Inequality and Influencing Factors of Spatial Accessibility of Medical Facilities in Rural Areas of China: A Case Study of Henan Province

Abstract
:1. Introduction
2. Materials and Methods
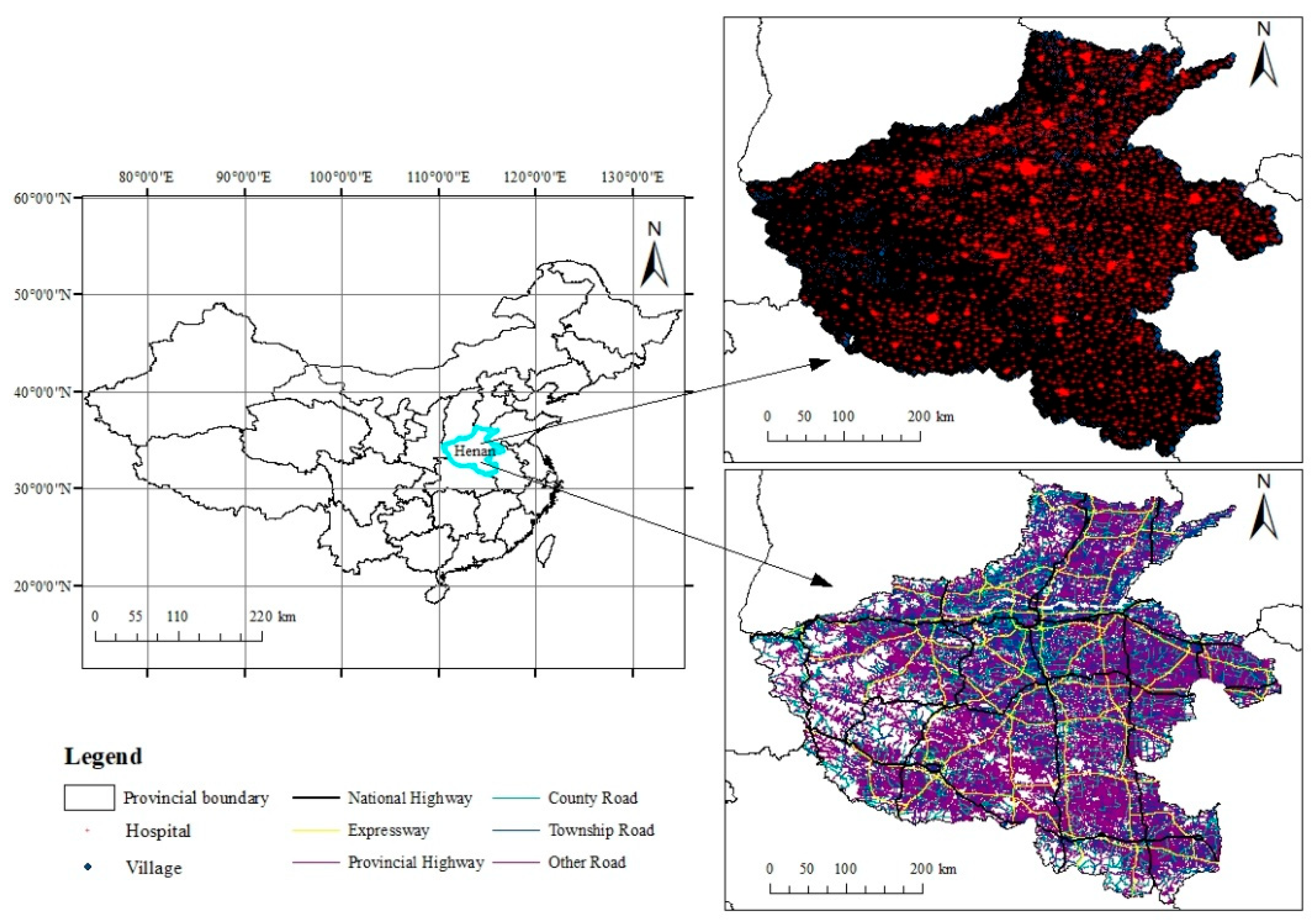
2.1. Study Area and Data Sources
2.2. Methods
2.2.1. Spatial Accessibility Calculation
2.2.2. Coefficient of Variation
2.2.3. Spatial Autocorrelation
2.2.4. Geographically Weighted Regression
3. Results
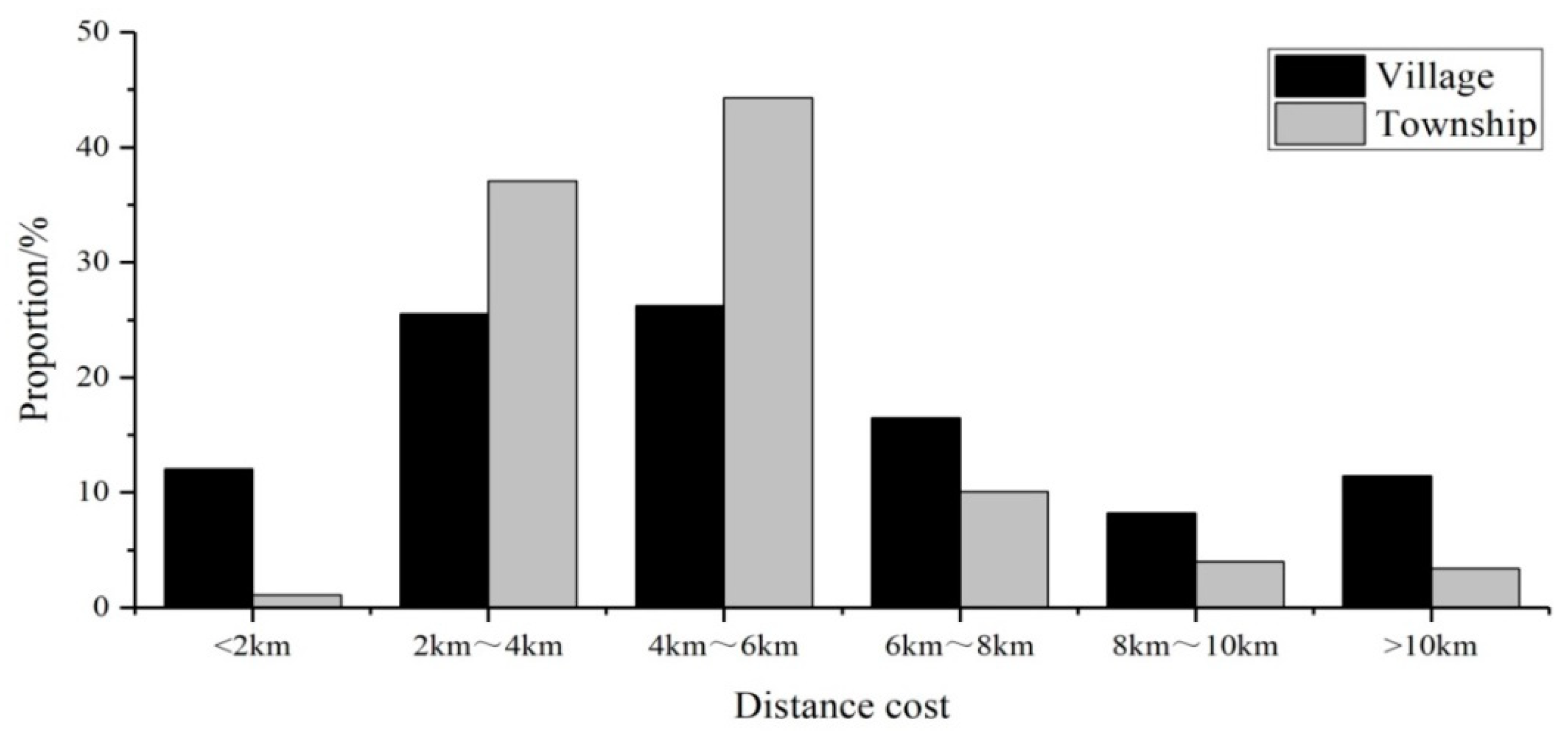
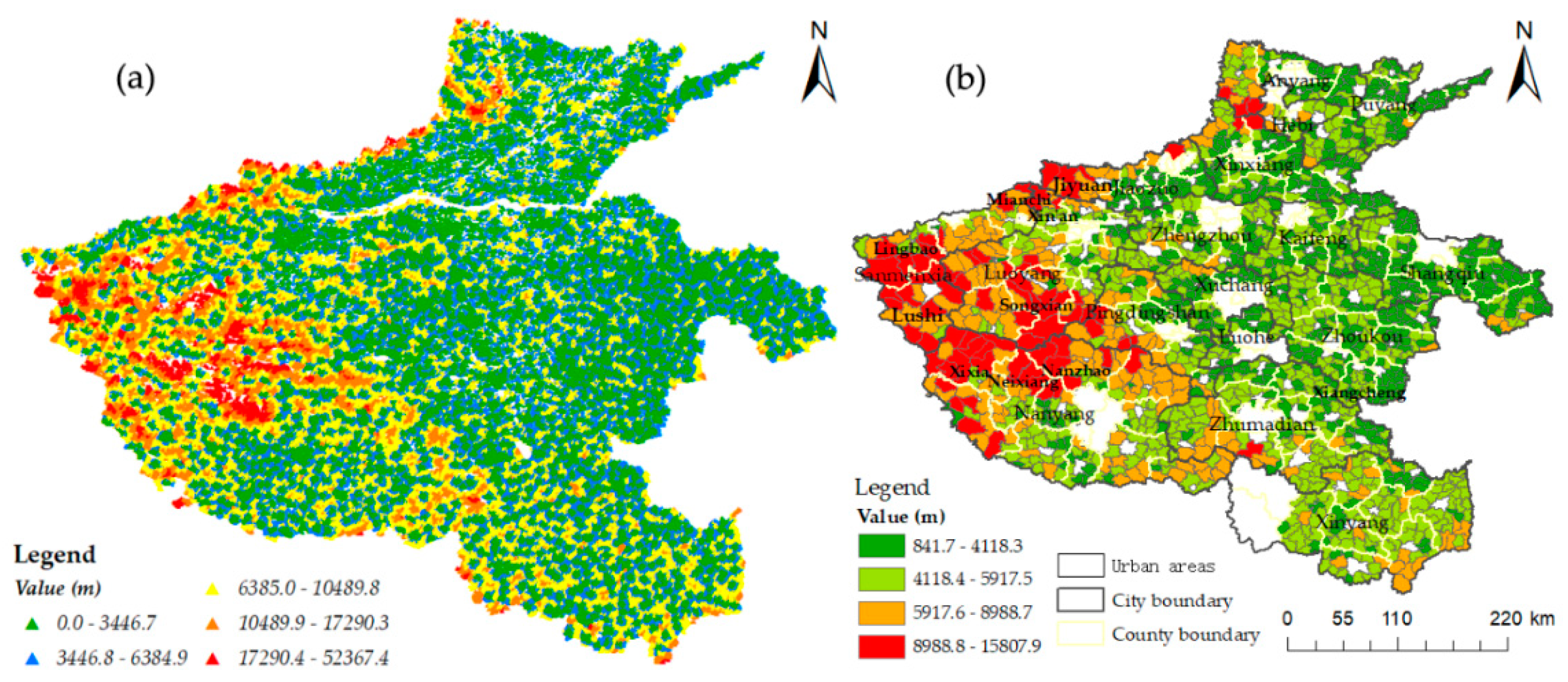
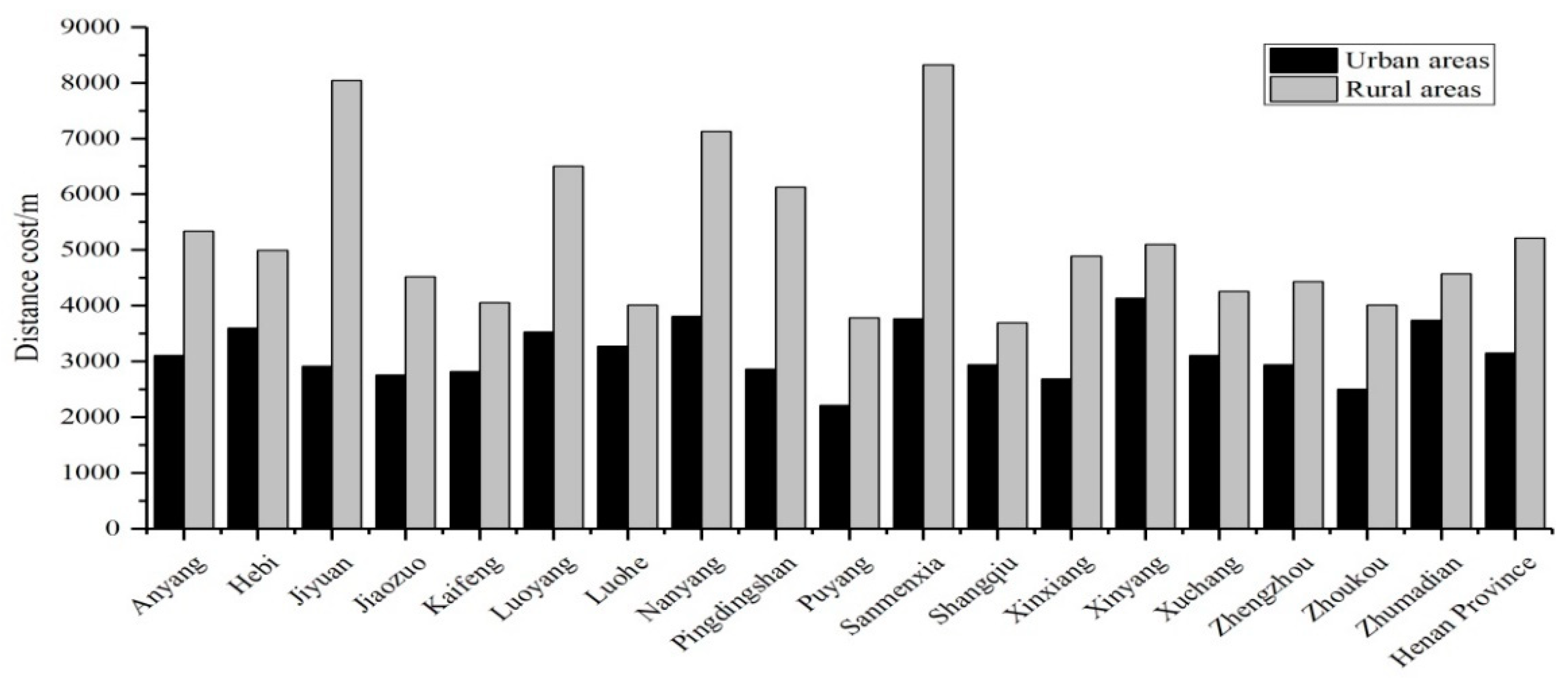
3.1. Analysis of Spatial Accessibility in Rural Areas
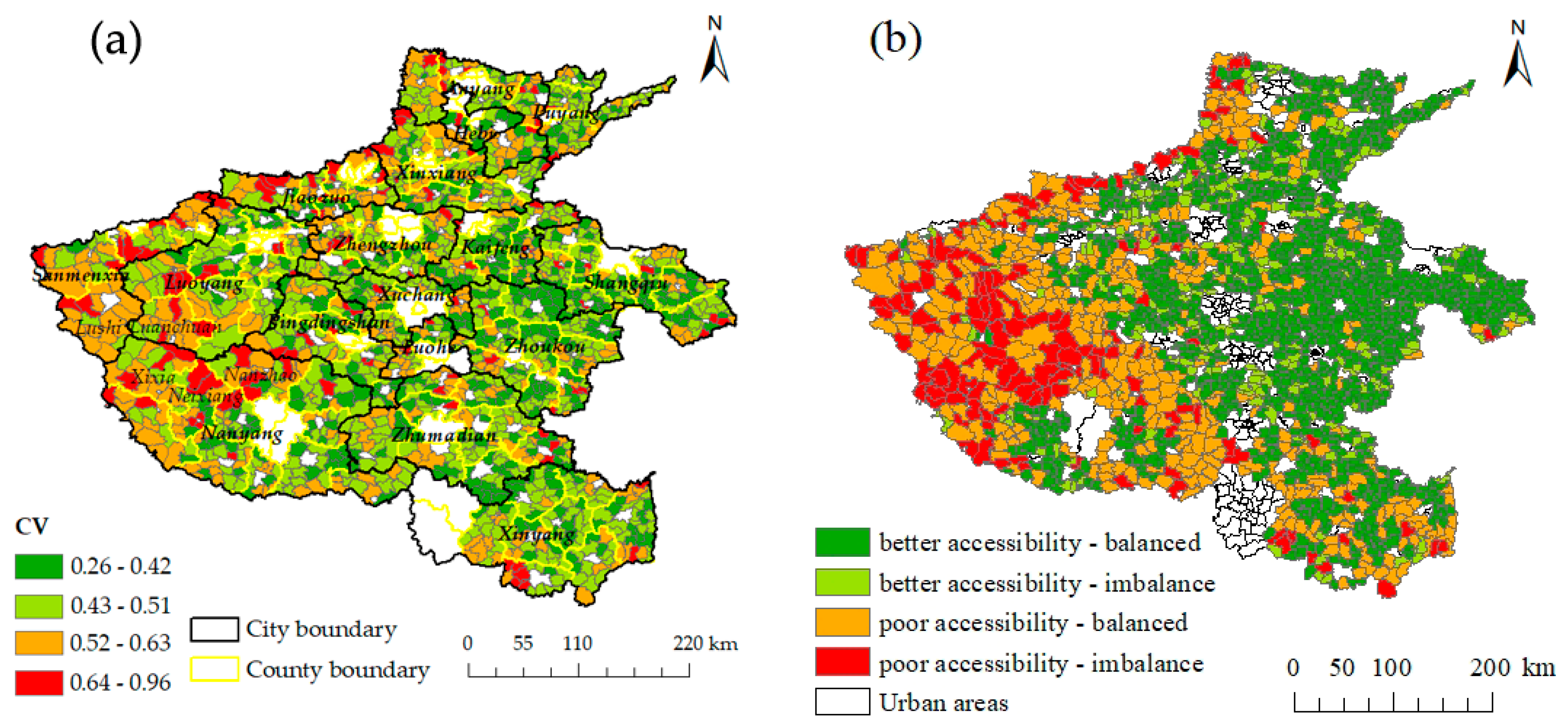
3.2. Spatial Equilibrium of Accessibility
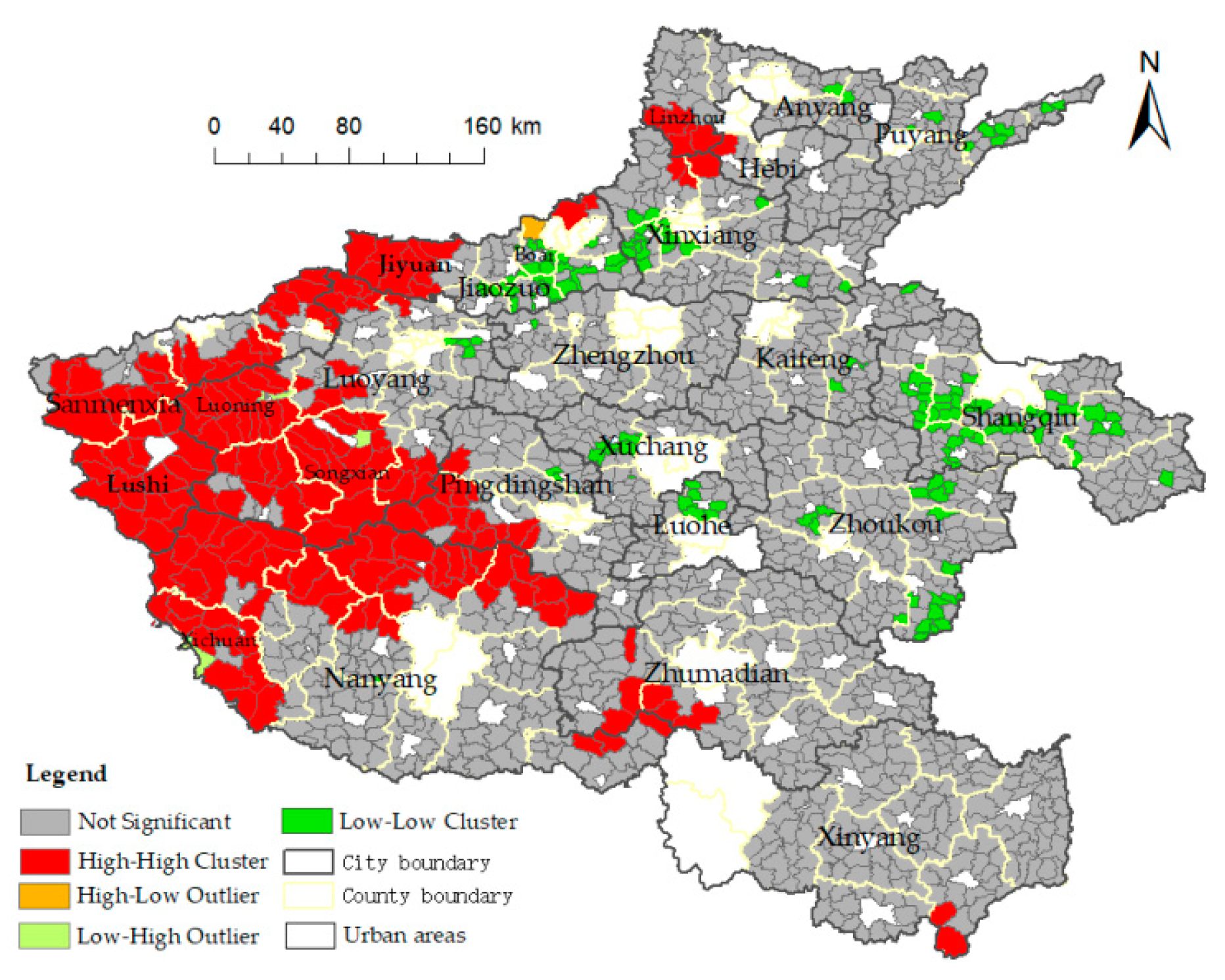
3.3. Spatial Autocorrelation Analysis
3.4. Spatial Heterogeneity Analysis Based on the GWR Model
3.4.1. OLS Regression Analysis
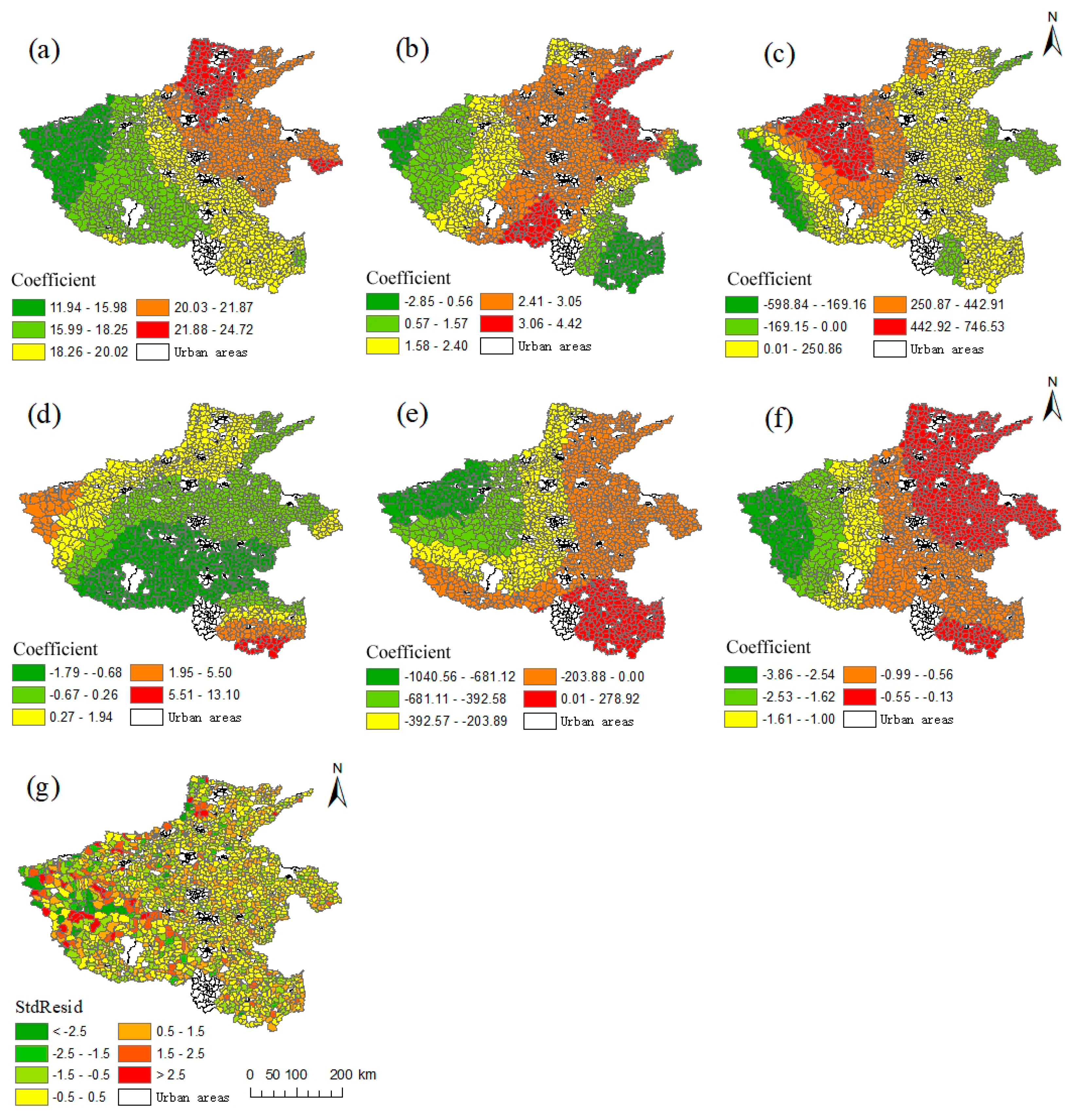
