Metabolic Syndrome Biomarkers of World Trade Center Airway Hyperreactivity: A 16-Year Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
3. Results
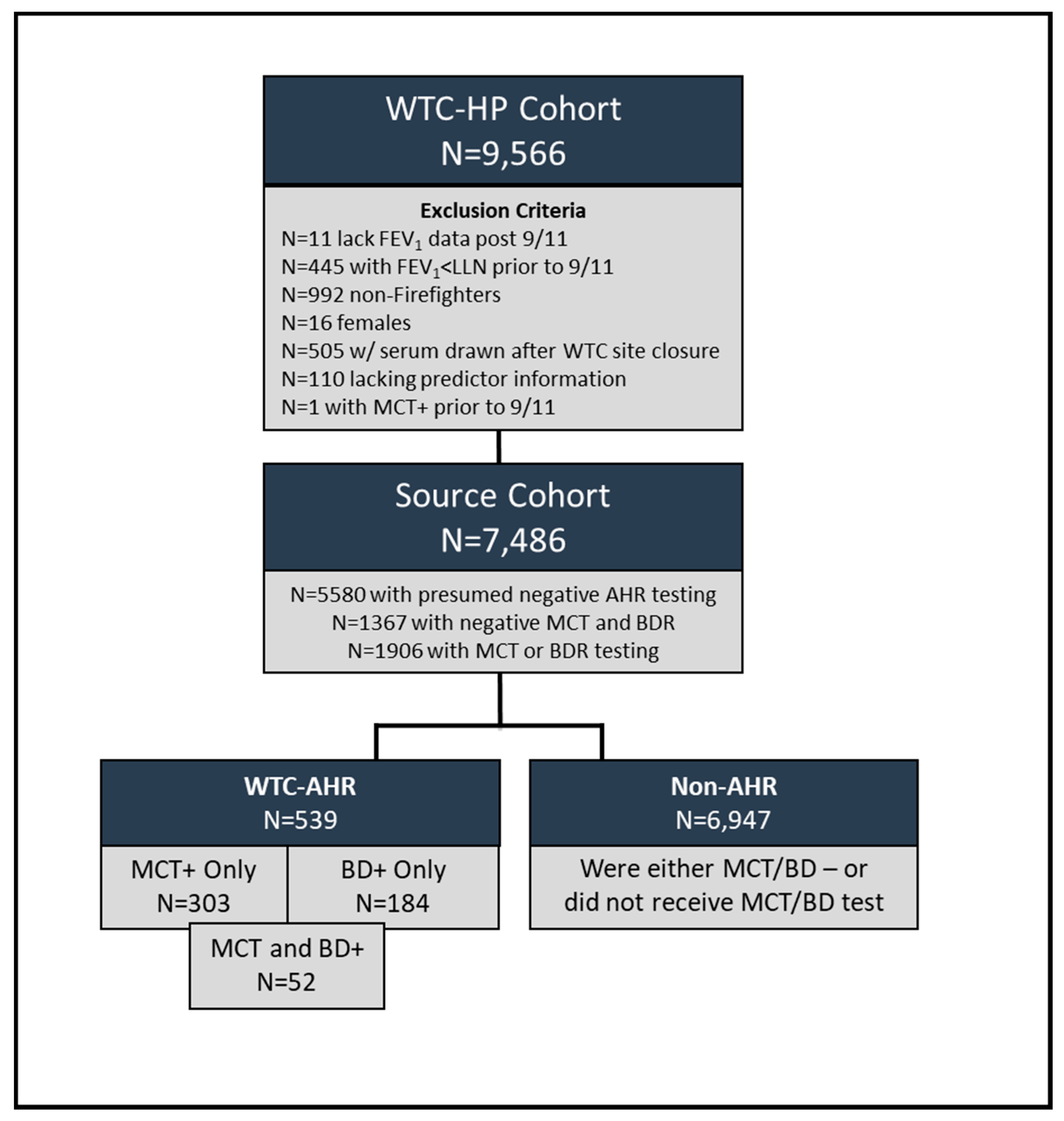
3.1. WTC-AHR Cohort
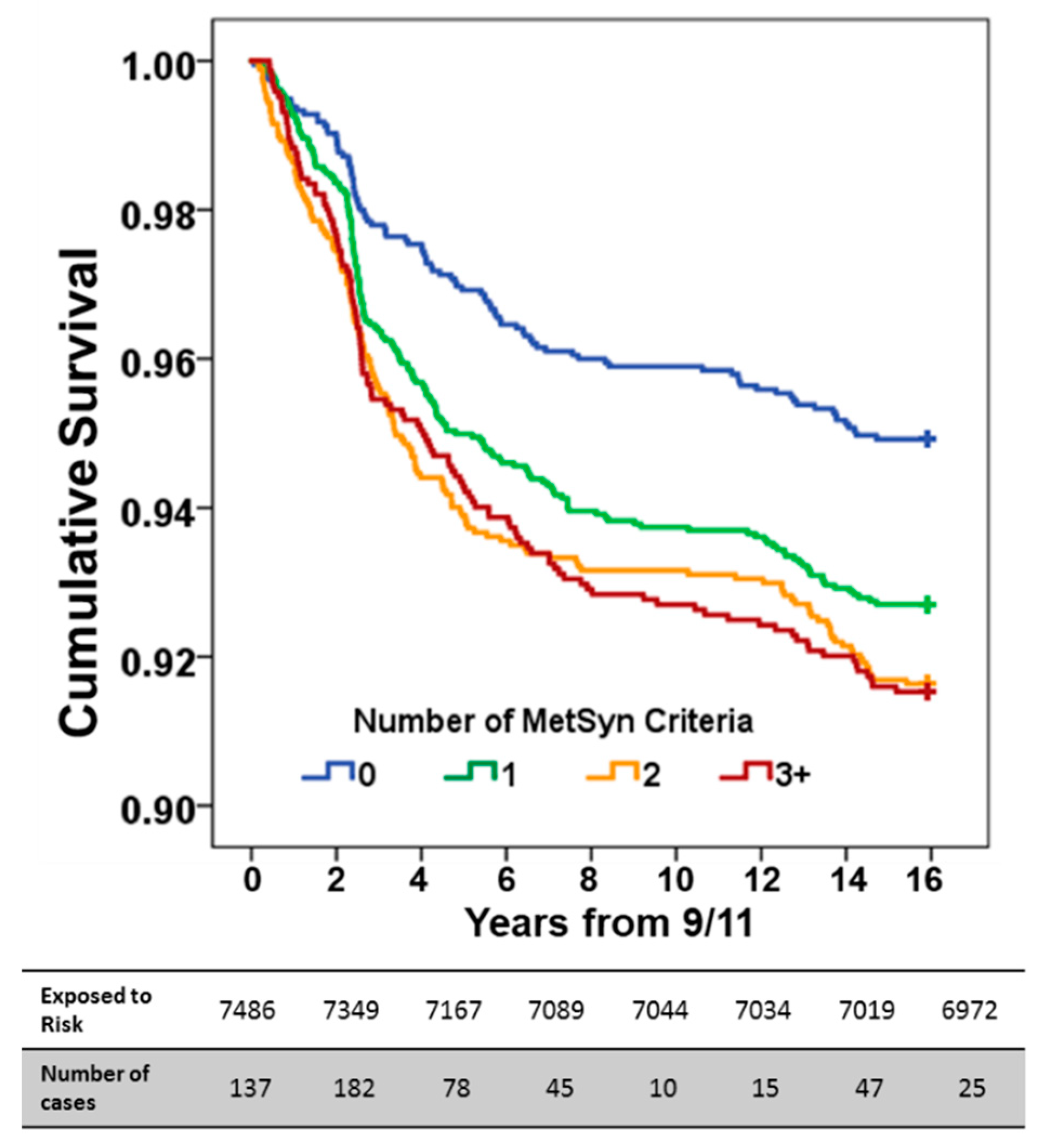
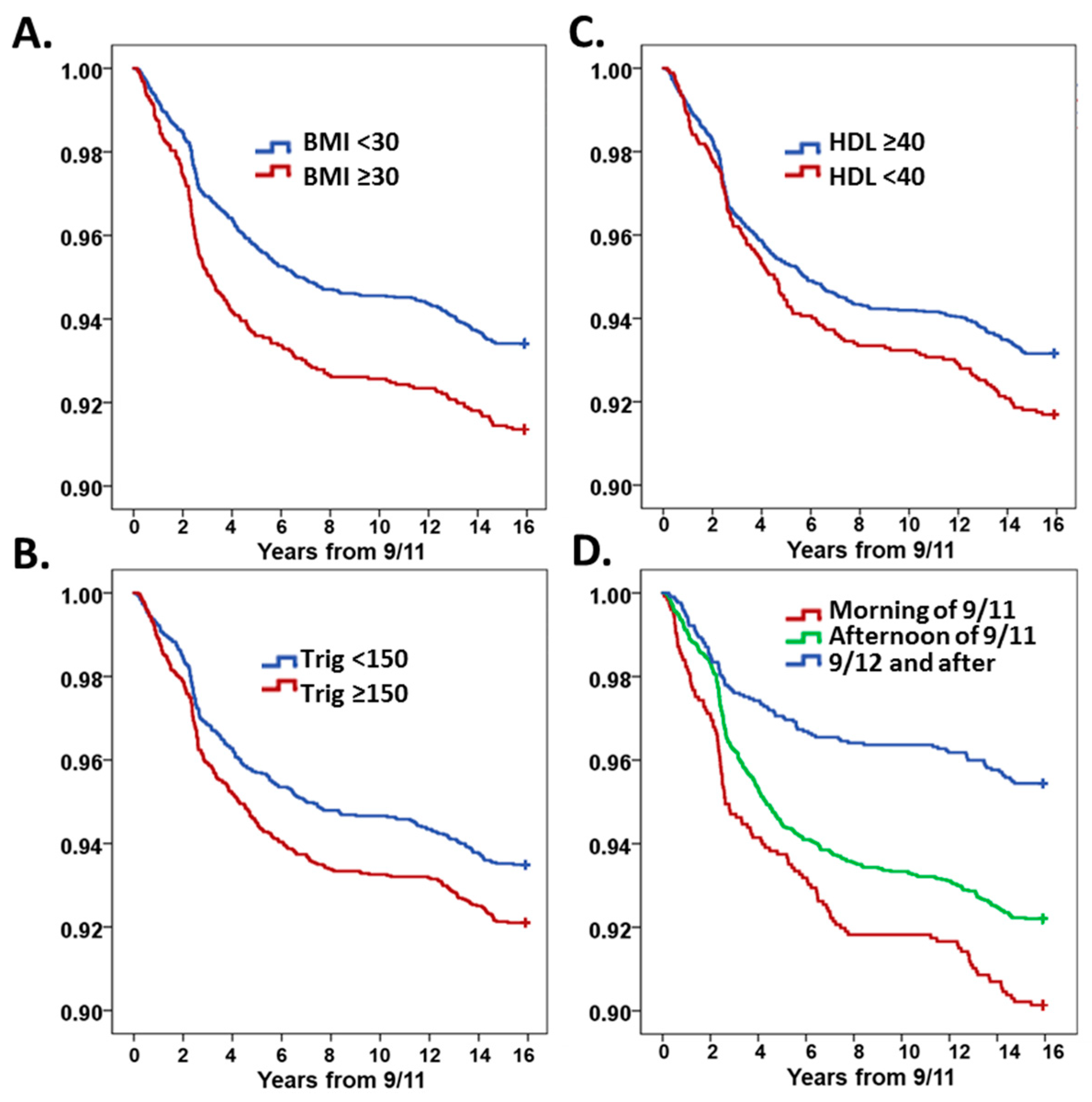
3.2. Model Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AHR | Airway hyperreactivity |
| ATP III | Adult treatment panel III |
| BDR | Bronchodilator response |
| BMI | Body mass index |
| CRP | C-reactive protein |
| CI | Confidence interval |
| DBP | Diastolic blood pressure |
| EMR | Electronic medical record |
| FDNY | Fire Department of City of New York |
| FEV1 | Forced expiratory volume over 1 second |
| FVC | Forced vital capacity |
| HDL | High density lipoprotein |
| HR | Hazards ratio |
| LDL | Low density lipoprotein |
| LLN | Lower limit of normal |
| MCT | Methacholine test |
| MetSyn | Metabolic syndrome |
| NCEP | National Cholesterol Education Program |
| OAD | Obstructive Airways Disease |
| PC20 | Methacholine dose required to reduce FEV1 by 20%. |
| PFT | Pulmonary function test |
| PM | Particulate matter |
| SBP | Systolic blood pressure |
| SD | Standard deviation |
| TNF | Tumor necrosis factor |
| US | United States |
| WBC | White blood cell |
| WHO | World Health Organization |
| WTC | World Trade Center |
| WTC-AHR | World Trade Center-airway hyperreactivity |
| WTC-HP | World Trade Center-health program |
| WTC-LI | WTC-lung injury |
References
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef] [PubMed]
- Dabass, A.; Talbott, E.O.; Rager, J.R.; Marsh, G.M.; Venkat, A.; Holguin, F.; Sharma, R.K. Systemic inflammatory markers associated with cardiovascular disease and acute and chronic exposure to fine particulate matter air pollution (PM2.5) among US NHANES adults with metabolic syndrome. Environ. Res. 2018, 161, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Crowley, G.; Caraher, E.J.; Haider, S.H.; Lam, R.; Veerappan, A.; Yang, L.; Liu, M.; Zeig-Owens, R.; Schwartz, T.; et al. Validation of Predictive Metabolic Syndrome Biomarkers of World Trade Center Lung Injury: A 16-Year Longitudinal Study. Chest 2019. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, R.S.; Colicino, E.; Zhong, J.; Kloog, I.; Coull, B.A.; Vokonas, P.; Schwartz, J.D.; Baccarelli, A.A. Ambient Fine Particulate Matter, Outdoor Temperature, and Risk of Metabolic Syndrome. Am. J. Epidemiol. 2017, 185, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Sun, Z.; Brook, J.R.; Zhao, X.; Ruan, Y.; Yan, J.; Mukherjee, B.; Rao, X.; Duan, F.; Sun, L.; et al. Extreme Air Pollution Conditions Adversely Affect Blood Pressure and Insulin Resistance: The Air Pollution and Cardiometabolic Disease Study. Hypertension 2016, 67, 77–85. [Google Scholar] [CrossRef]
