
Superior Effects of Antiretroviral Treatment among Men Who have Sex with Men Compared to Other HIV At-Risk Populations in a Large Cohort Study in Hunan, China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Clinical Laboratory Testing at Baseline
2.3. Disease Progression Indicators
- (1)
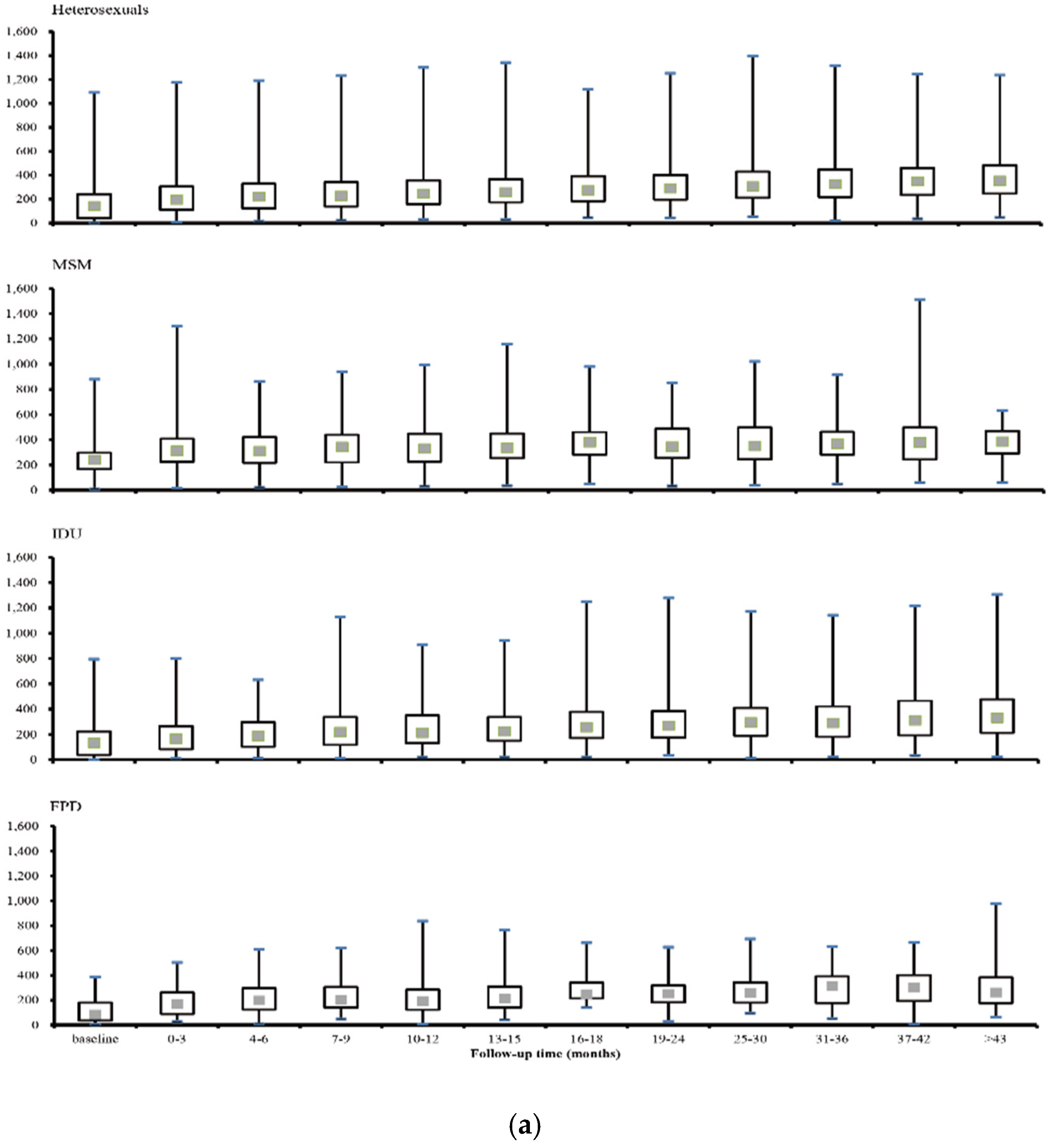