3.4.2. Spatial Heterogeneity of the Influencing Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Luo, J.; Tian, L.; Luo, L.; Yi, H.; Wang, F. Two-step optimization for spatial accessibility improvement: A case study of health care planning in rural China. BioMed Res. Int. 2017, 2017, 2094654. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.P.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Hu, P.; Liu, Z.; Lan, J. Equity and Efficiency in Spatial Distribution of Basic Public Health Facilities: A Case Study from Nanjing Metropolitan Area. Urban Policy Res. 2018. [Google Scholar] [CrossRef]
- Song, Y.Z.; Tan, Y.; Song, Y.M.; Wu, P.; Cheng, J.C.P.; Kim, M.J.; Wang, X. Spatial and temporal variations of spatial population accessibility to public hospitals: A case study of rural-urban comparison. Gisci. Remote Sens. 2018. [Google Scholar] [CrossRef]
- Tao, Z.L.; Cheng, Y.; Zheng, Q.J.; Li, G. Measuring spatial accessibility to healthcare services with constraint of administrative boundary: A case study of Yanqing District, Beijing, China. Int. J. Equity Health 2018, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Yin, P. Urban–rural inequalities in spatial accessibility to prenatal care: A GIS analysis of Georgia, USA, 2000–2010. GeoJournal 2018. [Google Scholar] [CrossRef]
