Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Analysis
2.4. Study Quality Assessment
3. Results
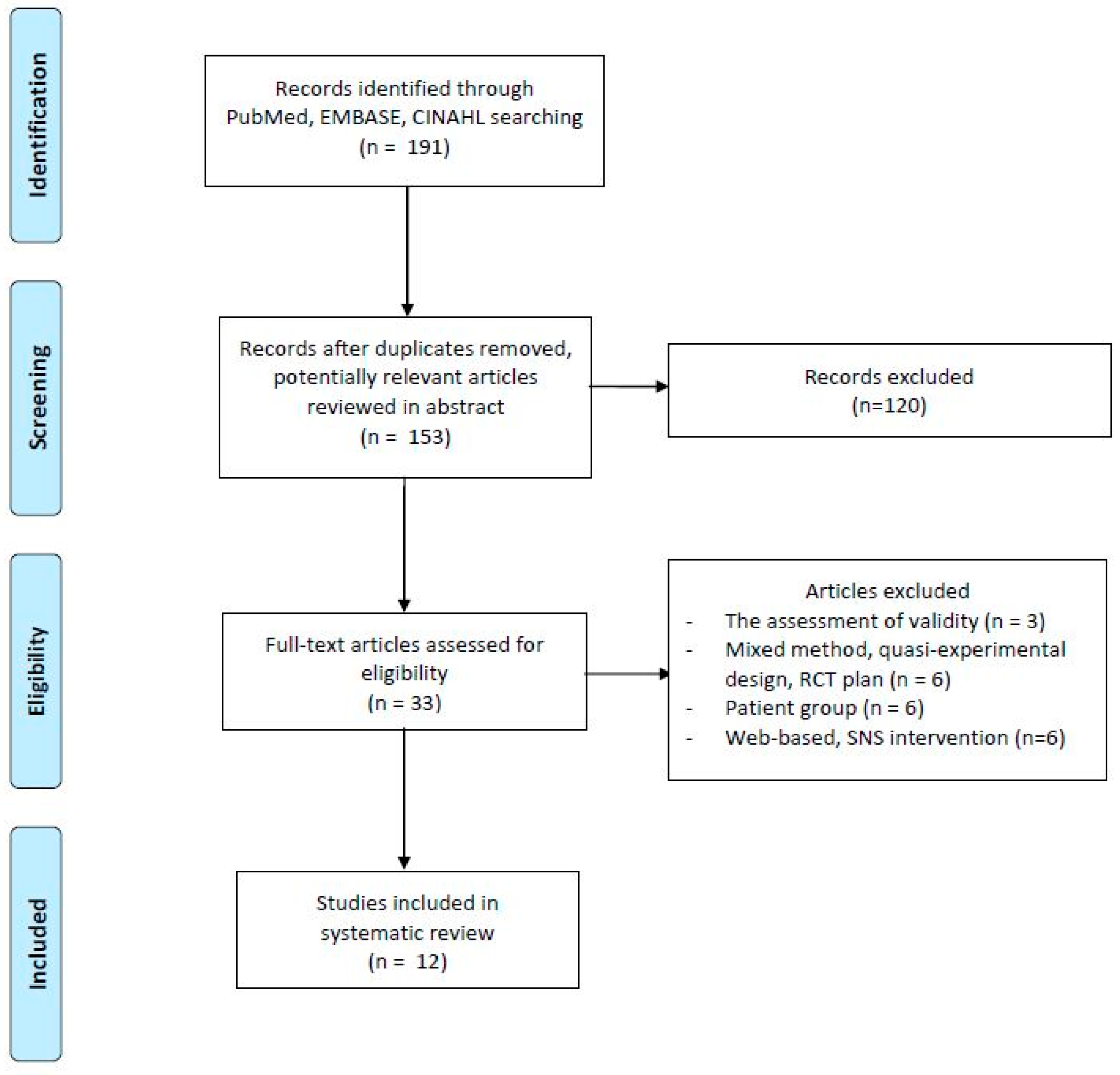
3.1. Study Selection
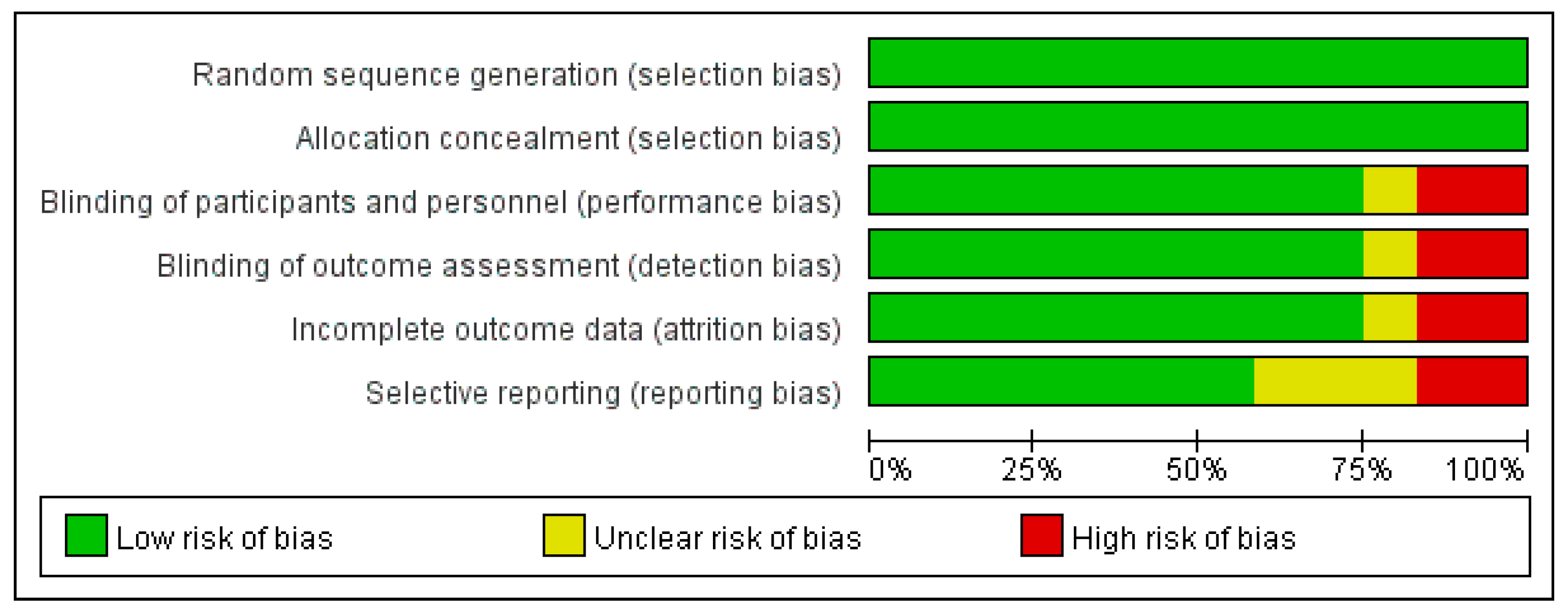
3.2. Result of Quality Assessment
3.3. General Study Characteristics
3.4. Usefulness of Mobile App-Based Health Promotion Interventions
3.4.1. Diet and Physical Activity
3.4.2. Other Health-Promoting Behaviors
3.5. Mobile App-Based Health Promotion Intervention Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Riley, W.T.; Rivera, D.E.; Atienza, A.A.; Nilsen, W.; Allison, S.M.; Mermelstein, R. Health behavior models in the age of mobile interventions: Are our theories up to the task? Transl. Behav. Med. 2011, 1, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, C.; Jackson, D. Selecting, appraising, recommending and using mobile applications (apps) in nursing. J. Clin. Nurs. 2017, 26, 3253–3255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Freeman, B.; Li, M. Can mobile phone apps influence people’s health behavior change? An evidence review. J. Med. Int. Res. 2016, 18. [Google Scholar] [CrossRef] [PubMed]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [PubMed]
- Payne, H.E.; Lister, C.; West, J.H.; Bernhardt, J.M. Behavioral functionality of mobile apps in health interventions: A systematic review of the literature. JMIR mHealth uHealth 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Mattila, E.; Orsama, A.-L.; Ahtinen, A.; Hopsu, L.; Leino, T.; Korhonen, I. Personal health technologies in employee health promotion: Usage activity, usefulness, and health-related outcomes in a 1-year randomized controlled trial. JMIR mHealth uHealth 2013, 1. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, R.; McRobbie, H.; Bullen, C.; Borland, R.; Rodgers, A.; Gu, Y. Mobile phone-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Gaziano, T.; Abrahams-Gessel, S.; Surka, S.; Sy, S.; Pandya, A.; Denman, C.A.; Mendoza, C.; Puoane, T.; Levitt, N.S. Cardiovascular disease screening by community health workers can be cost-effective in low-resource countries. Health Aff. 2015, 34, 1538–1545. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Jiang, Y.; Nguyen, H.D.; Poo, D.C.C.; Wang, W. The effect of a smartphone-based coronary heart disease prevention (SBCHDP) programme on awareness and knowledge of CHD, stress, and cardiac-related lifestyle behaviours among the working population in Singapore: A pilot randomised controlled trial. Health Qual. Life Outcomes 2017, 15, 49. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, Y.; Gay, C.L.; Joiner, K.L.; Vittinghoff, E. A novel diabetes prevention intervention using a mobile app: A randomized controlled trial with overweight adults at risk. Am. J. Prev. Med. 2015, 49, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balk-Møller, N.C.; Poulsen, S.K.; Larsen, T.M. Effect of a nine-month web-and app-based workplace intervention to promote healthy lifestyle and weight loss for employees in the social welfare and health care sector: A randomized controlled trial. J. Med. Int. Res. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Buller, D.B.; Berwick, M.; Lantz, K.; Buller, M.K.; Shane, J.; Kane, I.; Liu, X. Evaluation of immediate and 12-week effects of a smartphone sun-safety mobile application: A randomized clinical trial. JAMA Dermatol. 2015, 151, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Glynn, L.G.; Hayes, P.S.; Casey, M.; Glynn, F.; Alvarez-Iglesias, A.; Newell, J.; ÓLaighin, G.; Heaney, D.; O’Donnell, M.; Murphy, A.W. Effectiveness of a smartphone application to promote physical activity in primary care: The SMART MOVE randomised controlled trial. Br. J. Gen. Pract. 2014, 64, e384–e391. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-J.; Lee, S.-J.; Shin, N.-M.; Shin, H.; Jeon, S.; Lee, J.; Cho, I. Application and Effect of Mobiletype-Bone Health Intervention in Korean Young Adult Women with Low Bone Mass: A Randomized Control Trial. Asian Nurs. Res. 2017, 11, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.; Morrongiello, B.; Meckling, K. A randomized, controlled trial evaluating the efficacy of an online intervention targeting vitamin D intake, knowledge and status among young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 116. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.A.; Harray, A.J.; Pollard, C.M.; Dhaliwal, S.S.; Delp, E.J.; Howat, P.A.; Pickering, M.R.; Ahmad, Z.; Meng, X.; Pratt, I.S. The connecting health and technology study: A 6-month randomized controlled trial to improve nutrition behaviours using a mobile food record and text messaging support in young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Tran, R.; White, J.R. Smartphone-based glucose monitors and applications in the management of diabetes: An overview of 10 salient “apps” and a novel smartphone-connected blood glucose monitor. Clin. Diabetes 2012, 30, 173–178. [Google Scholar] [CrossRef]
- Mattila, E.; Lappalainen, R.; Pärkkä, J.; Salminen, J.; Korhonen, I. Use of a mobile phone diary for observing weight management and related behaviours. J. Telemed. Telecare 2010, 16, 260–264. [Google Scholar] [CrossRef]
- Mattila, E.; Pärkkä, J.; Hermersdorf, M.; Kaasinen, J.; Vainio, J.; Samposalo, K.; Merilahti, J.; Kolari, J.; Kulju, M.; Lappalainen, R. Mobile diary for wellness management—Results on usage and usability in two user studies. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 501–512. [Google Scholar] [CrossRef]
- Bort-Roig, J.; Gilson, N.D.; Puig-Ribera, A.; Contreras, R.S.; Trost, S.G. Measuring and influencing physical activity with smartphone technology: A systematic review. Sports Med. 2014, 44, 671–686. [Google Scholar] [CrossRef] [PubMed]
- Quanbeck, A.; Chih, M.-Y.; Isham, A.; Johnson, R.; Gustafson, D. Mobile delivery of treatment for alcohol use disorders: A review of the literature. Alcohol. Res. Curr. Rev. 2014, 36, 111–122. [Google Scholar]
- Klasnja, P.; Pratt, W. Healthcare in the pocket: Mapping the space of mobile-phone health interventions. J. Biomed. Inf. 2012, 45, 184–198. [Google Scholar] [CrossRef] [PubMed]