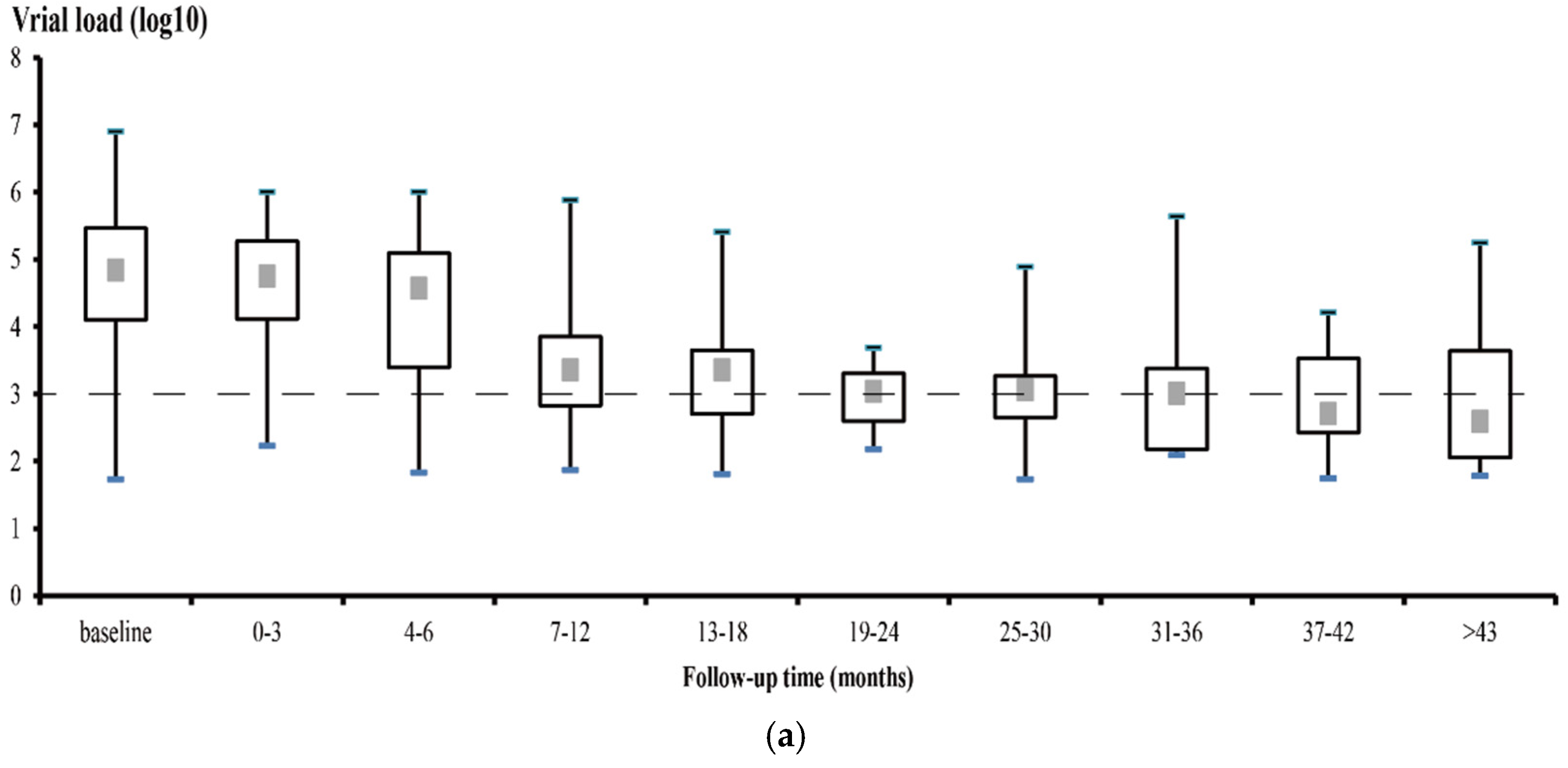
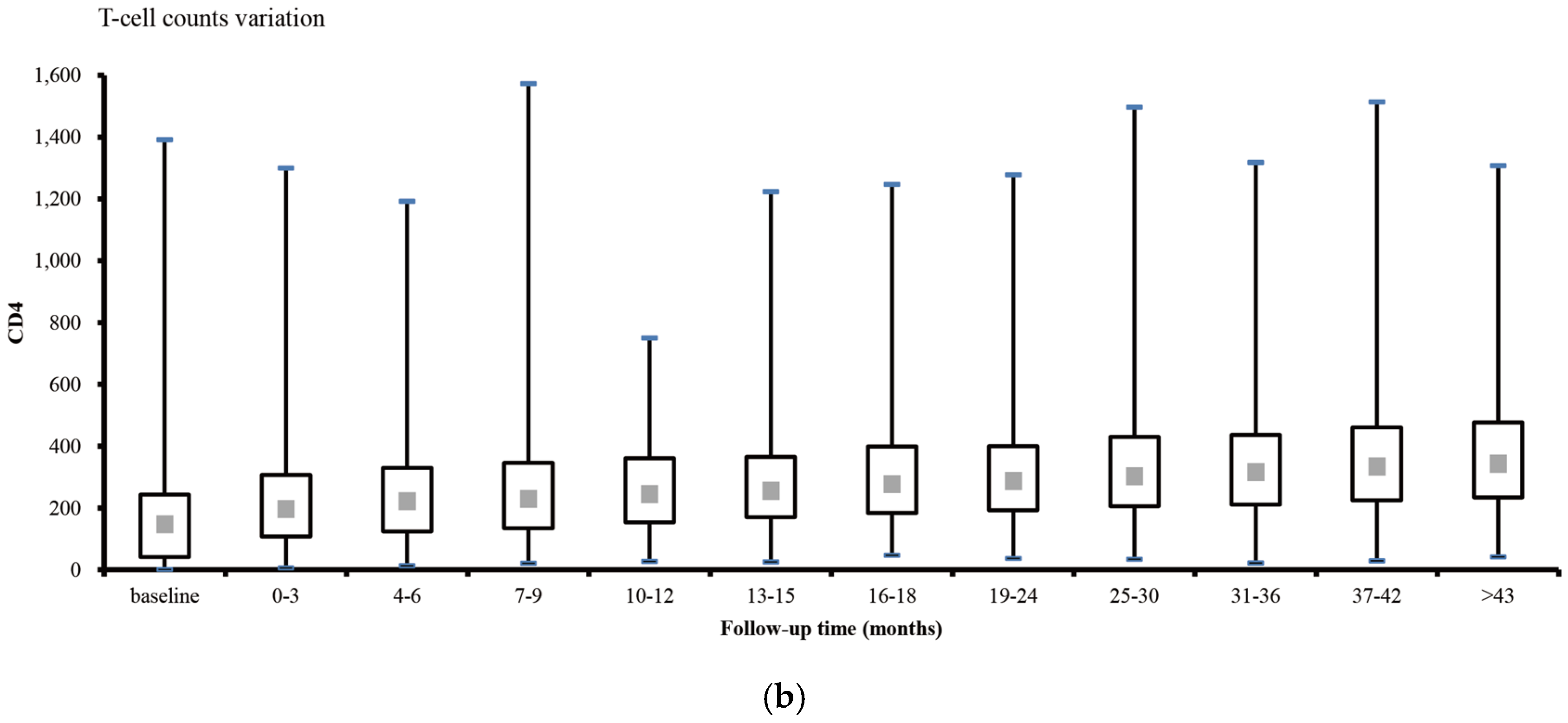
- CD4 and HIV viral levels. The median with interquartile range (IQR) of CD4 counts and viral load were calculated every three months in the first year then every six months over the remaining course of follow-up.
