Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? (GAPRESEARCH)

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Data Analysis
3. Results
3.1. Number of Published Items and Publication Trend
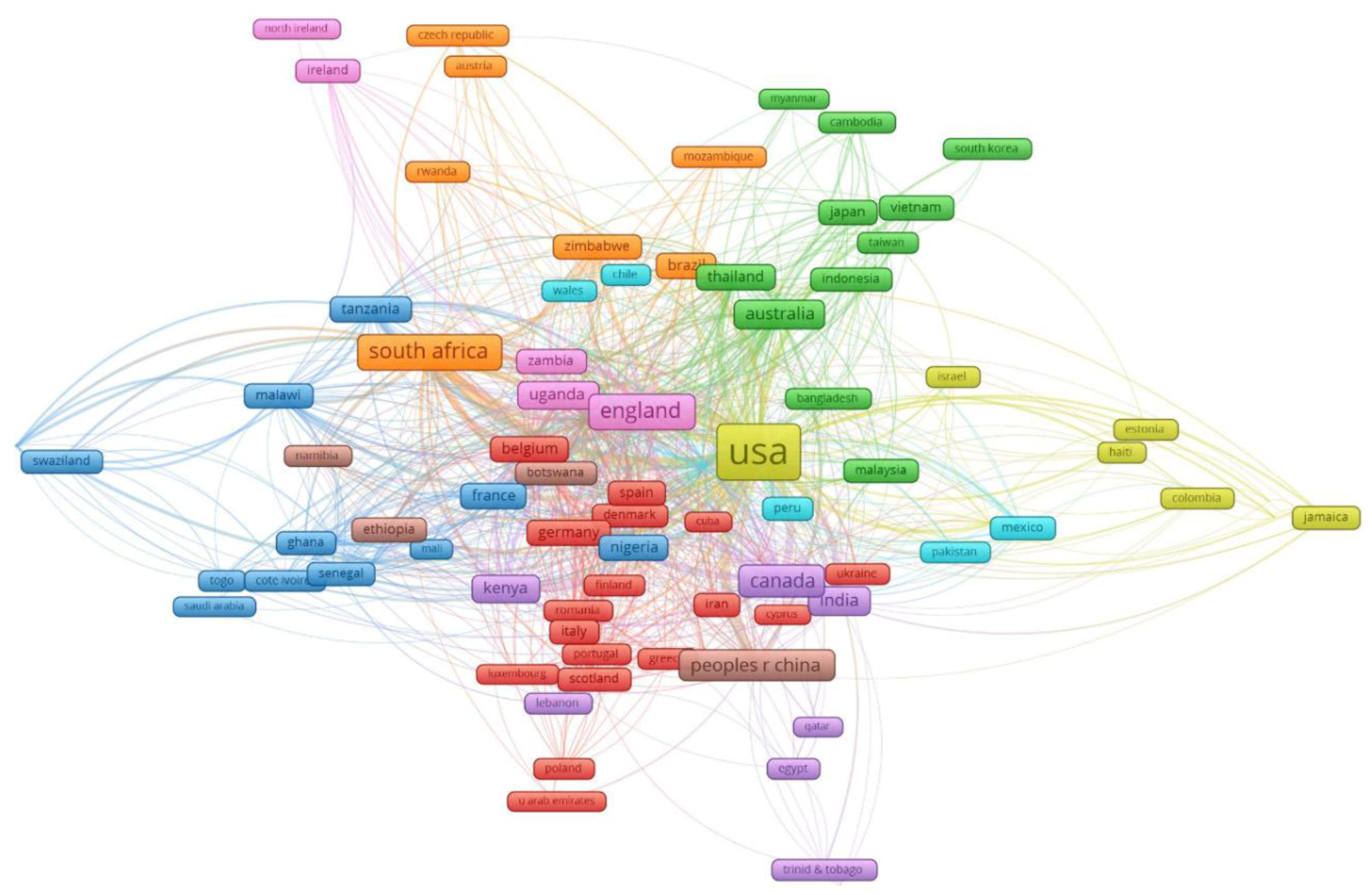
3.2. Authors and Collaborations
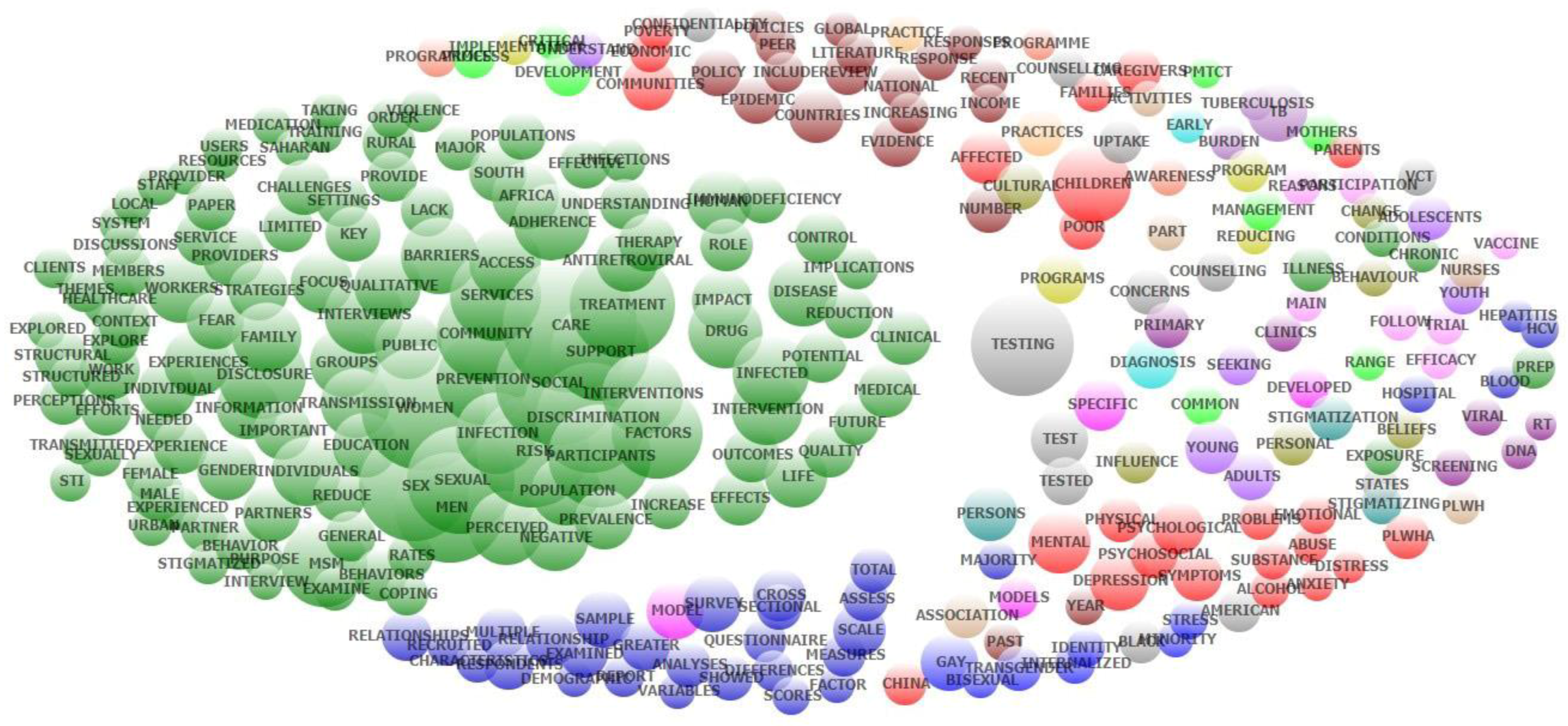
3.3. Keywords and Research Domains
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. HIV/AIDS. Available online: https://www.who.int/features/qa/71/en/ (accessed on 28 May 2019).
- World Health Organization. Data on the size of the HIV/AIDS epidemic. Available online: http://apps.who.int/gho/data/view.main.22100WHO?lang=en (accessed on 26 January 2019).
- Collaborators, G.H. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: The Global Burden of Disease Study 2015. Lancet HIV 2016, 3, e361–e387. [Google Scholar] [CrossRef]
- Grossman, C.I.; Stangl, A.L. Editorial: Global action to reduce HIV stigma and discrimination. J. Int. AIDS Soc. 2013, 16, 18881. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Morroni, C.; Zuniga, J.M.; Sherer, R.; Beyrer, C.; Solomon, S.; Schechter, M.; Rockstroh, J. HIV-related stigma, isolation, discrimination, and serostatus disclosure: A global survey of 2035 HIV-infected adults. J. Int. Assoc. Phys. AIDS Care 2012, 11, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease, C. Pneumocystis pneumonia—Los Angeles. MMWR Morb. Mortal. Wkly. Rep. 1981, 30, 250–252. [Google Scholar]
- Centers for Disease, C. Kaposi’s sarcoma and Pneumocystis pneumonia among homosexual men--New York City and California. MMWR Morb. Mortal. Wkly. Rep. 1981, 30, 305–308. [Google Scholar]
- Global Network of People Living with HIV (GNP+). The People Living with HIV Stigma Index. Secondary The People Living with HIV Stigma Index 2015. Available online: http://www.stigmaindex.org/ (accessed on 28 April 2019).