- Rabbi, M.; Pfammatter, A.; Zhang, M.; Spring, B.; Choudhury, T. Automated personalized feedback for physical activity and dietary behavior change with mobile phones: A randomized controlled trial on adults. JMIR mHealth uHealth 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Laing, B.Y.; Mangione, C.M.; Tseng, C.-H.; Leng, M.; Vaisberg, E.; Mahida, M.; Bholat, M.; Glazier, E.; Morisky, D.E.; Bell, D.S. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: A randomized, controlled trial. Ann. Intern. Med. 2014, 161, S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e86. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011. [Google Scholar] [CrossRef]
- Naimark, J.S.; Madar, Z.; Shahar, D.R. The impact of a Web-based app (eBalance) in promoting healthy lifestyles: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e56. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Batch, B.C.; Lin, P.-H.; Intille, S.S.; Corsino, L.; Tyson, C.C.; Bosworth, H.B.; Grambow, S.C.; Voils, C.; Loria, C. Cell phone intervention for you (CITY): A randomized, controlled trial of behavioral weight loss intervention for young adults using mobile technology. Obesity 2015, 23, 2133–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.C.; Hekler, E.B.; Grieco, L.A.; Winter, S.J.; Sheats, J.L.; Buman, M.P.; Banerjee, B.; Robinson, T.N.; Cirimele, J. Effects of three motivationally targeted mobile device applications on initial physical activity and sedentary behavior change in midlife and older adults: A randomized trial. PLoS ONE 2016, 11, e0156370. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, J.; Larsen, M.E.; Proudfoot, J.; Christensen, H. Mobile apps for bipolar disorder: A systematic review of features and content quality. J. Med. Internet Res. 2015, 17, e198. [Google Scholar] [CrossRef] [PubMed]
- Holmen, H.; Wahl, A.K.; Småstuen, M.C.; Ribu, L. Tailored communication within mobile apps for diabetes self-management: A systematic review. J. Med. Internet Res. 2017, 19, e227. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.; Young, A.; Rowntree, J.; Townsend, N.; Pearson, S.; Smith, J.; Gibson, O.; Cobern, W.; Larsen, M.; Tarassenko, L. Application of mobile phone technology for managing chemotherapy-associated side-effects. Ann. Oncol. 2007, 18, 1887–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grist, R.; Porter, J.; Stallard, P. Mental health mobile apps for preadolescents and adolescents: A systematic review. J. Med. Internet Res. 2017, 19, e176. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Kuhns, L.M. Texting and mobile phone app interventions for improving adherence to preventive behavior in adolescents: A systematic review. JMIR mHealth uHealth 2017, 5, e50. [Google Scholar] [CrossRef] [PubMed]
- Rabin, C.; Bock, B. Desired features of smartphone applications promoting physical activity. Telemed. E-Health 2011, 17, 801–803. [Google Scholar] [CrossRef]
- DeShazo, J.; Harris, L.; Turner, A.; Pratt, W. Designing and remotely testing mobile diabetes video games. J. Telemed. Telecare 2010, 16, 378–382. [Google Scholar] [CrossRef]