- (2)
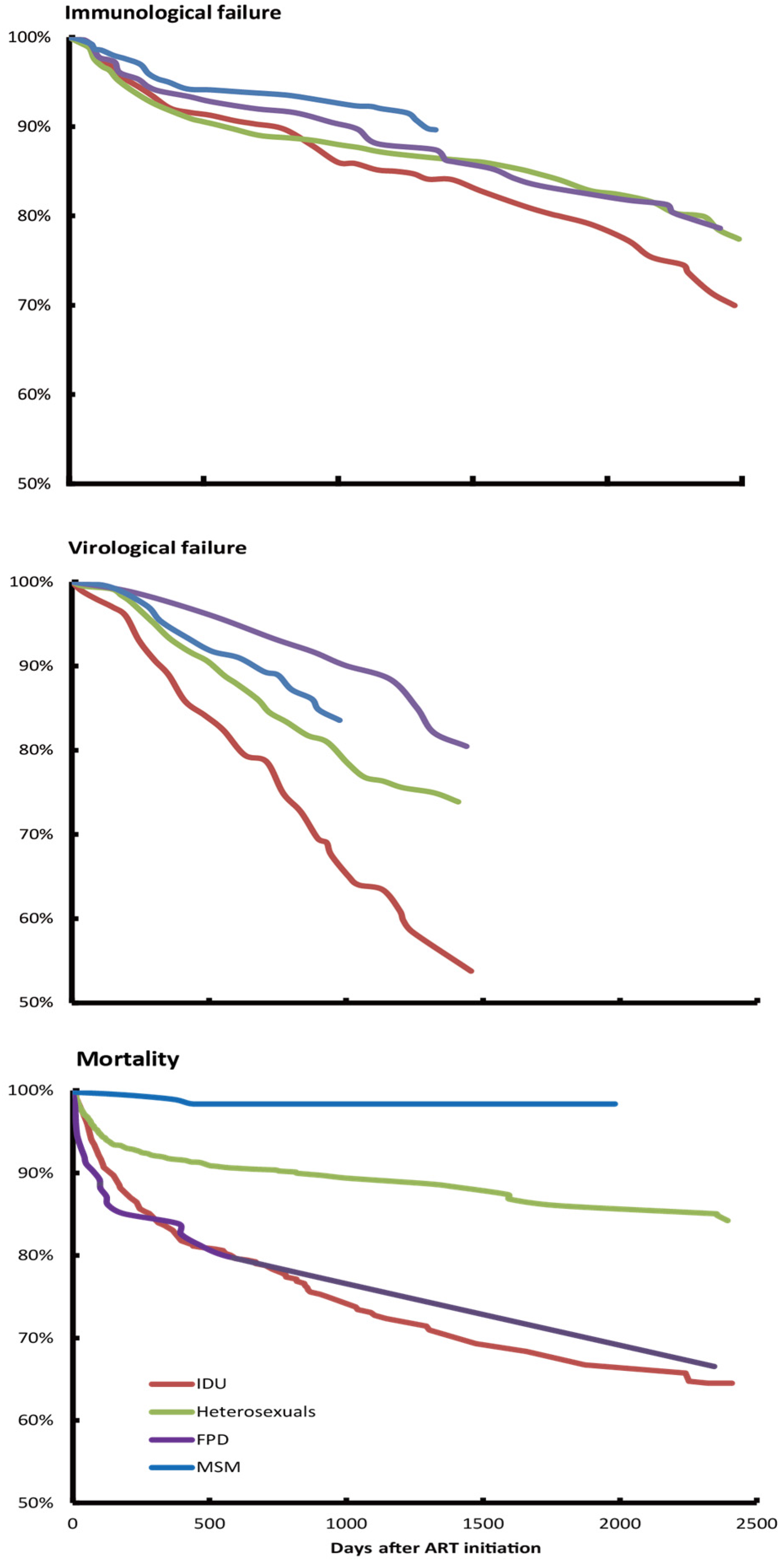
- Treatment failure (including both immunological and virological failure). Immunological failure was defined as CD4 Cell count of the patient fell below 100 cells/mm3 after receiving ART for three months without a concomitant diseases that may sharply decrease the CD4 counts [27]; virological failure was defined as plasma viral load above 1000 copies/mL based on two consecutive viral load measurements after 3 months of treatment [28].
- (3)
- HIV-related mortality. All death cases were recorded until the end of the study (December 2013). Mortality was compared across different CD4 count strata and transmission route categories. Factors associated with mortality were identified with Cox regression.
