Impact of Outpatient Rehabilitation Service in Preventing the Deterioration of the Care-Needs Level Among Japanese Older Adults Availing Long-Term Care Insurance: A Propensity Score Matched Retrospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
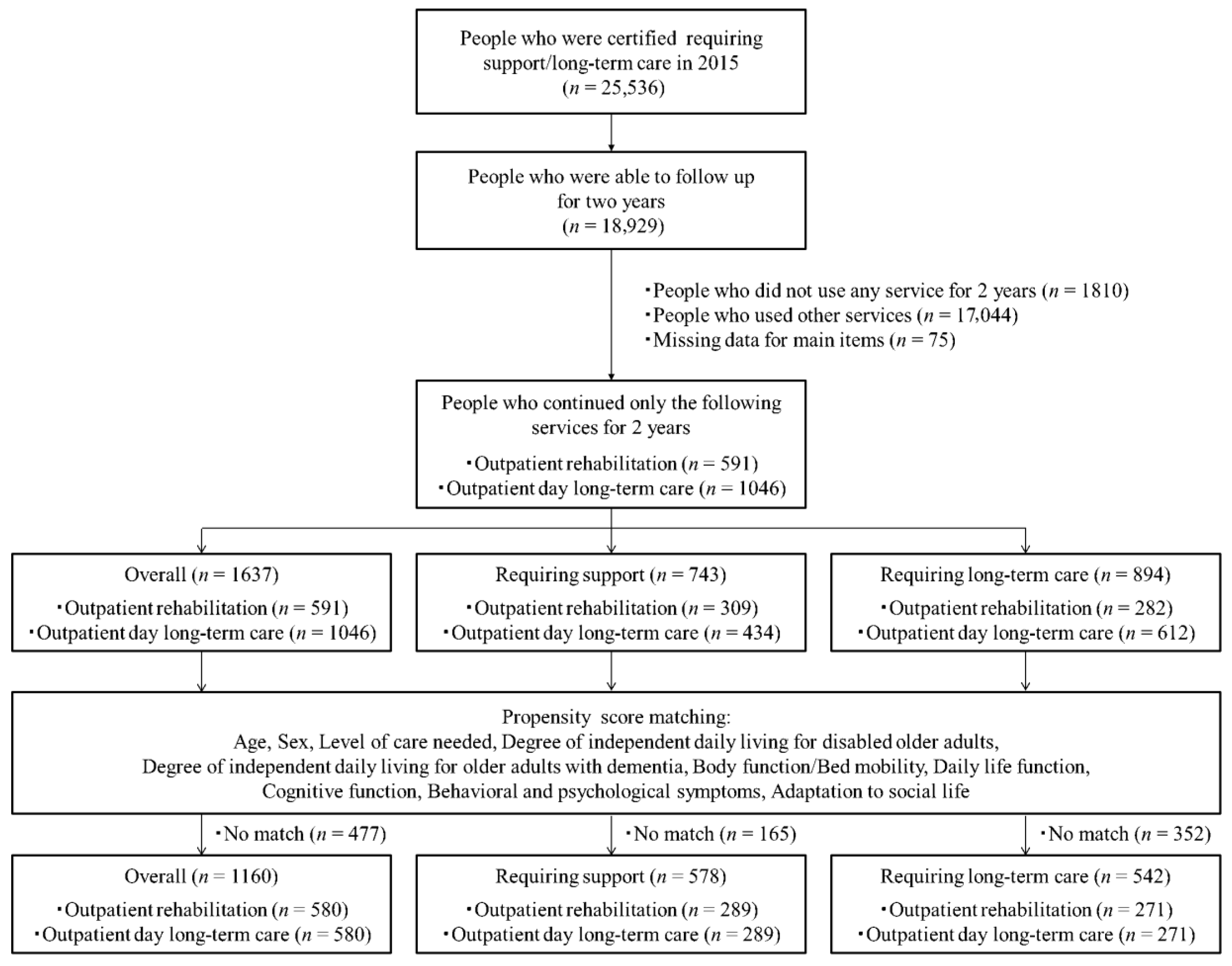
2.1. Study Population and Data Sources
2.2. Measurement
2.2.1. Body Function/Bed Mobility
2.2.2. Daily Life Function
2.2.3. Cognitive Function
2.2.4. Behavioral and Psychological Symptoms
2.2.5. Adaptation to Social Life
2.2.6. Degree of Independent Daily Living for Disabled Older Adults
2.2.7. Degree of Independent Daily Living for Older Adults with Dementia
2.3. Propensity Score Matching
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics Before and After Propensity Score Matching
3.2. Changes in Certification Survey Item Scores after 2 Years
3.3. Comparisons of the Certification Survey Items after Two Years Between Outpatient OR and ODLC Service Users
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Aging and Health 2015. Available online: https://www.who.int/ageing/events/world-report-2015-launch/en/ (accessed on 11 January 2019).