- Leone, N.; Courbon, D.; Thomas, F.; Bean, K.; Jego, B.; Leynaert, B.; Guize, L.; Zureik, M. Lung function impairment and metabolic syndrome: The critical role of abdominal obesity. Am. J. Respir. Crit. Care Med. 2009, 179, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Zammit, C.; Liddicoat, H.; Moonsie, I.; Makker, H. Obesity and respiratory diseases. Int. J. Gen. Med. 2010, 3, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Baffi, C.W.; Wood, L.; Winnica, D.; Strollo, P.J., Jr.; Gladwin, M.T.; Que, L.G.; Holguin, F. Metabolic Syndrome and the Lung. Chest 2016, 149, 1525–1534. [Google Scholar] [CrossRef]
- Peters, U.; Suratt, B.T.; Bates, J.H.T.; Dixon, A.E. Beyond BMI: Obesity and Lung Disease. Chest 2017, 153, 702–709. [Google Scholar] [CrossRef]
- Garmendia, J.V.; Moreno, D.; Garcia, A.H.; De Sanctis, J.B. Metabolic syndrome and asthma. Recent Pat. Endocr. Metab. Immune Drug Discov. 2014, 8, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.L.; Wang, C.C.; Wu, L.W.; Kao, T.W.; Chan, J.Y.; Chen, Y.J.; Yang, Y.H.; Chang, Y.W.; Peng, T.C. Relationship between lung function and metabolic syndrome. PLoS ONE 2014, 9, e108989. [Google Scholar] [CrossRef]
- Lee, E.J.; In, K.H.; Ha, E.S.; Lee, K.J.; Hur, G.Y.; Kang, E.H.; Jung, K.H.; Lee, S.Y.; Kim, J.H.; Lee, S.Y.; et al. Asthma-like symptoms are increased in the metabolic syndrome. J. Asthma 2009, 46, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Adeyeye, O.O.; Ogbera, A.O.; Ogunleye, O.O.; Brodie-Mens, A.T.; Abolarinwa, F.F.; Bamisile, R.T.; Onadeko, B.O. Understanding asthma and the metabolic syndrome—A Nigerian report. Int. Arch. Med. 2012, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.H.; Jeong, J.; Baeg, M.K.; Han, K.D.; Kim, H.S.; Yoon, J.S.; Kim, H.H.; Kim, J.T.; Chun, Y.H. Lipid profiles in adolescents with and without asthma: Korea National Health and nutrition examination survey data. Lipids Health Dis. 2018, 17, 158. [Google Scholar] [CrossRef] [PubMed]
- Thuesen, B.H.; Husemoen, L.L.; Hersoug, L.G.; Pisinger, C.; Linneberg, A. Insulin resistance as a predictor of incident asthma-like symptoms in adults. Clin. Exp. 2009, 39, 700–707. [Google Scholar] [CrossRef]
- Brumpton, B.M.; Camargo, C.A., Jr.; Romundstad, P.R.; Langhammer, A.; Chen, Y.; Mai, X.M. Metabolic syndrome and incidence of asthma in adults: The HUNT study. Eur. Respir. J. 2013, 42, 1495–1502. [Google Scholar] [CrossRef]
- Singh, V.P.; Aggarwal, R.; Singh, S.; Banik, A.; Ahmad, T.; Patnaik, B.R.; Nappanveettil, G.; Singh, K.P.; Aggarwal, M.L.; Ghosh, B.; et al. Metabolic Syndrome Is Associated with Increased Oxo-Nitrative Stress and Asthma-Like Changes in Lungs. PLoS ONE 2015, 10, e0129850. [Google Scholar] [CrossRef]
