta-analysis for non-linear and other multi-parameter associations. 2012, 31, 3821–3839. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [PubMed]
- Xu, Z.; Liu, Y.; Ma, Z.; Sam Toloo, G.; Hu, W.; Tong, S. Assessment of the temperature effect on childhood diarrhea using satellite imagery. Sci. Rep. 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, S.; Pan, X.; Tong, S.; Jaakkola, J.J.; Gasparrini, A.; Guo, Y.; Wang, S. The effects of ambient temperature on cerebrovascular mortality: an epidemiologic study in four climatic zones in China. Environ. Health 2014, 13, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Wu, J.; Xu, Z.; Zhu, R.; Wang, X. Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China. Sci. Total Environ. 2014, 497, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Beier, J.C.; Cantrell, R.S.; Cosner, C.; DeAngelis, D.L.; Ruan, S. Modelling the Effects of Seasonality and Socioeconomic Impact on the Transmission of Rift Valley Fever Virus. PLoS Negl. Trop Dis. 2015, 9. [Google Scholar] [CrossRef] [PubMed]
- Leckebusch, G.C.; Abdussalam, A.F. Climate and socioeconomic influences on interannual variability of cholera in Nigeria. Health Place 2015, 34, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Khasnis, A.A.; Nettleman, M.D. Global warming and infectious disease. Arch. Med. Res. 2005, 36, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Etzel, R.A.; Su, H.; Huang, C.; Guo, Y.; Tong, S. Impact of ambient temperature on children’s health: a systematic review. Environ. Res. 2012, 117, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. Time series analysis on the health effects of temperature: Advancements and limitations. Environ. Res. 2010, 110, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Yeager, J.G.; O’Brien, R.T. Enterovirus inactivation in soil. Appl. Environ. Microbiol. 1979, 38, 694–701. [Google Scholar] [PubMed]
- Bélanger, M.; Gray-Donald, K.; O’loughlin, J.; Paradis, G.; Hanley, J. Influence of Weather Conditions and Season on Physical Activity in Adolescents. Ann. Epidemiol. 2009, 19, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Suminski, R.R.; Poston, W.C.; Market, P.; Hyder, M.; Sara, P.A. Meteorological conditions are associated with physical activities performed in open-air settings. Int. J. Biometeorol. 2008, 52, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Smith, B.; Stoker, L.; Bellew, B.; Booth, M. Geographical influences upon physical activity participation: Evidence of a “coastal effect.”. Aust. NZ. J. Publ. Heal. 1999, 23, 322–324. [Google Scholar] [CrossRef]
- Rajtar, B.; Majek, M.; Polański, L.; Polz-Dacewicz, M. Enterovirus in water environment—A potential threat to public health. Ann. Agr. Env. Med. 2008, 15, 199–203. [Google Scholar]
- Pica, N.; Bouvier, N.M. Ambient temperature and respiratory virus infection. Pediatr. Infect. Dis. J. 2014, 33, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, N.; Ma, W.; Gao, Y.; Yang, S. Hand, foot, and mouth disease in mainland China. Lancet Infect. Dis. 2014, 14. [Google Scholar] [CrossRef]
- Mao, Q.; Wang, Y.; Liang, Z. Hand , foot , and mouth disease in mainland China. Lancet Infect. Dis. 2014, 14. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, L.; Yuan, Z.; Wang, X.; Li, J.; Wang, L.; Liu, Y.; Xue, F.; Liu, Y. The Impact of Ambient Temperature on Childhood HFMD Incidence in Inland and Coastal Area: A Two-City Study in Shandong Province, China. Int. J. Environ. Res. Public Health 2015, 12, 8691-8704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120808691
Zhu L, Yuan Z, Wang X, Li J, Wang L, Liu Y, Xue F, Liu Y. The Impact of Ambient Temperature on Childhood HFMD Incidence in Inland and Coastal Area: A Two-City Study in Shandong Province, China. International Journal of Environmental Research and Public Health. 2015; 12(8):8691-8704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120808691
Chicago/Turabian StyleZhu, Lin, Zhongshang Yuan, Xianjun Wang, Jie Li, Lu Wang, Yunxia Liu, Fuzhong Xue, and Yanxun Liu. 2015. "The Impact of Ambient Temperature on Childhood HFMD Incidence in Inland and Coastal Area: A Two-City Study in Shandong Province, China" International Journal of Environmental Research and Public Health 12, no. 8: 8691-8704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120808691