- Ikeda, N.; Saito, E.; Kondo, N.; Inoue, M.; Ikeda, S.; Satoh, T.; Wada, K.; Stickley, A.; Katanoda, K.; Mizoue, T.; et al. What has made the population of Japan healthy? Lancet 2011, 378, 1094–1105. [Google Scholar] [CrossRef]
- Tamiya, N.; Noguchi, H.; Nishi, A.; Reich, M.R.; Ikegami, N.; Hashimoto, H.; Shibuya, K.; Kawachi, I.; Campbell, J.C. Population ageing and wellbeing: Lessons from Japan's long-term care insurance policy. Lancet 2011, 378, 1183–1192. [Google Scholar] [CrossRef]
- Cabinet Office. Heisei 30 White Paper on Aging society. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2018/html/zenbun/index.html (accessed on 11 January 2019).
- Carlson, C.; Merel, S.E.; Yukawa, M. Geriatric syndromes and geriatric assessment for the generalist. Med. Clin. N. Am. 2015, 99, 263–279. [Google Scholar] [CrossRef]
- Campbell, J.C.; Ikegami, N. Long-term care insurance comes to Japan. Health Aff. (Millwood) 2000, 19, 26–39. [Google Scholar] [CrossRef] [Green Version]
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Nakao, H.; Yahata, Y.; Imai, H. In-depth descriptive analysis of trends in prevalence of long-term care in Japan. Geriatr. Gerontol. Int. 2008, 8, 166–171. [Google Scholar] [CrossRef]
- Ikegami, N. Rationale, design and sustainability of Long-Term Care Insurance in Japan-in Retrospect. Soc. Policy Soc. 2007, 6, 423–434. [Google Scholar] [CrossRef]
- Website of the Ministry of Health, Labour and Welfare. Long-Term Care, Health and Welfare Services for the Elderly. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/index.html (accessed on 14 January 2019).
- Harris-Kojetin, L.; Sengupta, M.; Park-Lee, E.; Valverde, R.; Caffrey, C.; Rome, V.; Lendon, J. Long-Term Care Providers and services users in the United States: Data from the National Study of Long-Term Care Providers, 2013-2014. Vital Health Stat. 3 2016, 38, 1–105. [Google Scholar]
- Behrndt, E.M.; Straubmeier, M.; Seidl, H.; Book, S.; Graessel, E.; Luttenberger, K. The German day-care study: Multicomponent non-drug therapy for people with cognitive impairment in day-care centres supplemented with caregiver counselling (DeTaMAKS)—Study protocol of a cluster-randomised controlled trial. BMC Health Serv. Res. 2017, 17, 492. [Google Scholar] [CrossRef]
- Lee, T.W.; Yim, E.S.; Choi, H.S.; Chung, J. Day care vs home care: Effects on functional health outcomes among long-term care beneficiaries with dementia in Korea. Int. J. Geriatr. Psychiatry 2019, 34, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Jarrott, S.E.; Zarit, S.H.; Stephens, M.A.; Townsend, A.; Greene, R. Adult day service use and reductions in caregiving hours: Effects on stress and psychological well-being for dementia caregivers. Int. J. Geriatr. Psychiatry 2003, 18, 55–62. [Google Scholar] [CrossRef]
- Tretteteig, S.; Vatne, S.; Rokstad, A.M. The influence of day care centres designed for people with dementia on family caregivers—A qualitative study. BMC Geriatr. 2017, 17, 5. [Google Scholar] [CrossRef]
- Mossello, E.; Caleri, V.; Razzi, E.; Di Bari, M.; Cantini, C.; Tonon, E.; Lopilato, E.; Marini, M.; Simoni, D.; Cavallini, M.C.; et al. Day care for older dementia patients: Favorable effects on behavioral and psychological symptoms and caregiver stress. Int. J. Geriatr. Psychiatry. 2008, 23, 1066–1072. [Google Scholar] [CrossRef]
