Benefits of Advanced Practice Nursing for Its Expansion in the Spanish Context

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Background
1.2. International Context
- Shortage of primary care physicians, mainly in remote and rural areas.
- Constant changes in the population’s health needs related to the increase of chronic diseases and population ageing.
- The need for improving the quality and continuity of assistance.
- To improve career prospects for nurses.
- Demand from the nursing associations.
- Patient support.
- Governments’ support by means of legislative changes and financing.
- Education systems’ capacity to train nurses for more advanced roles.
- Positive attitude of health managers.
1.3. Spanish Context
1.4. APN Competencies
- Advanced Clinic: patients’ first contact with the system, either by telephone assistance, emergencies, or planned appointments for patients with minor health problems. Some of these demands can be answered with health advice or specific indications, or with the prescription of drugs. In other more acute cases, the need for other diagnostic tests, further monitoring of the process, or referral to other professionals may be needed. The APN can also interpret the results and make clinical judgments both autonomously and jointly with other team members. This offers high autonomy in the chronic patient management and avoids unnecessary referrals and potential complications. The prescribing authority allows the APN to start a specific treatment or renew a previous one within their specific group of patients.
- Management: a management procedure that allows the APN to refer to socio-health professionals, and vice versa.
- Teaching: active participation in training programmes for nursing students and registered nurses.
- Research: evidence-base facilitator, elaborating evidence-based recommendations, protocol development and clinical practice guidelines, and taking part in the design of quality standards and indicators, and in patients’ assessment and safety.
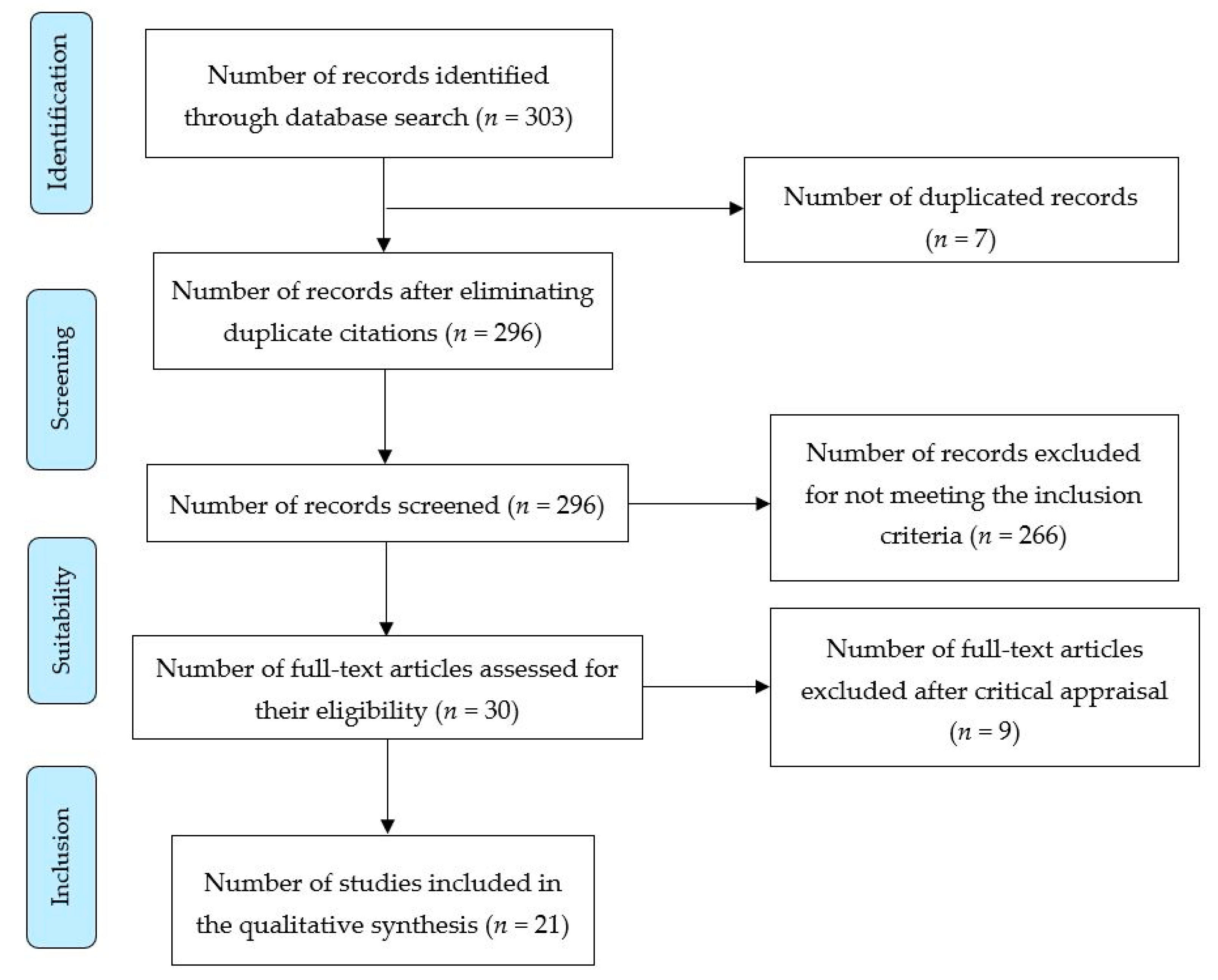
2. Materials and Methods
3. Results
3.1. Quality of Life
3.2. Cost-Effectiveness
3.3. Health Outcomes
3.4. Satisfaction