- Direito, A.; Jiang, Y.; Whittaker, R.; Maddison, R. Apps for improving fitness and increasing physical activity among young people: The aimfit pragmatic randomized controlled trial. J. Med. Int. Res. 2015, 17. [Google Scholar] [CrossRef]
- Whittaker, R.; Maddison, R.; McRobbie, H.; Bullen, C.; Denny, S.; Dorey, E.; Ellis-Pegler, M.; van Rooyen, J.; Rodgers, A. A multimedia mobile phone-based youth smoking cessation intervention: Findings from content development and piloting studies. J. Med. Int. Res. 2008, 10. [Google Scholar] [CrossRef] [PubMed]
- Gasser, R.; Brodbeck, D.; Degen, M.; Luthiger, J.; Wyss, R.; Reichlin, S. Persuasiveness of a mobile lifestyle coaching application using social facilitation. In International Conference on Persuasive Technology; Springer: Heidelberg/Berlin, Germany, 2006; pp. 27–38. [Google Scholar]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Consolvo, S.; McDonald, D.W.; Toscos, T.; Chen, M.Y.; Froehlich, J.; Harrison, B.; Klasnja, P.; LaMarca, A.; LeGrand, L.; Libby, R. Activity sensing in the wild: A field trial of ubifit garden. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Florence, Italy, 5–10 April 2008; ACM: New York, NY, USA, 2008; pp. 1797–1806. [Google Scholar]
- Matthews, L.; Pugmire, J.; Moore, L.; Kelson, M.; McConnachie, A.; McIntosh, E.; Morgan-Trimmer, S.; Murphy, S.; Hughes, K.; Coulman, E. Study protocol for the ‘HelpMeDoIt!’randomised controlled feasibility trial: An app, web and social support-based weight loss intervention for adults with obesity. BMJ Open 2017, 7, e017159. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Categories | n (%) |
|---|---|---|
| Type of Studies | Published journal | 12 (100.0) |
| Major field of researcher | Medicine (General, Nephrology, Dermatology) | 4 (33.3) |
| Nursing | 3 (25.0) | |
| Nutrition, Exercise and Sports | 4 (33.3) | |
| Public Health | 1 (8.4) | |
| Sample size | Under 100 | 5 (41.8) |
| 100–200 | 3 (25.0) | |
| 201–300 | 2 (16.6) | |
| Above 300 | 2 (16.6) | |
| Setting | Community | 12 (100.0) |
| No. | Author, Year [Reference] | Sample Size | App Name | Platform | App Purpose | Intervention Period (Week) | Major Outcome Indices | ||
|---|---|---|---|---|---|---|---|---|---|
| Total | Exp. | Cont. | |||||||
| 1 | Balk-Moller et al., 2017 [12] | 566 | 355 (App, E-mail, SMS, Communications in users) | 211 (None) | SoSu-life | - | - Provide information, feedback - Monitor health status | 16 | - Body weight, body fat, waist circumference, blood pressure, total cholesterol |
| 2 | Buller et al., 2015 [13] | 202 | 96 (App) | 106 (None) | Solar Cell | Android, iOS | - Provide information, feedback - Monitor behavior change | 8 | - Sun protection practices, time spent outdoors, sunburn prevalence |
| 3 | Carter et al., 2013 [30] | 128 | 43 (App, SMS, Photo) | 42 (Website), 43 (Paper diary) | My Meal Mate (MMM) | Android | - Provide feedback - Monitor behavior change - Set goal | 24 | - Body weight, BMI, body fat |