- Zarit, S.H.; Kim, K.; Femia, E.E.; Almeida, D.M.; Savla, J.; Molenaar, P.C. Effects of adult day care on daily stress of caregivers: A within-person approach. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 538–546. [Google Scholar] [CrossRef]
- Zank, S.; Schacke, C. Evaluation of geriatric day care units: Effects on patients and caregivers. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, 348–357. [Google Scholar] [CrossRef]
- Femia, E.E.; Zarit, S.H.; Stephens, M.A.; Greene, R. Impact of adult day services on behavioral and psychological symptoms of dementia. Gerontologist 2007, 47, 775–788. [Google Scholar] [CrossRef]
- Kasai, M.; Meguro, K.; Akanuma, K.; Yamaguchi, S. Alzheimer's disease patients institutionalized in group homes run by long-term care insurance exhibit fewer symptoms of behavioural problems as evaluated by the Behavioural Pathology in Alzheimer's Disease Rating Scale. Psychogeriatrics 2015, 15, 102–108. [Google Scholar] [CrossRef]
- Logsdon, R.G.; Pike, K.C.; Korte, L.; Goehring, C. Memory care and wellness services: Efficacy of specialized dementia care in adult day services. Gerontologist 2016, 56, 318–325. [Google Scholar] [CrossRef]
- Fields, N.L.; Anderson, K.A.; Dabelko-Schoeny, H. The effectiveness of adult day services for older adults: A review of the literature from 2000 to 2011. J. Appl. Gerontol. 2014, 33, 130–163. [Google Scholar] [CrossRef]
- Website of the Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/file/05-Shingikai-12601000-Seisakutoukatsukan-Sanjikanshitsu_Shakaihoshoutantou/0000168706.pdf (accessed on 14 January 2019).
- Website of the Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/file/05-Shingikai-12601000-Seisakutoukatsukan-Sanjikanshitsu_Shakaihoshoutantou/0000168705.pdf (accessed on 14 January 2019).
- Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/file/05-Shingikai-12601000-Seisakutoukatsukan-Sanjikanshitsu_Shakaihoshoutantou/0000126194.pdf (accessed on 14 January 2019).
- Gitlin, L.N.; Hauck, W.W.; Winter, L.; Dennis, M.P.; Schulz, R. Effect of an in-home occupational and physical therapy intervention on reducing mortality in functionally vulnerable older people: Preliminary findings. J. Am. Geriatr. Soc. 2006, 54, 950–955. [Google Scholar] [CrossRef]
- Sanford, J.A.; Griffiths, P.C.; Richardson, P.; Hargraves, K.; Butterfield, T.; Hoenig, H. The effects of in-home rehabilitation on task self-efficacy in mobility-impaired adults: A randomized clinical trial. J. Am. Geriatr. Soc. 2006, 54, 1641–1648. [Google Scholar] [CrossRef]
- Akune, T.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Tokimura, F.; Yoshida, H.; Suzuki, T.; Nakamura, K.; Yoshimura, N. Incidence of certified need of care in the long-term care insurance system and its risk factors in the elderly of Japanese population-based cohorts: The ROAD study. Geriatr. Gerontol. Int. 2014, 14, 695–701. [Google Scholar] [CrossRef]
- Akune, T.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Tokimura, F.; Yoshida, H.; Suzuki, T.; Nakamura, K.; Yoshimura, N. Association of physical activities of daily living with the incidence of certified need of care in the long-term care insurance system of Japan: The ROAD study. J. Orthop. Sci. 2014, 19, 489–496. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Sonoda, T.; Kayama, H.; Tanigawa, T.; Yukutake, T.; Aoyama, T. Cognitive decline predicts long-term care insurance requirement certification in community-dwelling older Japanese adults: A prospective cohort study. Dement Geriatr. Cogn. Dis. Extra 2013, 3, 312–319. [Google Scholar] [CrossRef]
