Resilience, Sense of Coherence, and Coping with Stress as Predictors of Psychological Well-Being in the Course of Schizophrenia. The Study Design

Abstract
:1. Introduction
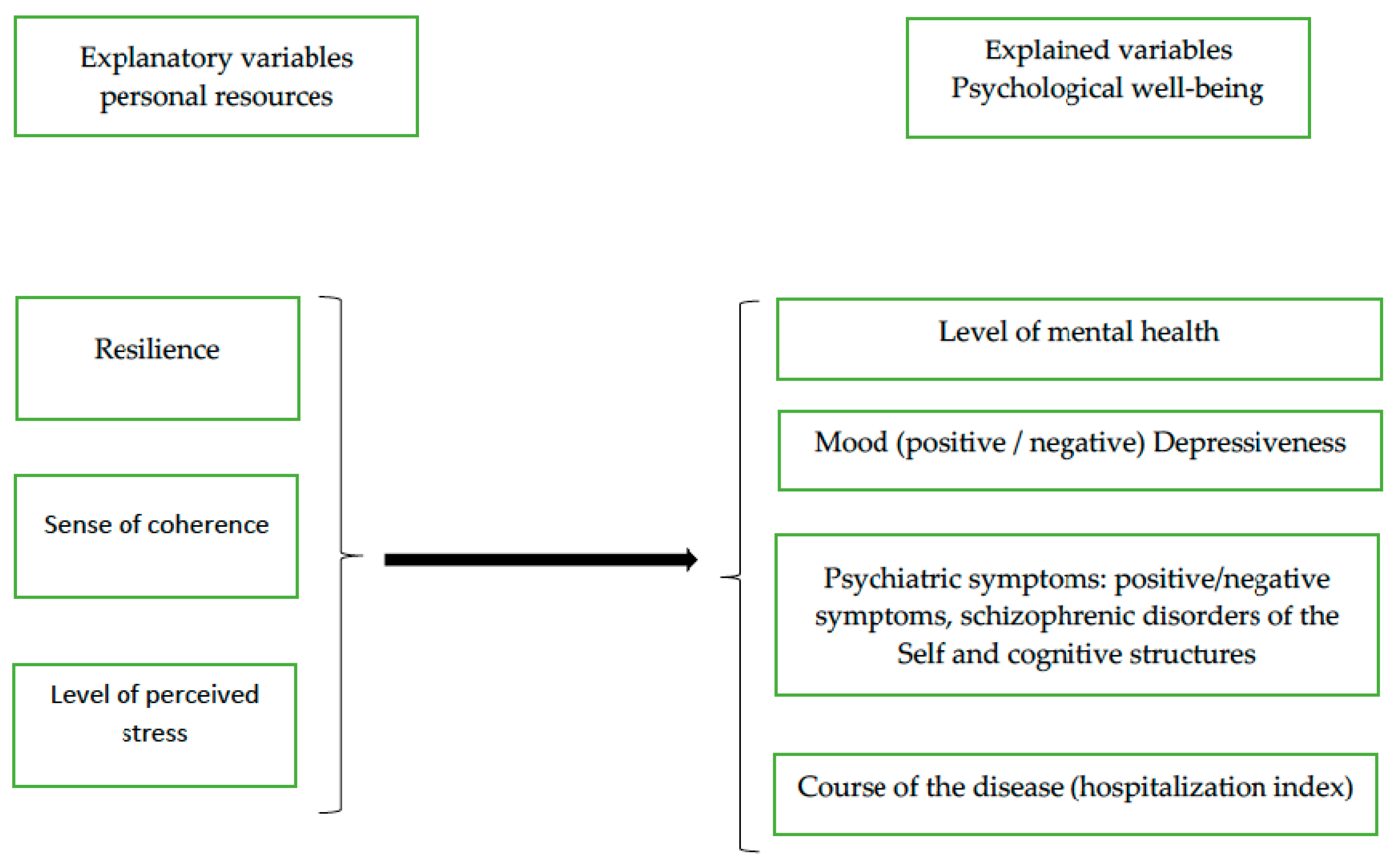
- Does resilience explain psychological well-being in patients with schizophrenia, and to what degree?
- Does sense of coherence explain psychological well-being in patients suffering from schizophrenia, and to what degree?
- Does the level of perceived stress (as a challenge versus threat) in subjects suffering from schizophrenia explain psychological well-being, and to what degree?