- Urman, R.; Eckel, S.; Deng, H.; Berhane, K.; Avol, E.; Lurmann, F.; McConnell, R.; Gilliland, F. Risk Effects of near-Roadway Pollutants and Asthma Status on Bronchitic Symptoms in Children. Environ. Epidemiol. 2018, 2. [Google Scholar] [CrossRef]
- Spira-Cohen, A.; Chen, L.C.; Kendall, M.; Lall, R.; Thurston, G.D. Personal exposures to traffic-related air pollution and acute respiratory health among Bronx schoolchildren with asthma. Environ. Health Perspect. 2011, 119, 559–565. [Google Scholar] [CrossRef]
- Ai, S.; Qian, Z.M.; Guo, Y.; Yang, Y.; Rolling, C.A.; Liu, E.; Wu, F.; Lin, H. Long-term exposure to ambient fine particles associated with asthma: A cross-sectional study among older adults in six low- and middle-income countries. Environ. Res. 2019, 168, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Rom, W.N.; Reibman, J.; Rogers, L.; Weiden, M.D.; Oppenheimer, B.; Berger, K.; Goldring, R.; Harrison, D.; Prezant, D. Emerging exposures and respiratory health: World Trade Center dust. Proc. Am. Thorac. Soc. 2010, 7, 142–145. [Google Scholar] [CrossRef]
- Berger, K.I.; Kalish, S.; Shao, Y.; Marmor, M.; Kazeros, A.; Oppenheimer, B.W.; Chan, Y.; Reibman, J.; Goldring, R.M. Isolated small airway reactivity during bronchoprovocation as a mechanism for respiratory symptoms in WTC dust-exposed community members. Am. J. Ind. Med. 2016, 59, 767–776. [Google Scholar] [CrossRef]
- Aldrich, T.K.; Weakley, J.; Dhar, S.; Hall, C.B.; Crosse, T.; Banauch, G.I.; Weiden, M.D.; Izbicki, G.; Cohen, H.W.; Gupta, A.; et al. Bronchial Reactivity and Lung Function After World Trade Center Exposure. Chest 2016, 150, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Prezant, D.J.; Weiden, M.; Banauch, G.I.; McGuinness, G.; Rom, W.N.; Aldrich, T.K.; Kelly, K.J. Cough and bronchial responsiveness in firefighters at the World Trade Center site. N. Engl. J. Med. 2002, 347, 806–815. [Google Scholar] [CrossRef]
- Edelman, P.; Osterloh, J.; Pirkle, J.; Caudill, S.P.; Grainger, J.; Jones, R.; Blount, B.; Calafat, A.; Turner, W.; Feldman, D.; et al. Biomonitoring of chemical exposure among New York City firefighters responding to the World Trade Center fire and collapse. Environ. Health Perspect. 2003, 111, 1906–1911. [Google Scholar] [CrossRef] [PubMed]
- Weiden, M.D.; Naveed, B.; Kwon, S.; Cho, S.J.; Comfort, A.L.; Prezant, D.J.; Rom, W.N.; Nolan, A. Cardiovascular biomarkers predict susceptibility to lung injury in World Trade Center dust-exposed firefighters. Eur. Respir. J. 2013, 41, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yip, J.; Zeig-Owens, R.; Weakley, J.; Webber, M.P.; Schwartz, T.M.; Prezant, D.J.; Weiden, M.D.; Hall, C.B. The Effect of World Trade Center Exposure on the Timing of Diagnoses of Obstructive Airway Disease, Chronic Rhinosinusitis, and Gastroesophageal Reflux Disease. Front. Public Health 2017, 5, 2. [Google Scholar] [CrossRef]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; Hankinson, J.L.; Irvin, C.G.; MacIntyre, N.R.; McKay, R.T.; Wanger, J.S.; Anderson, S.D.; et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am. J. Respir. Crit. Care Med. 2000, 161, 309–329. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Ingelsson, E.; Schaefer, E.J.; Contois, J.H.; McNamara, J.R.; Sullivan, L.; Keyes, M.J.; Pencina, M.J.; Schoonmaker, C.; Wilson, P.W.; D’Agostino, R.B.; et al. Clinical utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA 2007, 298, 776–785. [Google Scholar] [CrossRef]
- Lemieux, I.; Lamarche, B.; Couillard, C.; Pascot, A.; Cantin, B.; Bergeron, J.; Dagenais, G.R.; Despres, J.P. Total cholesterol/HDL cholesterol ratio vs. LDL cholesterol/HDL cholesterol ratio as indices of ischemic heart disease risk in men: The Quebec Cardiovascular Study. Arch. Intern. Med. 2001, 161, 2685–2692. [Google Scholar] [CrossRef] [PubMed]
- Keil, U.; Liese, A.D.; Hense, H.W.; Filipiak, B.; Doring, A.; Stieber, J.; Lowel, H. Classical risk factors and their impact on incident non-fatal and fatal myocardial infarction and all-cause mortality in southern Germany—Results from the MONICA Augsburg cohort study 1984–1992. Eur. Heart J. 1998, 19, 1197–1207. [Google Scholar] [CrossRef]
- Weiden, M.D.; Ferrier, N.; Nolan, A.; Rom, W.N.; Comfort, A.; Gustave, J.; Zeig-Owens, R.; Zheng, S.; Goldring, R.M.; Berger, K.I.; et al. Obstructive airways disease with air trapping among firefighters exposed to World Trade Center dust. Chest 2010, 137, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Naveed, B.; Comfort, A.L.; Ferrier, N.; Kasturiarachchi, K.J.; Rom, W.N.; Prezant, D.J.; Weiden, M.D.; Nolan, A. Biomarkers of metabolic syndrome predict accelerated decline of lung function in NYC firefighters that were exposed to WTC particulates. Am. J. Respir. Crit. Care Med. 2011, 183, A4795. [Google Scholar] [CrossRef]
- Kwon, S.; Naveed, B.; Comfort, A.L.; Ferrier, N.; Rom, W.N.; Prezant, D.J.; Nolan, A.; Weiden, M.D. Elevated MMP-3, MMP-12, and TIMP-3 in serum are biomarkers predictive of world trade center-lung injury in New York city firefighters. Am. J. Respir. Crit. Care Med. 2012, 185, A2019. [Google Scholar] [CrossRef]
- Naveed, B.; Kwon, S.; Comfort, A.L.; Ferrier, N.; Rom, W.N.; Prezant, D.J.; Weiden, M.D.; Nolan, A. Cardiovascular serum biomarkers predict world trade center lung injury in NYC firefighters. Am. J. Respir. Crit. Care Med. 2012, 185, A4894. [Google Scholar]
