Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Inclusion Criteria
2.2. Search Strategy
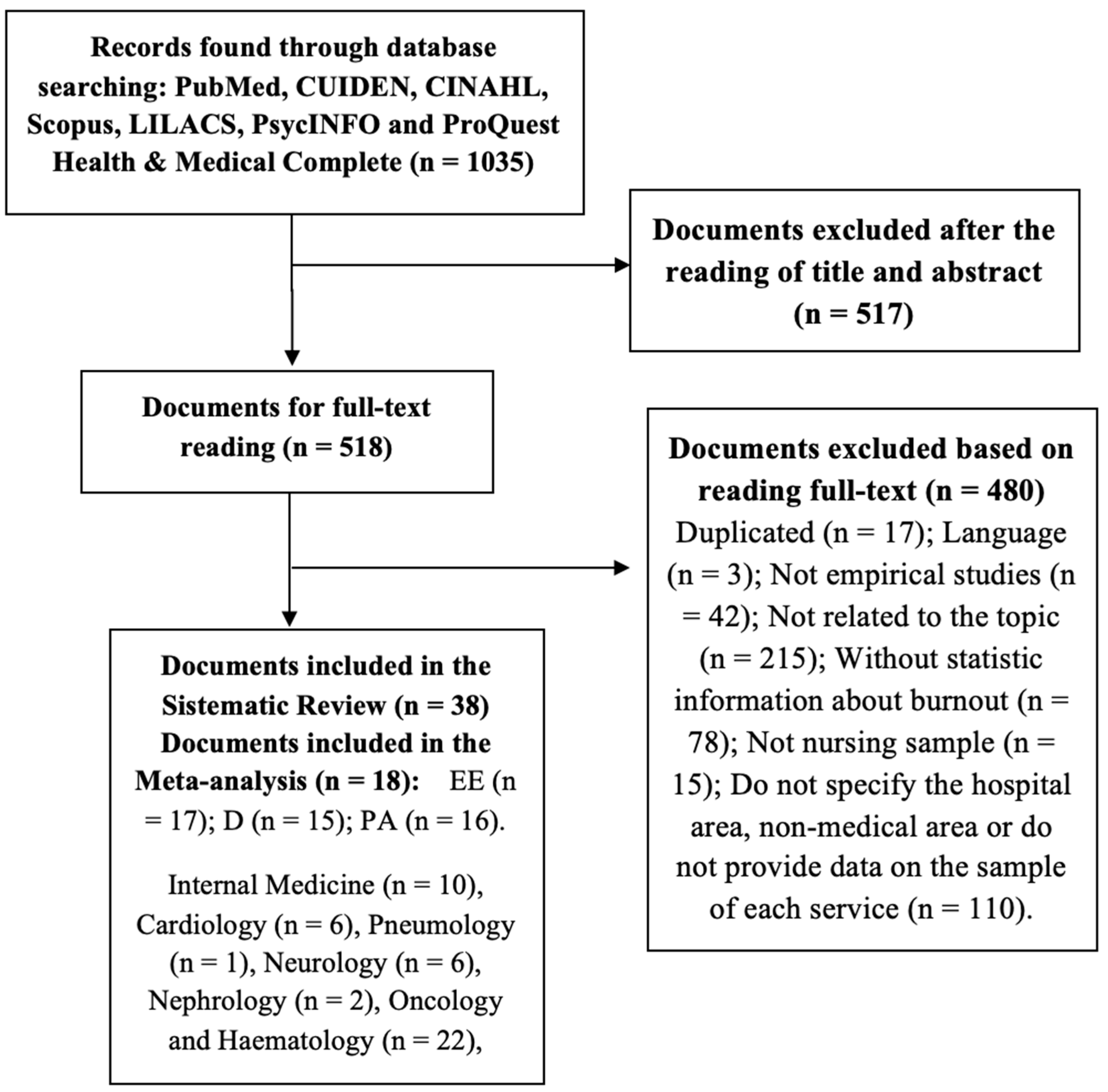
2.3. Study Selection
2.4. Data Coding
2.5. Data Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Main Risk Factors and Dimensions of Burnout
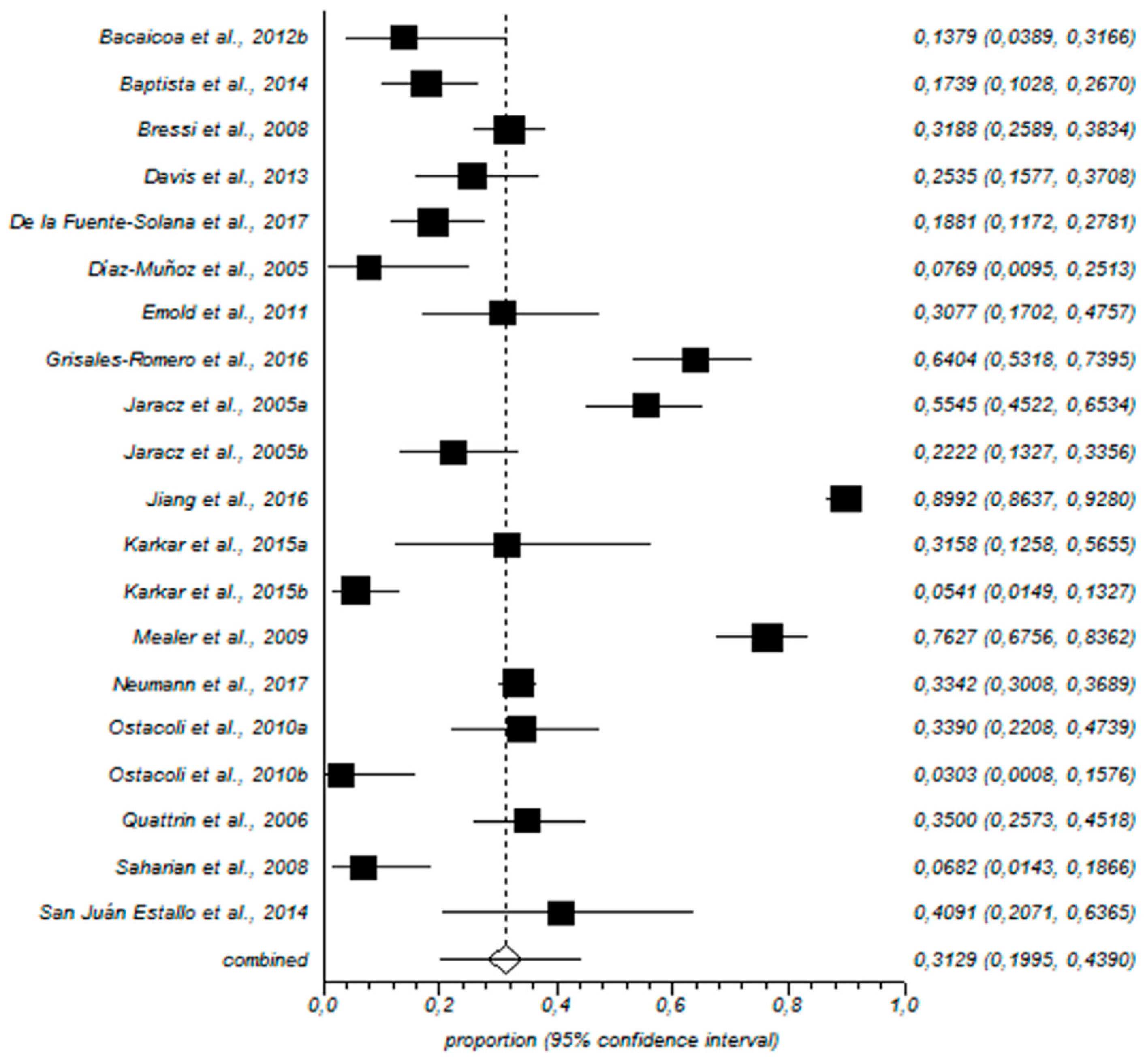
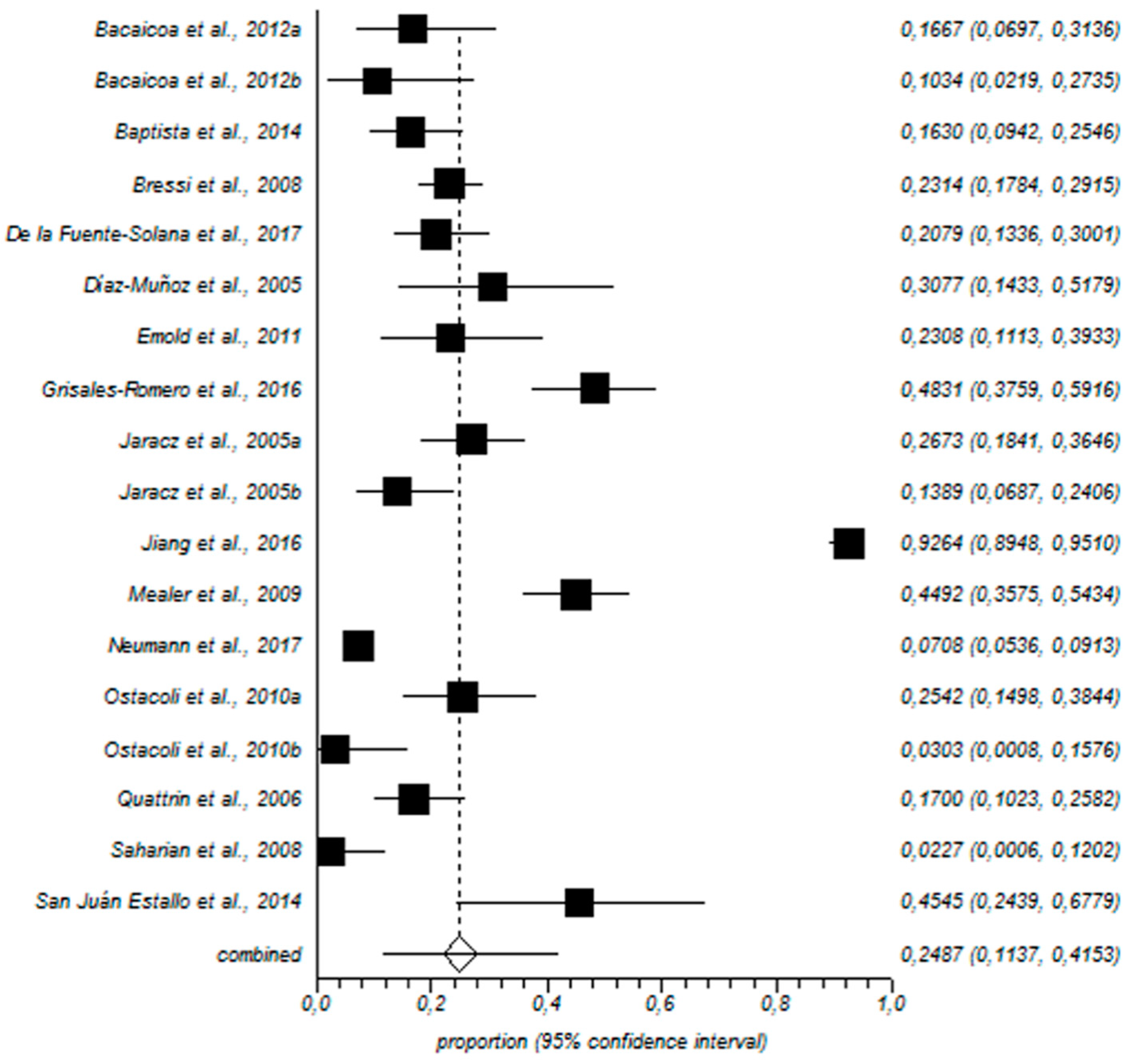
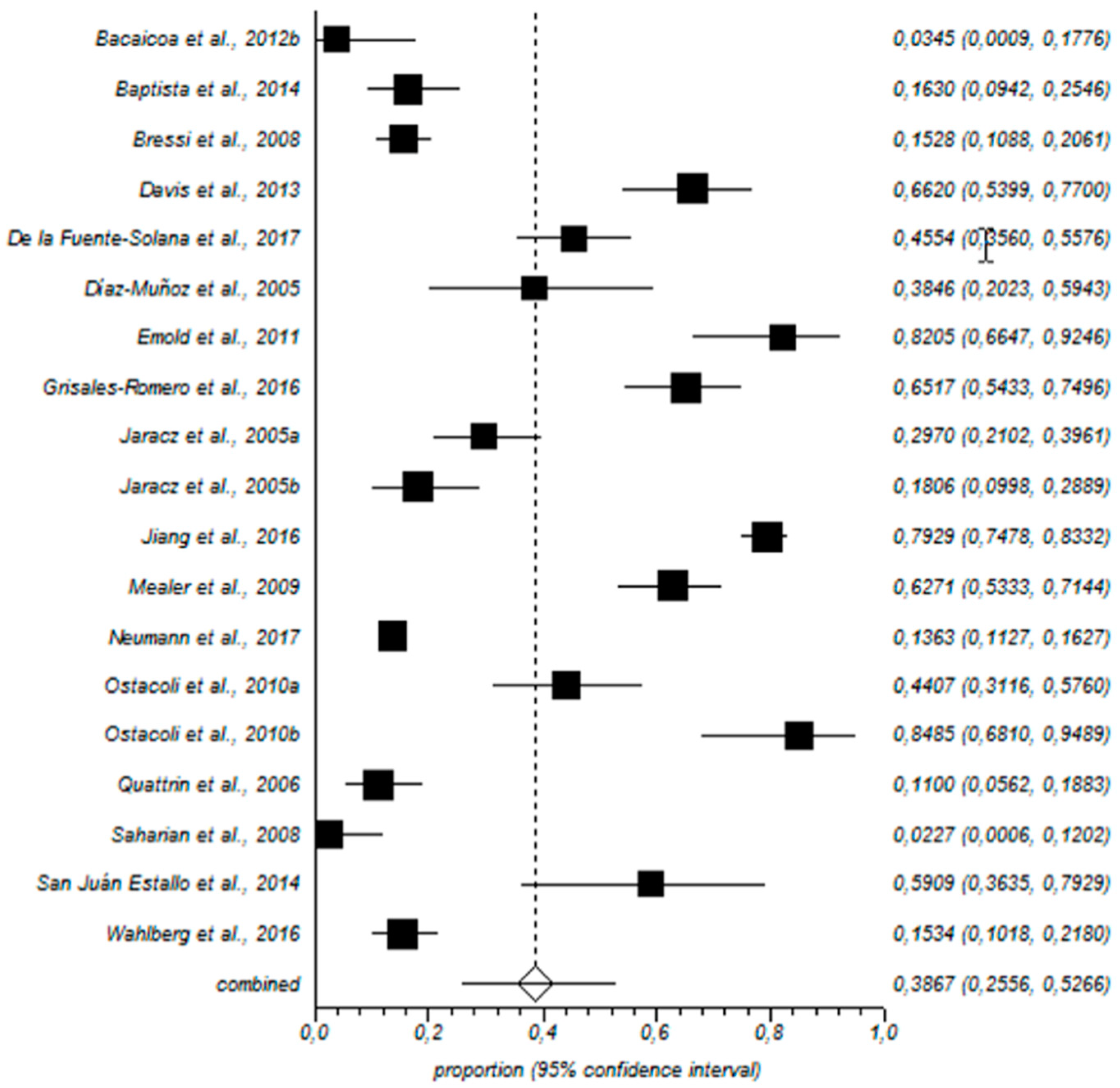
3.3. Meta-Analysis of Burnout Prevalence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Detzel, T.; Carlotto, M.S. Síndrome de burnout em trabalhadores da enfermagem de um hospital geral [Burnout syndrome in nursing staff in a general hospital]. Rev. SBPH 2008, 11 (Suppl. 1), 113–130. [Google Scholar]
- Lewis, H.S.; Cunningham, C.J. Linking nurse leadership and work characteristics to nurse burnout and engagement. Nurs. Res. 2016, 65 (Suppl. 1), 13–23. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C. Burnout: 35 years of research and practice. Career Dev. Int. 2009, 14 (Suppl. 3), 204–220. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Occup. Behav. 1981, 2 (Suppl. 2), 99–113. [Google Scholar] [CrossRef] [Green Version]
- Cañadas-De la Fuente, G.A.; San Luis, C.; Lozano, L.M.; Vargas, C.; García, I.; De la Fuente, E.I. Evidence for factorial validity of Maslach Burnout Inventory and burnout levels among health workers. Rev. Lat. Am. Psicol. 2014, 46 (Suppl. 1), 44–52. [Google Scholar] [CrossRef]
- Cañadas-De la Fuente, G.A.; Vargas, C.; San Luis, C.; García, I.; Cañadas, G.R.; De La Fuente, E.I. Risk factors and prevalence of burnout syndrome in the nursing profession. Int. J. Nurs. Stud. 2015, 52 (Suppl. 1), 240–249. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors related to physician burnout and its consequences: A review. Behav. Sci. (Basel). 2018, 8, 98. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Vargas, C.; De la Fuente, E.I.; Fernández-Castillo, R. Age as a Risk Factor for Burnout Syndrome in Nursing Professionals: A Meta-Analytic Study. Res. Nurs. Health 2017, 40 (Suppl. 2), 99–110. [Google Scholar] [CrossRef]
- Cañadas-De la Fuente, G.A.; Ortega, E.; Ramírez-Baena, L.; De la Fuente-Solana, E.I.; Vargas, C.; Gómez-Urquiza, J.L. Gender, marital status and children as risk factors for burnout in nurses: A meta-analytic study. Int. J. Environ. Res. Public Health 2018, 15, 2102. [Google Scholar] [CrossRef]
- Albendín, L.; Gómez, J.L.; Cañadas-De la Fuente, G.A.; Cañadas, G.R.; San Luis, C.; Aguayo, R. Bayesian prevalence and burnout levels in emergency nurses. A systematic review. Rev. Latinoam. Am. Psicol. 2016, 48 (Suppl. 2), 137–145. [Google Scholar] [CrossRef]
- Monsalve-Reyes, C.S.; San Luis-Costas, C.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo-Estremera, R.; Cañadas-De la Fuente, G.A. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Naz, S.; Hashmi, A.M.; Asif, A. Burnout and quality of life in nurses of a tertiary care hospital in Pakistan. J. Pak. Med. Assoc. 2016, 66, 532–536. [Google Scholar] [PubMed]
- Drach-Zahavy, A. How does service workers’ behavior affect their health? Service climate as moderator in the service behavior-health relationships. J. Occup. Health Psychol. 2010, 15 (Suppl. 2), 105–109. [Google Scholar] [CrossRef]
- Gandoy-Crego, M.; Clemente, M.; Mayán-Santos, J.M.; Espinosa, P. Personal determinants of burnout in nursing staff at geriatric centers. Arch. Gerontol. Geriatr. 2009, 48 (Suppl. 2), 246–249. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.P. Nurse retention and satisfaction in Ecuador: Implications for nursing administration. J. Nurs. Manag. 2014, 22 (Suppl. 1), 89–96. [Google Scholar] [CrossRef]
- Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L.; Ortega-Campos, E.M.; Cañadas, G.R.; Albendín-García, L.; De la Fuente-Solana, E.I. Prevalence of burnout syndrome in oncology nursing: A meta-analytic study. Psycho-Oncol. 2018, 27 (Suppl. 5), 1426–1433. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; De la Fuente-Solana, E.I.; Albendín-García, L.; Vargas-Pecino, C.; Ortega-Campos, E.M.; Cañadas-De la Fuente, G.A. Prevalence of burnout syndrome in emergency nurses: A meta-analysis. Crit. Care Nurse 2017, 37 (Suppl. 1), e1–e9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6 (Suppl. 7), e1000097. [Google Scholar] [CrossRef]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- Lipsey, M.W.; Wilson, D. Practical Meta-Analysis: Applied Social RESEARCH Methods, 1st ed.; SAGE Publications: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Phillips, B.; Ball, C.; Badenoch, D.; Straus, S.; Haynes, B.; Dawes, M. Oxford Centre for Evidence-based Medicine (CEBM). Levels of evidence. BJU Int. 2011, 107 (Suppl. 5), 870. [Google Scholar]
- Álvarez-Verdugo, L.P.; Bocanegra, P.; Migdolia, B. Prevalencia de desgaste profesional en personal de enfermería de un hospital de tercer nivel de Boyacá, Colombia. Enferm. Glob. 2013, 12 (Suppl. 29), 73–88. [Google Scholar]
- Bacaicoa, P.; Díaz, V.; Gea, M.; Linares, J.; Araya, E.; Alba, J.F.; Marrero, M. Comparativa y análisis del síndrome burnout entre el personal de enfermería en cardiología de dos hospitales de tercer nivel. Rev. Enferm. Cardiol. 2012, 19 (Suppls. 55–56), 34–40. [Google Scholar]
- Baptista, P.; Tito, R.; Felli, V.; Silva, F.; Silva, S. The shift work and the Burnout syndrome. Occup. Environ. Med. 2014, 71 (Suppl. 1), A108. [Google Scholar] [CrossRef]
- Basu, S.; Yap, C.; Mason, S. Examining the sources of occupational stress in an emergency department. Occup. Med. (Lond) 2016, 66 (Suppl. 9), 737–742. [Google Scholar] [CrossRef] [PubMed]
- Bressi, C.; Manenti, S.; Porcellana, M.; Cevales, D.; Farina, L.; Pescador, L. Haemato-oncology and burnout: An Italian survey. Br. J. Cancer 2008, 98 (Suppl. 6), 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.; Lind, B.; Sorensen, C. A comparison of burnout among oncology nurses working in adult and pediatric inpatient and outpatient settings. Oncol. Nurs. Forum 2013, 40 (Suppl. 4), E303–E311. [Google Scholar] [CrossRef]
- De la Fuente-Solana, E.I.; Gómez-Urquiza, J.L.; Cañadas, G.R.; Albendín-García, L.; Ortega-Campos, E.; Cañadas-De la Fuente, G.A. Burnout and its relationship with personality factors in oncology nurses. Eur. J. Oncol. Nurs. 2017, 30, 91–96. [Google Scholar] [CrossRef]
- Díaz-Muñoz, M.J. Síndrome del quemado en profesionales de Enfermería que trabajan en un hospital monográfico para pacientes cardíacos. Nure Inv. 2005, 18 (Suppl. 1), 1–8. [Google Scholar]
- Duarte, J.; Pinto-Gouveia, J. The role of psychological factors in oncology nurses’ burnout and compassion fatigue symptoms. Eur. J. Oncol. Nurs. 2017, 28, 114–121. [Google Scholar] [CrossRef]
- Emery, E.J. Perceived sources of stress among pediatric oncology nurses. J. Pediatr. Oncol. Nurs. 1993, 10 (Suppl. 3), 87–92. [Google Scholar] [CrossRef]
- Emold, C.; Schneider, N.; Meller, I.; Yagil, Y. Communication skills, working environment and burnout among oncology nurses. Eur. J. Oncol. Nurs. 2011, 15 (Suppl. 4), 358–363. [Google Scholar] [CrossRef]
- Faria, D.; Maia, E. Nursing professionals’ anxiety and feelings in terminal situations in oncology. Rev. Lat. Am. Enferm. 2007, 15 (Suppl. 6), 1131–1137. [Google Scholar] [CrossRef]
- Fawzy, F.; Wellisch, D.; Pasnau, R.; Leibowitz, B. Preventing nursing burnout: A challenge for liaison psychiatry. Gen. Hosp. Psychiat. 1983, 5 (Suppl. 2), 141–149. [Google Scholar] [CrossRef]
- Gama, G.; Barbosa, F.; Vieira, M. Personal determinants of nurses’ burnout in end of life care. Eur. J. Cancer Care 2014, 18 (Suppl. 5), 527–533. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.D.F.S.; Santos, M.M.M.C.C.; Carolino, E.T.D.M.A. Psycho-social risks at work: Stress and coping strategies in oncology nurses. Rev. Lat. Am. Enferm. 2013, 21 (Suppl. 6), 1282–1289. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Sánchez, M.; Álamo-Santos, M.; Amador-Bohórquez, M.; Ceacero-Molina, F.; Mayor-Pascual, A.; Muñoz-González, A.; Izquierdo-Atienza, M. Estudio de seguimiento del desgaste profesional en relación con factores organizativos en el personal de enfermería de medicina interna. Rev. SEMST 2009, 55, 52–62. [Google Scholar] [CrossRef]
- Grisales-Romero, H.; Muñoz, Y.; Osorio, D.; Robles, E. Síndrome de Burnout en el personal de enfermería de un hospital de referencia Ibagué, Colombia, 2014. Enferm. Glob. 2016, 41 (Suppl. 1), 244–257. [Google Scholar] [CrossRef]
