On the Development of Health-Based Ventilation Guidelines: Principles and Framework

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Rationale for Developing Health-Based Ventilation Guidelines
1.2. Objective
2. Proposed Framework for Setting Health-Based Ventilation Guidelines
2.1. Terms and Conditions for Developing the Guidelines
- (1)
- The guidelines should refer to established exposure guidelines that reduce health risks.
- (2)
- The guidelines should acknowledge that ventilation is a subordinate strategy for improving IAQ after the adoption of the due air pollution source control measures.
- (3)
- The guidelines should define the “base ventilation rate” that must always be guaranteed to remove emissions from humans (human bio-effluents) and, ultimately, the criteria to select the specific “health-based ventilation rate” for a specific building.
2.1.1. Health-Based Exposure Guidelines and Exposure Limits
2.1.2. Ventilation as a Subordinate Strategy for Controlling IAQ
2.1.3. Definition of Base Ventilation Rate and Decision Diagram to Select the Health-Based Ventilation Rate
2.2. Determination of the Base Ventilation Rate
2.2.1. The Evidence on the Effects of Human Bioeffluents
2.2.2. Modelling the Levels of CO2 from Humans
2.2.3. Modelling Moisture Levels Produced by Humans
- Ambient conditions with temperature of −10 °C and a relative humidity of 100%, that is, relatively dry but cold air that could potentially increase the risk of high humidity levels near the inner surfaces of the building envelope;
- Ambient conditions with temperature of +10 °C and a relative humidity of 75% and 85%, representing conditions that can favour the increased risk of house dust mites and mould growth.
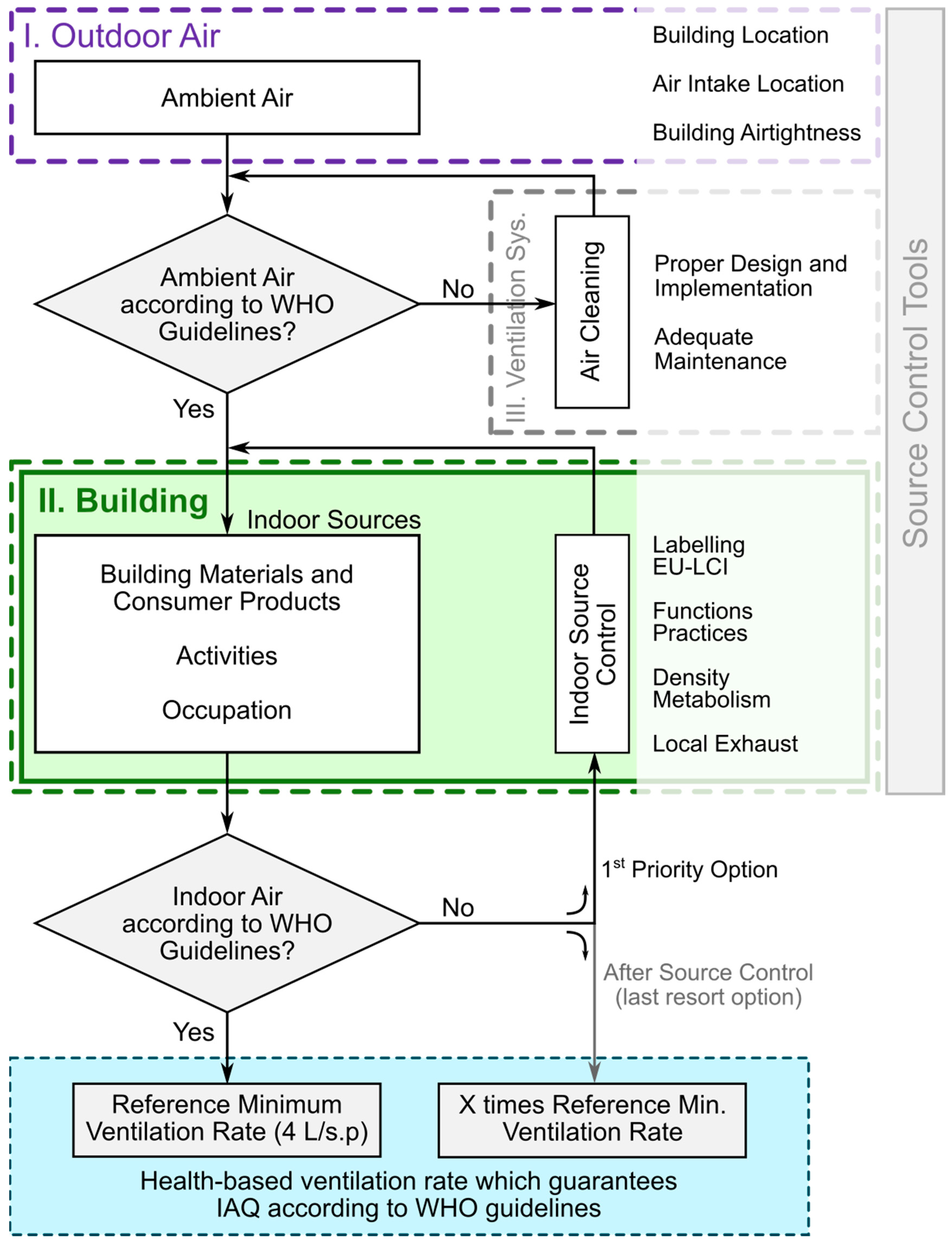
2.3. Decision Diagram for Selecting the Health-Based Ventilation Rate for a Specific Building
2.3.1. Outdoor Air
2.3.2. Building
2.3.3. Health-Based Ventilation Requirements
2.3.4. Ventilation System
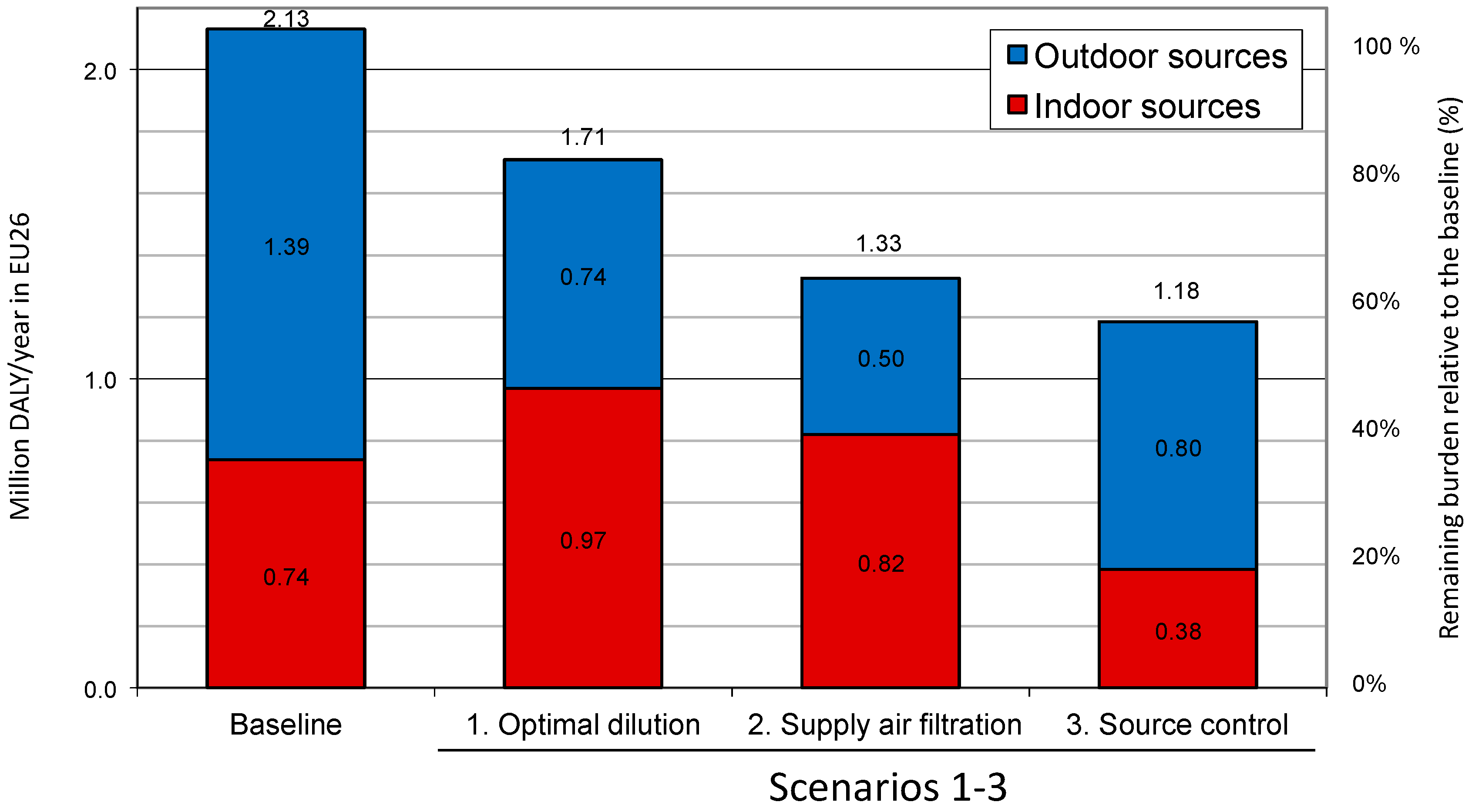
3. Benefits from Implementation of the Proposed Framework
- Scenario 1 represents a building stock with simply optimized ventilation (i.e., by changing ventilation only) to minimize the burden of disease.
