What Works? Prevention and Control of Sexually Transmitted Infections and Blood-Borne Viruses in Migrants from Sub-Saharan Africa, Northeast Asia and Southeast Asia Living in High-Income Countries: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Information Sources
2.2. Data Extraction
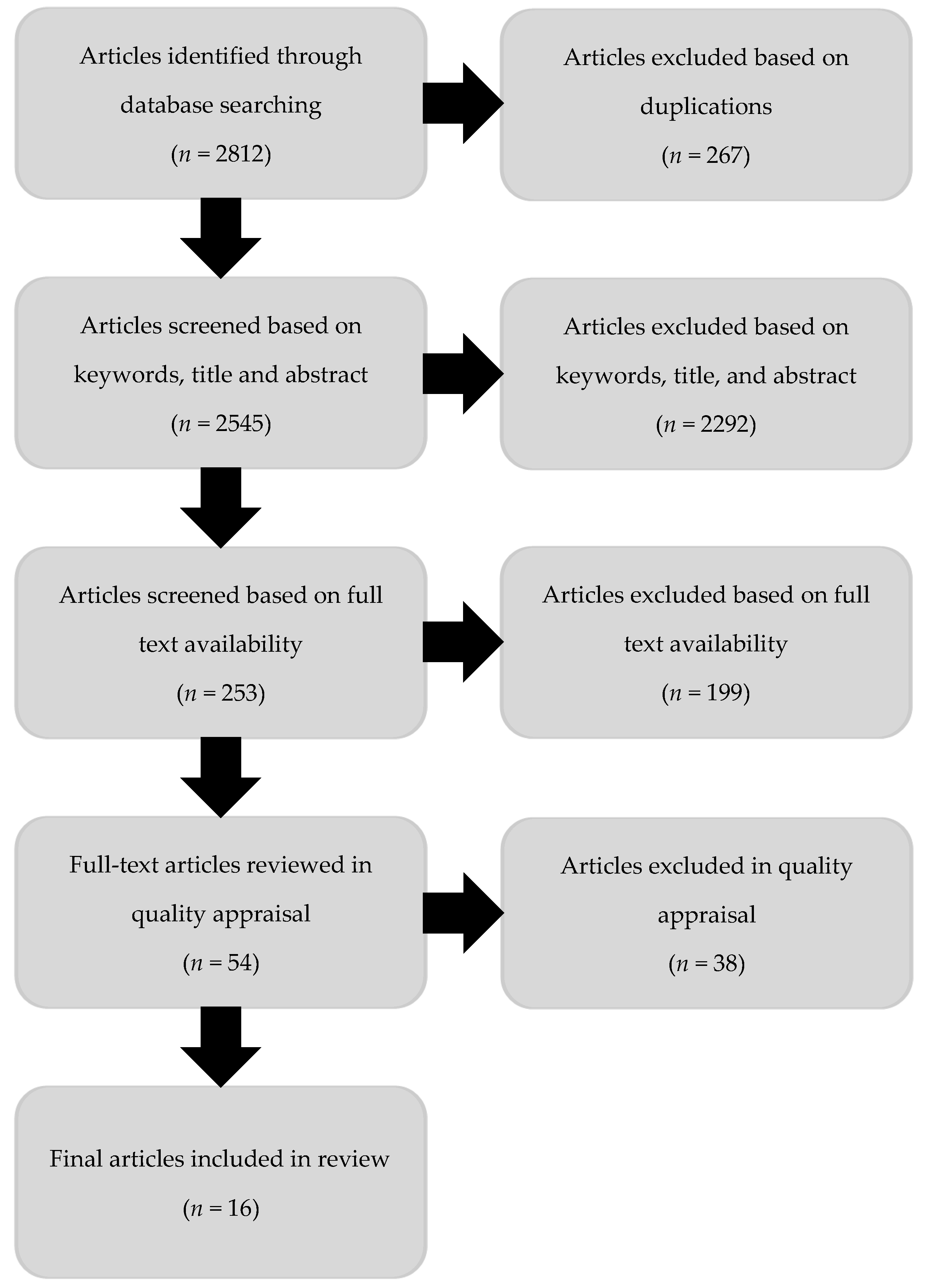
3. Results
- Overview of studies: location, design, methods of data collection and sample size.
- Participant characteristics: age, gender, migrants’ country of origin.