- Naveed, B.; Weiden, M.D.; Kwon, S.; Gracely, E.J.; Comfort, A.L.; Ferrier, N.; Kasturiarachchi, K.J.; Cohen, H.W.; Aldrich, T.K.; Rom, W.N.; et al. Metabolic syndrome biomarkers predict lung function impairment: A nested case-control study. Am. J. Respir. Crit. Care Med. 2012, 185, 392–399. [Google Scholar] [CrossRef]
- Landgren, O.; Zeig-Owens, R.; Giricz, O.; Goldfarb, D.; Murata, K.; Thoren, K.; Ramanathan, L.; Hultcrantz, M.; Dogan, A.; Nwankwo, G.; et al. Multiple Myeloma and Its Precursor Disease Among Firefighters Exposed to the World Trade Center Disaster. JAMA Oncol. 2018, 4, 821–827. [Google Scholar] [CrossRef]
- Haider, S.H.; Kwon, S.; Lam, R.; Lee, A.K.; Caraher, E.J.; Crowley, G.; Zhang, L.; Schwartz, T.M.; Zeig-Owens, R.; Liu, M.; et al. Predictive Biomarkers of Gastroesophageal Reflux Disease and Barrett’s Esophagus in World Trade Center Exposed Firefighters: A 15 Year Longitudinal Study. Sci. Rep. 2018, 8, 3106. [Google Scholar] [CrossRef]
- Hena, K.M.; Yip, J.; Jaber, N.; Goldfarb, D.; Fullam, K.; Cleven, K.; Moir, W.; Zeig-Owens, R.; Webber, M.P.; Spevack, D.M.; et al. Clinical Course of Sarcoidosis in World Trade Center-Exposed Firefighters. Chest 2018, 153, 114–123. [Google Scholar] [CrossRef]
- Cho, S.J.; Echevarria, G.C.; Kwon, S.; Naveed, B.; Schenck, E.J.; Tsukiji, J.; Rom, W.N.; Prezant, D.J.; Nolan, A.; Weiden, M.D. One airway: Biomarkers of protection from upper and lower airway injury after World Trade Center exposure. Respir. Med. 2014, 108, 162–170. [Google Scholar] [CrossRef]
- Nolan, A.; Naveed, B.; Comfort, A.L.; Ferrier, N.; Hall, C.B.; Kwon, S.; Kasturiarachchi, K.J.; Cohen, H.W.; Zeig-Owens, R.; Glaser, M.S.; et al. Inflammatory biomarkers predict airflow obstruction after exposure to World Trade Center dust. Chest 2012, 142, 412–418. [Google Scholar] [CrossRef]
- Lippman, M.; Cohen, M.D.; Chen, L.C. Health effects of World Trade Center (WTC) Dust: An unprecedented disaster with inadequate risk management. Critical Reviews in Toxicology. 2015, 45, 492–530. [Google Scholar] [CrossRef]
- Crowley, G.; Kwon, S.; Haider, S.H.; Caraher, E.J.; Lam, R.; St-Jules, D.E.; Liu, M.; Prezant, D.J.; Nolan, A. Metabolomics of World Trade Center-Lung Injury: A machine learning approach. BMJ Open Respir. Res. 2018, 5, e000274. [Google Scholar] [CrossRef]
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect 2002, 110, 703–714. [Google Scholar] [CrossRef]
- Levin, S.; Herbert, R.; Skloot, G.; Szeinuk, J.; Teirstein, A.; Fischler, D.; Milek, D.; Piligian, G.; Wilk-Rivard, E.; Moline, J. Health effects of World Trade Center site workers. Am. J. Ind. Med. 2002, 42, 545–547. [Google Scholar] [CrossRef]