- Lin, H.R.; Otsubo, T.; Imanaka, Y. Survival analysis of increases in care needs associated with dementia and living alone among older long-term care service users in Japan. BMC Geriatr. 2017, 17, 182. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, S.; Fujino, Y.; Kubo, T. Analysis of factors associated with changes in dependency level among the slightly frail elderly using the LTCI Services in Japan. Asian Pac. J. Dis. Manag. 2009, 3, 39–45. [Google Scholar] [CrossRef]
- Lin, HR.; Otsubo, T.; Imanaka, Y. The effects of dementia and long-term care services on the deterioration of care-needs levels of the elderly in Japan. Medicine 2015, 94, e525. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Suzuki, T. Impact of physical frailty on disability in community-dwelling older adults: A prospective cohort study. BMJ Open 2015, 5, e008462. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Lee, S.; Doi, T.; Nakakubo, S.; Hotta, R.; Suzuki, T. Social Frailty in community-dwelling older adults as a risk factor for disability. J. Am. Med. Dir Assoc. 2015, 16, 1003.e7–1003.e11. [Google Scholar] [CrossRef]
- Kato, G.; Tamiya, N.; Kashiwagi, M.; Sato, M.; Takahashi, H. Relationship between home care service use and changes in the care needs level of Japanese elderly. BMC Geriatr. 2009, 9, 58. [Google Scholar] [CrossRef]
- Kuzuya, M.; Masuda, Y.; Hirakawa, Y.; Iwata, M.; Enoki, H.; Hasegawa, J.; Iguchi, A. Day care service use is associated with lower mortality in community-dwelling frail older people. J. Am. Geriatr. Soc. 2006, 54, 1364–1371. [Google Scholar] [CrossRef]
- Kim, J.N.; Shiwaku, K. The effect of utilization of in-home services and the changes in levels of care needs of frail persons (2002-2004): Results of a two-year follow-up study. J. Rural Med. 2012, 7, 6–14. [Google Scholar] [CrossRef]
- Koike, S.; Furui, Y. Long-term care-service use and increases in care-need level among home-based elderly people in a Japanese urban area. Health Policy 2013, 110, 94–100. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Dementia; Assessment, Management and Support for People Living with Dementia and Their Carers (NICE Guideline NG97). Available online: https://www.nice.org.uk/guidance/ng97 (accessed on 29 January 2019).
- Dutzi, I.; Schwenk, M.; Kirchner, M.; Bauer, J.M.; Hauer, K. Cognitive change in rehabilitation patients with dementia: Prevalence and association with rehabilitation success. J. Alzheimers Dis. 2017, 60, 1171–1182. [Google Scholar] [CrossRef]
- Rodakowski, J.; Saghafi, E.; Butters, M.A.; Skidmore, E.R. Non-pharmacological interventions for adults with mild cognitive impairment and early stage dementia: An updated scoping review. Mol. Aspects Med. 2015, 43–44, 38–53. [Google Scholar] [CrossRef]
- Website of the Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-12300000-Roukenkyoku/0000077237.pdf (accessed on 14 January 2019).
- Sakka, M.; Goto, J.; Kita, S.; Sato, I.; Soejima, T.; Kamibeppu, K. Associations among behavioral and psychological symptoms of dementia, care burden, and family-to-work conflict of employed family caregivers. Geriatr. Gerontol. Int. 2019, 19, 51–55. [Google Scholar] [CrossRef]
