3.2. Benchmark Test
The test results for the direct effect of the HSR connection are reported in
Table 3. The fixed effects (FE) were selected by using the Hausman test, and a collinearity test on the variables was performed, the result of which shows that the mean variance inflation factor (VIF) was 4.16, less than 10, indicating that the collinearity of the variables selected in this paper was not significant. Column FE (1) shows the regression results without the control variables. Columns FE (2)–FE (5) show the regression results with four kinds of control variables, namely, the comprehensive development level, the public finance level of the local governments, population agglomeration, and the accessibility of the cities.
The regression coefficient of the direct effect of the HSR connection and the positive effect of the length of time for HSR development on the equalization level of medical and health services are gradually strengthened, indicating that although the HSR connection has a negative impact, it will improve the equalization level of medical and health services and reduce the pressure of cross-regional medical services in the long run.
In the era of HSR, economic growth is conducive to improving the capacity of medical and health services. Rural residents have a more powerful motive to pursue urban medical and health services due to the HSR and the unbalanced allocation of medical resources between urban and rural areas, which increases the demand for urban medical and health services and reduces their overall level of equalization.
Highway construction, which is viewed in public services as an improvement in the infrastructure, reflects the comprehensive financial capacity of local governments, which has a positive relationship with the supply of medical and health services. The passenger flow brought by the operation of civil aviation lines has significantly reduced the equalization level of medical and health services, and the absolute value of the coefficient for the direct effect of the HSR increased significantly after controlling for highway mileage and civil aviation. This result shows that the improvement in long-distance and short-distance passenger transportation modes, represented by HSR and civil aviation respectively, can fully exert the influence of transportation infrastructure on regional public services. Therefore, controlling for the impact of other modes of transportation in the analysis of the HSR direct effect is correct and necessary.
To investigate which city characteristics can optimize the equalization level of medical and health services considering the development of the HSR, this paper further adopts the cross-term regression method, which multiplies the virtual variable HSR and the control variables that have positive effects on the equalization level of medical and health services, as shown in
Table 3. The results of the optimization mechanism test are reported in
Table 4, which reports regression results only for the cross-terms that are statistically significant.
The results show that the government and social capital can improve the supply side by investing more in the medical and health care field to alleviate the pressure brought about by an increase in the population.
HSR development has removed regional barriers and increased the level of urbanization and the demand for medical and health services through population agglomeration; cost sharing may promote the supply of medical and health services. The urban variable did not significantly promote the equalization level of medical and health services in
Table 3, but the regression coefficient of HSR × Urban is significant. This finding shows that the positive effect of urbanization on the equalization level of medical and health services can be achieved through development of the HSR.
In addition, when the financial autonomy of the local government is high, more information can be used to better meet the medical needs of residents within the fiscal jurisdiction. In
Table 4, the Stru begins to significantly improve the equalization level of medical and health services, which shows that it is necessary to give full play to the financial capacity of local governments in the development of HSR.
We then decomposed the dynamic effect of HSR development time by year to assess whether the HSR effect turns from negative to positive after a certain number of years.
According to the regression results shown in
Table 5, the pressure of medical and health services caused by the HSR is instantaneous and is strongest in the year after connection. By the fourth year after the HSR connection onward, HSR development has an insignificant but positive impact on the equalization of medical and health services in cities. The above results show that HSR connection elicits a certain degree of medical crowding over the short term, resulting in a reduction in the per capita public resources and a relatively low supply level of medical and health services. However, the congestion related to medical and health services gradually decreases over time. Overall, the regression results for the dynamic effects show that cities should focus on the rapid increase in the demand for medical and other public services from the year of the HSR connection to the second year after the HSR connection and should pay more attention to increasing the supply of medical and health services over the long term.
3.3. Heterogeneity Test
The above empirical analysis shows that HSR development has a considerable impact on the equalization of medical and health services between cities. Next, we explore the performance of the HSR effect considering heterogeneous city characteristics. First, we conduct a grouping test based on the heterogeneity of city scale and then perform a DDD heterogeneity test for cities with different political attributes and financial capacities, as well as their geographical position in different economic regions.