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Prentice Hall: Upper Saddle River, NJ, USA, 1963. [Google Scholar]
- Turan, J.M.; Nyblade, L. HIV-related stigma as a barrier to achievement of global PMTCT and maternal health goals: A review of the evidence. AIDS Behav. 2013, 17, 2528–2539. [Google Scholar] [CrossRef]
- Schuster, M.A.; Collins, R.; Cunningham, W.E.; Morton, S.C.; Zierler, S.; Wong, M.; Tu, W.; Kanouse, D.E. Perceived discrimination in clinical care in a nationally representative sample of HIV-infected adults receiving health care. J. Gen. Intern. Med. 2005, 20, 807–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringer, K.L.; Turan, B.; McCormick, L.; Durojaiye, M.; Nyblade, L.; Kempf, M.C.; Lichtenstein, B.; Turan, J.M. HIV-Related Stigma Among Healthcare Providers in the Deep South. AIDS Behav. 2016, 20, 115–125. [Google Scholar] [CrossRef]
- Alexandra Marshall, S.; Brewington, K.M.; Kathryn Allison, M.; Haynes, T.F.; Zaller, N.D. Measuring HIV-related stigma among healthcare providers: A systematic review. AIDS Care 2017, 29, 1337–1345. [Google Scholar] [CrossRef]
- Wagner, A.C.; Girard, T.; McShane, K.E.; Margolese, S.; Hart, T.A. HIV-Related Stigma and Overlapping Stigmas Towards People Living With HIV Among Health Care Trainees in Canada. AIDS Educ. Prev. 2017, 29, 364–376. [Google Scholar] [CrossRef]
- Blake Helms, C.; Turan, J.M.; Atkins, G.; Kempf, M.C.; Clay, O.J.; Raper, J.L.; Mugavero, M.J.; Turan, B. Interpersonal Mechanisms Contributing to the Association Between HIV-Related Internalized Stigma and Medication Adherence. AIDS Behav. 2017, 21, 238–247. [Google Scholar] [CrossRef]
- Fekete, E.M.; Williams, S.L.; Skinta, M.D. Internalised HIV-stigma, loneliness, depressive symptoms and sleep quality in people living with HIV. Psychol. Health 2018, 33, 398–415. [Google Scholar] [CrossRef]
- Brown, M.J.; Serovich, J.M.; Kimberly, J.A.; Hu, J. Psychological reactance and HIV-related stigma among women living with HIV. AIDS Care 2016, 28, 745–749. [Google Scholar] [CrossRef]
- Kamen, C.; Arganbright, J.; Kienitz, E.; Weller, M.; Khaylis, A.; Shenkman, T.; Smith, S.; Koopman, C.; Gore-Felton, C. HIV-related stigma: Implications for symptoms of anxiety and depression among Malawian women. Afr. J. AIDS Res. 2015, 14, 67–73. [Google Scholar] [CrossRef]
- Ashaba, S.; Cooper-Vince, C.; Maling, S.; Rukundo, G.Z.; Akena, D.; Tsai, A.C. Internalized HIV stigma, bullying, major depressive disorder, and high-risk suicidality among HIV-positive adolescents in rural Uganda. Glob. Ment. Health 2018, 5, e22. [Google Scholar] [CrossRef] [Green Version]
- Rasoolinajad, M.; Abedinia, N.; Noorbala, A.A.; Mohraz, M.; Badie, B.M.; Hamad, A.; Sahebi, L. Relationship Among HIV-Related Stigma, Mental Health and Quality of life for HIV-Positive Patients in Tehran. AIDS Behav. 2018, 22, 3773–3782. [Google Scholar] [CrossRef]
- Rydstrom, L.L.; Wiklander, M.; Naver, L.; Ygge, B.M.; Eriksson, L.E. HIV-related stigma and health-related quality of life among children living with HIV in Sweden. AIDS Care 2016, 28, 665–671. [Google Scholar] [CrossRef]
- Shrestha, R.; Copenhaver, M.; Bazazi, A.R.; Huedo-Medina, T.B.; Krishnan, A.; Altice, F.L. A Moderated Mediation Model of HIV-Related Stigma, Depression, and Social Support on Health-Related Quality of Life among Incarcerated Malaysian Men with HIV and Opioid Dependence. AIDS Behav. 2017, 21, 1059–1069. [Google Scholar] [CrossRef]
- Katz, I.T.; Ryu, A.E.; Onuegbu, A.G.; Psaros, C.; Weiser, S.D.; Bangsberg, D.R.; Tsai, A.C. Impact of HIV-related stigma on treatment adherence: Systematic review and meta-synthesis. J. Int. AIDS Soc. 2013, 16, 18640. [Google Scholar] [CrossRef] [PubMed]
- Rueda, S.; Mitra, S.; Chen, S.; Gogolishvili, D.; Globerman, J.; Chambers, L.; Wilson, M.; Logie, C.H.; Shi, Q.; Morassaei, S.; et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: A series of meta-analyses. BMJ Open 2016, 6, e011453. [Google Scholar] [CrossRef]