- Matsumoto, N.; Ikeda, M.; Fukuhara, R.; Shinagawa, S.; Ishikawa, T.; Mori, T.; Toyota, Y.; Matsumoto, T.; Adachi, H.; Hirono, N.; et al. Caregiver burden associated with behavioral and psychological symptoms of dementia in elderly people in the local community. Dement Geriatr. Cogn. Disord. 2007, 23, 219–224. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kazui, H.; Yoshiyama, K.; Azuma, S.; Kanemoto, H.; Sato, S.; Suehiro, T.; Ikeda, M. Advantages of different care services for reducing neuropsychiatric symptoms in dementia patients. Psychogeriatrics 2018, 18, 252–258. [Google Scholar] [CrossRef]
- Fauth, E.B.; Gibbons, A. Which behavioral and psychological symptoms of dementia are the most problematic? Variability by prevalence, intensity, distress ratings, and associations with caregiver depressive symptoms. Int. J. Geriatr. Psychiatry 2014, 29, 263–271. [Google Scholar] [CrossRef]
- Wang, J.; Xiao, L.D.; Li, X.; De Bellis, A.; Ullah, S. Caregiver distress and associated factors in dementia care in the community setting in China. Geriatr. Nurs. 2015, 36, 348–354. [Google Scholar] [CrossRef]
- Dillon, C.; Serrano, C.M.; Castro, D.; Leguizamón, P.P.; Heisecke, S.L.; Taragano, F.E. Behavioral symptoms related to cognitive impairment. Neuropsychiatr. Dis. Treat. 2013, 9, 1443–1455. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, R.; Miura, Y. The effect of exercise intervention on frail elderly in need of care: Half-day program in a senior day-care service facility specializing in functional training. J. Phys. Ther. Sci. 2016, 28, 1957–1963. [Google Scholar] [CrossRef]
- Kikuzawa, S.; Sawai, M.; Fujii, K.; Matsubara, C. Effect of service use under long-term care insurance among those with light disability level: Analyses of change in disability level using panel data. Jpn. J. Gerontol. 2007, 29, 375–383. [Google Scholar]
- Tomita, N.; Yoshimura, K.; Ikegami, N. Impact of home and community-based services on hospitalisation and institutionalisation among individuals eligible for long-term care insurance in Japan. BMC Health Serv. Res. 2010, 10, 345. [Google Scholar] [CrossRef]
- Yeh, S.C.; Liu, Y.Y. Influence of social support on cognitive function in the elderly. BMC Health Serv. Res. 2003, 3, 9. [Google Scholar] [CrossRef]
- Koukouli, S.; Vlachonikolis, I.G.; Philalithis, A. Socio-demographic factors and self-reported functional status: The significance of social support. BMC Health Serv. Res. 2002, 2, 20. [Google Scholar] [CrossRef]


{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| OR Service User (n = 591) | ODLC Service User (n = 1046) | p-Value | OR Service User (n = 580) | ODLC Service User (n = 580) | p-Value | |
| Age, years, mean (SD) | 82.1(7.0) | 82.7(6.5) | 0.086 | 82.1(7.0) | 82.2(6.6) | 0.796 |
| Female sex, n(%) | 376(63.6) | 782(74.8) | 0.000 | 375(64.7) | 385(66.4) | 0.537 |
| Body function/Bed mobility, mean (SD) | 19.6(3.9) | 19.0(4.0) | 0.007 | 19.5(3.8) | 19.3(4.0) | 0.430 |
| Daily life function, mean (SD) | 14.3(3.8) | 14.1(3.4) | 0.440 | 14.2(3.5) | 14.1(3.4) | 0.819 |
| Cognitive function, mean (SD) | 9.6(1.2) | 9.7(1.2) | 0.010 | 9.6(1.2) | 9.6(1.2) | 0.820 |
| Behavioral and psychological symptoms, mean (SD) | 17.8(3.4) | 18.7(3.7) | 0.000 | 17.8(3.4) | 17.9(3.3) | 0.535 |
| Adaptation to social life, mean (SD) | 12.4(3.5) | 12.5(3.5) | 0.509 | 12.4(3.5) | 12.2(3.6) | 0.345 |
| Level of care needed, n (%) | 0.000 | 0.402 | ||||
| Requiring support 1 | 134(22.7) | 213(20.4) | 133(22.9) | 142(24.5) | ||
| Requiring support 2 | 175(29.6) | 221(21.1) | 171(29.5) | 162(27.9) | ||
| Requiring long-term care 1 | 164(27.7) | 405(38.7) | 163(28.1) | 177(30.5) | ||
