1. Introduction
In Lithuania and internationally, malocclusion is a major contributor to oral health among adolescents [
1,
2,
3]. Malocclusion causes a lot of trouble, but pain is not one of them. It can result also disturbances of oral function such as mastication, swallowing, and speech, as well as can cause psychosocial problems related to impaired dento-facial aesthetics which exert an adverse impact on the Oral Health-Related Quality of Life (OHRQoL) [
4,
5,
6]. Concern with the impact of malocclusion on OHRQoL has grown considerably in recent years as a consequence of increased patient awareness of this condition, as well as of heightened expectations regarding orthodontic treatment opportunities [
7]. The importance of OHRQoL is specifically relevant for adolescents, because they are particularly sensitive to a variety of impacts, such as appearance, that may affect their well-being and influence their social skills and education [
8,
9]. It has been suggested that the OHRQoL should be measured in oral health surveys for children and adolescents [
10].
Previous investigations have shown that a more unfavorable socioeconomic status (SES) generally translates to inferior oral health among children and adolescents [
11,
12]. The existence of social inequality may, therefore, also have impact upon the treatment of malocclusion. Most malocclusion cases are still not treated properly due to the lack of awareness of young patients and their parents about this condition, the inadequacy of dental resources, inaccessibility to dental services, the lack of a dental workforce, and many factors related to SES. Malocclusion treatment is often expensive and can be impossible for disadvantaged populations. It has also been demonstrated that SES resulted in poorer OHRQoL [
13,
14,
15,
16]. For instance, in the study of Brazilian schoolchildren aged 12 years, after adjusting for potential confounders, family income and mothers’ education showed a statistically significant association with all health domains of the OHRQoL [
17].
In general, OHRQoL is measured by instruments that have been validated for this purpose [
18]. Among these instruments, the Child Perceptions Questionnaire (CPQ
11–14), developed for children aged 11–14 years by a group of Canadian researchers [
19], has gained the highest popularity. It describes the following domains of OHRQoL: oral symptoms (OS), functional limitations (FL), emotional well-being (EWB), and social well-being (SWB) [
19]. It is important to consider that clinical and social determinants may have different impacts on domains of OHRQoL. Therefore, the evaluation of OHRQoL by its domains (OS, FL, EWB, SWB) allows for a more detailed analysis of SES determinants. However, the impact of adolescent family affluence on each domain has not yet been adequately explored, and the currently available results in this field of research are controversial [
17].
This study also intends to examine the impact of malocclusion on OHRQoL. Though, the objective quantitative assessment of malocclusion was necessary. The prevalence and severity of the various features of malocclusion can be assessed using orthodontic indexes. The index of orthodontic treatment need (IOTN) and index of complexity, outcome and need (ICON) are the most commonly used indexes in epidemiological studies [
20,
21,
22]. Our choice of ICON in this study was based on its advantage over other orthodontic indexes. ICON incorporates the esthetic score into an integral part of the five assessment components. Even more, what is important for epidemiological studies, the components can be measured directly on patients (no need to have dental casts). The present study aims to explore the impact of family affluence on OHRQoL among Lithuanian adolescents aged 11–18 years. The hypotheses tested in this study were: (1) higher family affluence is associated with better adolescent OHRQoL; (2) family affluence influences each CPQ domain specifically; (3) family affluence has a greater effect on OHRQoL than on malocclusion.
2. Materials and Methods
2.1. Ethical Statement
The ethical approval for the examination of schoolchildren was issued by the Kaunas Regional Biomedical Research Ethics Committee on 27 November 2012 (No. BE-2-47). Written informed consent for child’s examination was obtained from both parents of each child who participated in the study. Confidentiality and anonymity of participants was guaranteed.