- Scenarios 2 and 3 represent two alternative ways of improving indoor air quality in buildings. In Scenario 2 it is achieved by enhanced filtration of the outdoor air supplied, to remove ambient pollutants. In Scenario 3 it is attained by source control indoors together with application of a base ventilation rate.
4. Discussion
5. Implementation, Regulations, Research Needs on the Proposed Framework
- A common regulation of ventilation in Europe shall be developed that takes into account local climate and specific aspects of local culture.
- A harmonized framework of construction and consumer products emissions labelling criteria shall be developed.
- Building regulations that require products with certified emissions already at the building design stage shall be developed.
- Adequate regulations shall be developed for indoor air quality maintenance, inspection and operation.
- Criteria and requirements for energy efficient buildings shall be developed in which the requirements for health-based ventilation are decoupled from the requirements placed upon systems for maintaining thermal comfort (heating/cooling).
- European guidance shall be developed on the proper design, construction, maintenance and inspection of ventilation systems.
- Harmonization framework for indoor air monitoring which was recently developed by the European Commission (DG JRC and DG SANCO) in the context of the PILOT INDOOR AIR MONIT project, particularly useful in the context of auditing.
- Legislative instruments, such as Ecolabel criteria for various products, Ecodesign Directive Lot 6 on ventilation, CEN/TC 350/WG 5 prEN 16309 “Sustainability of construction works” [67].
- Population-representative measurement campaigns on indoor exposures in all major types of buildings including quantification of ventilation rates and analysis of the health impact of indoor and outdoor sources.
- Investigations that identify the health endpoints that are relevant to indoor exposures particularly with respect to examination of chronic health effects and subpopulations with special needs (vulnerable groups such as children, elderly or people with allergies or other hypersensitivities).
6. Conclusions
- Air quality shall comply with WHO Air Quality Guidelines.
- Source control should be the primary strategy for managing indoor air exposures.
- Ventilation is a supplementary strategy for improving indoor air quality in buildings.
- The health-based ventilation rate for a specific building should be determined according to the decision diagram proposed by the HealthVent project.
- The health-based ventilation rate must not be lower than the base ventilation rate.
- The base ventilation rate is proposed to be set at 4 L/s per person.