| Requiring long-term care 2 | 100(16.9) | 165(15.8) | 98(16.9) | 83(14.3) | ||
| Requiring long-term care 3 | 13(2.2) | 37(3.5) | 13(2.2) | 11(1.9) | ||
| Requiring long-term care 4 | 3(0.5) | 5(0.5) | 1(0.2) | 5(0.9) | ||
| Requiring long-term care 5 | 2(0.3) | 0(0) | 1(0.2) | 0(0) | ||
| Degree of independent daily living for disabled older adults, n (%) | 0.434 | 0.995 | ||||
| J1 | 3(0.5) | 10(1.0) | 3(0.5) | 4(0.7) | ||
| J2 | 198(33.5) | 356(34.0) | 198(34.1) | 200(34.5) | ||
| A1 | 197(33.3) | 377(36.0) | 194(33.4) | 197(34.0) | ||
| A2 | 167(28.3) | 266(25.4) | 163(28.1) | 156(26.9) | ||
| B1 | 18(3.0) | 30(2.9) | 17(2.9) | 17(2.9) | ||
| B2 | 7(1.2) | 7(0.7) | 5(0.9) | 6(1.0) | ||
| C1 | 1(0.2) | 0(0) | 0(0) | 0(0) | ||
| C2 | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Degree of independent daily living for older adults with dementia, n (%) | 0.000 | 0.996 | ||||
| Indepedence | 144(24.4) | 200(19.1) | 140(24.1) | 137(23.6) | ||
| I | 190(32.1) | 236(22.6) | 185(31.9) | 185(31.9) | ||
| IIa | 61(10.3) | 122(11.7) | 61(10.5) | 60(10.3) | ||
| IIb | 133(22.5) | 354(33.8) | 132(22.8) | 137(23.6) | ||
| IIIa | 55(9.3) | 115(11.0) | 55(9.5) | 56(9.7) | ||
| IIIb | 6(1.0) | 14(1.3) | 5(0.9) | 3(0.5) | ||
| IV | 2(0.3) | 5(0.5) | 2(0.3) | 2(0.3) | ||
| M | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| OR Service User (n = 309) | ODLC Service User (n = 434) | p-Value | OR Service User (n = 289) | ODLC Service User (n = 289) | p-Value | |
| Age, years, mean (SD) | 81.9(6.9) | 82.2(6.2) | 0.580 | 82.0(6.9) | 82.1(6.4) | 0.807 |
| Female sex, n (%) | 213(68.9) | 351(80.9) | 0.000 | 208(72.0) | 214(74.0) | 0.574 |
| Body function/Bed mobility, mean (SD) | 18.8(3.1) | 18.4(3.0) | 0.078 | 18.7(3.0) | 18.7(3.0) | 0.764 |
| Daily life function, mean (SD) | 12.7(1.3) | 12.6(1.2) | 0.461 | 12.7(1.3) | 12.7(1.2) | 0.920 |
| Cognitive function, mean (SD) | 9.1(0.3) | 9.1(0.2) | 0.594 | 9.0(0.2) | 9.0(0.2) | 1.000 |
| Behavioral and psychological symptoms, mean (SD) | 15.9(1.6) | 16.2(1.9) | 0.017 | 16.0(1.6) | 16.0(1.5) | 0.895 |
| Adaptation to social life, mean (SD) | 10.6(3.3) | 10.1(3.2) | 0.043 | 10.4(3.2) | 10.2(3.2) | 0.503 |
| Level of care needed, n (%) | 0.124 | 0.182 | ||||
| Requiring support 1 | 134(43.4) | 213(49.1) | 127(43.9) | 143(49.5) | ||
| Requiring support 2 | 175(56.6) | 221(50.9) | 162(56.1) | 146(50.5) | ||
| Degree of independent daily living for disabled older adults, n (%) | 0.253 | 0.989 | ||||
| J1 | 2(0.6) | 8(1.8) | 2(0.7) | 3(1.0) | ||
| J2 | 147(47.6) | 211(48.6) | 139(48.1) | 141(48.8) | ||
| A1 | 92(29.8) | 143(32.9) | 89(30.8) | 85(29.4) | ||
| A2 | 65(21.0) | 69(15.9) | 58(20.1) | 59(20.4) | ||
| B1 | 3(1.0) | 2(0.5) | 1(0.3) | 1(0.3) | ||
| B2 | 0(0) | 1(0.2) | 0(0) | 0(0) | ||
| C1 | 0(0) | 0(0) | 0(0) | 0(0) | ||
| C2 | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Degree of independent daily living for older adults with dementia, n (%) | 0.292 | 0.928 | ||||
| Indepedence | 131(42.4) | 193(44.5) | 128(44.3) | 128(44.3) | ||
| I | 144(46.6) | 182(41.9) | 131(45.3) | 133(46.0) | ||
| IIa | 23(7.4) | 29(6.7) | 19(6.6) | 19(6.6) | ||
| IIb | 10(3.2) | 28(6.5) | 10(3.5) | 7(2.4) | ||
| IIIa | 1(0.3) | 2(0.5) | 1(0.3) | 2(0.7) | ||
| IIIb | 0(0) | 0(0) | 0(0) | 0(0) | ||
| IV | 0(0) | 0(0) | 0(0) | 0(0) | ||
| M | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| OR Service User (n = 282) | ODLC Service User (n = 612) | p-Value | OR Service User (n = 271) | ODLC Service User (n = 271) | p-Value | |