2. Materials and Methods
2.1. Procedure and Study Population
2.2. Methods
- The sense of coherence scale (SOC-29) by Antonovsky (2005) in its authorized Polish version by the IPN Clinical Psychology Unit, the Unit of Psychoprophylaxis of the UAM Institute of Psychology, and the Occupational Psychology Unit at the Institute of Occupational Medicine in Łódź [34]. The questionnaire comprises 29 items that take the form of questions measuring sense of coherence and its three components of comprehensibility, manageability, and meaningfulness against a 7-point scale. It is possible to obtain results between 29 and 203 points. A high SOC-29 result denotes a strong sense of coherence. The following results for each subscale can be treated as high: For comprehensibility—11 to 77, for manageability (MA)—10 to 70, and for meaningfulness (ME)—8 to 56 points. The Cronbach α is 0.88.
- The resilience scale for adults (RSA) by Friborg et al. (2003), which serves the purpose of assessing resilience [22]. It comprises 6 factors measuring the following aspects: (1) perception of self, α = 0.70, (2) perception of future, α = 0.66, (3) social competence, α = 0.76, (4) structured style, α = 0.69, (5) family cohesion, α = 0.78, and social resources, α = 0.69. The mentioned RSA scales allow to measure protective factors describing the psychological characteristics labeled as resilience. The authors of this work used the Polish adaptation of RSA prepared by Jelonkiewicz, Kühn-Dymecka, and Zwoliński [35]. The Polish RSA scale comprises 20 items that measure personal strength (self-perception and perception of one’s own future), structured style, social competence, and the general factor. Subjects rated resilience responding to the RSA items on 5-point frequency scales (from: “I know how to accomplish” to “I am not sure”). The reliability of the whole scale is Cronbach α = 0.77, while the reliabilities of each of the subscales are as follows: For personal strength, Cronbach α = 0.74; for self-perception, α = 0.64; for perception of own future, α = 0.69; for social competences, α = 0.77; for structured style, α = 0.49. The internal consistency of the Polish RSA adaptation is highly similar to the original version. The only doubtful issue is the structured style scale, which demonstrated a much lower reliability than the original version [35]. Due to the unsatisfactory psychometric properties, total scores in the structured style scale were not used in the analyses.
- The stress appraisal measure for adolescents by Rowley et al. [36] in its Polish adaptation for adolescents and adults by Kosińska-Dec and Zwoliński [35] was used to measure the level of perceived stress. The instrument comprises 14 items for measuring general cognitive appraisal of the stress experienced by an individual in terms of challenge and threat. The scale for stress appraisal in terms of Challenge comprises 7 items (4 original ones and 3 created by the authors of the adaptation), and the threat appraisal scale consists of 7 original items. The whole instrument has demonstrated good internal consistency for both scales (Cronbach α for the challenge scale = 0.85, while for the threat scale, α = 0.82).
- The positive and negative syndrome scale (PANSS) by Kay, Opler, and Fiszbein [37]. The PANSS scale consists of 30 items (number of obtainable points ranges between 30 and 210). The scale comprises 30 items divided into 3 parts: The first one (7 items) is designed to assess positive symptoms, the second one (7 items) negative symptoms, while the third one (16 items) the so-called general psychopathology. The instrument allows a clinical practitioner to assess positive, negative, and general symptoms as well as to calculate a total score. High scores indicate the level of psychopathological symptoms’ intensity. Total results that are lower than 60 points indicate progression in terms of symptoms, while results higher than 60 points indicate exacerbation of schizophrenic disorders. Each of the symptoms is assessed by the subjects against a 7-point scale. The instrument demonstrated good reliability (Cronbach α = 0.85).
- The mood scale by Wojciszke and Baryła [38], in a modified version by Jelonkiewicz, Kühn-Dymecka and Zwoliński [35]. The instrument consists of 20 items describing positive and negative mood. It measures positive and negative mood and the proportion of positive to negative mood. Subjects indicate the experienced feelings against 7-point frequency scales (from never to always). The scale has demonstrated good reliability, both for the positive mood scale (Cronbach α = 0.86) and negative mood scale (Cronbach α = 0.89).