- Jaracz, K.; Gorna, K.; Konieczna, J. Burnout, stress and styles of coping among hospital nurses. Ann. Acad. Med. Bialostoc. 2005, 50 (Suppl. 1), 216–219. [Google Scholar]
- Jiang, H.; Li, C.; Gu, Y.; Lu, H. Nurse satisfaction and burnout in Shanghai neurology wards. Rehabil. Nurs. 2016, 41 (Suppl. 2), 120–127. [Google Scholar] [CrossRef]
- Karakoc, A.; Yilmaz, M.; Alcalar, N.; Esen, B.; Kayabasi, H.; Sit, D. Burnout syndrome among hemodialysis and peritoneal dialysis nurses. Iran J. Kidney Dis. 2016, 10 (Suppl. 6), 395–404. [Google Scholar]
- Karkar, A.; Dammang, M.L.; Bouhaha, B.M. Stress and burnout among hemodialysis nurses: A single-center, prospective survey study. Saudi J. Kidney Dis. Transpl. 2015, 26 (Suppl. 1), 12. [Google Scholar] [CrossRef]
- Kousloglou, S.A.; Mouzas, O.D.; Bonotis, K.; Roupa, Z.; Vasilopoulos, A.; Angelopoulos, N.V. Insomnia and burnout in Greek nurses. Hippokratia 2014, 18 (Suppl. 2), 150–155. [Google Scholar] [PubMed]
- Książek, I.; Stefaniak, T.J.; Stadnyk, M.; Książek, J. Burnout syndrome in surgical oncology and general surgery nurses: A cross-sectional study. Eur. J. Oncol. Nurs. 2011, 15 (Suppl. 4), 347–350. [Google Scholar] [CrossRef] [PubMed]
- Kutluturkan, S.; Sozeri, E.; Uysal, N.; Bay, F. Resilience and burnout status among nurses working in oncology. Ann. Gen. Psychiatry 2016, 15 (Suppl. 1), 33. [Google Scholar] [CrossRef] [PubMed]
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress. Anxiety 2009, 26 (Suppl. 12), 1118–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowakowska, I.; Rasinska, R.; Glowacka, M.D. The influence of factors of work environment and burnout syndrome on self-efficacy of medical staff. Ann. Agric. Environ. Med. 2016, 23 (Suppl. 2), 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, J.L.; Mau, L.W.; Virani, S.; Denzen, E.M.; Boyle, D.A.; Majhail, N.S. Burnout, moral distress, work-life balance, and career satisfaction among hematopoietic cell transplantation professionals. Biol. Blood Marrow Transplant. 2017, 24 (Suppl. 4), 849–860. [Google Scholar] [CrossRef] [PubMed]
- Ostacoli, L.; Cavallo, M.; Zuffranieri, M.; Negro, M.; Sguazzotti, E.; Furlan, P.M. Comparison of experienced burnout symptoms in specialist oncology nurses working in hospital oncology units or in hospices. Palliat. Support. Care 2010, 8 (Suppl. 4), 427–432. [Google Scholar] [CrossRef]
- Quattrin, R.; Zanini, A.; Nascig, E.; Annunziata, M.A.; Calligaris, L.; Brusaferro, S. Level of burnout among nurses working in oncology in an Italian region. Oncol. Nurs. Forum 2006, 33 (Suppl. 4), 815–820. [Google Scholar] [CrossRef]
- Rodrigues, A.B.; Chaves, E.C. Stressing factors and coping strategies used by oncology nurses. Rev. Lat. Am. Enferm. 2008, 16 (Suppl. 1), 24–28. [Google Scholar] [CrossRef]
- Sadati, A.K.; Hemmati, S.; Rahnavard, F.; Lankarani, K.B.; Heydari, S.T. The impact of demographic features and environmental conditions on rates of nursing burnout. SEMJ 2016, 17 (Suppl. 3), e37882. [Google Scholar] [CrossRef]
- Sahraian, A.; Fazelzadeh, A.; Mehdizadeh, A.R.; Toobaee, S.H. Burnout in hospital nurses: A comparison of internal, surgery, psychiatry and burns wards. Int. Nurs. Rev. 2008, 55 (Suppl. 1), 62–67. [Google Scholar] [CrossRef] [PubMed]
- Sanjuán-Estallo, L.; Arrazola-Alberdi, O.; García-Moyano, L.M. Prevalencia del síndrome del burnout en el personal de enfermería del servicio de cardiología, neumología y neurología del Hospital San Jorge de Huesca. Enferm. Glob. 2014, 13 (Suppl. 36), 253–264. [Google Scholar] [CrossRef]
- Sehlen, S.; Vordermark, D.; Schäfer, C.; Herschbach, P.; Bayerl, A.; Zehentmayr, F. Job stress and job satisfaction of physicians, radiographers, nurses and physicists working in radiotherapy: A multicenter analysis by the DEGRO Quality of Life Work Group. Radiat. Oncol. 2009, 4 (Suppl. 1), 6. [Google Scholar] [CrossRef] [PubMed]
- Sirilla, J. Moral distress in nurses providing direct care on inpatient oncology units. Clin. J. Oncol. Nurs. 2014, 18 (Suppl. 5), 536–541. [Google Scholar] [CrossRef] [PubMed]