| Age, years, mean (SD) | 82.3(7.0) | 83.1(6.7) | 0.119 | 82.4(7.0) | 82.6(7.3) | 0.695 |
| Female sex, n (%) | 163(57.8) | 431(70.4) | 0.000 | 161(59.4) | 166(61.3) | 0.661 |
| Body function/Bed mobility, mean (SD) | 20.4(4.5) | 19.5(4.6) | 0.003 | 20.2(4.3) | 20.5(4.7) | 0.416 |
| Daily life function, mean (SD) | 16.0(4.7) | 15.2(4.0) | 0.013 | 15.8(4.4) | 15.6(4.2) | 0.542 |
| Cognitive function, mean (SD) | 10.1(1.5) | 10.2(1.4) | 0.434 | 10.2(1.5) | 10.1(1.4) | 0.479 |
| Behavioral and psychological symptoms, mean (SD) | 19.8(3.7) | 20.4(3.7) | 0.018 | 19.9(3.7) | 19.9(3.5) | 0.914 |
| Adaptation to social life, mean (SD) | 14.4(2.3) | 14.3(2.6) | 0.356 | 14.4(2.3) | 14.2(2.6) | 0.297 |
| Level of care needed, n (%) | 0.019 | 0.706 | ||||
| Requiring long-term care 1 | 164(58.2) | 405(66.2) | 162(59.8) | 165(60.9) | ||
| Requiring long-term care 2 | 100(35.5) | 165(27.0) | 94(34.7) | 87(32.1) | ||
| Requiring long-term care 3 | 13(4.6) | 37(6.0) | 12(4.4) | 17(6.3) | ||
| Requiring long-term care 4 | 3(1.1) | 5(0.8) | 2(0.7) | 2(0.7) | ||
| Requiring long-term care 5 | 2(0.7) | 0(0) | 1(0.4) | 0(0) | ||
| Degree of independent daily living for disabled older adults, n (%) | 0.167 | 0.947 | ||||
| J1 | 1(0.4) | 2(0.3) | 1(0.4) | 2(0.7) | ||
| J2 | 51(18.1) | 145(23.7) | 50(18.5) | 49(18.1) | ||
| A1 | 105(37.2) | 234(38.2) | 102(37.6) | 96(35.4) | ||
| A2 | 102(36.2) | 197(32.2) | 99(36.5) | 102(37.6) | ||
| B1 | 15(5.3) | 28(4.6) | 14(5.2) | 18(6.6) | ||
| B2 | 7(2.5) | 6(1.0) | 5(1.8) | 4(1.5) | ||
| C1 | 1(0.4) | 0(0) | 0(0) | 0(0) | ||
| C2 | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Degree of independent daily living for older adults with dementia, n (%) | 0.000 | 0.996 | ||||
| Indepedence | 13(4.6) | 7(1.1) | 7(2.6) | 7(2.6) | ||
| I | 46(16.3) | 54(8.8) | 42(15.5) | 38(14.0) | ||
| IIa | 38(13.5) | 93(15.2) | 38(14.0) | 40(14.8) | ||
| IIb | 123(43.6) | 326(53.3) | 123(45.4) | 125(46.1) | ||
| IIIa | 54(19.1) | 113(18.5) | 54(19.9) | 55(20.3) | ||
| IIIb | 6(2.1) | 14(2.3) | 5(1.8) | 5(1.8) | ||
| IV | 2(0.7) | 5(0.8) | 2(0.7) | 1(0.4) | ||
| M | 0(0) | 0(0) | 0(0) | 0(0) | ||
| Overall | Requiring Support | Requiring Long-Term Care | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR Service User (n = 580) | ODLC Service User (n = 580) | OR Service User (n = 289) | ODLC Service User (n = 289) | OR Service User (n = 271) | ODLC Service User (n = 271) | |||||||||||||
| 2015 | 2017 | p-Value | 2015 | 2017 | p-Value | 2015 | 2017 | p-Value | 2015 | 2017 | p-Value | 2015 | 2017 | p-Value | 2015 | 2017 | p-Value | |
| Body function/Bed mobility, mean (SD) | 19.5(3.8) | 20.6(4.6) | 0.000 | 19.3(4.0) | 20.5(4.6) | 0.000 | 18.7(3.0) | 19.8(4.1) | 0.000 | 18.7(3.0) | 20.4(4.4) | 0.000 | 20.2(4.3) | 21.2(4.8) | 0.000 | 20.5(4.7) | 21.5(5.2) | 0.000 |
| Daily life function, mean (SD) | 14.2(3.5) | 15.6(5.8) | 0.000 | 14.1(3.4) | 15.7(5.7) | 0.000 | 12.7(1.3) | 14.0(5.0) | 0.000 | 12.7(1.2) | 14.4(5.4) | 0.000 | 15.8(4.4) | 17.2(6.1) | 0.000 | 15.6(4.2) | 17.5(6.5) | 0.000 |
| Cognitive function, mean (SD) | 9.6(1.2) | 9.9(1.6) | 0.000 | 9.6(1.2) | 9.9(1.5) | 0.000 | 9.0(0.2) | 9.2(0.7) | 0.000 | 9.0(0.2) | 9.3(0.9) | 0.000 | 10.2(1.5) | 10.6(2.0) | 0.000 | 10.1(1.4) | 10.6(1.8) | 0.000 |