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Result
3.1. Demographic Characteristics and CD4 Level at Baseline
3.2. Trend of CD4 and Viral Load Level
3.3. Treatment Failures among ART Patients
3.4. Mortality during Treatment
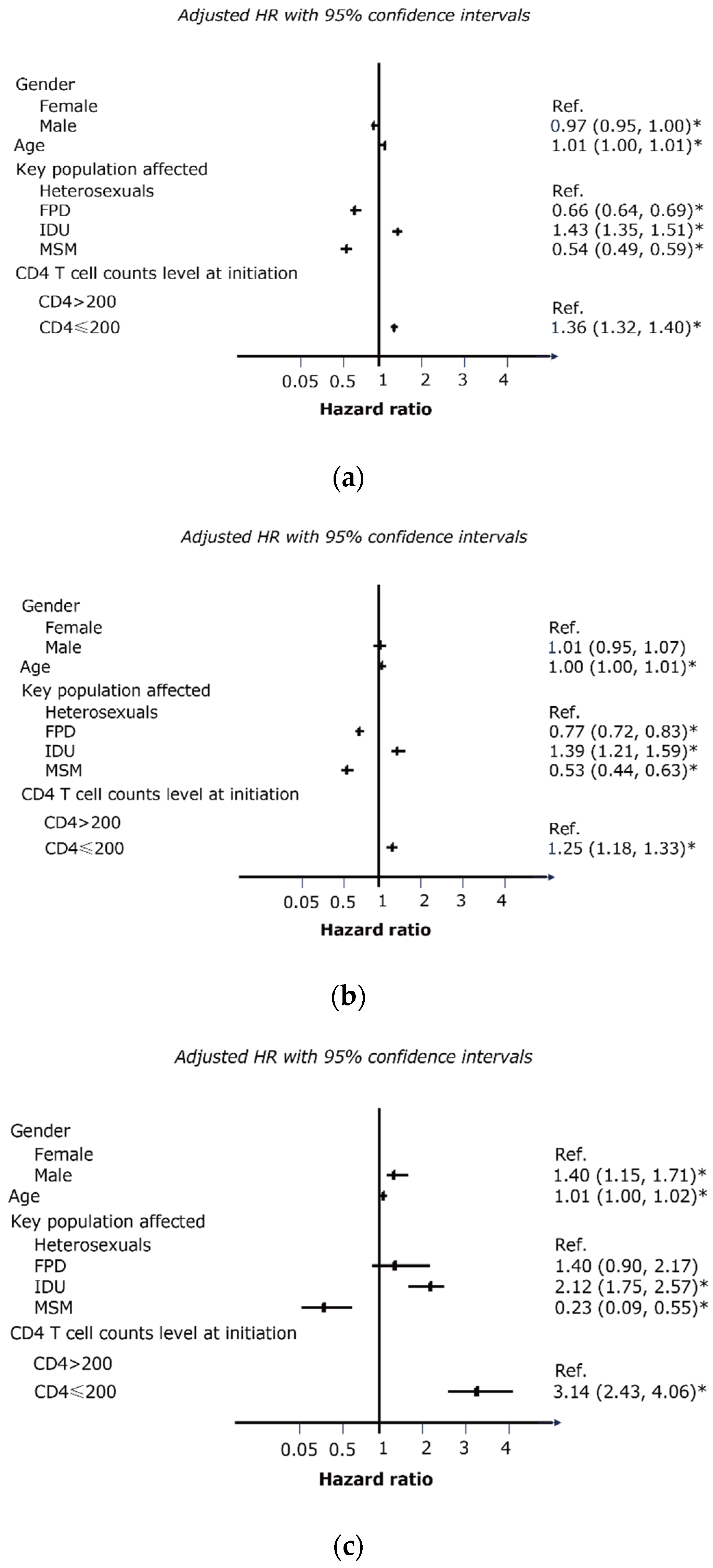
3.5. Significant Factors Associated with Treatment Failure and Mortality
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A


References
- Thompson, M.A.; Aberg, J.A.; Cahn, P.; Montaner, J.S.; Rizzardini, G.; Telenti, A.; Benson, C.; Cahn, P.; Eron, J.J.; Günthard, H.F.; et al. Antiretroviral treatment of adult HIV infection: 2010 Recommendations of the international AIDS society-USA panel. JAMA 2010, 304, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Hammer, S.M.; Squires, K.E.; Hughes, M.D.; Grimes, J.M.; Demeter, L.M.; Currier, J.S.; Eron, J.J., Jr.; Feinberg, J.E.; Balfour, H.H., Jr.; Deyton, L.R.; et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency vs. infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS Clinical Trials Group 320 Study Team. N. Engl. J. Med. 1997, 337, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.S.; Lima, V.D.; Harrigan, P.R.; Lourenco, L.; Yip, B.; Nosyk, B.; Wood, E.; Kerr, T.; Shannon, K.; Moore, D.; et al. Expansion of HAART coverage is associated with sustained decreases in HIV/AIDS morbidity, mortality and HIV transmission: The “HIV Treatment as Prevention” experience in a Canadian setting. PLoS ONE 2014, 9, e87872. [Google Scholar] [CrossRef] [PubMed]
- Paquette, D.; Schanzer, D.; Guo, H.; Gale-Rowe, M.; Wong, T. The impact of HIV treatment as prevention in the presence of other prevention strategies: Lessons learned from a review of mathematical models set in resource-rich countries. Prev. Med. 2014, 58, 1–8. [Google Scholar] [CrossRef] [PubMed]
- National Center for AIDS/STD Control and Prevention, China CDC (NCAIDS). Panel on National Free ART Manual; People’s Medical Publishing House: Beijing, China, 2005. [Google Scholar]
- Wu, Z.; Sullivan, S.G.; Wang, Y.; Rotheram-Borus, M.J.; Detels, R. Evolution of China’s response to HIV/AIDS. Lancet 2007, 369, 679–690. [Google Scholar] [CrossRef]
- National Center for AIDS/STD Control and Prevention, China CDC (NCAIDS). Panel on National Free ART Manual; People’s Medical Publishing House: Beijing, China, 2008. [Google Scholar]
- Kranzer, K.; Lawn, S.D.; Johnson, L.F.; Bekker, L.G.; Wood, R. Community viral load and CD4 count distribution among people living with HIV in a South African Township: Implications for treatment as prevention. J. Acquir. Immune Defic. Syndr. 2013, 63, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Anglemyer, A.; Rutherford, G.W.; Easterbrook, P.J.; Horvath, T.; Vitoria, M.; Jan, M.; Doherty, M.C. Early initiation of antiretroviral therapy in HIV-infected adults and adolescents: A systematic review. AIDS 2014, 28, S105–S118. [Google Scholar] [CrossRef] [PubMed]
- Abay, S.M.; Deribe, K.; Reda, A.A.; Biadgilign, S.; Datiko, D.; Assefa, T.; Todd, M.; Deribew, A. The effect of early initiation of antiretroviral therapy in TB/HIV-coinfected patients: A systematic review and meta-analysis. J. Int. Assoc. Provid. AIDS Care 2015, 14, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Chan, K.C. HAART for HIV in China—Much achieved, more to be done. Lancet Infect. Dis. 2011, 11, 491–492. [Google Scholar] [CrossRef]