- Individual interventions: recruitment into general practice and home-based testing, provider-initiated testing and outreach testing.
- Community interventions: sexual health education and stigma reduction.
- Structural interventions: mandatory screening and changes in laws impacting on sex work.
- Study recommendations: policy, practice (clinical and health promotion) and research.
3.1. Overview of the Studies
3.2. Participant Characteristics
3.3. Individual Interventions
3.3.1. Recruitment into General Practice and Home-Based Testing
3.3.2. Provider Initiated Testing
3.3.3. Outreach Testing
3.4. Community Interventions
3.4.1. Sexual Health Education
3.4.2. Mass Media Campaigns
3.4.3. Supporting People Living with HIV
3.5. Structural Interventions
3.5.1. Criminalization of Sex Work
3.5.2. Mandatory Screening Programs
3.6. Study Recommendations
4. Discussion
4.1. Overview of Findings
4.2. Study Design and Reporting Limitations
4.3. Strengths and Limitations of the Review
4.4. Implications for Research, Policy, and Practice
4.4.1. Research Opportunities
4.4.2. Clinical Practice Opportunities
4.4.3. Health Promotion Opportunities
4.4.4. Policy and Advocacy Opportunities
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nygren-Krug, H. International Migration, Health and Human Rights; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Platt, L.; Grenfell, P.; Fletcher, A.; Sorhaindo, A.; Jolley, E.; Rhodes, T.; Bonell, C. Systematic review examining differences in HIV, sexually transmitted infections and health-related harms between migrant and non-migrant female sex workers. Sex. Transm. Infect. 2013, 89, 311–319. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Population Mobility and AIDS. Unaids Technical Update; UNAIDS: Geneva, Switzerland, 2001. [Google Scholar]
- El-Bassel, N.; Gilbert, L.; Shaw, S.A.; Mergenova, G.; Terlikbayeva, A.; Primbetova, S.; Ma, X.; Chang, M.; Ismayilova, L.; Hunt, T.; et al. The silk road health project: How mobility and migration status influence HIV risks among male migrant workers in central asia. PLoS ONE 2016, 11, e0151278. [Google Scholar] [CrossRef] [PubMed]
- Haour-Knipe, M.; Zalduondo, B.; Samuels, F.; Molesworth, K.; Sehgal, S. HIV and “people on the move”: Six strategies to reduce risk and vulnerability during the migration process. Int. Migr. 2014, 52, 9–25. [Google Scholar] [CrossRef]
- Crawford, G.; Lobo, R.; Brown, G.; Macri, C.; Smith, H.; Maycock, B. HIV, other blood-borne viruses and sexually transmitted infections amongst expatriates and travellers to low-and middle-income countries: A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 1249. [Google Scholar] [CrossRef] [PubMed]
- De Cock, K.M.; Jaffe, H.W.; Curran, J.W. The evolving epidemiology of HIV/AIDS. AIDS 2012, 26, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Kirby Institute. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2018; Kirby Institute, UNSW Sydney: Sydney, Australia, 2018. [Google Scholar]
- Alvarez-del Arco, D.; Fakoya, I.; Thomadakis, C.; Pantazis, N.; Touloumi, G.; Gennotte, A.F.; Boesecke, C. High levels of postmigration HIV acquisition within nine european countries. AIDS 2017, 31, 1979–1988. [Google Scholar] [PubMed]
- Crawford, G.; Lobo, R.; Brown, G.; Maycock, B. The influence of population mobility on changing patterns of HIV acquisition: Lessons for and from australia. Health Promot. J. Aust. 2016, 27, 153–154. [Google Scholar] [CrossRef]
- Gray, C.; Crawford, G.; Reid, A.; Lobo, R. HIV knowledge and use of health services among people from south east asia and sub-saharan africa living in western australia. Health Promot. J. Aust. 2018. [Google Scholar] [CrossRef]
- Goldenberg, S.M.; Strathdee, S.A.; Perez-Rosales, M.D.; Sued, O. Mobility and HIV in central america and mexico: A critical review. J. Immigr. Minor. Health 2012, 14, 48–64. [Google Scholar] [CrossRef]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. “In my culture, we don’t know anything about that”: Sexual and reproductive health of migrant and refugee women. Int. J. Behav. Med. 2017, 24, 836–845. [Google Scholar] [CrossRef]
- Tompkins, M.; Smith, L.; Jones, K.; Swindells, S. HIV education needs among sudanese immigrants and refugees in the midwestern united states. AIDS Behav. 2006, 10, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Department of Health Australian Government. Eighth National HIV Strategy 2018–2022; Commonwealth of Australia: Canberra, ACT, Australia, 2018.