3.5. Accessibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Council of Nurses. Nurse Practitioner and Advanced Practice Nursing. Definition and Characteristics of the Role. 2013. Available online: https://international.aanp.org/Practice/APNRoles (accessed on 3 January 2019).
- Appleby, C.; Camacho-Bejarano, R. Challenges and opportunities: Contributions of the Advanced Practice Nurse in the chronicity. Learning from experiences. Enferm. Clin. 2014, 24, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Morales-Asencio, J.M. Barreras para la implementación de modelos de práctica avanzada en España. Metas Enferm. 2012, 15, 26–32. [Google Scholar]
- De Pedro, J.E. ¿Quién demanda una práctica de cuidados avanzados? Evidentia 2006, 3. Available online: http://www.index-f.com/evidentia/n11/248articulo.php (accessed on 3 January 2019).
- Sánchez-Martín, C.I. Chronic diseases and complexity: New roles in nursing. Advanced practice nurses and chronic patient. Enferm. Clin. 2014, 24, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Advanced Practice Registered Nurses Consensus Work Group & the National Council of State Boards of Nursing APRN Advisory Committee. Consensus Model for Advanced Practice Registered Nurses (APRN) Regulation: Licensure, Accreditation, Certification & Education. APRN Joint Dialogue Group Report. Available online: Ttps://www.ncsbn.org/Consensus_Model_for_APRN_Regulation_July_2008.pdf (accessed on 7 July 2008).
- San, L.M.R. Advanced practice in nursing and new organizational healthcare models. Enferm. Clin. 2016, 26, 155–157. [Google Scholar]
- Canadian Nurses Association. Advanced Nursing Practice. Position Statement. Available online: https://www.cna-aiic.ca/-/media/cna/page-content/pdf-en/ps60_advanced_nursing_practice_2007_e.pdf? la=en&hash= FAAD706F3BC50ACEBC457888837B9437CA59EE14 (accessed on 3 January 2019).
- Camacho-Bejarano, R.; Rodríguez-Gómez, S.; Gómez-Salgado, J.; Lima-Serrano, M.; Padín-López, S. Quality, accessibility and sustainability: Keys for Advanced Nursing Practice in Spain. Enferm. Clin. 2015, 25, 221–222. [Google Scholar] [PubMed]
- Delamaire, M.; Lafortune, G. Nurses in Advanced Roles. A Description and Evaluation of Experiences in 12 Developed Countries. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/docserver/5kmbrcfms5g7-en.pdf?expires=1551130320&id=id&accname=guest&checksum=3950870ACFB7E5EFC7F4F1595279E76F (accessed on 25 February 2019).