- The general health questionnaire (GHQ-12) by Goldberg, in its Polish adaptation by Makowska and Merecz [39]. The general score allowed a description of the sense of mental health (psychological condition) in subjects. The scale comprises 12 items, including 6 ones concerning a description of one’s general psychological condition, while the remaining ones describe the level of positive health—i.e., level of concentration, feelings of happiness and playing a useful part, the ability to face problems, make decisions, and enjoy everyday activities. Subjects indicated the experienced changes against 4-point frequency scales (ranging from “not at all” to “much more than usual”). The Polish adaptation of GHQ demonstrated sufficient reliability (Cronbach α = 0.87) and validity confirmed through intergroup comparisons and factor analyses of versions of [36].
2.3. Research Model
2.4. Statistical analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
- Resilience (explaining significantly the level of schizophrenic symptomatology: Negative symptoms and cognitive disorders);
- sense of coherence, which significantly predicted mood (in the case of manageability) and psychiatric symptomatology (comprehensibility).
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Birchwood, M.; Jackson, C. Schizofrenia. Modele kliniczne i techniki terapeutyczne; Clinical models and therapeutic techniques; Gdańskie Wydawnictwo Psychologiczne: Gdańsk, Poland, 2006; pp. 105–126. [Google Scholar]
- Stamm, R.; Bühler, K.E. Concepts of vulnerability of psychiatric diseases. Fortschr. Neurol. Psychiatr. 2001, 69, 300–309. [Google Scholar] [CrossRef]
- Zubin, J.; Spring, B. Vulnerability: A new view of schizophrenia. J. Abnorm. Psychol. 1977, 86, 103–126. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Dawson, M.E. A heuristic vulnerability/stress model of schizophrenic episodes. Schizophr. Bull. 1984, 10, 300–312. [Google Scholar] [CrossRef]
- Harrow, M.; Grossman, L.; Jobe, T.H.; Herbener, E.S. Do patients with schizophrenia ever show periods of recovery? A 15-years multi-follow-up study. Schizophr. Bull. 2005, 31, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Torgalsbøen, A.K. Full recovery from schizophrenia: The prognostic role of premorbid adjustment, symptoms at first admission, precipitating events and gender. Psychiatry Res. 2001, 88, 143–152. [Google Scholar] [CrossRef]
- Torgalsbøen, A.K.; Rund, B.R. Lessons learned from three studies of recovery from schizophrenia. Int. Rev. Psychiatry 2002, 14, 312–317. [Google Scholar] [CrossRef]
- Antonovsky, A. Rozwikłanie tajemnicy zdrowia: Jak radzić sobie ze stresem i nie zachorować; Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Wydawnictwo Instytutu Psychiatrii I Neurologii: Warszawa, Poland, 2005. [Google Scholar]
- Cechnicki, A. Schizofrenia—proces wielowymiarowy. Krakowskie prospektywne badania przebiegu, prognozy I wyników leczenia schizofrenii; Schizophrenia—A multidimensional process. Krakow's prospective studies on the course, prognosis and results of treatment of schizophrenia; Instytut Psychiatrii i Neurologii: Warszawa, Poland, 2011. [Google Scholar]
- Nuechterlein, K.H.; Dawson, M.E.; Ventura, J.; Gitlin, M.; Subotnik, K.L.; Snyder, K.S.; Mintz, J.; Bartzokis, G. The vulnerability/stress model of schizophrenic relapse; a longitudinal study. Acta Psychiatr. Scand. Suppl. 1994, 382, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Deveson, A. Resilience; Penguin: Sydney, Australia, 2003. [Google Scholar]
- Rutter, M. Implications of Resilience Concepts for Scientific Understanding. Ann. N. Y. Acad. Sci. 2006, 1094, 1–12. [Google Scholar] [CrossRef]
- American Psychological Association. The Road to Resilience. Available online: https://www.apa.org/helpcenter/road-resilience (accessed on 27 February 2018).