- Sweileh, W.M. Bibliometric analysis of literature in AIDS-related stigma and discrimination. Transl. Behav. Med. 2018, 10, 10. [Google Scholar] [CrossRef]
- Thapa, S.; Hannes, K.; Cargo, M.; Buve, A.; Peters, S.; Dauphin, S.; Mathei, C. Stigma reduction in relation to HIV test uptake in low- and middle-income countries: A realist review. BMC Public Health 2018, 18, 1277. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Data | Unit of Analysis | Analytical Methods | Presentations of Results |
|---|---|---|---|
| Key words, Countries | Words | Frequency of co-occurrence | (1) Map of keywords clusters |
| Abstracts | Words | Exploratory factors analyses | (2) Top 50 constructed research domains (3) Clustering map of the landscapes constructed by these domains. |
| Abstracts | Papers | Latent Dirichlet Allocation | (4) 10 classifications of research topics |
| WoS classification of research areas | WoS research areas | Frequency of co-occurrence | (5) Dendrogram of research disciplines (WoS classification) |
| # | Country | Freq. | Percent | # | Country | Freq. | Percent | # | Country | Freq. | Percent |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | United States | 406 | 14.26 | 42 | Rwanda | 10 | 0.35 | 84 | Sri Lanka | 3 | 0.11 |
| 2 | South Africa | 380 | 13.34 | 43 | Spain | 10 | 0.35 | 85 | Tajikistan | 3 | 0.11 |
| 3 | China | 230 | 8.08 | 44 | New Zealand | 9 | 0.32 | 86 | Togo | 3 | 0.11 |
| 4 | India | 177 | 6.21 | 45 | Senegal | 9 | 0.32 | 87 | Trinidad and Tobago | 3 | 0.11 |
| 5 | Uganda | 127 | 4.46 | 46 | Taiwan | 9 | 0.32 | 88 | Turkey | 3 | 0.11 |
| 6 | Kenya | 116 | 4.07 | 47 | Burkina Faso | 8 | 0.28 | 89 | Albania | 2 | 0.07 |
| 7 | Canada | 104 | 3.65 | 48 | Georgia | 8 | 0.28 | 90 | Bolivia | 2 | 0.07 |
| 8 | Tanzania | 82 | 2.88 | 49 | Ukraine | 8 | 0.28 | 91 | Cuba | 2 | 0.07 |
| 9 | Australia | 73 | 2.56 | 50 | Argentina | 7 | 0.25 | 92 | Czech | 2 | 0.07 |
| 10 | Viet Nam | 67 | 2.35 | 51 | Chile | 7 | 0.25 | 93 | Gabon | 2 | 0.07 |
| 11 | Ethiopia | 59 | 2.07 | 52 | Guatemala | 7 | 0.25 | 94 | Gambia | 2 | 0.07 |
| 12 | Thailand | 50 | 1.76 | 53 | Italy | 7 | 0.25 | 95 | Hungary | 2 | 0.07 |
| 13 | Brazil | 44 | 1.54 | 54 | Lao | 7 | 0.25 | 96 | Kazakhstan | 2 | 0.07 |
| 14 | Ghana | 44 | 1.54 | 55 | Pakistan | 7 | 0.25 | 97 | Libya | 2 | 0.07 |
| 15 | Malawi | 44 | 1.54 | 56 | Bangladesh | 6 | 0.21 | 98 | Madagascar | 2 | 0.07 |
| 16 | Botswana | 43 | 1.51 | 57 | Barbados | 6 | 0.21 | 99 | Mali | 2 | 0.07 |
| 17 | United Kingdom | 43 | 1.51 | 58 | Colombia | 6 | 0.21 | 100 | Philippines | 2 | 0.07 |
| 18 | Zimbabwe | 43 | 1.51 | 59 | Greece | 6 | 0.21 | 101 | Suriname | 2 | 0.07 |
| 19 | Zambia | 40 | 1.40 | 60 | Sudan | 6 | 0.21 | 102 | Wallis and Futuna | 2 | 0.07 |
| 20 | Ireland | 31 | 1.09 | 61 | Belgium | 5 | 0.18 | 103 | Afghanistan | 1 | 0.04 |
| 21 | Japan | 23 | 0.81 | 62 | Estonia | 5 | 0.18 | 104 | Angola | 1 | 0.04 |
| 22 | Mexico | 23 | 0.81 | 63 | Germany | 5 | 0.18 | 105 | Benin | 1 | 0.04 |
| 23 | Indonesia | 22 | 0.77 | 64 | Singapore | 5 | 0.18 | 106 | Bulgaria | 1 | 0.04 |
| 24 | Peru | 22 | 0.77 | 65 | United Arab Emirates | 5 | 0.18 | 107 | Burundi | 1 | 0.04 |
| 25 | Hong Kong | 21 | 0.74 | 66 | Yemen | 5 | 0.18 | 108 | Central African Republic | 1 | 0.04 |
| 26 | Namibia | 21 | 0.74 | 67 | El Salvador | 4 | 0.14 | 109 | Cyprus | 1 | 0.04 |
| 27 | Puerto Rico | 21 | 0.74 | 68 | Myanmar | 4 | 0.14 | 110 | Denmark | 1 | 0.04 |
| 28 | Malaysia | 20 | 0.70 | 69 | Portugal | 4 | 0.14 | 111 | Fiji | 1 | 0.04 |
| 29 | Iran | 19 | 0.67 | 70 | Russian Federation | 4 | 0.14 | 112 | French Guiana | 1 | 0.04 |
| 30 | Nepal | 18 | 0.63 | 71 | Saudi Arabia | 4 | 0.14 | 113 | Grenada | 1 | 0.04 |
| 31 | Swaziland | 16 | 0.56 | 72 | Switzerland | 4 | 0.14 | 114 | Guinea | 1 | 0.04 |
| 32 | France | 15 | 0.53 | 73 | Croatia | 3 | 0.11 | 115 | Jersey | 1 | 0.04 |
| 33 | Mozambique | 15 | 0.53 | 74 | Egypt | 3 | 0.11 | 116 | Macedonia | 1 | 0.04 |