- Wahlberg, L.; Nirenberg, A.; Capezuti, E. Distress and coping self-efficacy in inpatient oncology nurses. Oncol. Nurs. Forum 2016, 43 (Suppl. 6), 738–746. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Singh-Carlson, S.; Odell, A.; Reynolds, G.; Su, Y. Compassion fatigue, burnout, and compassion satisfaction among oncology nurses in the United States and Canada. Oncol. Nurs. Forum 2016, 43 (Suppl. 4), E161–E169. [Google Scholar] [CrossRef]
- Yu, H.; Jiang, A.; Shen, J. Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: A cross-sectional survey. Int. J. Nurs. Stud. 2016, 57, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.L.; Cannon, K.J.; Wellik, K.E.; Wu, Q.; Budavari, A.I. Burnout in inpatient-based versus outpatient-based physicians: A systematic review and meta-analysis. J. Hosp. Med. 2013, 8 (Suppl. 11), 653–664. [Google Scholar] [CrossRef] [Green Version]
- Billeter-Koponen, S.; Fredén, L. Long-term stress, burnout and patient-nurse relations: Qualitative interview study about nurses´ experience. Scand. J. Caring Sci. 2005, 19, 20–27. [Google Scholar] [CrossRef]
- Partlak Günüsen, N.; Ustün, B.; Erdem, S. Work stress and emotional exhaustion in nurses: The mediatin role of internal locus of control. Res. Theory Nurs. Pract. 2014, 28, 260–268. [Google Scholar] [CrossRef]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17 (Suppl. 1), 264. [Google Scholar] [CrossRef] [PubMed]
- Fuentelsaz-Gallego, C.; Moreno-Casbas, T.; López-Zorraquino, D.; Gómez-García, T.; González-María, E. Percepción del entorno laboral de las enfermeras españolas en los hospitales del Sistema Nacional de Salud. Proyecto RN4CAST-España. Enferm. Clín. 2012, 22 (Suppl. 5), 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, M.C.; Fischer, F.M. A cohort study of psychosocial work stressors on work ability among Brazilian hospital workers. Am. J. Ind. Med. 2015, 58 (Suppl. 7), 795–806. [Google Scholar] [CrossRef] [PubMed]
- Van Bogaert, P.; Kowalski, C.; Weeks, S.M.; Clarke, S.P. The relationship between nurse practice environment, nurse work characteristics, burnout and job outcome and quality of nursing care: A cross-sectional survey. Int. J. Nurs. Stud. 2013, 50 (Suppl. 12), 1667–1677. [Google Scholar] [CrossRef]
- McHugh, M.D.; Kutney-Lee, A.; Cimiotti, J.P.; Sloane, D.M.; Aiken, L.H. Nurses’ widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff. (Milwood) 2011, 30 (Suppl. 2), 202–210. [Google Scholar] [CrossRef] [PubMed]
- Grazziano, E.S.; Ferraz Bianchi, E.R. Impacto del estrés ocupacional y burnout en enfermeros. Enferm. Global 2010, 18, 1–20. [Google Scholar] [CrossRef]
- Russo, G.; Fronteira, I.; Jesus, T.S.; Buchan, J. Understanding nurses’ dual practice: A scoping review of what we know and what we still need to ask on nurses holding multiple jobs. Hum. Resour. Health 2018, 16 (Suppl. 1), 14. [Google Scholar] [CrossRef]
- McNeeley, M.F.; Perez, F.A.; Chew, F.S. The emotional wellness of radiology trainees: Prevalence and predictors of burnout. Acad. Radiol. 2013, 20 (Suppl. 5), 647–655. [Google Scholar] [CrossRef]
- Peters, L.; Cant, R.; Payne, S.; O’Connor, M.; McDermott, F.; Shimoinaba, K. How death anxiety impacts nurses’ caring for patients at the end of life: A review of literature. Open Nurs. J. 2013, 7, 14. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Hajiesmaeili, M.; Kangasniemi, M.; Fornés-Vives, J.; Hunsucker, R.L.; Rahimibashar, F.; Pourhoseingholi, M.A.; Farrokhvar, L.; Miller, A.C. MORZAK Collaborative. Effects of stress on critical care nurses: A national cross-sectional study. J. Intensive Care Med. 2017, 20 (Suppl. 10), 1–12. [Google Scholar] [CrossRef]
- Stewart, D.; Thomas, B.; MacLure, K.; Pallivalapila, A.; El Kassem, W.; Awaisu, A.; McLay, J.S.; Wilbur, K.; Wilby, K.; Ryan, C.; et al. Perspectives of healthcare professionals in Qatar on causes of medication errors: A mixed methods study of safety culture. PLoS ONE 2018, 13, e0204801. [Google Scholar] [CrossRef] [PubMed]
- Cocker, F.; Joss, N. Compassion fatigue among healthcare, emergency and community service workers: A systematic review. Int. J. Environ. Res. Public Health. 2016, 13, 618. [Google Scholar] [CrossRef] [PubMed]