- Luthar, S.S. Resilience in development. A synthesis of research across five decades. In Developmental Psychopathology: Risk, Disorder and Adaptation, 2nd ed.; Cicchetti, D., Cihen, D.J., Eds.; Wiley and Sons: New York, NY, USA, 2006; Volume 3, pp. 739–795. [Google Scholar]
- Gillespie, B.M.; Chaboyer, W.; Wallis, M. Development of a theoretically derived model of resilience through concept analysis. Contemp. Nurse 2007, 25, 124–135. [Google Scholar] [CrossRef]
- Holaday, M.; McPhearson, R.W. Resilience and severe burns. J. Couns. Dev. 1997, 75, 346–357. [Google Scholar] [CrossRef]
- Richardson, G.E. Metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience in developing systems: Progress and promise as the fourth wave rises. Dev. Psychopathol. 2007, 19, 921–930. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the resilience scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Torgalsbøen, A.K.; Rund, B.R. Maintenance of Recovery from Schizophrenia at 20-Years Follow-up: What Happened? Psychiatry 2010, 73, 70–83. [Google Scholar] [CrossRef]
- Deegan, P.E. The importance of personal medicine: Aqualitative study of resilience in people with psychiatric distabilities. Scand. J. Public Health 2005, 33 (Suppl. 66), 29–35. [Google Scholar] [CrossRef]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int. J. Methods Psychiatr. Res. 2003, 12, 65–76. [Google Scholar] [CrossRef]
- Rossi, A.; Galderisi, S.; Rocca, P.; Bertolino, A.; Rucci, P.; Gilbertoni, D.; Stratta, P.; Bucci, P.; Mucci, A.; Aguglia, E.; et al. Personal resources and depression in schizophrenia: The role of self-esteem, resilience and internalized stigma. Psychiatry Res. 2017, 256, 359–364. [Google Scholar] [CrossRef]
- Palmer, B.W.; Martin, A.S.; Depp, C.A.; Glorioso, D.K.; Jeste, D.V. Welness within illness: Happiness in schizophrenia. Schizophr. Res. 2014, 159, 151–156. [Google Scholar] [CrossRef]
- Mizuno, Y.; Warteisteiner, F.; Frajo-Apor, B. Resilience research in schizophrenia: A review of recent developments. Curr. Opin. Psychiatry 2016, 29, 218–223. [Google Scholar] [CrossRef]
- Heszen, I.; Sęk, H. Psychologia zdrowia. [Health Psychology]; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2018; pp. 75–89. [Google Scholar]
- Świtaj, P.; Grygiel, P.; Chrostek, A.; Nowak, I.; Wciórka, J.; Anczewska, M. The relationship between internalized stigma and quality of life among people with mental illness: Are self-esteem and sense of coherence sequential mediators? Qual. Life Res. 2017, 26, 2471–2478. [Google Scholar] [CrossRef]
- Witkowska-Łuć, B. Schizophrenia and sense of coherence. Psychiatr. Pol. 2018, 52, 217–226. [Google Scholar] [CrossRef]
- Werner, E.E.; Smith, R.S. Journeys from Childhood to Midlife: Risk, Resilience, and Recovery; Cornell University Press: New York, NY, USA, 2001. [Google Scholar]
- Hjemdal, O.; Friborg, O.; Stiles, T.C.; Rosenvinge, J.H.; Martinussen, M. Resilience predicting psychiatric symptoms: A prospective study of protective factors and their role in adjustment to stressful life events. Clin. Psychol. Psychother. 2006, 13, 194–201. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Kang, M.; Bang, M.; Young Lee, S.; Lee, E.; Yoo, S.W.; An, S.K. Coping styles in individuals at ultra-high risk for psychosis: Associations with cognitive appraisals. Psychiatry Res. 2018, 264, 162–168. [Google Scholar] [CrossRef]
- Rüsch, N.; Heekeren, K.; Theodoridou, A.; Müller, M.; Corrigan, P.W.; Mayer, B.; Metzler, S.; Dvorsky, D.; Walitza, S.; Röslerr, W. Stigma as a stressor and transition to schizophrenia after one year among young people at risk of psychosis. Schizophr. Res. 2015, 166, 43–48. [Google Scholar] [CrossRef]
- Mroziak, B.A. Antonovsky'ego koncepcja salutogenezy i poczucia koherencji (SOC). Nowiny Psychologiczne 1994, 1, 6–16. [Google Scholar]
- Zwoliński, M. Załącznik nr 17 do raportu z tematu IPiN, nr 26/2008. Annex 17 to the report on the subject of IPiN, No. 26/20; Institute of Psychiatry and Neurology: Warsaw, Poland, 2008. [Google Scholar]