- Shang, H.; Xu, J.; Han, X.; Spero Li, J.; Arledge, K.C.; Zhang, L. HIV prevention: Bring safe sex to China. Nature 2012, 485, 576–577. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Chow, E.P.; Jing, J.; Zhuang, X.; Li, X.S.; He, M.; Sun, H.M.; Li, X.Y.; Gorgens, M.; Wilson, D.; et al. HIV prevalence in China: Integration of surveillance data and a systematic review. Lancet Infect. Dis. 2013, 13, 955–963. [Google Scholar] [CrossRef]
- State Council AIDS Working Committee Office (SCAWCO). China 2010 UNGASS Country Progress Report; Ministry of Health of the People’s Republic of China: Beijing, China, 2010. [Google Scholar]
- MacKellar, D.A.; Valleroy, L.A.; Secura, G.M.; Behel, S.; Bingham, T.; Celentano, D.D.; Koblin, B.A.; Lalota, M.; McFarland, W.; Shehan, D.; et al. Unrecognized HIV infection, risk behaviors, and perceptions of risk among young men who have sex with men: Opportunities for advancing HIV prevention in the third decade of HIV/AIDS. J. Acquir. Immune Defic. Syndr. 2005, 38, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Li, H.M.; Peng, R.R.; Li, J.; Yin, Y.P.; Wang, B.; Cohen, M.S.; Chen, X.-S. HIV incidence among men who have sex with men in China: A meta-analysis of published studies. PLoS ONE 2011, 6, e23431. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Yang, H.; Li, J.; Wei, C.; Xu, J.; Liu, X.; Xu, X.; McFarland, W. Emerging disparity in HIV/AIDS disease progression and mortality for men who have sex with men, Jiangsu Province, China. AIDS Behav. 2014, 18, S5–S10. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.L. HIV testing as prevention among MSM in China: The business of scaling-up. Glob. Public Health 2014, 9, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Ruan, S.; Zhao, J.; Yang, H.; Zhu, Y.; Raymond, H.F. Which Chinese men who have sex with men miss out on HIV testing? Sex Transm. Infect. 2011, 87, 225–228. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; Lundgren, J.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.G.; Burman, W.; Clumeck, N.; Cohen, C.J.; et al. CD4+ count-guided interruption of antiretroviral treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [PubMed]
- Yang, J.; Xing, H.; Niu, J.; Liao, L.; Ruan, Y.; He, X.; Feng, Y.; Li, Z.; Shao, Y. The emergence of HIV-1 primary drug resistance genotypes among treatment-naive men who have sex with men in high-prevalence areas in China. Arch. Virol. 2013, 158, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; He, C.; Xing, H.; Liao, L.; Xu, X.; He, J.; Liu, Y.; Ling, H.; Liang, S.; His, J.H.; et al. Short communication: Emerging transmitted HIV type 1 drug resistance mutations among patients prior to start of first-line antiretroviral therapy in middle and low prevalence sites in China. AIDS Res. Hum. Retrovir. 2012, 28, 1637–1639. [Google Scholar] [CrossRef] [PubMed]
- China NBoSo. The Sixth National Population Census of China; National Bureau of Statistics of China: Beijing, China, 2010.