- Department of Health Australian Government. Third National Hepatitis b Strategy 2018–2022; Commonwealth of Australia: Canberra, ACT, Australia, 2018.
- Herbst, J.H.; Kay, L.S.; Passin, W.F.; Lyles, C.M.; Crepaz, N.; Marin, B.V.; Team, H.A.P.R.S. A systematic review and meta-analysis of behavioral interventions to reduce HIV risk behaviors of hispanics in the united states and puerto rico. AIDS Behav. 2007, 11, 25–47. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C. A Systematic Evaluation of Culturally Sensitive HIV/AIDS Prevention Interventions in the US, 1996-2007; Department of Sociology, Michigan State University: East Lansing, MI, USA, 2008. [Google Scholar]
- Charania, M.R.; Crepaz, N.; Guenther-Gray, C.; Henny, K.; Liau, A.; Willis, L.A.; Lyles, C.M. Efficacy of structural-level condom distribution interventions: A meta-analysis of u.S. And international studies, 1998-2007. AIDS Behav. 2011, 15, 1283–1297. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016-2021: Toward Ending STIs; World Health Organization Geneva: Geneva, Switzerland, 2016. [Google Scholar]
- Manhart, L.E.; Holmes, K.K. Randomized controlled trials of individual-level, population-level, and multilevel interventions for preventing sexually transmitted infections: What has worked? J. Infect. Dis. 2005, 191, S7–S24. [Google Scholar] [CrossRef] [PubMed]
- McMahon, T.; Ward, P.R. HIV among immigrants living in high-income countries: A realist review of evidence to guide targeted approaches to behavioural HIV prevention. Syst. Rev. 2012, 1, 56. [Google Scholar] [CrossRef] [PubMed]
- Coates, T.J.; Richter, L.; Caceres, C. Behavioural strategies to reduce HIV transmission: How to make them work better. Lancet 2008, 372, 669–684. [Google Scholar] [CrossRef]
- Ferguson, A.; Shannon, K.; Butler, J.; Goldenberg, S.M. A comprehensive review of HIV/STI prevention and sexual and reproductive health services among sex workers in conflict-affected settings: Call for an evidence- and rights-based approach in the humanitarian response. Confl. Health 2017, 11, 25. [Google Scholar] [CrossRef]
- Hankins, C.A.; de Zalduondo, B.O. Combination prevention: A deeper understanding of effective HIV prevention. AIDS 2010, 24 (Suppl. 4), S70–S80. [Google Scholar] [CrossRef]
- Kerrigan, D.; Kennedy, C.E.; Morgan-Thomas, R.; Reza-Paul, S.; Mwangi, P.; Win, K.T.; McFall, A.; Fonner, V.A.; Butler, J. A community empowerment approach to the HIV response among sex workers: Effectiveness, challenges, and considerations for implementation and scale-up. Lancet (Lond. Engl.) 2015, 385, 172–185. [Google Scholar] [CrossRef]
- International HIV/AIDS Alliance and the Global Network of People Living with HIV. Greater Involvement of People Living with HIV; International HIV/AIDS Alliance: England, UK, 2010. [Google Scholar]
- Crawford, G.; Lobo, R.; Brown, G.; Langdon, P. HIV and mobility in australia: Road map for action; Western Australian Centre for Health Promotion Research and Australian Research Centre in Sex, Health and Society: Perth, WA, Australia, 2014. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Burford, B.J.; Welch, V.; Waters, E.; Tugwell, P.; Moher, D.; O’Neill, J.; Koehlmoos, T.; Petticrew, M. Testing the prisma-equity 2012 reporting guideline: The perspectives of systematic review authors. PLoS ONE 2013, 8, e75122. [Google Scholar] [CrossRef]
- Leavy, J.E.; Crawford, G.; Portsmouth, L.; Jancey, J.; Leaversuch, F.; Nimmo, L.; Hunt, K. Recreational drowning prevention interventions for adults, 1990–2012: A review. J. Commun. Health 2015, 40, 725–735. [Google Scholar] [CrossRef]
- Leavy, J.E.; Crawford, G.; Leaversuch, F.; Nimmo, L.; McCausland, K.; Jancey, J. A review of drowning prevention interventions for children and young people in high, low and middle income countries. J. Commun. Health 2016, 41, 424–441. [Google Scholar] [CrossRef]
- Rade, D.; Crawford, G.; Lobo, R.; Gray, C.; Brown, G. Sexual health help-seeking behavior among migrants from sub-saharan africa and south east asia living in high income countries: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 1311. [Google Scholar] [CrossRef]
- Crawford, G.; Leavy, J.; Portsmouth, L.; Jancey, J.; Leaversuch, F.; Nimmo, L.; Reid-Dornbusch, L.; Hills, E. Development of a systematic review of public health interventions to prevent children drowning. Open J. Prev. Med. 2014, 4, 100–106. [Google Scholar] [CrossRef]
- World Health Organization. Universal Health Coverage. Available online: https://afro.who.int/media-centre/events/world-health-day-2018-universal-health-coverage (accessed on 13 December 2018).