2.2. Sample Size Calculation
The calculation of sample size was produced with software G*Power 3.1 (University of Dusseldorf, Dusseldorf, Germany) [
23]. The procedure of calculation assumed a Poisson regression, considering 80% power, a confidence level of 5%, and a mean sum score ratio to be detected of at least 1.1. For each age group, the minimum number of participants required by these parameters was 260. Thus, since three age groups were studied, the total required sample size was estimated to be
n = 3 × 260 = 780.
2.3. Study Design, Participants, and Data Collection
This observational study had a cross-sectional design and targeted adolescents from 11 to 18 years old, who were divided into three age groups: 11–14, 15–16, and 17–18.
A random, two-stage sampling design was used to select the initial sample. Twenty public schools were randomly selected from the list of schools in Lithuania, and, in each school, classes from grades 6 to 11 were randomly selected. The initial sample (n = 1464) was almost twice as big as the estimated required value, because only half of the students were expected to participate in the study.
The principals of the selected schools were contacted introducing the study and discussing the most appropriate circumstances of the schoolchildren’s examination. An information letter was then sent to parents asking them for permission their child to be examined.
Both a questionnaire survey and dental examination were conducted to collect data. Under the supervision of a class teacher, schoolchildren completed anonymous self-administrated questionnaires in the classroom before their dental examination. Dental examinations were performed in school medical offices.
In the selected schools, 1160 students participated in the questionnaire survey, and 996 students completed the dental examination. Thus, the response rates for the questionnaire survey and examination were 80% and 68%, respectively.
2.4. Evaluation of Oral Health-Related Quality of Life
The Child Perception Questionnaire (CPQ), originally developed by Jokovic et al. [
19], was used to evaluate OHRQoL. The Lithuanian version of this questionnaire was translated, revised, and validated by Kavaliauskiene et al. [
24]. The instrument, which includes a modification of the item concerning oral pain, has presented good results for the assessment of psychometric properties among adolescents 11 to 18 years of age [
24,
25].
The whole CPQ consists of 37 items scored on a 5-point Likert scale ranging from 0 (“never”) to 4 (“every day or almost every day”) (
Supplementary File S1). There are four subscales to describe OHRQoL domains: oral symptoms (OS, six items), functional limitations (FL, nine items), emotional well-being (EWB, nine items), and social well-being (SWB, 13 items). In the analysis, the scores for each item were added together to get a sum score of each domain, as well as of the whole CPQ. Note that higher sum scores refer to inferior OHRQoL.
2.5. Evaluation of Orthodontic Status
The dental examinations were performed according to the recommendations of the World Health Organization for epidemiological surveys [
26]. Orthodontic examination was a part of the complex dental examination. All students were examined by one orthodontic specialist (A.K.) who was trained and graded in the reliability of assessing orthodontic status (U.K. Cardiff University School of Dentistry, 2012).
The Index of Complexity, Outcome, and Need (ICON) has been shown to be a valid measure of orthodontic status in epidemiological studies [
21,
22]. The index was recorded using the methodology by Richmond [
27]. A single ICON score is based on five occlusal traits that are weighted and then added together: (1) an aesthetic component (AC) (weighted by 7); (2) upper arch crowding or spacing (weighted by 5); (3) crossbite (weighted by 5); (4) overbite or open bite (weighted by 4); and (5) left and right buccal segment antero-posterior relationship (weighted by 3). The AC consists of 10 color photographs showing front-view dentition graded from 1 (most attractive) to 10 (least attractive) which were used to identify and rate the participant (
Supplementary File S2). A cut-off point of 43 was set to mark the unambiguous need for orthodontic treatment [
27].
2.6. Evaluation of Family Affluence
The social position of adolescents was evaluated by their family affluence using Family Affluence Scale (FAS), which was specially designed for the questionnaire surveys among children and adolescents [
28]. For this purpose, the adolescents were asked how many cars, home computers, child’s bedrooms, and travels with children on holiday their family had (
Supplementary File S1). Based on respondent’s responses to these four items, a sum score was calculated. Then, a three-point ordinal variable FAS was compiled: 1 = low affluence (score 0–3); 2 = medium affluence (score 4–5); 3 = high affluence (score 6 and more) [
28].