| Behavioral and psychological symptoms, mean (SD) | 17.8(3.4) | 18.3(4.0) | 0.000 | 17.9(3.3) | 18.7(4.0) | 0.000 | 16.0(1.6) | 16.6(2.6) | 0.000 | 16.0(1.5) | 17.1(3.0) | 0.000 | 19.9(3.7) | 20.3(4.3) | 0.039 | 19.9(3.5) | 20.5(4.1) | 0.009 |
| Adaptation to social life, mean (SD) | 12.4(3.5) | 13.0(3.5) | 0.000 | 12.2(3.6) | 13.1(3.6) | 0.000 | 10.4(3.2) | 11.1(3.5) | 0.000 | 10.2(3.2) | 11.3(3.6) | 0.000 | 14.4(2.3) | 15.0(2.2) | 0.000 | 14.2(2.6) | 15.0(2.5) | 0.000 |
| Overall | Requiring Support | Requiring Long-Term Care | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR Service User (n = 580) | ODLC Service User (n = 580) | p-Value | OR Service User (n = 289) | ODLC Service User (n = 289) | p-Value | OR Service User (n = 271) | ODLC Service User (n = 271) | p-Value | |
| Body function/Bed mobility, mean (SD) | −1.08(3.49) | −1.19(3.59) | 0.613 | −1.17(3.52) | −1.64(4.09) | 0.133 | −1.00(3.28) | −0.98(3.62) | 0.941 |
| Daily life function, mean (SD) | −1.40(5.40) | −1.56(4.99) | 0.608 | −1.29(5.07) | −1.72(5.20) | 0.320 | −1.39(5.32) | −1.98(5.65) | 0.211 |
| Cognitive function, mean (SD) | −0.31(1.10) | −0.36(1.12) | 0.398 | −0.17(0.73) | −0.28(0.86) | 0.118 | −0.44(1.34) | −0.55(1.36) | 0.309 |
| Behavioral and psychological symptoms, mean (SD) | −0.52(2.73) | −0.82(3.12) | 0.084 | −0.63(2.22) | −1.10(2.68) | 0.022 | −0.41(3.23) | −0.55(3.46) | 0.608 |
| Adaptation to social life, mean (SD) | −0.59(2.18) | −0.87(2.28) | 0.029 | −0.69(2.37) | −1.09(2.73) | 0.060 | −0.55(1.78) | −0.77(1.67) | 0.143 |
| Changes in level of care needed, improve/maintain, n(%) | 402(69.3) | 348(60.0) | 0.001 | 191(66.1) | 138(47.8) | 0.000 | 197(72.7) | 197(72.7) | 1.000 |
| Changes in degree of independent daily living for disabled older adults, improve/maintain, n(%) | 458(79.0) | 434(74.8) | 0.095 | 229(79.2) | 211(73.0) | 0.079 | 213(78.6) | 209(77.1) | 0.679 |
| Changes in degree of independent daily living for older adults with dementia, improve/maintain, n(%) | 422(72.8) | 379(65.3) | 0.006 | 210(72.7) | 168(58.1) | 0.000 | 198(73.1) | 194(71.6) | 0.701 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maruta, M.; Tabira, T.; Makizako, H.; Sagari, A.; Miyata, H.; Yoshimitsu, K.; Han, G.; Yoshiura, K.; Kawagoe, M. Impact of Outpatient Rehabilitation Service in Preventing the Deterioration of the Care-Needs Level Among Japanese Older Adults Availing Long-Term Care Insurance: A Propensity Score Matched Retrospective Study. Int. J. Environ. Res. Public Health 2019, 16, 1292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071292
Maruta M, Tabira T, Makizako H, Sagari A, Miyata H, Yoshimitsu K, Han G, Yoshiura K, Kawagoe M. Impact of Outpatient Rehabilitation Service in Preventing the Deterioration of the Care-Needs Level Among Japanese Older Adults Availing Long-Term Care Insurance: A Propensity Score Matched Retrospective Study. International Journal of Environmental Research and Public Health. 2019; 16(7):1292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071292
Chicago/Turabian StyleMaruta, Michio, Takayuki Tabira, Hyuma Makizako, Akira Sagari, Hironori Miyata, Koji Yoshimitsu, Gwanghee Han, Kazuhiro Yoshiura, and Masahiro Kawagoe. 2019. "Impact of Outpatient Rehabilitation Service in Preventing the Deterioration of the Care-Needs Level Among Japanese Older Adults Availing Long-Term Care Insurance: A Propensity Score Matched Retrospective Study" International Journal of Environmental Research and Public Health 16, no. 7: 1292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071292