| 4 | Fukuoka et al., 2015 [10] | 61 | 30 (App, Pedometer) | 31 (Pedometer) | Mobile Phone–Based Diabetes Prevention Program (mDPP) | iOS | - Provide information - Monitor health status - Alarm on the health behavior | 20 | - Body weight, BMI, hip circumference, blood pressure, lipid profile, glucose levels, daily steps, minutes per day |
| 5 | Glynn et al., 2014 [14] | 90 | 45 (App, Call weekly) | 45 (Call weekly) | Accupedo-Pro Pedometer app | Android | - Provide information, feedback - Monitor behavior change | 8 | - Daily step count, blood pressure, resting heart rate, body weight, mental health, qualityof life |
| 6 | Goodman et al., 2016 [16] | 109 | 59 (App) | 50 (None) | Vitamin D Calculator app (VDC-app) | iOS | - Provide information, feedback | 12 | - Intake, knowledge, perceptions of vitamin D, blood concentrations of 25(OH) D3 |
| 7 | Kerr et al., 2016 [17] | 247 | 82 (Dietary feedback and weekly SMS), 83 (Dietary feedback only) | 82 (None) | Mobile food record (mFR) app | iOS | - Provide information, feedback - Monitor behavior change | 24 | - Intake of fruits, vegetables, energy-dense nutrient-poor foods and sugar-sweetened beverages, body weight, BMI |
| 8 | King et al., 2016 [32] | 95 | 22 (Social app), 24 (Affect app), 22 (Analytic app) | 27 (Control tracking diet app) | Analytically framed app, a socially framed app, an affectively framed app, or a diet-tracker control app | Android | - Monitor behavior change | 8 | - Duration of physical activity, sitting time |
| 9 | Park et al., 2017 [15] | 103 | 36 (Mobile type bone health intervention),38 (Group education only) | 29 (None) | Strong bone, Fit body (SbFb) | Android | - Provide feedback - Record | 20 | - Bone mineral density, minerals, biochemical, markers, food intake diary, knowledge, health belief, self-efficacy |
| 10 | Naimark et al., 2015 [29] | 99 | 69 (App) | 30 (None) | eBalance | web-based | - Provide information, feedback - Monitor behavior change | 14 | - Nutrition knowledge, diet quality, physical activity, weight, waist circumference |
| 11 | Svetkey et al., 2015 [31] | 365 | 122 (Cell phone), 120 (Personal coaching) | 123 (None) | CITY | Android | - Provide feedback - Monitor health status, behavior change | 24months | - Body weight |
| 12 | Zhang et al., 2017 [9] | 80 | 40 (App, SMS) | 40 (None) | Care4 Heart | Android, iOS | - Provide information | 4 | - Knowledge of coronary heart disease, perceived stress level, cardiac-related lifestyle behaviors |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122838
Lee M, Lee H, Kim Y, Kim J, Cho M, Jang J, Jang H. Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2018; 15(12):2838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122838
Chicago/Turabian StyleLee, Mikyung, Hyeonkyeong Lee, Youlim Kim, Junghee Kim, Mikyeong Cho, Jaeun Jang, and Hyoeun Jang. 2018. "Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature" International Journal of Environmental Research and Public Health 15, no. 12: 2838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122838