2.7. Statistical Analysis
The study data were analyzed using the SPSS statistical package supplemented with AMOS (version 21; IBM SPSS Inc, Chicago, IL, USA, 2012). Descriptive statistics were first estimated as the mean, standard deviation, median, interquartile range (IQR), and percentages, as appropriate. Categorical variables were tested by the Chi-square test and Z test with Bonferroni correction. p-values were obtained from two-sided statistical tests, and significance level was p ≤ 0.05.
The Kolmogorov–Smirnov test showed that the sum scores of the whole CPQ and its domains had a non-normal distribution. They were skewed in the direction of low values, and consequently, more-or-less followed a Poisson distribution. Thus, non-parametric methods of statistical data analysis were employed. For the same reason, the direct association of the sum scores of the CPQ with clinical and socio-demographic variables was analyzed using the Negative Binomial Regression (NBR), a modified Poisson regression model [
29,
30,
31]. In the present analyses, the sum score of the whole CPQ or its domains was the dependent variable, and the ICON and socio-demographic variables were the independent variables. The strength of association between dependent and independent variables was measured using the Ratio of Sum Score Means (RSSM), which indicates how many times the mean value of a dependent variable increases when the value of an independent variable increases by one unit.
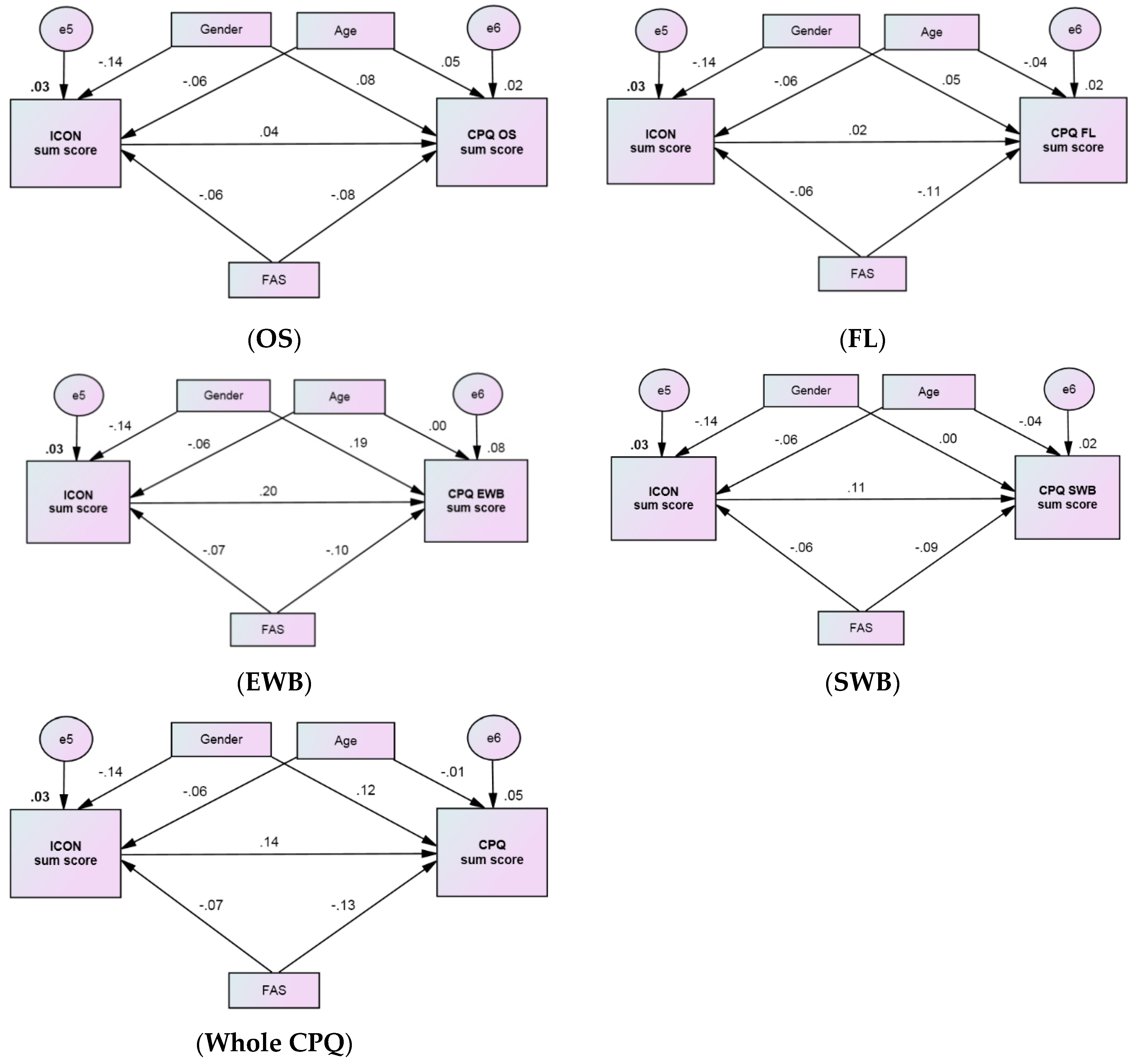
Finally, path analysis was used to examine the hypothesized causal relationships of OHRQoL with ICON, family affluence, gender, and age. These relationships were assumed to be unidirectional. Structural equation modelling was conducted to assess the final model using a maximum likelihood estimation method, given its applicability to non-normal data [
32,
33,
34]. The final model provided standardized regression weights (
β) which showed the strength of the relationship between two connected variables. The χ
2 statistic was used to assess the magnitude of the discrepancy between the sample and fitted covariance matrices, where