- Banauch, G.I.; Dhala, A.; Alleyne, D.; Alva, R.; Santhyadka, G.; Krasko, A.; Weiden, M.; Kelly, K.J.; Prezant, D.J. Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Crit. Care Med. 2005, 33, S102–S106. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Lioy, P.J.; Thurston, G.; Berkowitz, G.; Chen, L.C.; Chillrud, S.N.; Gavett, S.H.; Georgopoulos, P.G.; Geyh, A.S.; Levin, S.; et al. Health and environmental consequences of the world trade center disaster. Environ. Health Perspect. 2004, 112, 731–739. [Google Scholar] [CrossRef]
- Farfel, M.; DiGrande, L.; Brackbill, R.; Prann, A.; Cone, J.; Friedman, S.; Walker, D.J.; Pezeshki, G.; Thomas, P.; Galea, S.; et al. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. J. Urban Health 2008, 85, 880–909. [Google Scholar] [CrossRef]
- Aldrich, T.K.; Vossbrinck, M.; Zeig-Owens, R.; Hall, C.B.; Schwartz, T.M.; Moir, W.; Webber, M.P.; Cohen, H.W.; Nolan, A.; Weiden, M.D.; et al. Lung Function Trajectories in World Trade Center-Exposed New York City Firefighters Over 13 Years: The Roles of Smoking and Smoking Cessation. Chest 2016, 149, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Niles, J.K.; Webber, M.P.; Cohen, H.W.; Hall, C.B.; Zeig-Owens, R.; Ye, F.; Glaser, M.S.; Weakley, J.; Weiden, M.D.; Aldrich, T.K.; et al. The respiratory pyramid: From symptoms to disease in World Trade Center exposed firefighters. Am. J. Ind. Med. 2013, 56, 870–880. [Google Scholar] [CrossRef] [PubMed]
- Zeig-Owens, R.; Singh, A.; Aldrich, T.K.; Hall, C.B.; Schwartz, T.; Webber, M.P.; Cohen, H.W.; Kelly, K.J.; Nolan, A.; Prezant, D.J.; et al. Blood Leukocyte Concentrations, FEV1 Decline, and Airflow Limitation. A 15-Year Longitudinal Study of World Trade Center-exposed Firefighters. Ann. Am. Thorac. Soc. 2018, 15, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, M.; Tran, T.N.; van den Berge, M.; Brusselle, G.G.; Gopalan, G.; Jones, R.C.M.; Kocks, J.W.H.; Menzies-Gow, A.; Nuevo, J.; Pavord, I.D.; et al. Association between blood eosinophil count and risk of readmission for patients with asthma: Historical cohort study. PLoS ONE 2018, 13, e0201143. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Rigazio, A.; Campbell, J.D.; Bleecker, E.R.; Corrigan, C.J.; Thomas, M.; Wenzel, S.E.; Wilson, A.M.; Small, M.B.; Gopalan, G.; et al. Blood eosinophil count and prospective annual asthma disease burden: A UK cohort study. Lancet Respir. Med. 2015, 3, 849–858. [Google Scholar] [CrossRef]
- Bolton, C.E.; Evans, M.; Ionescu, A.A.; Edwards, S.M.; Morris, R.H.; Dunseath, G.; Luzio, S.D.; Owens, D.R.; Shale, D.J. Insulin resistance and inflammation—A further systemic complication of COPD. J. Chron. Obstruct. Pulm. Dis. 2007, 4, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Caraher, E.J.; Kwon, S.; Haider, S.H.; Crowley, G.; Lee, A.; Ebrahim, M.; Zhang, L.; Chen, L.C.; Gordon, T.; Liu, M.; et al. Receptor for advanced glycation end-products and World Trade Center particulate induced lung function loss: A case-cohort study and murine model of acute particulate exposure. PLoS ONE 2017, 12, e0184331. [Google Scholar] [CrossRef]