- Goodman, C.; Morales Asensio, J.M.; de la Torre-Aboki, J. La contribución de la enfermera de Práctica Avanzada como respuesta a las necesidades cambiantes de salud de la población. Metas Enferm. 2013, 16, 20–25. [Google Scholar]
- Hutchinson, M.; East, L.; Stassa, H.; Jackson, D. Deriving consensus on the characteristics of advanced practice nursing. Meta-summary of more than 2 decades of research. Nurs. Res. 2014, 62, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Hamric, A.B.; Spross, J.A.; Hanson, C.M. Advanced Practice Nursing: An Integrative Approach; Elsevier: Saunders, Hong Kong, 2014. [Google Scholar]
- Hernández Yáñez, J.F. La Enfermería Frente al Espejo: Mitos y Realidades. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=3717836 (accessed on 3 January 2019).
- Jones, D.A. La Novedosa Aportación de la Enfermería Clínica Avanzada. Available online: http://www.google.es/url?url=http://www.cun.es/dms/cun/revista-noticiasCUN/resumenes/80/42_firma_invitada_0.pdf&rct=j&frm=1&q=&esrc=s&sa=U&ved=0CBwQFjABahUKEwiGiOWfxvHGAhVENxQKHRtjA3Q&usg=AFQjCNGtvPImjQxHarBwrTLul2dV5qi-Nw (accessed on 3 January 2019).
- Clínica Universitaria de Navarra. Incorporación de la Evidencia Científica a la Práctica, Calidad Asistencial y Seguridad del Paciente, Principales Aportaciones de la Enfermera Clínica Avanzada. 2012. Available online: http://www.cun.es/actualidad/noticias/calidad-asistencial-enfermeria-clinica-50-aniversario (accessed on 3 January 2019).
- Universidad de Navarra. Máster en Práctica Avanzada y Gestión en Enfermería. 2015. Available online: http://www.unav.edu/web/master-en-practica-avanzada-y-gestion-en-enfermeria/presentacion (accessed on 3 January 2019).
- National Organization of Nurse Practitioner Faculty. Nurse Practitioner Core Competences Content. 2017. Available online: Https://cdn.ymaws.com/www.nonpf.org/resource/resmgr/competencies/2017_NPCoreComps_with_Curric.pdf (accessed on 3 January 2019).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Cabello, J.B. Lectura Crítica de la Literatura Médica; Elsevier: Barcelona, Spain, 2015. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews: The PRISMA Statement. PLoS Med. 2009, 6, E1000097. [Google Scholar] [CrossRef] [PubMed]
- Laurant, M.G.; Hermens, R.P.; Braspenning, J.C.; Sibbald, B.; Grol, R.P. Impact of nurse practitioners on workload of general practitioners: Randomized control trial. BMJ 2004, 328, 927. [Google Scholar] [CrossRef] [PubMed]
- Kuethe, M.C.; Vaessen-Verberne, A.A.P.H.; Elbers, R.G.; Van Aalderen, W.M.C. Nurse versus physician-led care for the management of asthma (Review). Cochrane Database 2013, 19. [Google Scholar] [CrossRef]
- Taylor, S.J.; Candy, B.; Bryar, R.M.; Ramsay, J.; Vrijhoef, H.J.M.; Esmond, G.; Griffiths, C.J. Effectiveness of innovations in nurse led chronic disease management for patients with chronic obstructive pulmonary disease: Systematic review of evidence. BMJ 2005, 331, 485. [Google Scholar] [CrossRef] [PubMed]
- Donald, F.; Martin-Misener, R.; Carter, N.; Donald, E.E.; Kaasakainen, S.; Wickson-Griffiths, A.; Lloyd, M.; Akhtar-Danesh, N.; DiCenso, A. A systematic review of the effectiveness of advanced practice nurses in long-term care. J. Adv. Nurs. 2013, 69, 2148–2161. [Google Scholar] [CrossRef] [PubMed]
- Ortún, V. Nursing in the world to come. Enferm. Clin. 2013, 23, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Brooten, D.; Naylor, M.D.; York, R.; Brown, L.P.; Munro, B.H.; Hollingsworth, A.O.; Cohen, S.M.; Finkler, S.; Deatrick, J.; Youngblut, J.M. Lessons Learned from Testing the Quality Cost Model of Advanced Practice Nursing (APN) Transitional Care. J. Nurs. Sch. 2002, 34, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Ishani, A.; Greer, N.; Taylor, B.C.; Kubes, L.; Cole, P.; Atwood, M.; Clothier, B.; Ercan-Fang, N. Effect of nurse case management compared with usual care on controlling cardiovascular risk factors in patients with diabetes. Diabetes Care 2011, 34, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- Chouinard, M.C.; Hudon, C.; Dubois, M.F.; Roberge, P.; Loignon, C.; Tchouaket, E.; Fortin, M.; Couture, E.-M.; Sasseville, M. Case management and self-management support for frequent users with chronic disease in primary care: A pragmatic randomized controlled trial. BMC Health Serv. Res. 2013, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Eficacia de las Enfermeras de Práctica Avanzada (EPA) en Centros de Atención a Personas Mayores. Available online: http://www.evidenciaencuidados.es/BPIS/PDF/2010_14_19_BestPrac.pdf (accessed on 29 May 2012).