| 34 | Jamaica | 14 | 0.49 | 75 | Guyana | 3 | 0.11 | 117 | Micronesia | 1 | 0.04 |
| 35 | Cambodia | 13 | 0.46 | 76 | Honduras | 3 | 0.11 | 118 | Mongolia | 1 | 0.04 |
| 36 | Netherlands | 13 | 0.46 | 77 | Israel | 3 | 0.11 | 119 | Morocco | 1 | 0.04 |
| 37 | Cameroon | 11 | 0.39 | 78 | Jordan | 3 | 0.11 | 120 | Romania | 1 | 0.04 |
| 38 | Haiti | 11 | 0.39 | 79 | Kyrgyzstan | 3 | 0.11 | 121 | Solomon Islands | 1 | 0.04 |
| 39 | Sweden | 11 | 0.39 | 80 | Nicaragua | 3 | 0.11 | 122 | Somalia | 1 | 0.04 |
| 40 | Lebanon | 10 | 0.35 | 81 | Poland | 3 | 0.11 | 123 | Timor-Leste | 1 | 0.04 |
| 41 | Lesotho | 10 | 0.35 | 82 | Serbia | 3 | 0.11 | 124 | Tunisia | 1 | 0.04 |
| 83 | Sierra Leone | 3 | 0.11 | 125 | Uruguay | 1 | 0.04 |
| Year Published | Total # Papers | Total Citations | Mean Cite Rate Per Year | Total Usage Last 6 Month | Total Usage Last 5 Years | Mean Use Rate Last 6 Month | Mean Use Rate Last 5 Year |
|---|---|---|---|---|---|---|---|
| 2017 | 633 | 806 | 1.27 | 1150 | 3455 | 1.82 | 1.09 |
| 2016 | 661 | 2418 | 1.83 | 712 | 5409 | 1.08 | 1.64 |
| 2015 | 632 | 4208 | 2.22 | 481 | 5930 | 0.76 | 1.88 |
| 2014 | 493 | 5691 | 2.89 | 363 | 5756 | 0.74 | 2.34 |
| 2013 | 520 | 8340 | 3.21 | 337 | 7136 | 0.65 | 2.74 |
| 2012 | 418 | 6992 | 2.79 | 172 | 4369 | 0.41 | 2.09 |
| 2011 | 356 | 6544 | 2.63 | 159 | 3068 | 0.45 | 1.72 |
| 2010 | 340 | 6818 | 2.51 | 131 | 2388 | 0.39 | 1.40 |
| 2009 | 286 | 7486 | 2.91 | 125 | 2133 | 0.44 | 1.49 |
| 2008 | 284 | 8846 | 3.11 | 127 | 1897 | 0.45 | 1.34 |
| 2007 | 243 | 7669 | 2.87 | 107 | 1521 | 0.44 | 1.25 |
| 2006 | 184 | 6523 | 2.95 | 58 | 1052 | 0.32 | 1.14 |
| 2005 | 146 | 6606 | 3.48 | 67 | 920 | 0.46 | 1.26 |
| 2004 | 98 | 4542 | 3.31 | 43 | 634 | 0.44 | 1.29 |
| 2003 | 81 | 7844 | 6.46 | 86 | 1099 | 1.06 | 2.71 |
| 2002 | 68 | 2874 | 2.64 | 25 | 284 | 0.37 | 0.84 |
| 2001 | 59 | 3175 | 3.17 | 18 | 334 | 0.31 | 1.13 |
| 2000 | 69 | 3491 | 2.81 | 28 | 395 | 0.41 | 1.14 |
| 1999 | 53 | 2396 | 2.38 | 12 | 226 | 0.23 | 0.85 |
| 1998 | 40 | 1021 | 1.28 | 11 | 123 | 0.28 | 0.62 |
| 1997 | 54 | 3866 | 3.41 | 14 | 213 | 0.26 | 0.79 |
| 1996 | 53 | 1704 | 1.46 | 9 | 159 | 0.17 | 0.60 |
| 1995 | 46 | 2460 | 2.33 | 12 | 189 | 0.26 | 0.82 |
| 1994 | 31 | 1776 | 2.39 | 8 | 132 | 0.26 | 0.85 |
| 1993 | 26 | 960 | 1.48 | 5 | 69 | 0.19 | 0.53 |
| 1992 | 24 | 1539 | 2.47 | 4 | 111 | 0.17 | 0.93 |
| 1991 | 12 | 565 | 1.74 | 2 | 24 | 0.17 | 0.40 |
| No | Name | Keywords | Eigenvalue | Freq. | % Cases |
|---|---|---|---|---|---|
| 1 | Men (Msm; Sex Sexual) | msm; men; sex; sexual; risk | 4.71 | 6175 | 50.94% |
| 2 | Care Providers | providers; provider; service; care; services; healthcare | 1.61 | 5107 | 48.18% |
| 3 | Fsws; Female Sex | fsws; female; workers; clients; work; sex | 1.75 | 3542 | 39.24% |
| 4 | Sexual Partners | partners; partner; sexual; disclosure; communication | 1.28 | 3347 | 38.17% |
| 5 | Antiretroviral; Therapy | antiretroviral; therapy; adherence; medication; treatment; taking | 2.63 | 4236 | 37.58% |
| 6 | Dna; Rt | dna; rt; viral; discrimination | 1.92 | 2449 | 36.15% |
| 7 | Testing | testing; vct; test; counselling; uptake; tested; counseling; confidentiality | 2.06 | 3227 | 31.50% |
| 8 | Reduction Intervention | intervention; trial; reduction; follow; control; reducing | 2.27 | 2586 | 31.40% |
| 9 | Gender; Transgender | gender; transgender; women; identity | 1.29 | 2412 | 31.23% |
| 10 | Depression and Anxiety; Psychological | anxiety; depression; psychological; distress; symptoms; mental; stress; psychosocial; physical | 4.19 | 3187 | 28.76% |
| 11 | Children; Parents | children; parents; families; caregivers; family; affected | 2.46 | 2544 | 27.82% |
| 12 | Gay Men | gay; bisexual; men; identity | 1.42 | 2156 | 25.20% |
| 13 | Chronic Illness | illness; chronic; disease; conditions | 2.48 | 1834 | 24.60% |
| 14 | Scale Scores; Factor | scale; factor; scores; developed; measures | 1.35 | 1771 | 23.16% |