- Chow, E.P.F.; Jing, J.; Feng, Y.J.; Min, D.; Zhang, J.; Wilson, D.P.; Zhang, X.H.; Zhang, L. Pattern of HIV testing and multiple sexual partnerships among men who have sex with men in China. BMC Infect. Dis. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhang, F.; Zhao, Y.; Zang, C.; Zhao, D.; Dou, Z.; Yu, L.; Fang, H.; Zhu, T.Y.; Chen, R.Y. Cohort profile: The Chinese national free antiretroviral treatment cohort. Int. J. Epidemiol. 2010, 39, 973–979. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Case Definitions of HIV for Surveillance and Revised Clinical Staging and Immunological Classification of HIV-Related Disease in Adults and Children; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- The University of California SFU, Cochrane Review Group on HIV/AIDS. How Accurately Do the WHO 2010 Immunological or Clinical Criteria Predict Virological Failure in Adults and Children Receiving ART? World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- Xing, H.; Ruan, Y.; Hsi, J.H.; Kan, W.; Liao, L.; Leng, X.; Wang, J.; He, C.; Shao, Y.; National HIVDR Working Group. Reductions in virological failure and drug resistance in Chinese antiretroviral-treated patients due to lamivudine-based regimens, 2003–2012. J. Antimicrob. Chemother. 2015, 70, 2097–2103. [Google Scholar] [PubMed]
- Moore, R.D.; Keruly, J.C. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin. Infect. Dis. 2007, 44, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Gras, L.; Kesselring, A.M.; Griffin, J.T.; van Sighem, A.I.; Fraser, C.; Ghani, A.C.; Miedema, F.; Reiss, P.; Lange, J.M.A.; de Wolf, F. CD4 cell counts of 800 cells/mm3 or greater after 7 years of highly active antiretroviral therapy are feasible in most patients starting with 350 cells/mm3 or greater. J. Acquir. Immune Defic. Syndr. 2007, 45, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Hu, N.; Xin, Q.; Beck, J. HIV testing among men who have sex with men in China: A systematic review and meta-analysis. AIDS Behav. 2012, 16, 1717–1728. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lu, H.; Raymond, H.F.; Sun, Y.; Jia, Y.; He, X.; Fan, S.; Shao, Y.; McFarland, W.; Xiao, Y.; et al. Untested and undiagnosed: Barriers to HIV testing among men who have sex with men, Beijing, China. Sex Transm. Infect. 2012, 88, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Ma, N.; Zheng, M.; Liu, M.; Chen, X.; Zheng, J.; Chen, H.G.; Wang, N. Impact of condom use and standardized sexually transmitted disease treatment on HIV prevention among men who have sex with men in hunan province: Using the Asian epidemic model. AIDS Res. Hum. Retrovir. 2012, 28, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Muessig, K.E.; McLaughlin, M.M.; Nie, J.M.; Cai, W.; Zheng, H.; Yang, L.; Tucher, J.D. Suboptimal antiretroviral therapy adherence among HIV-infected adults in Guangzhou, China. AIDS Care 2014, 26, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Leng, X.; Liang, S.; Ma, Y.; Dong, Y.; Kan, W.; Goan, D.; His, J.H.; Liao, L.; Wang, J.; He, C.; et al. HIV virological failure and drug resistance among injecting drug users receiving first-line ART in China. BMJ Open 2014, 4, e005886. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; He, C.; Hsi, J.H.; Xu, X.; Liu, Y.; He, J.; Ling, H.; Ding, P.; Tong, Y.; Zou, X.; et al. Virological outcomes and drug resistance in Chinese patients after 12 months of 3TC-based first-line antiretroviral treatment, 2011–2012. PLoS ONE 2014, 9, e88305. [Google Scholar] [CrossRef] [PubMed]