- Oeseburg, B.; Wynia, K.; Middel, B.; Rejineveld, S. Effects of case management for frail older people or those with chronic illness: A systematic review. Nurs. Res. 2009, 58, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Dierick-Van Daele, A.T.M.; Metsemakers, J.F.M.; Derckx, E.W.C.C.; Spreeuwenberg, C.; Vrijhoef, H.J.M. Nurse practitioners substituting for general practitioners: Randomized controlled trial. J. Adv. Nurs. 2008, 65, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Kinnersley, P.; Anderson, E.; Parry, K.; Clement, J.; Archard, L.; Turton, P.; Rogers, C. Randomised controlled trial of nurse practitioner versus general practitioner care for patients requesting “same day” consultations in primary care. BMJ 2000, 320, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Horrocks, S.; Anderson, E.; Salisbury, C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ 2002, 324, 819–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Countries | Date of Implementation | Institutional Support | APN Categories | Educational Level | Diagnostic Tests Prescription Competence | Medical Prescription Competence | Specialist Referral Competence |
|---|---|---|---|---|---|---|---|
| Australia | 1990s | stralian Nursing and Midwifery Council, (ANMC) | NP | Degree Master | yes | yes | yes |
| Belgium | No | APN | Degree Master | yes | |||
| Canada | 1960s | Yes | NP/CNS | Degree | yes | yes | yes |
| Cyprus | Yes | Diabetic Nurse CMHN MHN Community Nurse | Postgraduate | ||||
| Czech Republic | Now | Yes | SN | Clinic Master Specialty | yes | no | |
| Finland | Yes | Public health nurse. Chronic patients nurse manager. Acute health issues nurse. | Postgraduate | yes | yes | ||
| France | HPST law | Expert nurse: AP/Home chemotherapy/Haemodialysis/Hepatitis C/Neuro-oncological link/Gastrointestinal examination/Blood donation. | Postgraduate Master | yes | |||
| Ireland | 1990s | NCNM legislation | CNS/APN | Specialty postgraduate Master | yes | yes | |
| Japan | now | yes | APN Specialist | 5 years of specialty clinical practice and 3 specific years | |||
| Poland | now | yes | APN | yes | no | ||
| United Kingdom | 1970s | yes | CNS/ANP/Nurse consultant/Modern Matrons/Community matrons | Graduate and experience in the specialty. Postgraduate Master | yes | yes | yes |
| USA | 1960s | yes | APRN/CNS/CRNA/CNM/CNP/NP | Graduate Postgraduate | yes | yes | yes |
| Author, Year, Country, Study Design | Critical Appraisal (CASPe Score) | Aim | Results |
|---|---|---|---|
| Appleby & Camacho-Bejarano, 2014 [2], Spain, Narrative review | 5 | To analyse APN as a suitable strategy to obtain the best outcomes in terms of overall health and quality of life of patients with chronic conditions. | APN contribution to chronic patients’ management: health outcomes, coordination/team work, service quality, patient interaction-relation. |
| Morales Asencio, 2012 [3], Spain, Narrative review | 5 | Analysis of the different conceptual, regulative, legislative, and competence barriers, as well as organisational and professional ones, that Spanish nursing is facing in its new consolidation of roles. | Five big barriers were identified: difficulties in the conceptualisation and regulation n of the APN, professional interests, service organisational characteristics, training, and professional competitiveness. In the Spanish context, APN follows disparate guidelines of the Regional Governments. |
| De Pedro, 2006 [4], Spain, Qualitative study | 5 | Comprehensive analysis of the reality concerning the social demand of care, how social changes interfere with this demand, and of our ability to address it as a collective. | The first step must be a debate with the academic area, where a readjustment of the educational training and a redefinition of competencies must be done. All the more, care provision progressively requires a complexity that justifies advanced and specialised practice. We need leaders who are capable of combining the strategic vision, the precise knowledge of our abilities, and the society needs. The application and management of the Specialisation Law places us in the need for a regulation for advanced practice. |