| 15 | General Population | general; population | 1.48 | 1522 | 21.77% |
| 16 | Family Members | members; family; network | 1.28 | 1466 | 19.45% |
| 17 | Coping Strategies | coping; internalized; strategies | 1.18 | 1262 | 18.63% |
| 18 | Policy and Practice | practice; implications; policy | 1.18 | 1300 | 18.55% |
| 19 | Substance Abuse | abuse; substance; alcohol; mental; violence | 1.67 | 1517 | 18.37% |
| 20 | South Africa | africa; saharan; south | 1.69 | 1745 | 17.06% |
| 21 | Transmission (PMTCT) | pmtct; mothers; transmission | 1.63 | 1124 | 16.34% |
| 22 | QoL; Life Quality | qol; quality; life | 1.5 | 1287 | 16.06% |
| 23 | Youth; Adults and Adolescents | youth; adolescents; young; adults | 1.78 | 1181 | 15.74% |
| 24 | Income Countries | income; countries; global | 3.09 | 1140 | 15.54% |
| 25 | Human Immunodeficiency | immunodeficiency; human | 1.39 | 1460 | 14.97% |
| 26 | Behavior | behavior; behaviors | 1.15 | 951 | 13.52% |
| 27 | Staff Training | staff; management; training | 1.19 | 923 | 13.49% |
| 28 | Sexually Transmitted | transmitted; sexually; infections; sti | 2.11 | 1384 | 12.77% |
| 29 | Drug Users | users; drug | 1.45 | 968 | 12.63% |
| 30 | Black; States | black; states; american | 1.25 | 805 | 11.75% |
| 31 | Majority | majority; respondents | 1.27 | 753 | 11.66% |
| 32 | Cultural Beliefs | beliefs; cultural | 1.24 | 750 | 11.33% |
| 33 | Association of Nurses | nurses; plwh; association | 1.44 | 762 | 11.25% |
| 34 | Demographic Characteristics | characteristics; demographic | 1.38 | 743 | 10.51% |
| 35 | Urban and Rural | rural; urban | 1.31 | 751 | 10.46% |
| 36 | Counselling | counselling programme; programmes; | 1.81 | 737 | 10.16% |
| 37 | Structural | structural | 1.14 | 514 | 8.59% |
| 38 | Vaccine Trial | vaccine; trial; participation | 1.38 | 567 | 8.19% |
| 39 | Order | order | 1.25 | 421 | 7.04% |
| 40 | Common | common | 1.16 | 420 | 7.02% |
| 41 | Prep | prep; exposure | 1.54 | 365 | 5.06% |
| 42 | Resources | resources | 1.22 | 296 | 4.95% |
| 43 | Behaviour | behaviour | 1.13 | 289 | 4.83% |
| 44 | Tuberculosis (Tb | tb; tuberculosis | 1.86 | 333 | 3.59% |
| 45 | Home | home | 1.21 | 198 | 3.31% |
| 46 | India | india | 1.23 | 195 | 3.26% |
| 47 | Screening | screening | 1.56 | 195 | 3.26% |
| 48 | PLHIV | plhiv | 1.18 | 154 | 2.57% |
| 49 | Hepatitis | hepatitis; hcv | 1.98 | 213 | 2.52% |
| 50 | Sexual | couple; disclosure; | 1.25 | 145 | 2.39% |
| # | Title | Journal | Citations | Years | Cite Rate |
|---|---|---|---|---|---|
| 1 | Interventions to reduce HIV/AIDs stigma: What have we learned? | Aids Education And Prevention | 413 | 2003 | 27.5 |
| 2 | AIDS-related Kaposi’s sarcoma: Prospective validation of the AIDS Clinical Trials Group staging classification | Journal Of Clinical Oncology | 156 | 1997 | 7.4 |
| 3 | A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: how far have we come? | Journal Of The International Aids Society | 136 | 2013 | 27.2 |
| 4 | HIV Interventions to Reduce HIV/AIDS Stigma: A Systematic Review | Aids And Behavior | 135 | 2011 | 19.3 |
| 5 | Health work, female sex workers and HIV/AIDS: Global and local dimensions of stigma and deviance as barriers to effective interventions | Social Science & Medicine | 95 | 2008 | 9.5 |
| 6 | Willingness to volunteer in future preventive HIV vaccine trials: Issues and perspectives from three US communities | Journal Of Acquired Immune Deficiency Syndromes | 84 | 2001 | 4.9 |
| 7 | A Qualitative Study of the Barriers and Facilitators to Retention-in-Care Among HIV-Positive Women in the Rural Southeastern United States: Implications for Targeted Interventions | Aids Patient Care And STDs | 77 | 2010 | 9.6 |
| 8 | Getting me back on track”: The role of outreach interventions in engaging and retaining people living with HIV/AIDS in medical care | Aids Patient Care And STDs | 72 | 2007 | 6.5 |
| 9 | Linking sexual and reproductive health and HIV interventions: a systematic review | Journal Of The International Aids Society | 70 | 2010 | 8.8 |