- Rowley, A.A.; Roesch, S.C.; Jurica, B.J.; Vaughn, A.A. Developing and validating a stress appraisal measure for minority adolescents. J. Adolesc. 2005, 28, 547–557. [Google Scholar] [CrossRef]
- Rzewuska, M. Validity and reliability of the Polish version of the Positive and Negative Syndrome Scale (PANSS). Int. J. Meth. Psych. Res. 2002, 11, 27–32. [Google Scholar] [CrossRef]
- Wojciszke, B.; Baryła, W. Skale do pomiaru nastroju i sześciu emocji. Scales for measuring mood and six emotions. Czasopismo Psyhcologiczne 2005, 11, 31–47. [Google Scholar]
- Makowska, Z.; Merecz, D. Ocena Zdrowia Psychicznego na podstawie badań kwestionariuszami Davida Goldberga. The General Health Questionnaire; Pracownia Testów Psychologicznych PTP: Warszawa, Poland, 2001. [Google Scholar]
- Lysaker, P.H.; Buck, K.D. Is recovery from schizophrenia possible? An overview of concepts evidence and clinical implications. Prim. Psychiatry 2008, 15, 50. [Google Scholar]
- Skrzypnica, D.; Słodka, M. Kto może zachorować na schizofrenię? Czyli o modelach podatność-stres. Who can get schizophrenia? So the vulnerability and stress models. In Młoda Psychologia New Psychology; Drop, E., Maćkiewicz, M., Eds.; Liberi Libri: Warszawa, Poland, 2012; Volume 1, pp. 369–385. [Google Scholar]
- Vauth, R.; Stieglitz, R.D. Trening inteligencji emocjonalnej w schizofrenii. Poradnik terapeuty. Das Training Emotionaler Intelligenz bei schizophrenen Störungen; Wydawnictwo DK Media: Warszawa, Poland, 2014. [Google Scholar]
- Clamor, A.; Warmuth, M.; Lincoln, T.M. Arousal Predisposition as a Vulnerability Indicator for Psychosis: A General Population Online Stress Induction Study. Schizophr. Res. Treatment 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kosmidis, M.H.; Bozikas, V.P.; Giannakou, M.; Anezoulaki, D.; Fantie, B.D.; Karavatos, A. Impaired emotion perception in schizophrenia: A differential deficit. Psychiatry Res. 2007, 149, 279–284. [Google Scholar] [CrossRef]
- Cooper, C.; Flint-Taylor, J.; Pearn, M. Building Resilience for Success: A Resource for Managers and Organizations; Palgrave Macmillan: London, UK, 2013. [Google Scholar]
- Bengtsson-Tops, A.; Brunt, D.; Rask, M. The structure of Antonovsky’s sense of coherence in patients with schizophrenia and its relationship to psychopathology. Scand. J. Caring Sci. 2005, 19, 280–287. [Google Scholar] [CrossRef]
- Gassmann, W.; Christ, O.; Lampert, J.; Berger, H. The influence of Antonovsky’s sense of coherence (SOC) and psychoeducational family intervention (PEFI) on schizophrenic outpatients’ perceived quality of life: A longitudinal field study. BMC Psychiatry 2013, 13, 10. [Google Scholar] [CrossRef]
- Chiu-Yueh, H.; Yun-Fang, T. Factors of caregiver burden and family functioning among Taiwanese family caregivers living with schizophrenia. J. Clin. Nurs. 2014, 24, 1546–1556. [Google Scholar]
- Choo, C.C.; Chew, P.K.H.; Ho, C.S.; Ho, R.C. Prediction of Quality of Life in Asian Patients with Schizophrenia: A Cross-sectional Pilot Study. Front. Psychiatry 2017, 8, 198. [Google Scholar] [CrossRef]


{kind=link}
| Psychological Well-being | M | SD |
|---|---|---|
| Psychiatric symptomatology | 3.52 | 1.33 |
| Level of mental health | 2.32 | 0.68 |
| Mood level | ||
| Positive mood | 3.95 | 1.07 |
| Negative mood | 3.91 | 1.18 |
| Sociodemographic Variables | % of Subjects with Schizophrenia | |
| Sex (%) | Female | 47.3 |
| Male | 52.7 | |
| Age | Mean | 28.97 |
| Range | 18–62 | |
| Education completed (%) | Elementary school | 8.5 |
| Vocational school | 2.5 | |
| High school | 53.7 | |
| University | 35.3 | |
| Source of income (%) | Permanent job | 10.4 |
| Permanent/temping job/parents/annuities | 16.0 | |
| Temping job | 3.5 | |
| Temping job/parents/scholarship | - | |
| Parents/other people | 27.9 | |
| Parents/annuities/social aids | 14.5 | |
| Scholarship | 1.0 | |