- Global Residence Index. The 2018 STC Health Index. Available online: http://globalresidenceindex.com/hnwi-index/health-index/ (accessed on 11 June 2018).
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519#East_Asia_and_Pacific (accessed on 21 June 2018).
- International Organization for Migration: Country Office for Belgium and Luxembourg. Key migration terms. Available online: http://belgium.iom.int/key-migration-terms%E2%80%8B (accessed on 15 June 2018).
- Higgins, J.; Green, S. Handbook for Systematic Reviews of Interventions Version 5.1. 0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- National Institute for Clinical Excellence. Methods for the Development of NICE Public Health Guidance; NICE: London, UK, 2006. [Google Scholar]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual; The Joanna Briggs Institute: Adelaide, Australia, 2014. [Google Scholar]
- Esteban-Vasallo, M.D.; Morán-Arribas, M.; García-Riolobos, C.; Domínguez-Berjón, M.F.; Rico-Bermejo, J.; Collado-González, S.; Jiménez-García, R.; Guionnet, A.; de la Fuente, B.P.; El Kertat, R.; et al. Targeted rapid HIV testing in public primary care services in madrid. Are we reaching the vulnerable populations? Int. J. Infect. Dis. 2014, 19, 39–45. [Google Scholar] [CrossRef]
- Bartelsman, M.; Joore, I.K.; van Bergen, J.E.; Hogewoning, A.A.; Zuure, F.R.; van Veen, M.G. HIV testing week 2015: Lowering barriers for HIV testing among high-risk groups in amsterdam. BMC Infect. Dis. 2017, 17. [Google Scholar] [CrossRef]
- Stornaiuolo, G.; Cuniato, V.; Cuomo, G.; Nocera, E.; Brancaccio, G.; De Rosa, M.; Pontarelli, A.; Grasso, G.; Danzi, G.; Grossi, A.; et al. Active recruitment strategy in disadvantaged immigrant populations improves the identification of human immunodeficiency but not of hepatitis b or c virus infections. Dig. Liver Dis. 2014, 46, 62–66. [Google Scholar] [CrossRef]
- van Gemert, C.; Wang, J.; Simmons, J.; Cowie, B.; Boyle, D.; Stoove, M.; Enright, C.; Hellard, M. Improving the identification of priority populations to increase hepatitis b testing rates, 2012. BMC Public Health 2016, 16, 95. [Google Scholar] [CrossRef]
- Dokkum, N.F.B.; Koekenbier, R.H.; van den Broek, I.V.F.; van Bergen, J.E.A.M.; Brouwers, E.E.H.G.; Fennema, J.S.A.; Götz, H.M.; Hoebe, C.J.P.A.; Pars, L.L.; van Ravesteijn, S.M.; et al. Keeping participants on board: Increasing uptake by automated respondent reminders in an internet-based chlamydia screening in the netherlands. BMC Public Health 2012, 12, 176. [Google Scholar] [CrossRef]
- Frati, E.R.; Fasoli, E.; Martinelli, M.; Colzani, D.; Bianchi, S.; Carnelli, L.; Amendola, A.; Olivani, P.; Tanzi, E. Sexually transmitted infections: A novel screening strategy for improving women’s health in vulnerable populations. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef]
- Uccella, I.; Petrelli, A.; Vescio, M.F.; De Carolis, S.; Fazioli, C.; Pezzotti, P.; Rezza, G. HIV rapid testing in the framework of an sti prevention project on a cohort of vulnerable italians and immigrants. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2017, 29, 996–1002. [Google Scholar] [CrossRef]
- Veldhuijzen, I.K.; Wolter, R.; Rijckborst, V.; Mostert, M.; Voeten, H.A.; Cheung, Y.; Boucher, C.A.; Reijnders, J.G.; de Zwart, O.; Janssen, H.L. Identification and treatment of chronic hepatitis b in chinese migrants: Results of a project offering on-site testing in rotterdam, the netherlands. J. Hepatol. 2012, 57, 1171–1176. [Google Scholar] [CrossRef]
- Worth, H.; Denholm, N.; Bannister, J. HIV/AIDS and the african refugee education program in new zealand. AIDS Educ. Prev. 2003, 15, 346–356. [Google Scholar] [CrossRef]