- Ventilation systems and health-based ventilation standards shall comply with the health-based ventilation guidelines’ framework.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bluyssen, P.M.; De Olivera Fernandes, E.; Groes, L.; Clausen, G.; Fanger, P.O.; Valbjørn, O.; Bernhard, C.A.; Roulet, C.A. European indoor air quality audit project in 56 office buildings. Indoor Air 1996, 6, 221–238. [Google Scholar] [CrossRef]
- Fisk, W.J.; Mirer, A.G.; Mendell, M.J. Quantitative relationship of sick building syndrome symptoms with ventilation rates. Indoor Air 2009, 19, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wargocki, P.; Wyon, D. Ten questions concerning thermal and indoor air quality effects on the performance of office work and schoolwork. Build. Environ. 2017, 112, 359–366. [Google Scholar] [CrossRef]
- Mendell, M.J.; Naco, G.M.; Wilcox, T.G.; Sieber, W.K. Environmental Risk Factors and Work-Related Lower Respiratory Symptoms in 80 Office Buildings: An Exploratory Analysis of NIOSH Data. Am. J. Ind. Med. 2003, 43, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Seppänen, O.; Fisk, W.J.; Mendell, M.J. Association of ventilation rates and CO2 concentrations with health and other responses in commercial and institutional buildings. Indoor Air 1999, 9, 226–252. [Google Scholar] [CrossRef] [PubMed]
- Wargocki, P.; Lagercrantz, L.; Witterseh, T.; Sundell, J.; Wyon, D.P.; Fanger, P.O. Subjective perceptions, symptom intensity and performance: A comparison of two independent studies, both changing similarly the pollution load in an office. Indoor Air 2002, 12, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Sundell, J.; Levin, H.; Nazaroff, W.W.; Cain, W.S.; Fisk, W.J.; Grimsrud, D.T.; Gyntelberg, F.; Li, Y.; Persily, A.K.; Pickering, A.C.; et al. Ventilation rates and health: Multidisciplinary review of the scientific literature. Indoor Air 2011, 21, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Carrer, P.; Wargocki, P.; Fanetti, A.; Bischof, W.; de Oliveira Fernandes, E.; Hartmann, T.; Kephalopoulos, S.; Palkonen, S.; Seppänen, O. What does the scientific literature tell us about the ventilation–health relationship in public and residential buildings? Build. Environ. 2015, 94, 273–286. [Google Scholar] [CrossRef]
- Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings e Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics; EN 15251; CEN: Brussels, Belgium, 2007.
- Ventilation for Acceptable Indoor Air Quality; ASHRAE Standard 62.1; ASHRAE: Atlanta, GA, USA, 2016.
- Mazzarella, L.; Hogeling, J. CEN Standard EN 16798-3:2017 on Ventilation for Non-Residential Buildings: Performance Requirements; REHVA Journal: Brussels, Belgium, 2018. [Google Scholar]
- Energy Performance of Buildings; EN 16798-1; Draft BS EN 16798-1; Revision of EN 15251; CEN: Brussels, Belgium, 2015.
- Fanger, P.O.; Berg Munch, B. Ventilation and body odor. In Proceedings of Engineering Foundation Conference of Atmospheres in Tightly Enclosed Spaces; ASHRAE: Atlanta, GA, USA, 1983; pp. 45–50. [Google Scholar]
- Berg-Munch, B.; Clausen, G.; Fanger, P.O. Ventilation requirements for the control of body odor in spaces occupied by women. Environ. Int. 1986, 12, 195–199. [Google Scholar] [CrossRef]
- Gunnarsen, L.; Fanger, P.O. Adaptation to indoor air pollution. Environ. Int. 1992, 18, 43–54. [Google Scholar] [CrossRef]
- Wargocki, P. Sensory pollution sources in buildings. Indoor Air 2004, 14 (Suppl. 7), 82–91. [Google Scholar] [CrossRef] [PubMed]
- Wargocki, P.; Fanger, P.O.; Krupicz, P.; Szczecinski, A. Sensory pollution loads in six office buildings and a department store in journal. Energy Build. 2004, 36, 995–1001. [Google Scholar] [CrossRef]
- De Oliveira Fernandes, E.; Jantunen, M.; Carrer, P.; Seppänen, O.; Harrison, P.; Kephalopoulos, S. Co-ordination Action on Indoor Air Quality and Health Effects (ENVIE). Final Report. 2009, p. 165. Available online: https://www.researchgate.net/publication/308890054_ENVIE (accessed on 26 June 2018).
- Jantunen, M.; de Oliveira Fernandes, E.; Carrer, P.; Kephalopoulos, S. Promoting Actions for Healthy Indoor Air (IAIAQ); European Commission Directorate General for Health and Consumers: Luxembourg, 2011; ISBN 978-92-79-20419-7. [Google Scholar]
- Quinet, E.; Baumstark, L.; Bonnet, J.; Croq, A.; Ducos, G.; Meunier, D.; Rigard-Cerison, A.; Roquigny, Q. L’évaluation Socio-Économique des Investissements Publics; Commissariat Général à la Stratégie et à la Prospective: Paris, France, 2013.