| 10 | Global burden, distribution, and interventions for infectious diseases of poverty | Infectious Diseases Of Poverty | 67 | 2014 | 16.8 |
| 11 | Who Gets Tested for HIV in a South African Urban Township? Implications for Test and Treat and Gender-Based Prevention Interventions | Journal Of Acquired Immune Deficiency Syndromes | 59 | 2011 | 8.4 |
| 12 | Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions | Social Science & Medicine | 54 | 2015 | 18.0 |
| 13 | Preventing discrimination against volunteers in prophylactic HIV vaccine trials: Lessons from a phase II trial | Journal Of Acquired Immune Deficiency Syndromes And Human Retrovirology | 42 | 1998 | 2.1 |
| 14 | Trial-related discrimination in HIV vaccine clinical trials | Aids Research And Human Retroviruses | 40 | 2001 | 2.4 |
| 15 | Informing Faith-Based HIV/AIDS Interventions: HIV-Related Knowledge and Stigmatizing Attitudes at Project FAITH Churches in South Carolina | Public Health Reports | 33 | 2010 | 4.1 |
| 16 | Eliminating the latent HIV reservoir by reactivation strategies Advancing to clinical trials | Human Vaccines & Immunotherapeutics | 31 | 2013 | 6.2 |
| 17 | It’s an Uphill Battle Everyday”: Intersectionality, Low-Income Black Heterosexual Men, and Implications for HIV Prevention Research and Interventions | Psychology Of Men & Masculinity | 31 | 2013 | 6.2 |
| 18 | A model for community representation and participation in HIV prevention trials among women who engage in transactional sex in Africa | Aids Care-Psychological And Socio-Medical Aspects Of Aids/HIV | 27 | 2008 | 2.7 |
| 19 | Uptake of prevention of mother to child transmission interventions in Kenya: health systems are more influential than stigma | Journal Of The International Aids Society | 26 | 2011 | 3.7 |
| 20 | Why blacks do not take part in HIV vaccine trials | Journal Of The National Medical Association | 26 | 2007 | 2.4 |
| 21 | HIV prevention interventions to reduce sexual risk for African Americans: The influence of community-level stigma and psychological processes | Social Science & Medicine | 26 | 2014 | 6.5 |
| 22 | Attitudes and beliefs related to HIV/AIDS in urban religious congregations: Barriers and opportunities for HIV-related interventions | Social Science & Medicine | 25 | 2012 | 4.2 |
| 23 | What can HIV vaccine trials teach us about future HIV vaccine dissemination? | Vaccine | 25 | 2008 | 2.5 |
| 24 | Barriers to participation in HIV drug trials: a systematic review | Lancet Infectious Diseases | 22 | 2006 | 1.8 |
| 25 | Interventions to Improve Psychological Functioning and Health Outcomes of HIV-Infected Individuals with a History of Trauma or PTSD | Current HIV/Aids Reports | 22 | 2012 | 3.7 |
| 26 | Interventions to reduce the sexual risk behaviour of injecting drug users | International Journal Of Drug Policy | 21 | 2005 | 1.6 |
| 27 | Articulating A Rights-Based Approach to HIV Treatment and Prevention Interventions | Current HIV Research | 21 | 2011 | 3.0 |
| 28 | Experiences in conducting multiple community-based HIV prevention trials among women in KwaZulu-Natal, South Africa | Aids Research And Therapy | 21 | 2010 | 2.6 |
| 29 | Willingness to Participate in HIV Vaccine Trials among Men Who Have Sex with Men in Chennai and Mumbai, India: A Social Ecological Approach | Plos One | 20 | 2012 | 3.3 |
| 30 | Community empowerment and involvement of female sex workers in targeted sexual and reproductive health interventions in Africa: a systematic review | Globalization And Health | 19 | 2014 | 4.8 |
| 31 | Why Culture Matters in Health Interventions: Lessons From HIV/AIDS Stigma and NCDs | Health Education & Behavior | 18 | 2014 | 4.5 |
| 32 | Willingness of Chinese injection drug users to participate in HIV vaccine trials | Vaccine | 18 | 2008 | 1.8 |
| 33 | What HIV-Positive MSM Want from Sexual Risk Reduction Interventions: Findings from a Qualitative Study | Aids And Behavior | 18 | 2012 | 3.0 |