- Spillane, H.; Nicholas, S.; Tang, Z.; Szumilin, E.; Balkan, S.; Pujades-Rodriguez, M. Incidence, risk factors and causes of death in an HIV care programme with a large proportion of injecting drug users. Trop. Med. Int. Health 2012, 17, 1255–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Yang, L.; Li, H.; Zuo, L.; Liang, S.; Liu, W.; Dong, Y.; Yang, S.; Shang, H.; Li, J.; et al. Factors associated with HIV virologic failure among patients on HAART for one year at three sentinel surveillance sites in China. Curr. HIV Res. 2011, 9, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Zaccarelli, M.; Barracchini, A.; de Longis, P.; Perno, C.F.; Soldani, F.; Liuzzi, G.; Serraino, D.; Ippolito, G.; Antinori, A. Factors related to virologic failure among HIV-positive injecting drug users treated with combination antiretroviral therapy including two nucleoside reverse transcriptase inhibitors and nevirapine. AIDS Patient Care STDS 2002, 16, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Knobel, H.; Guelar, A.; Carmona, A.; Espona, M.; Gonzalez, A.; Lopez-Colomes, J.L.; Saballs, P.; Gimeno, J.L.; Díez, A. Virologic outcome and predictors of virologic failure of highly active antiretroviral therapy containing protease inhibitors. AIDS Patient Care STDS 2001, 15, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Waldrop-Valverde, D.; Valverde, E. Homelessness and psychological distress as contributors to antiretroviral nonadherence in HIV-positive injecting drug users. AIDS Patient Care STDS 2005, 19, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, M.P.; Chesney, M.A.; Spire, B.; Loundou, A.; Sobel, A.; Lepeu, G.; Moatti, J.P. Failure to maintain adherence to HAART in a cohort of French HIV-positive injecting drug users. Int. J. Behav. Med. 2003, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.E.; Hanson, D.L.; Jones, J.L.; Dworkin, M.S. Viral load as an independent risk factor for opportunistic infections in HIV-infected adults and adolescents. AIDS 2001, 15, 1831–1836. [Google Scholar] [CrossRef] [PubMed]
- Okoye, A.A.; Picker, L.J. CD4(+) T-cell depletion in HIV infection: Mechanisms of immunological failure. Immunol. Rev. 2013, 254, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Masur, H.; Brooks, J.T.; Benson, C.A.; Holmes, K.K.; Pau, A.K.; Kaplan, J.E. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Updated Guidelines from the Centers for Disease Control and Prevention, National Institutes of Health, and HIV Medicine Association of the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 58, 1308–1311. [Google Scholar] [PubMed]
- Lucas, S.; Nelson, A.M. HIV and the spectrum of human disease. J. Pathol. 2015, 235, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, C.J.; Harrington, R.D.; Dhanireddy, S.; Crane, H.M.; Casper, C.; Kitahata, M.M. Paradoxical immune reconstitution inflammatory syndrome in HIV-infected patients treated with combination antiretroviral therapy after AIDS-defining opportunistic infection. Clin. Infect. Dis. 2012, 54, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.; Zolopa, A. Initiation of antiretroviral therapy in the hospitalized patient with an acute AIDS-related opportunistic infection and other conditions: No time to lose. Curr. HIV/AIDS Rep. 2009, 6, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Dou, Z.; Chen, R.Y.; Wang, Z.; Ji, G.; Peng, G.; Qiao, X.; Fu, J.; Meng, X.; Bulterys, M.; Ma, Y.; et al. HIV-infected former plasma donors in rural Central China: From infection to survival outcomes, 1985–2008. PLoS ONE 2010, 5, e13737. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Dou, Z.; Yu, L.; Xu, J.; Jiao, J.H.; Wang, N.; Ma, Y.; Zhao, Y.; Zhao, H.; Chen, R.Y. The effect of highly active antiretroviral therapy on mortality among HIV-infected former plasma donors in China. Clin. Infect. Dis. 2008, 47, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Badri, M.; Cleary, S.; Maartens, G.; Pitt, J.; Bekker, L.G.; Orrell, C.; Wood, R. When to initiate highly active antiretroviral therapy in sub-Saharan Africa? A South African cost-effectiveness study. Antivir. Ther. 2006, 11, 63–72. [Google Scholar] [PubMed]
- Konrad, S.; Skinner, S.; Kazadi, G.B.; Gartner, K.; Lim, H.J. HIV disease progression to CD4 count <200 cells/muL and death in Saskatoon, Saskatchewan. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, 97–101. [Google Scholar] [PubMed]