City scale represents the potential comprehensive development ability of the city. Some studies have reported that there is a statistically positive correlation between city scale and the capacity of the floating population, the level of public service, the floating population’s recognition of the region, and the willingness to settle or leave. All of these factors were shown to have an important impact on the change in city scale and its rank order [
52]. It is recognized that an HSR is essential for improvement in the public services offered in a city, which can enhance the geographical identity of the floating population. In this study, city scale is measured by the permanent population size of urban areas. According to the official classification criteria (In 2014, the State Council of China issued the “Notice on Adjusting the Standards for Dividing Urban Sizes”, which took the permanent population of urban areas as the statistical caliber and divided the cities into five categories. Cities with an urban resident population of 200,000 to 500,000 are considered to be small cities, those with a population of 500,000 to 1,000,000 are medium-sized cities, those with a population of 1,000,000 to 5,000,000 are large cities, those with a population of 5,000,000 to 10,000,000 are megacities, and those with a population over 10,000,000 are super-large cities (the high numbers are included, while the low numbers are excluded).) used by the State Council of China, which divide cities into five categories, this paper divides the sample cities into four categories by combining cities with a population of 200,000–500,000 and cities with a population of 500,000–1,000,000. Then, a grouping test is conducted by separating regression per class of cities to analyze the direct effect of the HSR connection on the equalization level of medical and health services. The regression results are presented in
Table 6.
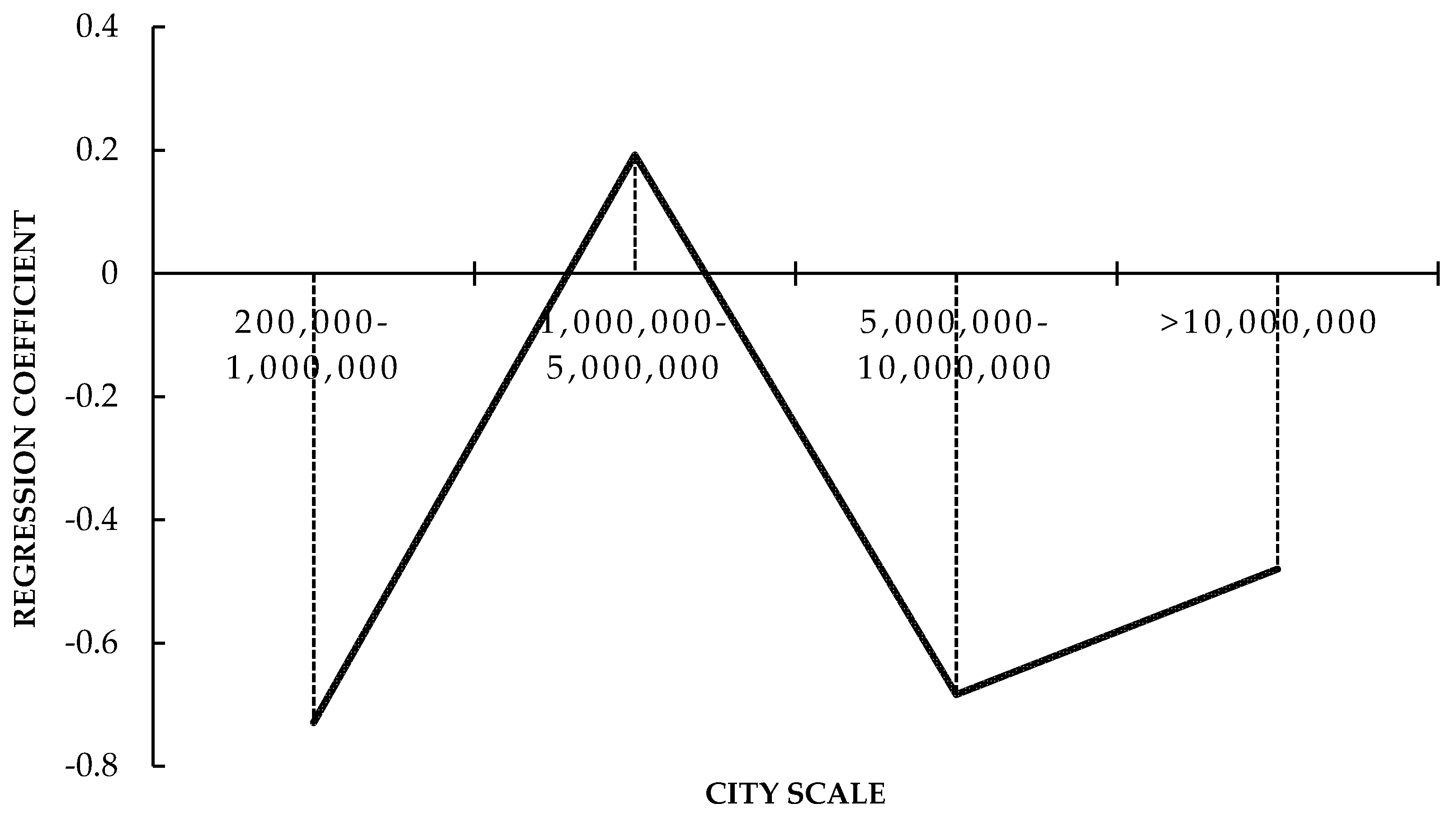
The regression results show that there are significant differences in the direct effect of HSR in cities with different population scales. The regression coefficients of the four categories of cities show an "N"-shaped change with the evolution of the city scale (
Figure 3).