| Sánchez-Martín, 2014 [5], Spain, Narrative review | 5 | To describe the need to reorganise and reinforce PC teams so that this area deals with chronic patients and their home comprehensive care. | APN is cost-effective and highly conclusive. It improves assistance quality and coordination with the social and health sector, decreases emergency admissions in complex patients with multiple illnesses, and improves assistance satisfaction. |
| Delamaire & Lafortune, 2010 [10], France, Systematic review | 8 | To review the evolution of the APN in 12 countries with a special emphasis on primary care functions. To review the assessment of the impact on patients’ care and on costs. | The APN can improve the access to services and reduce waiting times. They are able to offer the same quality care as physicians for specific types of patients, including those with minor ailments and those who need monitoring. A higher level of patients’ satisfaction. |
| Goodman et al., 2013 [11], Narrative review | 5 | To highlight the added benefits that the APN brings to both patients and their families in those centres with these resources, as opposed to those which provide traditional assistance. | The functions of APN are safe and as effective as those of physicians. In addition, they achieve a high level of patients’ satisfaction compared to that obtained by physicians. The APN services contribute to a neutral cost, facilitate hospitalisation costs and the use of the emergency services and, at the same time, improve the access to specific services. |
| Hernández Yáñez, 2010 [14], Spain, Narrative review | 5 | To contextualise and document the current situation of nursing in industrialised countries, with a particular focus on Spanish nursing. | The CPN is valued very positively, both for its rationalisation of qualified human resources, as well as for its contribution to financial efficiency and its impact on care quality and safety. |
| Laurant et al., 2004 [22], UK, Randomised clinical trial | 10 | To evaluate general physicians’ burden when adding a NP to their team. | The number of out-of-hours consultations in the NP intervention group was reduced. The addition of the NP to general medical teams reduced the workload, at least, in the short term. This implies that the NP is used as a complement, instead of as a replacement. |
| Kuethe, Vaessen-Verberne, Elbers & Van Aalderen, 2013 [23], Netherlands, Systematic review | 9 | To review the effectiveness of asthma care provided by nurses specialised in asthma, a NP, a medical assistant, or a professional nurse specialised in other areas working independently, as opposed to the traditional care given by a physician, both in hospitals and in PC. | There were no statistical differences in the number of asthma exacerbations and in the acuteness of the same after the treatment. Only one research had the outcome parameter of health costs, not finding statistically significant differences. |
| Taylor et al., 2005 [24], UK, Systematic review | 9 | To determinate the effectiveness of innovations in the development of chronic illness implying nurses’ actions with COPD patients. | Long-term interventions did not improve the patients’ health as for their psychological welfare, impairment, or lung function. A greater control of the symptoms and a decrease of the exacerbations is highlighted, although the results are not always conclusive. |
| Donald et al., 2013 [25], Canada, Systematic review | 8 | To deliver quantitative evidence of the effectiveness of the APN functions, specialists in clinical nursing, and nurses in meeting the health needs of older adults who live in long-term care homes. | Long-term care homes with APNs had lower rates of urine incontinence, pressure ulcers, and aggressive behaviour. Most residents experienced improvements in the achievement of personal goals and a higher level of satisfaction of the families. The APN is associated with improvements in several health status situations and in the behaviour of residents in long-term stays, as well as a higher level of satisfaction of the families. |