p > 0.05 indicated that the model and data were consistent. In addition, the root mean square error of approximation (RMSEA), the comparative fit index (CFI), and the incremental fit index (IFI) were employed to evaluate the model’s goodness-of-fit (RMSEA < 0.08, and CFI > 0.90, and IFI > 090 indicate an acceptable model fit; and RMSEA < 0.05, and CFI > 0.95 and IFI > 0.95 indicate a very good fit) [
32]. Path analysis was performed using AMOS 21 (SPSS Inc., Chicago, IL, USA) [
33].
4. Discussion
The models examined in the current study provided a reasonable fit for the data, indicating that they effectively identified the impact of family affluence on OHRQoL among adolescents in Lithuania. All models based on the correlation analysis, negative binomial regression analysis, and path analysis showed evidence that higher family socioeconomic status has a direct positive impact on adolescent OHRQoL rather than an indirect impact via malocclusion that certainly provides a negative influence on OHRQoL.
This conclusion was reached in response to several questions. Firstly, the relationship between malocclusion and OHRQoL was assessed. Although several hypotheses have been proposed and tested, there is still no generally accepted opinion among researchers [
35]. One of the causes for this might be the use of an inappropriate model (analysis method) in previous studies, since this association is much more sophisticated than a simple linear one. It is possible that, for this reason, some population-based studies reported no significant relationship between the CPQ sum score and malocclusion [
14,
36]. However, recent systematic reviews and meta-analyses of the literature have claimed that there is evidence for a clear negative influence of malocclusion on OHRQoL [
5]. They showed also that the strength of the association differs between the OHRQoL domains. In most cases, a negative impact of malocclusion on the social and emotional domains of OHRQoL has been reported [
4,
5,
6]. The results of the present study and our recent study [
37] support this, agreeing with findings of the studies that affirmed a significant relationship between the severity of malocclusion and sum scores of the EWB and SWB domains [
38,
39,
40,
41]. The reasons for this finding is that social life and emotional perceptions play important roles in adolescents’ values. For example, visible orthodontic traits can be particularly relevant for adolescents, who can then become the victims of teasing and bullying [
42,
43].