Cities with the smallest population scale are most sensitive to the effects of the HSR connection. This paper considers that these cities have more space and bearing capacity to carry inflowing populations that continue to migrate from rural areas and lower-level cities, so the increasing population density and degree of agglomeration lead to a decline in the equalization of medical and health services.
When the population scale reaches 1,000,000 to 5,000,000, due to the considerable pressure of increasing population density, cities begin to build new subcenter cities around the HSR station, which effectively diffuses the population, pushing them to the surrounding areas, thus reducing the pressure of the medical and health services offered by the central city. When cities are larger, the coefficient of the direct effect of HSR is significantly negative. Most provincial capital cities belong to this category, their unique political attributes attract the population in a sustained manner. Therefore, the population inflow caused by the HSR connection significantly reduces the equalization level of medical and health services. However, in cities with a population of more than 10,000,000, due to the highly mature operating system and city layout, medical and health services are relatively adequate, and the crowding effect caused by the inflow of migrants is eased. HSR development disperses the population and relieves population density, which subsequently alleviates the pressure of public goods in cities, so HSR development brings the most improvement effects.
Next, we used the DDD model to test the heterogeneity of cities in terms of their political attributes, financial capabilities, and the economic regions in which they are located. The regression results of the effect of the HSR connection are shown in
Table 7, the cross-term shown in the table means the
=1 in equation (3), and
Table 8 shows the effect of the HSR development based on classification samples. To further analyze the direction of population flow, in
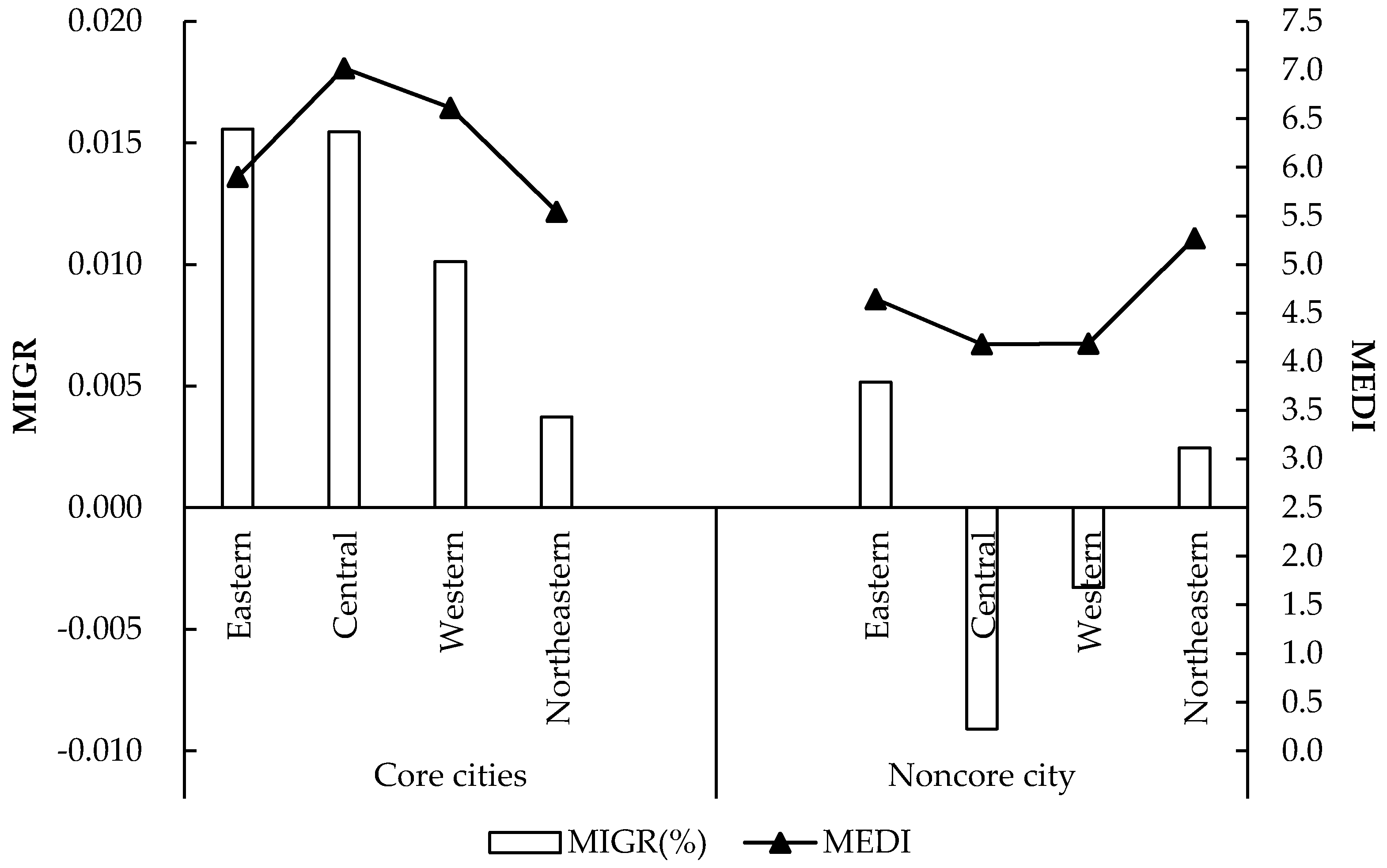
Figure 4 we show the yearly migration rate of the population (Migr) in cities with different political attributes in four different regions.
For the heterogeneity test, we used the following definitions for “core city” and “noncore city”: the provincial capital cities and municipalities directly under the central government are considered to be core cities, and all other cities are classified as noncore cities. For noncore cities, an HSR connection has a strong negative effect, while the equalization level of medical and health services in core cities tends to significantly improve after the HSR connection. This result indicates that the inherent foundation of medical and health services offered in core cities and the relatively mature construction of subcenter cities along HSR lines substantially reduce the pressure that occurs due to population inflow. This process takes precedence over many noncore cities, so the equalization of medical resources in noncore cities depends more on the development of HSR.