- Drummond, P.D.; Mizan, A.; Brocx, K.; Wright, B. Using peer education to increase sexual health knowledge among west african refugees in western australia. Health Care Women Int. 2011, 32, 190–205. [Google Scholar] [CrossRef]
- Roberts, M.; Lobo, R.; Sorenson, A. Evaluating the sharing stories youth theatre program: An interactive theatre and drama-based strategy for sexual health promotion among multicultural youth. Health Promot. J. Aust. 2017, 28, 30–36. [Google Scholar] [CrossRef]
- McMahon, T.; Fairley, C.K.; Donovan, B.; Wan, L.; Quin, J. Evaluation of an ethnic media campaign on patterns of HIV testing among people from culturally and linguistically diverse backgrounds in australia. Sex. Health 2004, 1, 91–94. [Google Scholar] [CrossRef]
- Li, A.T.W.; Fung, K.P.L.; Maticka-Tyndale, E.; Wong, J.P.H. Effects of HIV stigma reduction interventions in diasporic communities: Insights from the champ study. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2018, 30, 739–745. [Google Scholar] [CrossRef]
- Ackermann, N.; Marosevic, D.; Hormansdorfer, S.; Eberle, U.; Rieder, G.; Treis, B.; Berger, A.; Bischoff, H.; Bengs, K.; Konrad, R.; et al. Screening for infectious diseases among newly arrived asylum seekers, bavaria, germany, 2015. Eurosurveillance 2018, 23, 2–12. [Google Scholar] [CrossRef]
- Zencovich, M.; Kennedy, K.; MacPherson, D.W.; D Gushulak, B. Immigration medical screening and HIV infection in canada. Int. J. STD AIDS 2006, 17, 813–816. [Google Scholar] [CrossRef]
- Anderson, S.; Shannon, K.; Li, J.; Lee, Y.; Chettiar, J.; Goldenberg, S.; Krusi, A. Condoms and sexual health education as evidence: Impact of criminalization of in-call venues and managers on migrant sex workers access to HIV/STI prevention in a canadian setting. BMC Int. Health Hum. Rights 2016, 16, 30. [Google Scholar] [CrossRef]
- Manirankunda, L.; Loos, J.; Debackaere, P.; Nostlinger, C. “It is not easy”: Challenges for provider-initiated HIV testing and counseling in flanders, belgium. AIDS Educ. Prev. 2012, 24, 456–468. [Google Scholar] [CrossRef]
- Blondell, S.J.; Kitter, B.; Griffin, M.P.; Durham, J. Barriers and facilitators to HIV testing in migrants in high-income countries: A systematic review. AIDS Behav. 2015, 19, 2012–2024. [Google Scholar] [CrossRef]
- Collaboration for Evidence Research and Impact in Public Health. “I Want to Test But I’m Afraid”: Barriers to HIV Testing among People Born in South East Asia and Sub-Saharan Africa: Final Report; Curtin University: Perth, WA, Australia, 2018. [Google Scholar]
- Aung, E.; Blondell, S.J.; Durham, J. Interventions for increasing HIV testing uptake in migrants: A systematic review of evidence. AIDS Behav. 2017. [Google Scholar] [CrossRef]
- Asante, A.D.; Körner, H. Knowledge and access are not enough: HIV risk and prevention among people from culturally and linguistically diverse backgrounds in sydney. Med. J. Aust. 2012, 196, 502. [Google Scholar] [CrossRef]
- Smith, J.L.; Fenwick, J.; Skinner, R.; Hallet, J.; Merriman, G.; Marshall, L. Sex, condoms and sexually transmissible infections: A qualitative study of sexual health in young australian men. Arch. Sex. Behav. 2012, 41, 487–495. [Google Scholar] [CrossRef]
- Bova, C.; Nnaji, C.; Woyah, A.; Duah, A. HIV stigma, testing attitudes and health care access among african-born men living in the united states. J. Immigr. Minority Health 2016, 18, 187–193. [Google Scholar] [CrossRef]
- Hosseinzadeh, H.; Hossain, S.Z.; Bazargan-Hejazi, S. Perceived stigma and social risk of HIV testing and disclosure among iranian-australians living in the sydney metropolitan area. Sex Health 2012, 9, 171–177. [Google Scholar] [CrossRef]