| 34 | Perceptions of barriers and facilitators to participation in clinical trials in HIV-Positive latinas: A pilot study | Journal Of Womens Health | 16 | 2007 | 1.5 |
| 35 | Community-based HIV/AIDS interventions to promote psychosocial well-being among people living with HIV/AIDS: a literature review | Health Psychology And Behavioral Medicine | 15 | 2013 | 3.0 |
| 36 | Limited role of culture conversion for decision-making in individual patient care and for advancing novel regimens to confirmatory clinical trials | BMC Medicine | 15 | 2016 | 7.5 |
| 37 | Preparedness for AIDS vaccine trials in India | Indian Journal Of Medical Research | 15 | 2008 | 1.5 |
| 38 | Community preparedness for HIV vaccine trials in the Democratic Republic of Congo | Culture Health & Sexuality | 14 | 2006 | 1.2 |
| 39 | Community-based HIV prevention interventions that combat anti-gay stigma for men who have sex with men and for transgender women | Journal Of Public Health Policy | 14 | 2013 | 2.8 |
| 40 | Perceptions of a community sample about participation in future HIV vaccine trials in South India | Aids And Behavior | 14 | 2007 | 1.3 |
| 41 | Systematic review of stigma reducing interventions for African/Black diasporic women | Journal Of The International Aids Society | 14 | 2015 | 4.7 |
| 42 | ‘Rumours’ and clinical trials: a retrospective examination of a pediatric malnutrition study in Zambia, southern Africa | Bmc Public Health | 14 | 2010 | 1.8 |
| 43 | Gender-Specific HIV Prevention Interventions for Women Who Use Alcohol and Other Drugs: The Evolution of the Science and Future Directions | Jaids-Journal Of Acquired Immune Deficiency Syndromes | 12 | 2015 | 4.0 |
| 44 | The influence of social determinants on evidence-based behavioral interventions-considerations for implementation in community settings | Translational Behavioral Medicine | 11 | 2012 | 1.8 |
| 45 | Women, reproductive rights, and HIV/AIDS: Issues on which research and interventions are still needed | Journal Of Health Population And Nutrition | 11 | 2006 | 0.9 |
| 46 | What Interventions Are Needed for Women and Girls Who Use Drugs? A Global Perspective | Journal Of Acquired Immune Deficiency Syndromes | 10 | 2015 | 3.3 |
| 47 | The preexposure prophylaxis revolution; from clinical trials to programmatic implementation | Current Opinion In HIV And Aids | 10 | 2016 | 5.0 |
| 48 | Antiretroviral interventions to reduce mother-to-child transmission of human immunodeficiency virus: challenges for health systems, communities and society | Bulletin Of The World Health Organization | 10 | 2000 | 0.6 |
| 49 | If It’s Not Working, Why Would They Be Testing It?”: mental models of HIV vaccine trials and preventive misconception among men who have sex with men in India | BMC Public Health | 9 | 2013 | 1.8 |
| 50 | Effectiveness of Sport-Based HIV Prevention Interventions: A Systematic Review of the Evidence | Aids And Behavior | 9 | 2013 | 1.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; Phan, H.T.; Latkin, C.A.; Nguyen, H.L.T.; Hoang, C.L.; Ho, C.S.H.; Ho, R.C.M. Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? (GAPRESEARCH). Int. J. Environ. Res. Public Health 2019, 16, 1899. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111899
Tran BX, Phan HT, Latkin CA, Nguyen HLT, Hoang CL, Ho CSH, Ho RCM. Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? (GAPRESEARCH). International Journal of Environmental Research and Public Health. 2019; 16(11):1899. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111899
Chicago/Turabian StyleTran, Bach Xuan, Hai Thanh Phan, Carl A. Latkin, Huong Lan Thi Nguyen, Chi Linh Hoang, Cyrus S.H. Ho, and Roger C.M. Ho. 2019. "Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? (GAPRESEARCH)" International Journal of Environmental Research and Public Health 16, no. 11: 1899. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16111899