The association between SES and OHRQoL seems to be commonly questioned in this field of research. We also hypothesized that there is a direct association between higher family affluence and better adolescent OHRQoL, e.g., a lower CPQ sum score. This hypothesis was confirmed by both NBR and path analyses. The link was significant for all CPQ domains but, according to the NBR analysis, the highest impact of family affluence was found in the FL, EWB, and SWB domains. Many researchers have also noted that individuals from more affluent families have significantly better OHRQoL than their peers from less affluent families [
16,
44,
45,
46,
47,
48]. There is evidence that children living in more affluent families are more likely to benefit from good oral hygiene, regularly visit a dentist, and be better educated in healthy lifestyle skills, thus resulting in better OHRQoL [
5,
49,
50,
51,
52]. Similarly, in a study of 12–15-year-old orphans in India, Kumar et al. found that children without parents presented poorer scores for OHRQoL compared with those that had parents [
53].
An indirect effect of family affluence on OHRQoL across all aspects of orthodontic status was relatively small, because a negligible relationship between malocclusion and family affluence was found. The literature contains a few studies that have investigated the impact of social variables on malocclusion prevalence among children and adolescents. Among these, several studies described severe malocclusions in lower SES adolescents undergoing orthodontic treatment [
54] or a higher prevalence of malocclusion among adolescents residing in less affluent districts [
55]. An inverse association, in which high SES children showed a higher prevalence of malocclusion, was revealed by Normando et al. in a study of primary dentition in children from the Brazilian Amazon [
56]. Moreover, household social class was considered to be a predictor of the orthodontic treatment outcome [
57]. In contrast to these studies, the present findings corroborate the results of other studies which showed that the distribution of the type and grading of the treatment need is similar throughout the different social classes [
58,
59].
In the present study, OHRQoL was investigated throughout the full adolescence period (11–18 years). Hence, we were able to regard adolescent age as a predictor of malocclusion and OHRQoL. The path analysis showed a moderate effect of age on the severity of malocclusion, indicating a lower ICON sum score as adolescent age increased. Several studies on malocclusion in the Lithuanian adolescent population have shown similar results [
3]. However, the present analysis did not indicate any significant relationship between age and OHRQoL. The available research data on this relationship is controversial [
7].
Adolescent gender appeared to be a more important factor in the prevalence of malocclusion and in the assessment of OHRQoL. The comparison of genders in the path analysis showed that the ICON sum score was lower among girls, which means that the need for orthodontic treatment was more prevalent among boys. In contrast, the literature shows that the demand for orthodontic treatment is higher among girls than among boys [
60]. The gender difference in seeking of orthodontic treatment appears to be related to differences in perceived health and the value of oral health among boys and girls [
51]. Our research showed that girls were more likely to experience issues related to emotional well-being (EWB domain). Similar observations have been described in other studies [
40,
61,
62,
63], although some others have not found that such a relationship exists [
7,
50].
The present study is one of the first studies on OHRQoL in Lithuanian adolescents [
24,
37]. However, methodological procedures were used to increase the power of the study, such as the validation of the CPQ instrument [
24,
25], obtaining a representative and population-based sample, performing a pilot study, and standardized examiner. The use of path analysis can also be considered a positive aspect due to its usefulness in the interpretation of relationships among the variables.
The main limitations of the present study are the cross-sectional design, which did not enable a causal relationship between the variables to be established. Moreover, the ICON was developed for permanent teeth and so has a tendency to be oversensitive during the mixed dentition period, possibly confounding the results in the group of adolescents aged 11–14 years [
27]. In addition, a possible weakness of this study may be related to the use of the CPQ, which is a generic measure of OHRQoL, so some of its items could not address aspects specifically related to malocclusion. Regardless, the present findings highlight the impact of social factors (namely, family affluence) on adolescent OHRQoL and can assist in the establishment of more effective actions in orthodontic practice and public health.




{kind=link}