The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol

 , ,
, ,
Abstract
:1. Introduction
1.1. Research Questions
- Research Question (RQ) 1:How do newly arrived humanitarian migrants understand/perceive oral health?
- RQ2:Through what pathways do newly arrived humanitarian migrants access oral health care?
- RQ3:What is the oral health status of newly arrived humanitarian migrants? We hypothesize a significantly higher proportion of humanitarian migrants will have untreated dental caries compared to Canadians.
- RQ4:What are the barriers to accessing oral health services among newly arrived humanitarian migrants?
1.2. Frameworks
1.3. Preliminary Work
2. Methods and Analysis
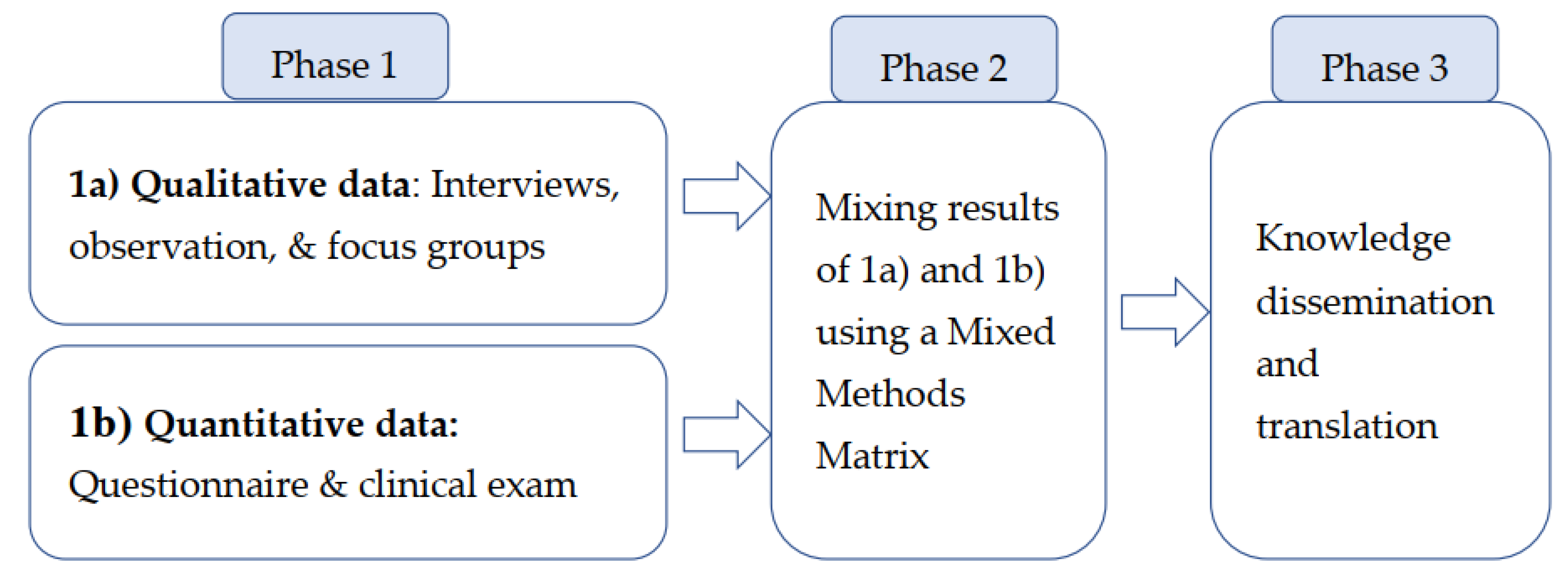
2.1. Study Design
2.1.1. Phase 1a, Focus Group Verification
2.1.2. Phase 1b, Clinical Examination and Quantitative Survey
2.2. Study Population
2.3. Sampling
2.4. Recruitment
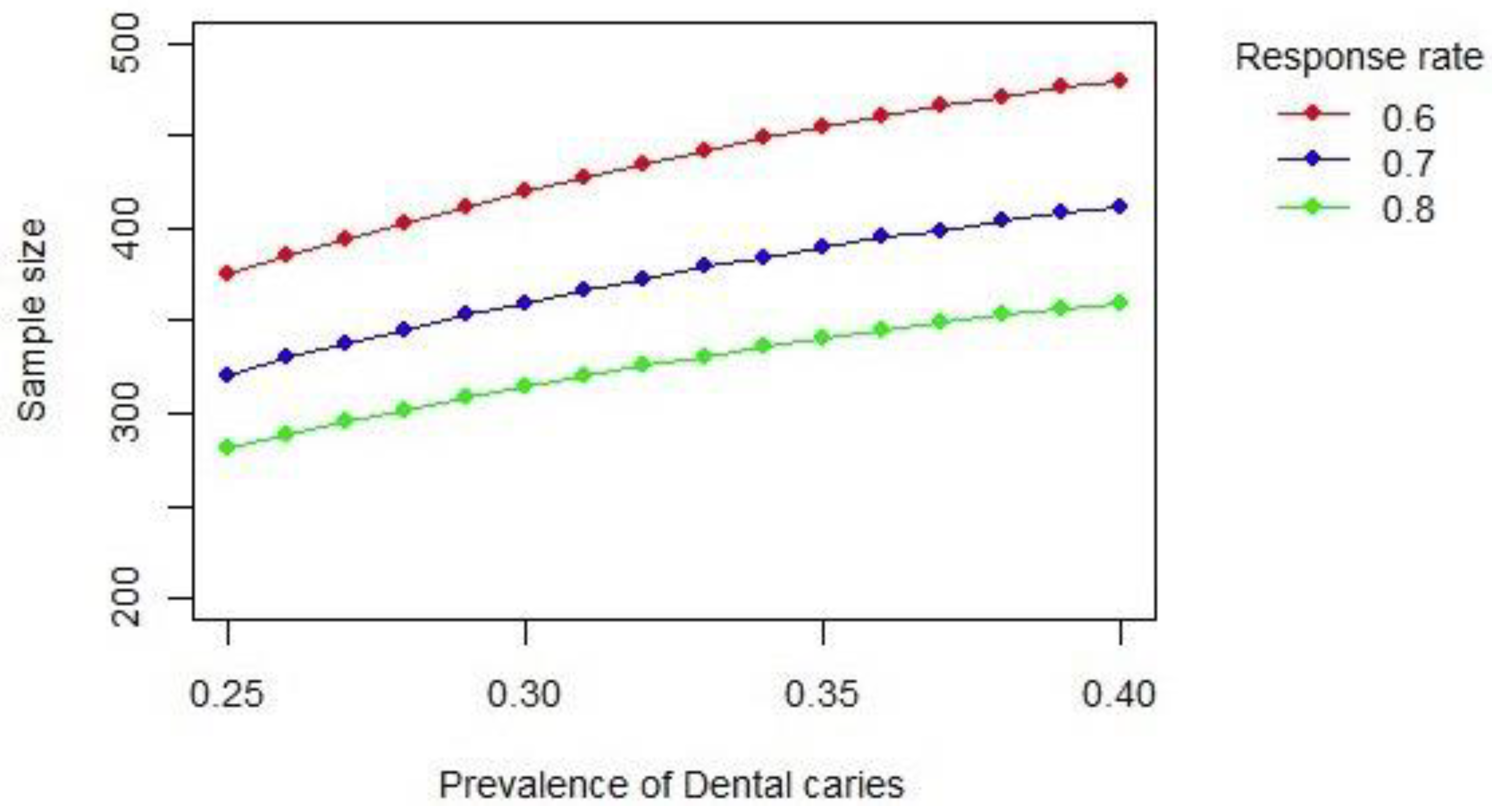
2.5. Sample Size
2.6. Ethics and Dissemination
3. Data Collection
3.1. Oral Health Status
3.2. Structured Questionnaire
3.3. Data Quality
3.4. Data Analysis
3.5. Phase 2, Mixed Methods Integration
3.6. Phase 3, Knowledge Translation and Future Directions
4. Expertise, Activities, Timeline
5. Strengths and Limitations of This Study
6. Significance
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations High Commissioner for Refugees. Global Trends: Forced Displacement in 2017; Geveva, 2017; Available online: http://www.unhcr.org/globaltrends2017/ (accessed on 3 September 2017).
- Government of Canada. Resettled Refugees: Monthly IRCC Updates. Government of Canada, 2017. Available online: http://open.canada.ca/data/en/dataset/4a1b260a-7ac4-4985-80a0-603bfe4aec11?_ga=2.36990112.1290328107.1504484075-50681910.1504484075 (accessed on 3 September 2017).
- World Health Organization. The Health of Migrants: The Way Forward. Report of a Global Consultation, Madrid, Spain, 3–5 March 2010; WHO: Geneva, Switzerland, 2010; Available online: http://www.who.int/hac/events/consultation_report_health_migrants_colour_web.pdf (accessed on 15 August 2016).