- Stangl, A.L.; Lloyd, J.K.; Brady, L.M.; Holland, C.E.; Baral, S. A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: How far have we come? J. Int. AIDS Soc. 2013, 16, 18734. [Google Scholar] [CrossRef]
- Kärki, T.; Napoli, C.; Riccardo, F.; Fabiani, M.; Dente, M.G.; Carballo, M.; Noori, T.; Declich, S. Screening for infectious diseases among newly arrived migrants in eu/eea countries—varying practices but consensus on the utility of screening. Int. J. Environ. Res. Public Health 2014, 11, 11004–11014. [Google Scholar] [CrossRef]
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; MacDonald, N.E. Evidence-based clinical guidelines for immigrants and refugees. Can. Med. Assoc. J. 2011, 183, E824–E925. [Google Scholar]
- Thomas, F.; Aggleton, P.; Anderson, J. “If i cannot access services, then there is no reason for me to test”: The impacts of health service charges on HIV testing and treatment amongst migrants in england. AIDS Care 2010, 22, 526–531. [Google Scholar] [CrossRef]
- Adedimeji, A.A.; Asibon, A.; O’Connor, G.; Carson, R.; Cowan, E.; McKinley, P.; Leider, J.; Mallon, P.; Calderon, Y. Increasing HIV testing among african immigrants in ireland: Challenges and opportunities. J. Immigr. Minor. Health 2015, 17, 89–95. [Google Scholar] [CrossRef]
- Agu, J.; Lobo, R.; Crawford, G.; Chigwada, B. Migrant sexual health help-seeking and experiences of stigmatization and discrimination in perth, western australia: Exploring barriers and enablers. Int. J. Environ. Res. Public Health 2016, 13, 485. [Google Scholar] [CrossRef]
- Korner, H. ‘If i had my residency i wouldn’t worry’: Negotiating migration and HIV in sydney, australia. Ethn Health 2007, 12, 205–225. [Google Scholar] [CrossRef]
- UNAIDS. On the Fast-Track to End AIDS. Unaids 2016–2021 Strategy; UNAIDS: Geneva, Switzerland, 2015. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (coreq): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Community of Practice for Action on HIV and Mobility. HIV and Mobility in Australia: Priority Actions; Collaboration for Evidence, Research and Impact in Health Promotion: Perth, WA, Australia, 2018. [Google Scholar]
- Caffrey, L.; Munro, E. A systems approach to policy evaluation. Evaluation 2017, 23, 463–478. [Google Scholar] [CrossRef]
- Drummond, P.D.; Mizan, A.; Wright, B. HIV/AIDS knowledge and attitudes among west african immigrant women in western australia. Sex. Health 2008, 5, 251–259. [Google Scholar] [CrossRef]
- Deane, K.D.; Parkhurst, J.O.; Johnston, D. Linking migration, mobility and HIV. Trop. Med. Int. Health 2010, 15, 1458–1463. [Google Scholar] [CrossRef]
- Stromdahl, S.; Liljeros, F.; Thorson, A.E.; Persson, K.I.; Forsberg, B.C. HIV testing and prevention among foreign-born men who have sex with men: An online survey from sweden. BMC Public Health 2017, 17, 139. [Google Scholar] [CrossRef]
- van Griensven, F.; Guadamuz, T.E.; de Lind van Wijngaarden, J.W.; Phanuphak, N.; Solomon, S.S.; Lo, Y.-R. Challenges and emerging opportunities for the HIV prevention, treatment and care cascade in men who have sex with men in asia pacific. Sex. Transm. Infect. 2017, 93, 356–362. [Google Scholar] [CrossRef]
- Åkerman, E.; Essén, B.; Westerling, R.; Larsson, E. Healthcare-seeking behaviour in relation to sexual and reproductive health among thai-born women in sweden: A qualitative study. Cult. Health Sex. 2017, 19, 194–207. [Google Scholar] [CrossRef]
- Korner, H. Late HIV diagnosis of people from culturally and linguistically diverse backgrounds in sydney: The role of culture and community. AIDS Care 2007, 19, 168–178. [Google Scholar] [CrossRef]