- Boulanger, G.; Bayeux, T.; Mandin, C.; Kirchner, S.; Vergriette, B.; Pernelet-Joly, V.; Kopp, P. Socio-economic costs of indoor air pollution: A tentative estimation for some pollutants of health interest in France. Environ. Int. 2017, 104, 14–24. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization). The Right to Healthy Indoor Air. In Proceedings of the WHO Meeting, Bilthoven, The Netherlands, 15–17 May 2000; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Dimitroulopoulou, C. Ventilation in European dwellings: A review. Build. Environ. 2012, 47, 109–125. [Google Scholar] [CrossRef]
- Framework for Health-Based Ventilation Guidelines in Europe; ECA Report No. 30; EUR 27640 EN; European Commission’s Joint Research Centre; Publications Office of the European Union: Luxembourg, 2018; in press.
- Seifert, B.; Levin, H.; Lindvall, T.; Moschandreas, D. A critical review of criteria and procedures for developing indoor air quality guidelines and standards. Proc. Indoor Air 1993, 3, 465–470. [Google Scholar]
- WHO (World Health Organization). Air Quality Guidelines for Europe; WHO Regional Publications, European Series, No. 23; World Health Organisation (WHO)—Regional Office for Europe: Copenhagen, Denmark, 1987. [Google Scholar]
- WHO (World Health Organization). Air Quality Guidelines for Europe, 2nd ed.; WHO Regional Publications, European Series, No. 91; World Health Organization (WHO)—Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- WHO (World Health Organization). WHO Air Quality Guidelines, Global Update 2005; Regional Office for Europe: Copenhagen, Denmark, 2006; p. 484. [Google Scholar]
- WHO (World Health Organization). WHO Guidelines for Indoor Air Quality: Dampness and Mould; WHO Regional Office for Europe: Copenhagen, Denmark, 2009. [Google Scholar]
- WHO (World Health Organization). Guidelines for Indoor Air Quality: Selected Pollutants; WHO Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Kotzias, D.; Koistinen, K.; Kephalopoulos, S.; Schlitt, C.; Carrer, P.; Maroni, M. The INDEX Project, Critical Appraisal of the Setting and Implementation of Indoor Exposure Limits in the EU; Final Report, EUR 21590 EN. European Commission, Directorate General, Joint Research Centre, 2005. Available online: http://ec.europa.eu/health/ph_projects/2002/pollution/fp_pollution_2002_exs_02.pdf (accessed on 26 June 2018).
- Koistinen, K.; Kotzias, D.; Kephalopoulos, S.; Schlitt, C.; Carrer, P.; Jantunen, M.; Kirchner, S.; McLaughlin, J.; Mølhave, L.; Fernandes, E.O.; et al. The INDEX project: Executive summary of a European Union project on indoor air pollutants. Allergy 2008, 63, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Von Pettenkofer, M. Über den Luftwechsel in Wohngebäuden; Cotta´sche Buchhandlung: München, Germany, 1858. [Google Scholar]
- Zhang, X.; Wargocki, P.; Lian, Z. Effects of exposures to human bioeffluents. In Proceedings of the 14th International Conference on Indoor Air Quality and Climate, Ghent, Belgium, 3–8 July 2016. [Google Scholar]
- Bakò-Birò, Z.; Kochhar, N.; Clements-Croome, D.J.; Awbi, H.B.; Williams, M. Ventilation rates in schools and learning performance. In Proceedings of the REHVA World Congress Clima, WellBeing Indoors, Helsinki, Finland, 10–14 June 2017; p. 1434. [Google Scholar]
- Maddalena, R.; Mendell, M.J.; Eliseeva, K.; Chan, W.R.; Sullivan, D.P.; Russell, M.; Satish, U.; Fisk, W.J. Effects of ventilation rate per person and per floor area on perceived air quality, sick building syndrome symptoms, and decision-making. Indoor Air 2015, 25, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Vehviläinen, T.; Lindholm, H.; Rintamäki, H.; Pääkkönen, R.; Hirvonen, A.; Niemi, O.; Vinha, J. High indoor CO2 concentrations in an office environment increases the transcutaneous CO2 level and sleepiness during cognitive work. J. Occup. Environ. Hygiene 2016, 13, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Strøm-Tejsen, P.; Zukowska, D.; Wargocki, P.; Wyon, D.P. The effects of bedroom air quality on sleep and next and day performance. Indoor Air 2016, 26, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, A.; Goto, T.; Yoshino, H.; Iino, Y.; Muramatsu, S. Regulations and standards for indoor air environment (IAE) in schools—An international review. In Healthy Buildings; Queensland University of Technology: Brisbane, Australia, 2012. [Google Scholar]