- Newbold, B. The short-term health of Canada’s new immigrant arrivals: Evidence from LSIC. Ethn. Health 2009, 14, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.L. A review on the oral health impacts of acculturation. J. Immigr. Minority Health 2011, 13, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Khoo, S.E. Health and humanitarian migrants’ economic participation. J. Immigr. Minority Health 2010, 12, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Keboa, M.T.; Hiles, N.; Macdonald, M.E. The oral health of refugees and asylum seekers: A scoping review. Glob. Health 2016, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Ghiabi, E.; Matthews, D.C.; Brillant, M.S. The oral health status of recent immigrants and refugees in Nova Scotia, Canada. J. Immigr. Minor. Health 2014, 16, 95–101. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Matthews, D.; Pottie, K.; Maze, B.; Dharamsi, S.; Swinkels, H.; Jivani, K.; Welch, V.; Ullah, A. Guidelines for Immigrant Health Appendix 16: Dental disease: Evidence review for newly arriving immigrants and refugees. Can. Med. Assoc. J. 2011, 183, E824–E925. [Google Scholar]
- Finney Lamb, C.E.; Whelan, A.K.; Michaels, C. Refugees and oral health: Lessons learned from stories of Hazara refugees. Aust. Health Rev. 2009, 33, 618–627. [Google Scholar] [CrossRef]
- Calvasina, P.; Muntaner, C.; Quinonez, C. The deterioration of Canadian immigrants’ oral health: Analysis of the Longitudinal Survey of Immigrants to Canada. Community Dent. Oral Epidemiol. 2015, 43, 424–432. [Google Scholar] [CrossRef] [PubMed]
- King, C. Understanding the Oral Health Needs of Government Assisted Refugees; Simon Fraser University: Vancouver, BC, Canada, 2012. [Google Scholar]
- Butani, Y.; Weintraub, J.; Barker, J.C. Oral health-related cultural beliefs for four racial/ethnic groups: Assessment of the literature. BMC Oral Health 2008, 8, 26. [Google Scholar] [CrossRef]
- Prowse, S.; Schroth, R.J.; Wilson, A.; Edwards, J.M.; Sarson, J.; Levi, J.A.; Moffatt, M.E. Diversity considerations for promoting early childhood oral health: A pilot study. Int. J. Dent. 2014. [Google Scholar] [CrossRef]
- Garcia, I.; Tabak, L. Global oral health inequalities: The view from a research funder. Adv. Dent. Res. 2011, 23, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Gelberg, L.; Andersen, R.M.; Leake, B.D. The Behavioral Model for Vulnerable Populations: Application to medical care use and outcomes for homeless people. Health Serv. Res. 2000, 34, 1273–12302. [Google Scholar] [PubMed]
- Muirhead, V.E.; Quinonez, C.; Figueiredo, R.; Locker, D. Predictors of dental care utilization among working poor Canadians. Community Dent. Oral Epidemiol. 2009, 37, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.R. Applying Andersen’s behavioural model to oral health: What are the contextual factors shaping perceived oral health outcomes? Community Dent. Oral Epidemiol. 2009, 37, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Canadian Health Measures Survey (CHMS) Data User Guide: Cycle 1. Ottawa, 2011. Available online: http://www23.statcan.gc.ca/imdb-bmdi/pub/document/5071_D2_T1_V1-eng.htm (accessed on 13 August 2017).