- Peng, J.; Luo, J.; Xiong, J.; Zhen, W.S. Review of domestic and foreign research on the basic public service accessibility. Areal Res. Dev. 2012, 31, 20–25. [Google Scholar]
- Lu, B.; Zhang, C.; Chen, T.P. Study on Changes in Job Accessibility for the Urban Low-Income: A Case Study of Beijing. City Plan. Rev. 2013, 37, 56–63. [Google Scholar]
- Joseph, A.E.; Bantock, P.R. Measuring potential physical accessibility to general practitioners in rural areas: Amethod and case study. Soc. Sci. Med. 1982, 16, 85–90. [Google Scholar] [CrossRef]
- Song, Z.N.; Chen, W.; Che, Q.J. Measurement of Spatial Accessibility to Health Care Facilities and Defining Health Professional Shortage Areas Based on Improved Potential Model—A Case Study of Rudong County in Jiangsu Province. Sci. Geogr. Sin. 2010, 30, 213–219. [Google Scholar]
- Luo, W.; Wang, F.H. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef]
- Tao, Z.L.; Cheng, Y. Research progress of the two-step floating catchment area method and extensions. Prog. Geogr. 2016, 35, 589–599. [Google Scholar]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.L.; Cheng, Y.; Dai, T.Q. Measuring spatial accessibility to residential care facilities in Beijing. Prog. Geogr. 2014, 33, 616–624. [Google Scholar]
- Dai, D.J. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Dai, D.J.; Wang, F.H. Geographic disparities in accessibility to food stores in southwest Mississippi. Environ. Plan. B Plan. Des. 2011, 38, 659–677. [Google Scholar] [CrossRef]
- Luo, W.; Whippo, T. Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health Place 2012, 18, 789–795. [Google Scholar] [CrossRef] [PubMed]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Appl. Geogr. 2014, 54, 182–188. [Google Scholar] [CrossRef]
- Jamtsho, S.; Corner, R.; Dewan, A. Spatio-temporal analysis of spatial accessibility to primary health care in Bhutan. ISPRS Int. J. Geoinf. 2015, 4, 1584–1604. [Google Scholar] [CrossRef]