- Sundell, J. Guidelines for Nordic building regulations regarding indoor air quality. Environ. Int. 1982, 8, 17–20. [Google Scholar] [CrossRef]
- Mendell, M.J. Non-specific symptoms in office workers: A review and summary of the epidemiologic literature. Indoor Air 1993, 3, 227–236. [Google Scholar] [CrossRef]
- Tsushima, S.; Wargocki, P.; Tanabe, S. Sensory evaluation and chemical analysis of exhaled and dermally emitted bioeffluents. Indoor Air 2018, 28, 146–163. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wargocki, P.; Lian, Z. Human responses to carbon dioxide, a follow-up study at recommended exposure limits in non-industrial environments. Build. Environ. 2016, 100, 162–171. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wargocki, P.; Lian, Z. Physiological responses during exposure to carbon dioxide and bioeffluents at levels typically occurring indoors. Indoor Air 2017, 27, 65–77. [Google Scholar] [CrossRef] [PubMed]
- ACGIH. Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices; American Conference of Government Industrial Hygienists: Cincinnati, OH, USA, 2015.
- Jones, A.P. Indoor air quality and health. Atmos. Environ. 1999, 33, 4535–4564. [Google Scholar] [CrossRef]
- Satish, U.; Mendell, M.J.; Shekha, K.; Hotchi, T.; Sullivan, D.; Streufert, S.; Fisk, W.J. Is CO2 an Indoor Pollutant? Direct Effects of Low-to-Moderate CO2 Concentrations on Human Decision-Making Performance. Environ. Health Perspect. 2012, 120, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.G.; MacNaughton, P.; Satish, U.; Santanam, S.; Vallarino, J.; Spengler, J.D. Associations of Cognitive Function Scores with Carbon Dioxide, Ventilation, and Volatile Organic Compound Exposures in Office Workers: A Controlled Exposure Study of Green and Conventional Office Environments. Environ. Health Perspect. 2016, 124, 805–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajtár, L.; Herczeg, L. Influence of carbon-dioxide concentration on human wellbeing and intensity of mental work. Q. J. Hung. Meteorol. Serv. 2012, 116, 145–169. [Google Scholar]
- Liu, W.; Zhong, W.; Wargocki, P. Performance, acute health symptoms and physiological responses during exposure to high air temperature and carbon dioxide concentration. Build. Environ. 2017, 114, 96–105. [Google Scholar] [CrossRef]
- Fanger, P.O. Introduction of the olf and the decipol units to quantify air pollution perceived by humans indoors and outdoors. Energy Build. 1988, 12, 1–6. [Google Scholar] [CrossRef]
- Arlian, L.G.; Neal, J.S.; Morgan, M.S.; Vyszenski-Moher, D.L.; Rapp, C.M.; Alexander, A.K. Reducing relative humidity is a practical way to control dust mites and their allergens in homes in temperate climates. J. Allergy Clin. Immunol. 2001, 107, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Harriman, L.G.; Brundrett, G.W.; Kittler, R. Humidity Control Design Guide for Commercial and Institutional Buildings; ASHRAE: Atlanta, GA, USA, 2001. [Google Scholar]
- Umweltbundesamt (UBA). Recommendations on How to Prevent, Investigate, Evaluate, and Eliminate Indoor Mold Growth; German Federal Environmental Agency—Umweltbundesamt: Dessau-Roßlau, Germany, 2002.
- Harmonisation of Indoor Material Emissions Labelling Systems in the EU, Inventory of Existing Schemes; ECA Report No. 24; EUR 21891 EN; European Commission’s Joint Research Centre; Publications Office of the European Union: Luxembourg, 2005.