| Annuities | 20.9 | |
| Allowance/social aids/annuities | 5.0 | |
| Living conditions (%) | With both parents/ | 50.7 |
| One parent | 22.9 | |
| With someone else | 13.4 | |
| Alone | 10.9 | |
| Siblings | Only child | 14.9 |
| One sibling | 50.2 | |
| Two siblings | 19.4 | |
| Three or more siblings | 15.4 | |
| Parents’ education | Father | |
| -elementary school | 6.5 | |
| -incomplete high school | 14.4 | |
| -high school | 35.8 | |
| -university | 39.3 | |
| -higher than university | 2.5 | |
| Mother | ||
| -elementary school | 9.0 | |
| -incomplete high school | 8.5 | |
| -high school | 38.3 | |
| -university | 43.3 | |
| -higher than university | 0.5 | |
| Family economic situation | Very bad/bad | 3.5 |
| Rather bad | 9.0 | |
| Tolerable | 33.8 | |
| Rather good | 28.9 | |
| Good/very good | 24.9 | |
| Personal Resources | M | SD |
|---|---|---|
| Resilience | 63.01 | |
| Perception of self | 17.72 | 5.25 |
| Perception of future | 12.72 | 4.37 |
| Personal strength | 30.38 | 8.76 |
| Resilience (general score) | 63.01 | 14.43 |
| Sense of coherence Sense of coherence (general score) | 122.41 | 26.27 |
| Comprehensibility | 42.00 | 10.22 |
| Manageability | 42.83 | 10.35 |
| Meaningfulness | 37.66 | 9.72 |
| Perceived stress | ||
| Perceived efficiency of coping with stress (general score) | 8.94 | 3.89 |
| Stress appraised as challenge | 5.74 | 2.85 |
| Stress appraised as threat | 18.42 | 5.47 |
| Explained Variable | Significant Predictors | Model Summary | |
|---|---|---|---|
| Course of the disease | Number of hospitalizations/years of disease | n.s. | n.s. |
| Number of hospitalizations | SOC Manageability Beta = −0.212 | F(3144) = 2.53 R2 corrected = 0.050 p < 0.05 | |
| Psychological well-being | Mental health | SOC comprehensibility Beta = 0.468 | F(3144) = 30.83 R2 corrected = 0.37 p < 0.001 |
| Positive mood | SOC manageability Beta = 0.580 SOS stress appraised as challenge Beta = 0.164 | F(3144) = 49.23 R2 corrected = 0.496 p < 0.001 | |
| Negative mood, depressiveness | SOC manageability—Beta = −0.534 SOS stress appraised as threat Beta = 0.190 | F(2145) = 49.60 R2 corrected = 0.398 p < 0.001 | |
| Psychological well-being (Psychiatric symptoms) | General index | RSA Resilience Beta = −0.302 | F(3144) = 3.08 R2 corrected = 0.041 p < 0.05 |
| Positive symptoms | n.s. | n.s. | |
| Negative symptoms | RSA Resilience Beta = −0.385 SOC Comprehensibility Beta = 0.311 | F(4143) = 2.94 R2 corrected =0.050 p < 0.05 | |
| Excessive arousal | SOC Comprehensibility Beta = 0.173 | F(2145) = 3.97 R2 corrected = 0.039 p < 0.05 | |
| Cognitive disorganization | SOC Comprehensibility Beta = 0.330 RSA Resilience Beta = −0.303 | F(3144) = 4.16 R2 corrected = 0.060 p < 0.01 | |
| Depression | n.s. | n.s. | |
| Anxiety | n.s. | n.s. | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izydorczyk, B.; Sitnik-Warchulska, K.; Kühn-Dymecka, A.; Lizińczyk, S. Resilience, Sense of Coherence, and Coping with Stress as Predictors of Psychological Well-Being in the Course of Schizophrenia. The Study Design. Int. J. Environ. Res. Public Health 2019, 16, 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071266
Izydorczyk B, Sitnik-Warchulska K, Kühn-Dymecka A, Lizińczyk S. Resilience, Sense of Coherence, and Coping with Stress as Predictors of Psychological Well-Being in the Course of Schizophrenia. The Study Design. International Journal of Environmental Research and Public Health. 2019; 16(7):1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071266
Chicago/Turabian StyleIzydorczyk, Bernadetta, Katarzyna Sitnik-Warchulska, Aleksandra Kühn-Dymecka, and Sebastian Lizińczyk. 2019. "Resilience, Sense of Coherence, and Coping with Stress as Predictors of Psychological Well-Being in the Course of Schizophrenia. The Study Design" International Journal of Environmental Research and Public Health 16, no. 7: 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071266