- Wan, N.; Zou, B.; Sternberg, T. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Delamater, P.L. Spatial accessibility in suboptimally configured health care systems: A modified two-step floating catchment area (M2SFCA) metric. Health Place 2013, 24, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Luo, J. Integrating the Huff model and floating catchment area methods to analyze spatial access to healthcare services. Trans. GIS 2014, 18, 436–448. [Google Scholar] [CrossRef]
- Ngui, A.N.; Apparicio, P. Optimizing the two-step floating catchment area method for measuring spatial accessibility to medical clinics in Montreal. BMC Health Serv. Res. 2011, 11, 166. [Google Scholar] [CrossRef]
- Mao, L.; Nekorchuk, D. Measuring spatial accessibility to healthcare for populations with multiple transportation modes. Health Place 2013, 24, 115–122. [Google Scholar] [CrossRef]
- Fransen, K.; Neutens, T.; De Maeyer, P.; Deruyter, G. A commuter-based two-step floating catchment area method for measuring spatial accessibility of daycare centers. Health Place 2015, 32, 65–73. [Google Scholar] [CrossRef]
- Donald, H.T.; Hoenig, H. Access to health care services for the disabled elderly. Health Serv. Res. 2010, 41, 743–758. [Google Scholar]
- Wu, H.C.; Tseng, M.H. Evaluating Disparities in Elderly Community Care Resources: Using a Geographic Accessibility and Inequality Index. Int. J. Environ. Res. Public Health 2018, 15, 1353. [Google Scholar] [CrossRef]
- Tao, Y.H.; Shen, Y. Spatial difference of medical facility accessibility and influencing factors: A comparative study of registered and floating populations in Shanghai. Prog. Geogr. 2018, 37, 1075–1085. [Google Scholar]
- Meng, T.T.; Zhang, J. Evaluation of Health Care Service Spatial Accessibility and the Analysis of the Spatial Distribution Characteristics in Beijing. Geospat. Inf. 2017, 15, 62–65. [Google Scholar]
- Zhong, S.Y.; Yang, X.; Chen, R. The accessibility measurement of hierarchy public service facilities based on multi-mode network dataset and the two-step 2SFCA: A case study of Beijing’s medical facilities. Geogr. Res. 2016, 35, 731–744. [Google Scholar]
- Huang, A.; Xu, Y.Q.; Liu, C. Research on the Spatial Differentiation of Healthcare Service Function and ItsIntensity Based on Accessibility: A Case Study of Zhangjiakou City in Hebei Province. Econ. Geogr. 2018, 38, 61–71. [Google Scholar]
- Cheng, M.; Lian, Y.J. Spatial accessibility of urban medical facilities based on improved potential model: A case study of Yangpu District in Shanghai. Prog. Geogr. 2018, 37, 266–275. [Google Scholar]
- Yin, C.; He, Q.; Liu, Y.; Chen, W.Q.; Gao, Y. Inequality of public health and its role in spatial accessibility to medical facilities in China. Appl. Geogr. 2018, 92, 50–62. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, H.Y.; Xiong, W.K.; Chen, G. Spatial Accessibilities of Medical Services at County Level Based on Optimized Two-step Floating Catchment Area Method. Sci. Geogr. Sin. 2017, 37, 728–737. [Google Scholar]
- Baidu Map. Available online: http://api.map.baidu.com/lbsapi/getpoint/index.html (accessed on 20 September 2018).