- Scott, H.A.; Gibson, P.G.; Garg, M.L.; Wood, L.G. Airway inflammation is augmented by obesity and fatty acids in asthma. Eur. Respir. J. 2011, 38, 594–602. [Google Scholar] [CrossRef]
- Wadden, D.; Allwood Newhook, L.A.; Twells, L.; Farrell, J.; Gao, Z.W. Sex-Specific Association between Childhood BMI Trajectories and Asthma Phenotypes. Int. J. Pediat. 2018, 2018, 9057435. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measure | MCT+ N = 355 | BD+ N = 236 | Non-AHR N = 6947 | WTC-AHR N = 539 | p | |
|---|---|---|---|---|---|---|
| Age on 9/11 | 40.3 (6.3) | 40.9 (6.8) | 39.5 (7.5) | 40.5 (6.5) | 0.004 | |
| Years of service * | 19.3 (7.3) | 20.1 (7.2) | 22.8 (6.5) | 19.7 (7.3) | <0.001 | |
| Ever smokers | 122 (34%) | 89 (38%) | 2531 (36%) | 191 (35%) | 0.643 | |
| Race | Caucasian | 342 (96%) | 220 (93%) | 6529 (94%) | 512 (95%) | 0.560 |
| African American | 3 (1%) | 6 (3%) | 183 (3%) | 9 (2%) | ||
| Hispanic | 9 (3%) | 10 (4%) | 215 (3%) | 17 (3%) | ||
| Asian/other | 1 (.3%) | 0 (0%) | 20 (0.3%) | 1 (0.2%) | ||
| Exposure group | Morning of 9/11 | 79 (22%) | 59 (25%) | 1124 (16%) | 123 (23%) | <0.001 |
| Afternoon of 9/11 | 211 (59%) | 134 (57%) | 3749 (54%) | 317 (59%) | ||
| On or after 9/12 | 65 (18%) | 43 (18%) | 2074 (30%) | 99 (18%) | ||
| Pre-9/11 | FEV1% pred. | 101.5 (11.6) | 101.5 (13.5) | 106.3 (13.0) | 101.7 (12.4) | <0.001 |
| FVC% pred. | 97.7 (10.9) | 98.4 (12.7) | 99.6 (12.1) | 98.2 (11.7) | 0.017 | |
| Ratio | 82.9 (5.7) | 82.4 (5.4) | 85.3 (4.9) | 82.7 (5.6) | <0.001 | |
| WTC-HP entry | FEV% pred. | 91.8 (13.4) | 90.7 (14.8) | 98.1 (13.1) | 91.6 (13.9) | <0.001 |
| FVC% pred. | 89.6 (12.0) | 89.3 (21.1) | 92.4 (11.8) | 89.6 (12.2) | <0.001 | |
| Ratio | 82.0 (6.0) | 81.2 (6.6) | 84.6 (4.9) | 81.7 (6.3) | <0.001 | |
| Measure | MCT+ N = 355 | BD+ N = 236 | Non-AHR N = 6947 | WTC-AHR N = 539 | p |
|---|---|---|---|---|---|
| Systolic BP, mmHg | 118.0 (12.5) | 118.3 (12.6) | 117.1 (12.5) | 118.0 (12.7) | 0.092 |
| Diastolic BP, mmHg | 73.4 (8.0) | 74.3 (8.3) | 73.4 (8.4) | 73.6 (8.2) | 0.598 |
| BMI at WTC-HP entry, kg/m2 | 29.2 (3.2) | 28.9 (3.0) | 28.6 (3.3) | 29.1 (3.2) | 0.001 |
| White blood cells × 109 cells/L * | 6.5 (1.9) | 6.5 (1.8) | 6.3 (1.6) | 6.5 (1.9) | 0.021 |
| Neutrophils (ANC) | 3809.8 (1654.5) | 3697.7 (1400.1) | 3664.6 (1290.1) | 3758.1 (1524.8) | 0.113 |
| Lymphocytes (ALC) | 1818.9 (534.4) | 1861.8 (590.2) | 1830.9 (540.3) | 1843.4 (561.2) | 0.608 |
| Eosinophils (AEC) | 227.8 (149.9) | 227.2 (160.3) | 187.1 (130.9) | 229.3 (156.6) | <0.001 |
| Monocytes (AMC) | 579.4 (194.3) | 605.7 (216.2) | 581.3 (193.2) | 591.1 (204.8) | 0.263 |