- Grice, J.; Barrett, P.; Cota, L.; Felix, C.; Taylor, Z.; Garner, S.; Medellin, E.; Vest, A. Four Bad Habits of Modern Psychologists. Behav. Sci. 2017, 7, 53. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Country, Year | Study design | Total sample and MA | Burnout Questionnaire | EE (k) | D (k) | PA (k) | Main results | LE | DR |
|---|---|---|---|---|---|---|---|---|---|
| Álvarez-Verdugo et al., Colombia, 2013 [22] | Cross-sectional, descriptive | k = 22 GYNE k = 2 PAED k = 3 ORTHO k = 4 NEURO k = 5 IM k = 5 SRGY k = 3 | MBI | - | - | - | Higher EE in the first 10 years of work and lower EE subsequently. Night work is a risk factor for burnout. Job insecurity is a risk factor for EE. Gender, age, marital status and education do not influence the appearance of burnout. | 2c | B |
| Bacaicoa et al., Spain, 2012 [23] | Cross-sectional, descriptive | k = 71 CARDIO | MBI | 13 | 7 | 25 | Cardiology nurses suffer high EE and low PA. The most influential factors for burnout are the family, changes of medical service, the pressure of hospital admissions, training outside working hours, the need to work weekends and poor adherence to the interdisciplinary team. | 2c | B |
| 4 | 3 | 1 | |||||||
| Baptista et al., Brazil, 2014 [24] | Cross-sectional, descriptive | k = 92 CARDIO | MBI | 16 | 15 | 15 | Shift work affects nurses’ quality of life and the health care provided. All three dimensions of burnout presented similar levels of prevalence. | 2c | B |
| Basu et al., UK, 2016 [25] | Cross-sectional, descriptive | k=174 A&E k = 61 NEURO k = 45 | Health and Safety Executive Stress Indicator Tool | - | - | - | Management of and participation in organisational change can reduce work stress. Lack of job recognition, together with organisational injustice, can provoke burnout in neurology nurses. | 2c | B |
| Bressi et al., Italy, 2008 [26] | Cross-sectional, descriptive | k = 350 ONC-HAEM | MBI | 73 | 53 | 35 | There is a high prevalence of burnout in oncological nurses, associated with increased depression and anxiety. High levels of EE were recorded, well above those of D and inadequate PA. Age, sex, personal dissatisfaction, physical fatigue and working with demanding patients all predispose to burnout. | 2c | B |
| Davis et al., USA, 2013 [27] | Cross-sectional, descriptive | k = 71 ONC-HAEM | MBI | 18 | - | 47 | The work environment can provoke EE and D, although low PA is the major dimension of burnout. EE is lower in younger and busier nurses. Job satisfaction is inversely associated with EE in the oncology services. | 2c | B |
| De la Fuente-Solana et al., Spain, 2017 [28] | Cross-sectional, descriptive | k = 101 ONC-HAEM | MBI | 19 | 21 | 46 | D and EE are positively correlated with neuroticism, anxiety and depression and inversely with friendliness, responsibility, extraversion and openness. PA is inversely correlated with all the personality variables considered and with anxiety and depression. | 2c | B |
| Díaz-Muñoz, Spain, 2005 [29] | Cross-sectional, descriptive | k = 26 CARDIO k = 11 ICU k = 15 | MBI | 2 | 8 | 10 | EE was observed more frequently in female nurses, those who are single and those without children. There was greater D among nurses with less training and those without children. PA was low among single nurses and ward staff, and was the dimension most strongly affected among all respondents. The degree of burnout observed was relatively low, although only 8% of nurses reported normal scores for the three subscales. | 2c | B |
| Duarte et al., Portugal, 2017 [30] | Cross-sectional, descriptive | k = 221 ONC-HAEM | Professional Quality of Life Scale and Interpersonal Reactivity Index | - | - | - | Nurses who are more likely to experience the negative consequences associated with providing health care (burnout and fatigue compassion) are more self-critical and have greater psychological rigidity. Moreover, they experience more personal feelings of anguish when they see others suffering and less feelings of empathy and sensitivity. | 2c | B |