| Brooten et al., 2002 [27], USA, Systematic review | 7 | To describe the development of the Quality Cost Model of APN in transitional care of patients’ evolution and health assistance in the US for 22 years. To formulate what has been learnt about the evolution of nursing, its practice, and additional research. | Patients’ improvement and costs reduction in all groups that worked with APN. Time reduction in re-hospitalisations due to an early intervention and detection. |
| Ishani et al., 2011 [28], USA, Randomised clinical trial | 11 | To determine if the nurse case manager with a therapeutic algorithm can effectively improve the control rates for arterial hypertension, hyperglycaemia, and hyperlipidaemia, in contrast with the assistance received among the diabetes veterans. | A greater number of people assigned to case management achieved the results of having all outcome measures under control. In addition, they achieved the goals of individual treatment. |
| Chouinard et al., 2013 [29], UK, Cases and control study | 8 | Analysis of the efficiency and cost-effectiveness of the intervention in patients with chronic diseases who perform numerous visits to hospital services. This combines the management of cases by a nurse and the promotion of self-management. | The integration of a nurse case manager intervention and of the self-management group for primary care practices have the potential to positively impact on the patients’ improvement and their quality of life. The health care workload is expected to be reduced. |
| Joanna Briggs Institute, 2010 [30], Systematic review | 9 | To present the best evidence available of the APN role in elderly care homes. | Statistically significant decrease in emergency visits and lower rate of hospitalisation when the APN was integrated into the medical team. Implementation of APN as a supplier of primary care to reduce the use of acute assistance services to elderly people in elderly care homes. |
| Oeseburg, Wynia, Middel & Rejineveld, 2009 [31], Netherlands, Systematic review | 9 | To evaluate the effect of case management in the patients’ use of the health services and in health costs for older patients with mayor impairments or adults with chronic somatic illnesses that live in the community. | No research showed a relevant clinical increase of the use of services and of costs, whereas two researches showed that case management reduced the use of health services and was more cost-effective. The implementation of case management should be prioritised for patients with chronic illnesses and for older handicapped people. |
| Dierick-van Daele, Metsemaker, Derckx, Spreeuwenberg & Vrijhoef, 2009 [32], Netherlands, Randomised clinical trial | 10 | To evaluate the process and the results in the assistance provided to patients with common complaints by general nurses or specifically trained nurses (NP) as a first point of contact. | In both groups, the patients appreciated the quality of the assistance provided. There were no statistically significant differences in their health status, use of the medical resources, and the commitment to PC practical guidelines. Patients in the NP intervention group were more frequently asked to visit again, had more monitoring consultations, and these were significantly longer. |
| Kinnersley et al., 2000 [33], UK, Randomised clinical trial | 10 | To identify the differences between the NP and the general practitioner assistance for patients who ask for immediate consultations in primary care. | The NP consultations were longer and the patients confirmed to have been better assisted and informed. This is associated with a greater level of satisfaction. |