- Harmonisation Framework for Indoor Products Labelling Systems in EU; ECA Report No. 27; EUR 25276 EN; European Commission’s Joint Research Centre; Publications Office of the European Union: Luxembourg, 2012.
- Harmonisation Framework for Health Based Evaluation of Indoor Emissions from Construction Products in the European Union Using the EU-LCI Concept; ECA Report No. 29; EUR 26168 EN; European Commission’s Joint Research Centre; Publications Office of the European Union: Luxembourg, 2013.
- AIRLESS. A European Project to Optimise Indoor Air Quality and Energy Consumption of HVAC-Systems. 7th REHVA World Congress and Clima at Naples, Italy 2000. Available online: https://www.researchgate.net/publication/316845303_AIRLESS_A_European_project_to_optimise_indoor_air_quality_and_energy_consumption_of_HVAC-systems (accessed on 26 June 2018).
- Bluyssen, P.M.; Cox, C.; Seppänen, O.; de Oliveira Fernandes, E.; Clausen, G.; Müller, B.; Roulet, C.A. Why, when and how do HVAC-systems pollute the indoor environment and what to do about it? The European AIRLESS project. Build. Environ. 2003, 38, 209–225. [Google Scholar] [CrossRef]
- Asikainen, A.; Hänninen, O.; Kuhn, A.; Yang, A.; Loh, M.; Gerharz, L.; Brelih, N.; Jantunen, M. Modelling residential ventilation rates in European countries. In Proceedings of the Healthy Buildings Conference, Brisbane, Australia, 8–12 July 2012. [Google Scholar]
- Asikainen, A.; Hänninen, O.; Brelih, N.; Leal, V.; Allard, F.; Wargocki, P. Proportion of residences in European countries with ventilation rates below the limit defined by regulations. Int. J. Vent. 2013, 12, 129–134. [Google Scholar] [CrossRef]
- Hänninen, O.; Asikainen, A.; Bischof, W.; Carrer, P.; Seppänen, O.; de Oliveira Fernandes, E.; Wargocki, P. Health implications of alternative potential ventilation guidelines. In Proceedings of the Healthy Buildings Conference, Brisbane, Australia, 8–12 July 2012. [Google Scholar]
- Hänninen, O.; Asikainen, A.; Allard, F.; Bischof, W.; Carrer, P.; Seppänen, O.; Leal, V.; Kephalopoulos, S.; Warcocki, P. Optimal ventilation: Balancing exposures to indoor and outdoor pollutants. In Proceedings of the Ventilation 2012 Conference, Paris, France, 17–19 September 2012. [Google Scholar]
- Hänninen, O.; Asikainen, A. (Eds.) Efficient Reduction of Indoor Exposures: Health Benefits from Optimizing Ventilation, Filtration and Indoor Source Controls; Report 2/2013; National Institute for Health and Welfare (THL): Helsinki, Finland, 2013; p. 92.
- Horalek, J.; de Smet, P.; de Leeuw, F.; Kurfürst, P.; Benešová, N. European Air Quality Maps for 2015. ETC/ACM Technical Paper 2017/7; Bilthoven, The Netherlands. Available online: http://acm.eionet.europa.eu/reports/ETCACM_TP_2017_7_AQMaps2015 (accessed on 26 June 2018).
- Ventilation for Non-Residential Buildings—Performance Requirements for Ventilation and Room-Conditioning Systems; EN 13779; CEN: Brussels, Belgium, 2007.
- Sustainability of Construction Works. Assessment of Social Performance of Buildings—Methods; EN 16309; CEN: Brussels, Belgium, 2014.