- Sabbahi, D.A.; Lawrence, H.P.; Limeback, H.; Rootman, I. Development and evaluation of an oral health literacy instrument for adults. Community Dent. Oral Epidemiol. 2009, 37, 451–462. [Google Scholar] [CrossRef]
- Groleau, D.; Young, A.; Kirmayer, L.J. The McGill Illness Narrative Interview (MINI): An interview schedule to elicit meanings and modes of reasoning related to illness experience. Transcult. Psychiatry 2006, 43, 671–691. [Google Scholar] [CrossRef] [PubMed]
- Keboa, M.T. Understanding Oral Health and Dental Care Pathways of Refugees and Asylum Seekers in Montreal; Manuscript-Based; McGill University: Montreal, QC, Canada, 2017. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative and Mixed Methods Approaches; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Wisdom, J.P.; Cavaleri, M.A.; Onwuegbuzie, A.J.; Green, C.A. Methodological reporting in qualitative, quantitative, and mixed methods health services research articles. Health Serv. Res. 2012, 47, 721–745. [Google Scholar] [CrossRef]
- Nicolau, B.; Castonguay, G.; Levine, A.; Hong, Q.N.; Pluye, P.; Afrashtehfar, K.I.; Al-Sahan, M.; Amin, M.; Benbow, P.; de Oliveira, A.C.B.; et al. Applied Mixed Methods in Oral Health Research: Importance and Example of a Training Program. JDR Clin. Transl. Res. 2017, 2, 206–210. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research; Sage: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Vang, Z.M.; Sigouin, J.; Flenon, A.; Gagnon, A. Are immigrants healthier than native-born Canadians? A systematic review of the healthy immigrant effect in Canada. Ethn. Health 2017, 22, 209–241. [Google Scholar] [CrossRef]
- Font, J.; Méndez, M. Surveying Ethnic Minorities and Immigrant Populations: Methodological Challenges and Research Strategies; IMISCOE; Amsterdam University Press: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Merry, L.; Gagnon, A.; Hemlin, I.; Clarke, H.; Hickey, J. Cross-border movement and women’s health: How to capture the data. Int. J. Equity Health 2011, 10, 56. [Google Scholar] [CrossRef]
- Salganik, M.J.; Heckathorn, D.D. Sampling and estimation in hidden populations using Respondent-Driven Sampling. Sociol. Methodol. 2004, 34, 193–240. [Google Scholar]
- Salganik, M.J. Variance estimation, design effects, and sample size calculations for respondent-driven sampling. J. Urban Health 2006, 83, i98–i112. [Google Scholar] [CrossRef] [PubMed]
- Cornfield, J. The determination of sample size. Am. J. Public Health 1951, 41, 654–661. [Google Scholar] [CrossRef]
- Melzack, R. The short-form McGill Pain Questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Strohschein, F.J.; Merry, L.; Thomas, J.; Gagnon, A.J. Strengthening data quality in studies of migrants not fluent in host languages: A Canadian example with reproductive health questionnaires. Res. Nurs. Health 2010, 33, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Vrieze, S.I. Model selection and psychological theory: A discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol. Methods 2012, 17, 228–243. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Three techniques for integrating data in mixed methods studies. BMJ 2010, 341, c4587. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Interpretation of ‘Barriers’ | ||
Using data from:
| ||
| What = identification of what barriers exist. How = examining how barriers operate. | ||
| Relevant actual qualitative results (How) | Relevant hypothetical quantitative results (What) | Hypothetical integration: Convergence, complementarity, divergence, uniqueness |
| Low importance of oral health in cultures of origin; yet, participants were aware of the importance of good oral health to their wellbeing | n/a | Unique to qualitative: Qualitative data highlights how culturally specific views affect care seeking. Important for culturally attuned service development. Could be used in future survey research? |
| Lack of finances and lack of dental insurance were the main issues that prevented participants from seeking dental care. | Lack of finances/insurance associated with care avoidance | Convergence and uniqueness: Quantitative data suggests a possible connection between financial factors and the social process of stigmatization, both of which impede access to oral health care. Could follow up with this in the verification focus groups. |
| Stigma/fear associated with care avoidance | ||
| Oral health was a priority for participants, possibly resulting from disease experience | Lack of time/availability associated with low care seeking | Divergence; to discuss with larger team |
| Oral disease impacts were prevalent and limited daily functions of participants | Mobility/health keeps some people from seeking care | Convergence; this seems especially important for service planning. |
| Participants felt community organizations were useful for finding a dentist who would accept to provide care despite their financial limitations | Lack of awareness of resources represents a common reason for not seeking care. | Divergence; Hypothesis: Perhaps sampling bias in qualitative sample? |
| Observations revealed that language constituted a barrier during episodes of care | Language prevents people from seeking care | Convergence (language) and uniqueness (race) |
| Overall, participants felt they could use public transport systems well | Transportation represents a common reason for avoiding care | Divergence (return to data to re-assess) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macdonald, M.E.; Keboa, M.T.; Nurelhuda, N.M.; Lawrence, H.P.; Carnevale, F.; McNally, M.; Singhal, S.; Ka, K.; Nicolau, B. The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol. Int. J. Environ. Res. Public Health 2019, 16, 542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040542
Macdonald ME, Keboa MT, Nurelhuda NM, Lawrence HP, Carnevale F, McNally M, Singhal S, Ka K, Nicolau B. The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol. International Journal of Environmental Research and Public Health. 2019; 16(4):542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040542
Chicago/Turabian StyleMacdonald, Mary Ellen, Mark T. Keboa, Nazik M. Nurelhuda, Herenia P. Lawrence, Franco Carnevale, Mary McNally, Sonica Singhal, Khady Ka, and Belinda Nicolau. 2019. "The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol" International Journal of Environmental Research and Public Health 16, no. 4: 542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040542