| Emery, USA, 1993 [31] | Cross-sectional, descriptive | k = 155 ONC-HAEM | Spielberger State Trait Anxiety Inventory and Pediatric Oncology Nurse Stressor Questionnaire | - | - | - | Nurses who only work in paediatric oncology for extended periods present higher levels of burnout than those who work in different areas. Specialisation and studies to obtain a Master’s degree protect against burnout. Coping styles, positive reinforcement and social support are necessary to deal with the syndrome. | 2c | B |
| Emold et al., Israel, 2011 [32] | Cross-sectional, descriptive | k = 39 ONC-HAEM | MBI | 12 | 9 | 32 | EE and low PA are different experiences that can occur simultaneously. High scores were recorded for lack of PA. Communication skills, self-efficacy and cynicism are all related to the occurrence of burnout. | 2c | B |
| Faria et al., Brazil, 2007 [33] | Cross-sectional, descriptive | k = 43 ONC-HAEM | Spielberger State Trait Anxiety Inventory | - | - | - | Oncology nurses experience high levels of anxiety and stress. The number of patients treated, the hours worked, multiple employment, age and work experience all influence the development of burnout. | 2c | B |
| Fawzy et al., USA, 1983 [34] | Longitudinal, cohorts | k = 57 ONC-HAEM k = 12 GYNE k = 11 IM k = 11 CARDIO k = 11 SRGY k = 12 | Minnesota MultiPhasic Inventory, Locus of Control Test and Work Environment Scale | - | - | - | IM nurses have less job satisfaction than oncology nurses, as well as lower PA. No statistically significant association was found between personality variables and burnout. Older, married and more experienced nurses suffer greater burnout. Social support is the main protector against the syndrome. | 2b | B |
| Gama et al., Portugal, 2014 [35] | Cross-sectional, descriptive | k = 360 IM k = 184 ONC-HAEM k = 176 (ONC k = 48 HAEM k = 69 PALLIAT k = 59) | MBI | - | - | - | By burnout scores, there were no significant differences between hospital departments, except in palliative care, which presented lower EE and D and greater satisfaction and PA. Attitudes towards death and life, social support and length of professional experience are all protective factors against burnout. | 2c | B |
| Gomes et al., Portugal, 2013 [36] | Cross-sectional, descriptive | k = 96 ONC-HAEM | Occupational Stressors Inventory and Brief COPE | - | - | - | Oncology nurses present high levels of EE and burnout, due to a lack of work recognition, the special characteristics of the patient and attitudes towards death. Depression and anxiety are common in oncology nurses. Active coping mechanisms should be encouraged. | 2c | B |
| Gómez-Sánchez et al., Spain, 2009 [37] | Longitudinal, cohorts | k = 132 IM | MBI | - | - | - | Between 1998 and 2005, levels of EE fell, D remained constant and low PA worsened among IM nurses. Reducing work overload and enhancing safety would protect against burnout. | 2b | B |
| Grisales-Romero et al., Colombia, 2014 [38] | Cross-sectional, descriptive | k = 174 IM k = 89 SRGY k = 9 ICU k = 36 CB k = 29 OTHER k = 11 | MBI | 57 | 43 | 58 | The prevalence of burnout is higher in the study hospital than elsewhere. Male gender, multiple employment and less education are all positively associated with burnout. In IM, low PA among nurses is particularly apparent. | 2c | B |
| Jaracz et al., Poland, 2005 [39] | Cross-sectional, descriptive | k = 173 IM k = 101 | MBI | 56 | 27 | 30 | The level of stress influences burnout in nurses. The correlation between burnout and coping style is weak but statistically significant. EE is the burnout dimension that is most strongly affected in IM and neurology nurses. | 2c | B |
| NEURO k = 72 | 16 | 10 | 13 | ||||||
| Jiang et al., China, 2014 [40] | Cross-sectional, descriptive | k = 367 NEURO | MBI | 330 | 340 | 291 | Neurology nurses present high levels of burnout; D is the dimension that is most affected. Length of experience and holding a senior position both predispose nurses to abandon the profession and/or to suffer burnout. | 2c | B |
| Karakoc et al., Turkey, 2017 [41] | Cross-sectional, descriptive | k = 171 NEPHRO | MBI | - | - | - | No differences were observed between the prevalence of burnout among nephrological nurses and in other hospital services. EE and D are higher in those who wish to leave the service, those lacking training and those who have difficulty in working as a team. Male gender, youth, a lack of experience and working more than 50 h a week all predispose to D. Low PA is more evident among younger nurses. | 2c | B |