| Glucose | 92.9 (18.8) | 91.7 (10.4) | 91.6 (13.9) | 92.5 (16.4) | 0.177 |
| Triglyceride | 195.7 (139.1) | 190.7 (126.0) | 185.1 (136.6) | 197.4 (137.9) | 0.046 |
| HDL | 48.0 (12.6) | 47.1 (12.1) | 48.1 (11.7) | 47.6 (12.4) | 0.351 |
| LDL | 133.1 (34.5) | 128.3 (32.4) | 128.3 (33.5) | 131.6 (33.7) | 0.028 |
| Cholesterol | 217.4 (40.1) | 210.2 (36.0) | 210.8 (38.7) | 216.3 (38.5) | 0.009 |
| Cholesterol/HDL ratio | 4.8 (1.5) | 4.7 (1.3) | 4.6 (1.4) | 4.8 (1.4) | 0.007 |
| MetSyn definition | 82 (23%) | 54 (23%) | 1329 (19%) | 123 (23%) | <0.001 |
| SBP ≥ 130 and/or DBP ≥ 85 mmHg | 78 (22%) | 56 (24%) | 1384 (20%) | 119 (22%) | 0.229 |
| HDL < 40 mg/dL | 94 (27%) | 72 (31%) | 1667 (24%) | 151(28%) | 0.036 |
| Triglycerides ≥ 150 mg/dL | 194 (55%) | 123 (52%) | 3428 (49%) | 294 (55%) | 0.020 |
| Glucose ≥ 100 mg/dL | 72 (20%) | 45 (19%) | 1269 (18%) | 106 (20%) | 0.419 |
| BMI ≥ 30 kg/m2 | 130 (30%) | 78 (33%) | 2040 (29%) | 193 (36%) | 0.002 |
| Measure | Hazards (95% CI) | |
|---|---|---|
| Cholesterol/HDL ratio ≥ 3.5 | 1.332 (1.057–1.679) | |
| BMI ≥ 30 kg/m2 | 1.329 (1.114–1.585) | |
| Glucose ≥ 100 mg/dL | 1.062 (0.857–1.315) | |
| Lipids mg/dL | HDL < 40 | 1.237 (1.025–1.492) |
| Triglycerides ≥ 150 | 1.204 (1.016–1.427) | |
| Blood pressure mmHg | Systolic ≥ 130 | 1.079 (0.872–1.335) |
| Diastolic ≥ 85 | 0.970 (0.718–1.309) | |
| Number of MetSyn risk factors | 1 | 1.441 (1.124–1.847) |
| 2 | 1.690 (1.310–2.151) | |
| 3+ | 1.654 (1.268–2.158) | |
| Exposure intensity | Morning of 9/11 | 2.240 (1.719–2.919) |
| Afternoon of 9/11 | 1.759 (1.403–2.205) | |
| After 9/12 | Reference | |
| Ever smoker | 1.759 (1.403–2.205) | |
| Age (per year) | 1..017 (1.005–1.029) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, S.; Crowley, G.; Mikhail, M.; Lam, R.; Clementi, E.; Zeig-Owens, R.; Schwartz, T.M.; Liu, M.; Prezant, D.J.; Nolan, A. Metabolic Syndrome Biomarkers of World Trade Center Airway Hyperreactivity: A 16-Year Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091486
Kwon S, Crowley G, Mikhail M, Lam R, Clementi E, Zeig-Owens R, Schwartz TM, Liu M, Prezant DJ, Nolan A. Metabolic Syndrome Biomarkers of World Trade Center Airway Hyperreactivity: A 16-Year Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(9):1486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091486
Chicago/Turabian StyleKwon, Sophia, George Crowley, Mena Mikhail, Rachel Lam, Emily Clementi, Rachel Zeig-Owens, Theresa M. Schwartz, Mengling Liu, David J. Prezant, and Anna Nolan. 2019. "Metabolic Syndrome Biomarkers of World Trade Center Airway Hyperreactivity: A 16-Year Prospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 9: 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091486