- Mengesha, Z.B.; Dune, T.; Perz, J. Culturally and linguistically diverse women’s views and experiences of accessing sexual and reproductive health care in australia: A systematic review. Sex. Health 2016, 13, 299–310. [Google Scholar] [CrossRef]
- Henderson, S.; Kendall, E. Culturally and linguistically diverse peoples’ knowledge of accessibility and utilisation of health services: Exploring the need for improvement in health service delivery. Aust. J. Prim. Health 2011, 17, 195–201. [Google Scholar] [CrossRef]
- Vearey, J. Moving forward: Why responding to migration, mobility and HIV in south(ern) africa is a public health priority. J. Int. AIDS Soc. 2018, 21, e25137. [Google Scholar] [CrossRef]
- Gupta, G.R.; Parkhurst, J.O.; Ogden, J.A.; Aggleton, P.; Mahal, A. Structural approaches to HIV prevention. Lancet 2008, 372, 764–775. [Google Scholar] [CrossRef]
- Parkhurst, J.O. Structural approaches for prevention of sexually transmitted HIV in general populations: Definitions and an operational approach. J. Int. AIDS Soc. 2014, 17, 19052. [Google Scholar] [CrossRef]


{kind=link}
| Databases: | PsycINFO, MEDLINE, ProQuest, Scopus, Global Health and Web of Science |
| Migrants: | refugee * or “international students” or “ethnic group *“ or “culturally and linguistically diverse” or “non English speaking” or “ethnic minorit *“ or “transient* and migrant *“ or immigrant * or emigrant * or “asylum seeker *“ or “migrant workers” or overseas |
| Intervention: | interven * or evaluate * or “health promot *“ or “public health” or polic * or prevent * or “best practi? e” or “good practi? e” |
| Sexual Health Issues: | “sexually transmitted disease *“ or “sexually transmitted infection *“ or “venereal disease *“ or “sexually transmissible infection *“ or “sexually transmissible disease *“ or “genital disease *“ or “human immunodeficiency virus” or “hepatitis B virus” or “blood borne virus” or STIs or HIV or STDs or BBVs |
| Intervention Types | Definition and Examples | Number of Studies (n) | Citations |
|---|---|---|---|
| Individual | Included clinical interventions, such as testing, vaccination and treatment uptake or adherence. | 8 | [43,44,45,46,47,48,49,50] |
| Community | Included mass media and group or peer education | 6 | [50,51,52,53,54,55] |
| Structural | Included interventions addressing broader social, economic and political environments | 3 | [56,57,58] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghimire, S.; Hallett, J.; Gray, C.; Lobo, R.; Crawford, G. What Works? Prevention and Control of Sexually Transmitted Infections and Blood-Borne Viruses in Migrants from Sub-Saharan Africa, Northeast Asia and Southeast Asia Living in High-Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071287
Ghimire S, Hallett J, Gray C, Lobo R, Crawford G. What Works? Prevention and Control of Sexually Transmitted Infections and Blood-Borne Viruses in Migrants from Sub-Saharan Africa, Northeast Asia and Southeast Asia Living in High-Income Countries: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(7):1287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071287
Chicago/Turabian StyleGhimire, Sajana, Jonathan Hallett, Corie Gray, Roanna Lobo, and Gemma Crawford. 2019. "What Works? Prevention and Control of Sexually Transmitted Infections and Blood-Borne Viruses in Migrants from Sub-Saharan Africa, Northeast Asia and Southeast Asia Living in High-Income Countries: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 7: 1287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071287