- Phanuphak, P.; Lo, Y.R. Implementing early diagnosis and treatment: Programmatic considerations. Curr. Opin. HIV AIDS 2015, 10, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Krusi, A.; Wood, E.; Montaner, J.; Kerr, T. Social and structural determinants of HAART access and adherence among injection drug users. Int. J. Drug Policy 2010, 21, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.; Kerr, T.; Tyndall, M.W.; Montaner, J.S. A review of barriers and facilitators of HIV treatment among injection drug users. AIDS 2008, 22, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Dou, Z.; Xu, J.; Jiao, J.H.; Ma, Y.; Durako, S.; Yu, L.; Zhao, Y.; Zhang, F. Gender difference in 2-year mortality and immunological response to ART in an HIV-infected Chinese population, 2006–2008. PLoS ONE 2011, 6, e22707. [Google Scholar] [CrossRef] [PubMed]
- Collazos, J.; Asensi, V.; Carton, J.A. Sex differences in the clinical, immunological and virological parameters of HIV-infected patients treated with HAART. AIDS 2007, 21, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Rotger, M.; Csajka, C.; Telenti, A. Genetic, ethnic, and gender differences in the pharmacokinetics of antiretroviral agents. Curr. HIV/AIDS Rep. 2006, 3, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Nash, D.; Katyal, M.; Brinkhof, M.W.; Keiser, O.; May, M.; Hughes, R.; Dabis, F.; Wood, R.; Sprinz, E.; Schechter, M.; et al. Long-term immunologic response to antiretroviral therapy in low-income countries: A collaborative analysis of prospective studies. AIDS 2008, 22, 2291–2302. [Google Scholar] [CrossRef] [PubMed]
- Cornell, M.; Myer, L.; Kaplan, R.; Bekker, L.G.; Wood, R. The impact of gender and income on survival and retention in a South African antiretroviral therapy programme. Trop. Med. Int. Health 2009, 14, 722–731. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (Percent) | |
|---|---|---|
| Sex | ||
| Female | 2436 (33.2%) | |
| Male | 4897 (66.8%) | |
| Age, years, median (IQR) | 40 (32–49) | |
| Marriage status | ||
| Single | 1489 (20.3%) | |
| Married | 4230 (57.7%) | |
| Divorced | 963 (13.1%) | |
| Widowed | 639 (8.7%) | |
| Unknown | 12 (0.16%) | |
| CD4 at ART Initiation (cells/mm3) (IQR) | 151 (43–246) | |
| Female | 164 (79–283) | |
| Male | 138 (32–225) | |
| Viral Load at ART Initiation (log10 * copies/mL) (IQR) | 4.73 (3.69–5.47) | |
| WHO Stage at ART Initiation | ||
| Stage 1 | 2426 (33.1%) | |
| Stage 2 | 1471 (20.1%) | |
| Stage 3 | 1775 (24.2%) | |
| Stage 4 | 915 (12.5%) | |
| Missing | 746 (10.2%) | |
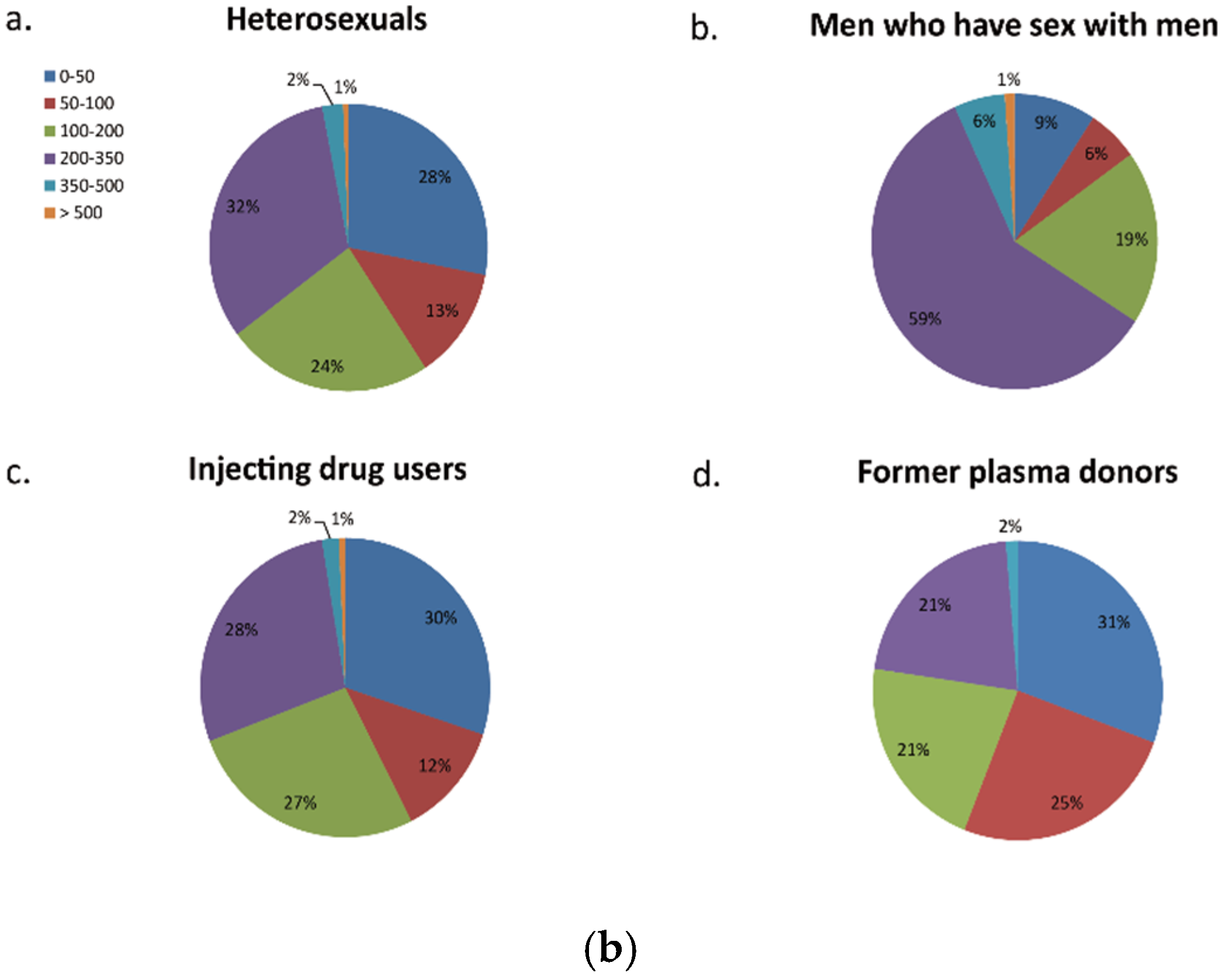
| CD4 group (cells/mm3) | ||
| 0–50 | 1905 (26.0%) | |
| 50–100 | 870 (11.9%) | |
| 100–200 | 1699 (23.2%) | |
| 200–350 | 2372 (32.3%) | |
| 350–500 | 169 (2.3%) | |
| >500 | 48 (0.7%) | |
| Missing | 270 (3.7%) | |
| Days from diagnosis to treatment(IQR) | 60 (26–273) | |
| Transmission route | ||
| Heterosexuals | 5484 (74.8%) | |
| Men who have sex with men | 553 (7.5%) | |
| Injecting drug users | 1164 (15.9%) | |
| Former plasma donor | 132 (1.8%) | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, S.; Chen, X.; Mao, L.; He, J.; Wei, X.; Jing, J.; Zhang, L. Superior Effects of Antiretroviral Treatment among Men Who have Sex with Men Compared to Other HIV At-Risk Populations in a Large Cohort Study in Hunan, China. Int. J. Environ. Res. Public Health 2016, 13, 283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13030283
Su S, Chen X, Mao L, He J, Wei X, Jing J, Zhang L. Superior Effects of Antiretroviral Treatment among Men Who have Sex with Men Compared to Other HIV At-Risk Populations in a Large Cohort Study in Hunan, China. International Journal of Environmental Research and Public Health. 2016; 13(3):283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13030283
Chicago/Turabian StyleSu, Shu, Xi Chen, Limin Mao, Jianmei He, Xiuqing Wei, Jun Jing, and Lei Zhang. 2016. "Superior Effects of Antiretroviral Treatment among Men Who have Sex with Men Compared to Other HIV At-Risk Populations in a Large Cohort Study in Hunan, China" International Journal of Environmental Research and Public Health 13, no. 3: 283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13030283