| Karkar et al., Saudi Arabia, 2012 [42] | Cross-sectional, descriptive | k = 93 NEPHRO | Modified stress and burnout questionnaires | 6 | - | - | Dialysis nurses present higher levels of burnout than other workers, due to the type of patients treated, the equipment employed and working in shifts. Verbal aggression by supervisors and/or patients contributes to a high prevalence of EE. Coping strategies should be developed. | 2c | B |
| 4 | - | - | |||||||
| Kousloglou et al., Greece, 2014 [43] | Cross-sectional, descriptive | k = 174 PSYCH k = 25 PAED k = 48 IM k = 47 SRGY k = 54 | MBI | - | - | - | An association was found between insomnia and burnout. The correlation was positive with EE and D, and negative with PA. Younger nurses, those who work more than four night shifts per month and those who work in the surgical area all experience higher levels of insomnia. | 2c | B |
| Ksiazek et al., Poland, 2011 [44] | Cross-sectional, descriptive | k = 60 ONC-HAEM | MBI | - | - | - | Levels of EE and burnout are higher in oncology nurses than in other hospital services. Psychological variables, depression and anxiety all influence the development of burnout. Decision making and greater involvement are relevant occupational factors. | 2c | B |
| Kutluturkan et al., Turkey, 2016 [45] | Cross-sectional, descriptive | k = 140 ONC-HEM | MBI | - | - | - | Greater resilience is associated with lower levels of burnout among oncology nurses. Coping styles, communication skills and social support all influence resilience and burnout. | 2c | B |
| Mealer et al., USA, 2010 [46] | Cross-sectional, descriptive | k = 332 ICU k = 98 OTHER = 74 IM k = 118 PHC k = 42 | MBI | 90 | 53 | 74 | Burnout has a dramatic effect on work-related and non-work-related perceptions. Anxiety and depression among nurses are common. MA nurses are more prone to burnout than those in other services. Of the three dimensions of burnout, EE presents the highest prevalence, followed by low PA and D. | 2c | B |
| Nowakowska et al., Poland, 2016 [47] | Cross-sectional, descriptive | k = 405 CARDIO k = 36 NEURO k = 32 ONC-HAEM k = 24 | Copenhagen Burnout Inventory | - | - | - | Organisational factors can promote professional effectiveness and efficiency, and the quality of health care provided by nurses. Those with low self-efficacy are more likely to suffer from burnout. | 2c | B |
| Neumann et al., USA, 2017 [48] | Cross-sectional, descriptive | k = 763 ONC-HAEM | MBI | 255 | 54 | 104 | Burnout is moderated by variables such as discipline and stamina. Nurses presenting burnout have a greater imbalance in their work and obtain less job satisfaction. Among the dimensions of burnout, EE is the most prominent. | 2c | B |
| Ostacoli et al., Italy, 2010 [49] | Cross-sectional, descriptive | k = 92 ONC-HAEM | MBI | 20 | 15 | 26 | There is a high prevalence of anxiety and depression among oncology nurses. EE is higher among hospital workers than in other institutions, while low PA is prevalent in both cases. Institutional factors are the main drivers of burnout, while personality variables have least impact. | 2c | B |
| 1 | 1 | 28 | |||||||
| Quattrin et al., Italy, 2006 [50] | Cross-sectional, descriptive | k = 100 ONC-HAEM | MBI | 35 | 17 | 11 | Most oncology nurses present high levels of stress and burnout, due to poor organisation of the health care institution. EE is the major burnout dimension, followed by D and low PA. Women aged over 40 years, those with more work experience and those working in the oncology service are all at higher risk of burnout. | 2c | B |
| Rodrigues et al., Brazil, 2008 [51] | Cross-sectional, descriptive | k = 77 ONC-HAEM | The Ways of Coping Questionnaire | - | - | - | The situations that predispose to burnout in oncological nurses are the deaths of patients, emergency situations and relationship problems with the nursing team. Positive coping styles are a protective factor against burnout. | 2c | B |