| Horrocks, 2002 [34], UK, Systematic review | 9 | To determine if NPs can provide first level contact assistance in a primary care centre. | Patients were more satisfied with the care provided by the NP. No differences were found in their health status. The NP had longer consultations and did more research than physicians. The NP quality of assistance was somehow better. |
| Advantages of APN Interventions | Clinical Research | Systematic Review | Case/Control | Narrative Reviews | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 22 | 28 | 32 | 33 | 27 | 34 | 10 | 23 | 24 | 31 | 25 | 29 | 2 | 5 | 26 | 11 | 14 | |
| Improve the control of cardiovascular risk factors in diabetes patients for a year. | 1c/A | ||||||||||||||||
| Obtain as good health outcomes and quality of assistance as physicians. | 1c/A | 1c/A | 1b/A | 1c/A | 1c/A | 1b/A | 1c/A | 1c/A | |||||||||
| Increase patients’ satisfaction with quality of service. | 1c/A | 1c/A | 1b/A | 1c/A | 1c/A | 1a/A | 1a/A | 1c/A | 1c/A | 1c/A | |||||||
| Closer patients’ follow-up. | 1c/A | 1c/A | 1c/A | 1c/A | 1c/A | ||||||||||||
| Longer time duration of consultations. | 1c/A | 1c/A | 1c/A | 1c/A | 1c/A | ||||||||||||
| More detailed information received by patients. | 1c/A | 1c/A | 1c/A | 1c/A | 1c/A | 1c/A | |||||||||||
| Positive impact on patients’ empowerment, health outcomes and quality of life. | 5/B | 3b/B | 3b/B | 5/B | 5/B | 5/B | |||||||||||
| Greater control of symptoms and a decrease of exacerbations in respiratory processes. | 1a/A | 1a/A | |||||||||||||||
| Decrease of hospital admissions, re-hospitalisation and hospital length of stay. | 2b/A/B | 1a/A | 1a/A | 1a/A | 2b/A/B | 2b/A/B | 2b/A/B | 1a/A | 1a/A | ||||||||
| Better management ability and commitment in patients with COPD. | 1a/A | 1a/A | 1a/A | 1a/A | |||||||||||||
| Reduces costs in health services | 1b/A | 1b/A | 1b/A | 1a/A | 1a/A | 1a/A | 1a/A | 2b/A/B | 1a/A | 1a/A | 2b/A/B | 1a/A | 5/B | ||||
| Earlier detection of patients’ problems. | 1a/A | 1a/A | 1a/A | 1a/A | 1a/A | ||||||||||||
| Improves the access to services and provision of care. | 1b/A | 1b/A | 1b/A | 2b/A/B | 1b/A | 2b/A/B | 2b/A/B | 2b/A/B | 2b/A/B | 1b/A | 2b/A/B | 1b/A | 5/B | ||||
| Reduces waiting list. | 1b/A | 1b/A | 1b/A | 1b/A | 1b/A | 1b/A | |||||||||||
| Greater satisfaction of patients’ relatives. | 3b/B | 3b/B | |||||||||||||||
| Better team work coordination | 5/B | 5/B | 5/B | 5/B | |||||||||||||
| Improve interaction/relationship with chronic patients. | 5/B | 5/B | 5/B | 5/B | |||||||||||||
| Supports sustainability of the services. | 5/B | 5/B | 5/B | 5/B | 5/B | 5/B | 5/B | 5/B | 5/B | ||||||||
| Effectiveness from the patients and the organisation’s perspective. | 5/B | ||||||||||||||||
| Greater balance between needs and resources. | 5/B | ||||||||||||||||
| Increase the capacity of problem-solving. | 5/B | 5/B | 5/B | 5/B | 5/B | ||||||||||||
| Care provision practice requires a complexity that justifies an advanced or specialised practice. | 5/B | ||||||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Gómez, M.B.; Ramos-Santana, S.; Gómez-Salgado, J.; Sánchez-Nicolás, F.; Moreno-Garriga, C.; Duarte-Clíments, G. Benefits of Advanced Practice Nursing for Its Expansion in the Spanish Context. Int. J. Environ. Res. Public Health 2019, 16, 680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050680
Sánchez-Gómez MB, Ramos-Santana S, Gómez-Salgado J, Sánchez-Nicolás F, Moreno-Garriga C, Duarte-Clíments G. Benefits of Advanced Practice Nursing for Its Expansion in the Spanish Context. International Journal of Environmental Research and Public Health. 2019; 16(5):680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050680
Chicago/Turabian StyleSánchez-Gómez, María Begoña, Sara Ramos-Santana, Juan Gómez-Salgado, Francisca Sánchez-Nicolás, Carlos Moreno-Garriga, and Gonzalo Duarte-Clíments. 2019. "Benefits of Advanced Practice Nursing for Its Expansion in the Spanish Context" International Journal of Environmental Research and Public Health 16, no. 5: 680. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050680