The level of economic development in the Eastern region is relatively high compared to that in the other three regions and has been accompanied by a large population inflow. In this region, the increasing demand of medical resources has outpaced the increasing supply, the HSR connection effect is significant. In the Central region, we find that the equalization level of medical and health services is the highest among the four regions. The core cities are experiencing population inflow, and the noncore cities are experiencing net outflow. Therefore, although the equalization level of medical and health services after the HSR connection has declined, it is not significant. The HSR network in the Eastern and Central regions has developed rapidly, and the regional development has transitioned to the stage of city groups. Therefore, the allocation of medical and health resources is more dependent on the development of the HSR.
Most of the core cities in the Western region have a population scale ranging from 200,000 to 5,000,000 with a positive population inflow rate, and the noncore cities have a population scale smaller than 1,000,000 with a net outflow rate. These noncore cities with HSR connections are all in the early stage of HSR development. They have been experiencing the stage of industrial agglomeration and undertaking the transfer of labor-intensive industries from the Central and Eastern regions caused by HSR development, causing a large number of rural people to migrate to urban areas. Therefore, the increase in the supply of medical and health public services cannot meet the rapid increase in demand, so the HSR connection is significantly negative. The Northeastern region is in a critical period of industrial transformation, moving from traditional secondary industries to advanced technical industries. The net population inflow indicates that human capital is being used to enhance advanced industries and sustainable development, so the population scale is growing even further, leading to the significantly continuous negative effect of HSR development. However, the Northeastern region is experiencing a high degree of population agglomeration and urbanization because it is becoming industrialized, and they are developing a more mature and equal system of medical and health services, which ranks second among the four regions. Therefore, although the growth of demand surpasses the increasing supply, the negative effect from the HSR connection is not significant.
In this paper, per capita medical and health expenditures are growing at a rate that is faster than or equal to the growth rate of per capita GDP in cities with considerable fiscal capacity, and vice versa. The medical and health services of cities with a stronger capacity are more sensitive to the effects of the HSR connection. This result shows that although medical expenditures are growing faster than economic growth, the more abundant and high-quality the medical resources are, the easier it is to attract people to enjoy medical and health services across regions. However, the reduction in equalization caused by the HSR connection in cities with weaker financial capacity is more obvious. Cities with stronger financial capacity depend more on HSR development to alleviate the crowding effect, and cities with weaker financial capacity should focus on improving their financial capacity first.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}