| Sadati et al., Iran, 2016 [52] | Cross-sectional, descriptive | k = 371 IM | MBI | - | - | - | Burnout is associated with sociodemographic and occupational risk factors. Personal reinforcement, nursing experience and rotating shift patterns are all elements that reduce burnout. | 2c | B |
| Sahraian et al., Iran, 2008 [53] | Cross-sectional, descriptive | k = 180 IM k = 44 SRGY k = 46 PSYCH k = 45 BURNS k = 45 | MBI | 3 | 1 | 1 | IM nurses experience less burnout than nurses in other services. EE is the major burnout dimension. Single status is a risk factor for burnout. Different work environments have varying degrees of impact on the development of burnout. | 2c | B |
| Sanjuán-Estallo et al., Spain, 2014 [54] | Cross-sectional, descriptive | k = 22 CARDIO k = 8 NEUMO k = 7 NEURO k = 7 | MBI | 9 | 10 | 13 | No significant differences in burnout were observed by age or among different hospital services. Neurology nurses present the same levels of burnout as other nurses in the MA. A notable prevalence of low PA was recorded in all hospital services. | 2c | B |
| Sehlen et al., Germany, 2009 [55] | Longitudinal, cohorts | k = 406 ONC-HAEM | Questionnaire for Ascertaining Stress on Doctors and Nurses and Global Job Satisfaction Questionnaire ad hoc | - | - | - | Nursing is the occupational area presenting highest levels of work-related stress and burnout. The work environment has a negative impact on the development of the syndrome. Low salaries, working night shifts and the nurse’s age all have a significant influence on burnout, as does long-term patient treatment. | 2b | B |
| Sirilla, USA, 2014 [56] | Cross-sectional, descriptive | k = 73 ONC-HAEM | Moral Distress Scale-Revised | - | - | - | High levels of burnout were recorded in oncology nurses, regardless of their experience or hospital service. The higher the level of education, the lower the degree of burnout experienced. | 2c | B |
| Wahlberg et al., USA, 2017 [57] | Cross-sectional, descriptive | k = 163 ONC-HAEM | Nurse Distress Thermometer and Occupational Coping Self-Efficacy Questionnaire for Nurses | - | - | 25 | Nurses who have active coping mechanisms are less subject to burnout. There is an inverse relationship between institutional support and burnout in oncology nurses. Low PA is the most significant dimension of burnout. | 2c | B |
| Wu et al., USA, 2017 [58] | Cross-sectional, descriptive | k = 549 ONC-HAEM | Professional Quality of Life Scale | - | - | - | A healthy working environment and institutional support are both essential to nurses’ health. Improvements in the workplace can help prevent burnout and improve health outcomes for patients. | 2c | B |
| Yu et al., China, 2016 [59] | Cross-sectional, descriptive | k = 650 ONC-HAEM | Chinese version of the Professional Quality of Life Scale for Nurses and Simplified Coping Style Questionnaire | - | - | - | Higher levels of burnout in oncology nurses were found in nurses with greater experience, those working in secondary hospitals and those with passive coping styles. The personality traits of openness and responsibility are protective against the syndrome, while neuroticism is a risk factor. | 2c | B |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Praena, J.; Ramirez-Baena, L.; Gómez-Urquiza, J.L.; Cañadas, G.R.; De la Fuente, E.I.; Cañadas-De la Fuente, G.A. Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study. Int. J. Environ. Res. Public Health 2018, 15, 2800. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122800
Molina-Praena J, Ramirez-Baena L, Gómez-Urquiza JL, Cañadas GR, De la Fuente EI, Cañadas-De la Fuente GA. Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study. International Journal of Environmental Research and Public Health. 2018; 15(12):2800. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122800
Chicago/Turabian StyleMolina-Praena, Jesús, Lucia Ramirez-Baena, José L. Gómez-Urquiza, Gustavo R. Cañadas, Emilia I. De la Fuente, and Guillermo A. Cañadas-De la Fuente. 2018. "Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study" International Journal of Environmental Research and Public Health 15, no. 12: 2800. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122800