- National Science & Technology Infrastructure of China, Data Sharing Infrastructure of Earth System Science -Data Center of Lower Yellow River Regions. Available online: http://henu.geodata.cn (accessed on 12 October 2018).
- OpenStreetMap (OSM). Available online: https://www.openstreetmap.org/ (accessed on 17 October 2018).
- National Bureau of Statistics. Available online: http://www.stats.gov.cn/tjsj/ (accessed on 10 October 2018).
- Zhang, L.; Lu, Y.Q.; Zhao, Y.Z. Accessibility Assessment and Planning of Hospital—A Case Study on Yizheng City. Hum. Geogr. 2008, 23, 60–66. [Google Scholar]
- Fotheringham, A.S.; Kelly, M.H.; Charlton, M. The demographic impacts of the Irish famine: Towards a greater geographical understanding. Trans. Inst. Br. Geogr. 2013, 38, 221–237. [Google Scholar] [CrossRef]
- Luo, J.; Chen, G.; Li, C.; Xia, B.Y.; Sun, X.; Chen, S. Use of an E2SFCA Method to Measure and Analyse Spatial Accessibility to Medical Services for Elderly People in Wuhan, China. Int. J. Environ. Res. Public Health 2018, 15, 1503. [Google Scholar] [CrossRef]
- Wang, X.; Yang, H.; Duan, Z.; Pan, J. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Soc. Sci. Med. 2018, 209, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.F.; Liu, S.H.; Qi, W. Spatial Differentiation and Influencing Mechanism of Medical Care Accessibility in Beijing: A Migrant Equality Perspective. Chin. Geogr. Sci. 2018, 28, 353–362. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Zhu, M.; Wang, W. Research on the Configuration of the Medical Facilities for elderly of Rural Community. Humanit. Soc. Sci. 2017, 5, 210–214. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Coefficient | p | VIF |
|---|---|---|---|
| Area | 17.982 | 0.000 * | 2.199 |
| Gross industrial output value | −0.000134 | 0.249 | 4.042 |
| Number of industrial enterprises | −0.106436 | 0.309 | 1.194 |
| Elevation | 2.643 | 0.000 * | 1.897 |
| Per capita industrial output | 0.063 | 0.034 * | 3.762 |
| Population density | −0.909 | 0.000 * | 2.129 |
| Road network density | −188.137 | 0.002 * | 1.481 |
| Residential area density | 118.689 | 0.015 * | 1.076 |
| Adjusted R2 | 0.722 | ||
| F-statistics | 522.366 | ||
| F-test | 0.000 * | ||
| AICc | 26927.965 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Qin, Y.; Xu, Y. Inequality and Influencing Factors of Spatial Accessibility of Medical Facilities in Rural Areas of China: A Case Study of Henan Province. Int. J. Environ. Res. Public Health 2019, 16, 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101833
Liu S, Qin Y, Xu Y. Inequality and Influencing Factors of Spatial Accessibility of Medical Facilities in Rural Areas of China: A Case Study of Henan Province. International Journal of Environmental Research and Public Health. 2019; 16(10):1833. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101833
Chicago/Turabian StyleLiu, Shirui, Yaochen Qin, and Yanan Xu. 2019. "Inequality and Influencing Factors of Spatial Accessibility of Medical Facilities in Rural Areas of China: A Case Study of Henan Province" International Journal of Environmental Research and Public Health 16, no. 10: 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101833