{kind=link}
{kind=link}
| Pollutant | Air Quality Guidelines | Specific Indoor Air Quality Guidelines | ||
|---|---|---|---|---|
| AQ WHO (2000) | AQ WHO (2006) | EU-INDEX (2005) | IAQ WHO (2010) | |
| CO (mg/m3) | 100 (15 min) | 100 (15 min) | 100 (15 min) | |
| 60 (30 min) | 60 (30 min) | 60 (30 min) | ||
| 30 (1 h) | 30 (1 h) | 30 (1 h) | ||
| 10 (8 h) | 10 (8 h) | 10 (8 h) | ||
| 7 (24 h) | ||||
| NO2 (μg/m3) | 200 (1 h) | 200 (1 h) | 200 (1 h) | 200 (1 h) |
| 40 (1 y) | 40 (1 y) | 40 (1 w) | 40 (1 y) | |
| SO2 (μg/m3) | 500 (10 min) | 500 (10 min) | ||
| 125 (24 h) | 20 (24 h) | |||
| PM10 (μg/m3) | 50 (24 h) | |||
| 20 (1 y) | ||||
| PM2.5 (μg/m3) | 25 (24 h) | |||
| 10 (1 y) | ||||
| OZONE (μg/m3) | 100 (8 h) | |||
| RADON (Bq/m3) | No safe level Refer. level: 100 | |||
| Benzene (μg/m3) | UR 6 × 10−6 | No safe level-Not more than outdoor level | No safe level | |
| Tetrachloroethylene (μg/m3) | 250 (1 y) 8000 (30 m) | 250 (1 y) | ||
| Toluene (μg/m3) | 260 (1 w) 1000 (30 m) | 300 (long-term) | ||
| Styrene (μg/m3) | 260 (1 w) 70 (30 m) | 250 (long-term) | ||
| Xylenes (μg/m3) | 200 (long-term) | |||
| Formaldehyde (μg/m3) | 100 (30 min) | 30 (30 min) | 100 (30 min) | |
| Naphthalene (μg/m3) | 10 (1 y) | |||
| Building Type (Occupation Density) | Ventilation Rate (L/s per per.) | CO2,max ppm | Time to Reach 98% of CO2,max | Time to 1000 ppm (h:mm) | Typical Occupation Periods | Average CO2 ppm |
|---|---|---|---|---|---|---|
| School (2 m2/per.) | 4 | 1692 | 1:31 | 0:15 | 5 × 1.5 h classes (20 min. breaks + 1.5 h lunch break) | 1456 |
| 6 | 1261 | 0:58 | 0:19 | 1145 | ||
| 8 | 1046 | 0:42 | 0:33 | 977 | ||
| Office (10 m2/per.) | 4 | 1692 | 7:36 | 1:18 | 4 h + 4 h (1.5 h lunch break) | 1237 |
| 6 | 1261 | 4:54 | 1:39 | 1025 | ||
| 8 | 1046 | 3:34 | 2:45 | 901 | ||
| Residential (25 m2/per.) | 4 | 1692 | 19:01 | 3:15 | 12 h (continuous) | 1182 |
| 6 | 1261 | 12:15 | 4:08 | 1016 | ||
| 8 | 1046 | 8:55 | 6:53 | 904 |
| Hypothetical Scenarios for Assessing Impacts on Burden of Disease Based on the Implementation of the Different Indoor Exposure Mitigation Approaches | |
|---|---|
| Baseline scenario | Existing building stock and existing distribution of mechanical ventilation by country |
| Scenario 1 | Dilution of indoor emissions by health-based optimisation of national average ventilation rates |
| Scenario 2 | Filtration of particulate matter (PM2.5) in the outdoor air supply by 50% |
| Scenario 3 | Source control (90% reduction in second-hand smoke (SHS), carbon monoxide (CO) and radon (Rn); 50% reduction of volatile organic compounds (VOC) and dampness; 25% reduction of indoor generated PM2.5) (4 L/s per person) 1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrer, P.; De Oliveira Fernandes, E.; Santos, H.; Hänninen, O.; Kephalopoulos, S.; Wargocki, P. On the Development of Health-Based Ventilation Guidelines: Principles and Framework. Int. J. Environ. Res. Public Health 2018, 15, 1360. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071360
Carrer P, De Oliveira Fernandes E, Santos H, Hänninen O, Kephalopoulos S, Wargocki P. On the Development of Health-Based Ventilation Guidelines: Principles and Framework. International Journal of Environmental Research and Public Health. 2018; 15(7):1360. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071360
Chicago/Turabian StyleCarrer, Paolo, Eduardo De Oliveira Fernandes, Hugo Santos, Otto Hänninen, Stylianos Kephalopoulos, and Pawel Wargocki. 2018. "On the Development of Health-Based Ventilation Guidelines: Principles and Framework" International Journal of Environmental Research and Public Health 15, no. 7: 1360. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071360