Understanding the Factors Influencing Patient E-Health Literacy in Online Health Communities (OHCs): A Social Cognitive Theory Perspective

Abstract
:1. Introduction
1.1. Online Health Communities
1.2. E-Health Literacy
1.3. Social Cognitive Theory
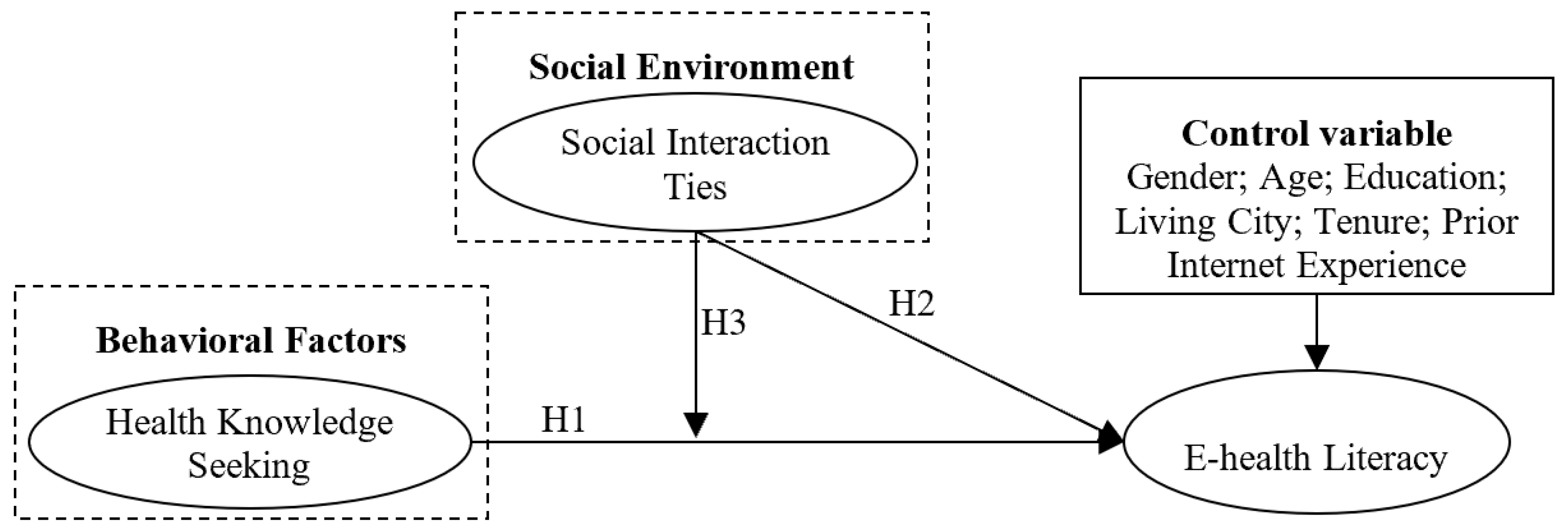
1.4. Hypotheses and Research Model
2. Materials and Methods
2.1. Research Design
2.2. Data Collection
2.3. Data Analysis
3. Results
4. Discussion
4.1. Theoretical Contributions
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gu, D.; Guo, J.; Liang, C.; Lu, W.; Zhao, S.; Liu, B.; Long, T. Social Media-Based health management systems and sustained health engagement: TPB perspective. Int. J. Environ. Res. Public Health 2019, 16, 1495. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.K.; Cheung, M. Online health information seeking and eHealth literacy among patients attending a primary care clinic in hong kong: A Cross-Sectional survey. J. Med. Internet Res. 2019, 21, e10831. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Schulz, P. The measurements and an elaborated understanding of chinese eHealth literacy (C-eHEALS) in chronic patients in china. Int. J. Environ. Res. Public Health 2018, 15, 1553. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Medicine 2.0: Social networking, collaboration, participation, apomediation, and openness. J. Med. Internet Res. 2008, 10, e22. [Google Scholar] [CrossRef] [PubMed]
- Hara, N.; Foon Hew, K. Knowledge-sharing in an online community of health-care professionals. Inf. Technol. People 2007, 20, 235–261. [Google Scholar] [CrossRef]
- Huang, K.; Chengalur-Smith, I.; Ran, W. Not just for support: Companionship activities in healthcare virtual support communities. Commun. Assoc. Inf. Syst. 2014, 29, 561–594. [Google Scholar] [CrossRef]
- Yan, L.; Tan, Y. Feeling blue? Go online: An empirical study of social support among patients. Inf. Syst. Res. 2014, 25, 667–891. [Google Scholar] [CrossRef]
- Yao, T.; Zheng, Q.; Fan, X. The impact of online social support on patients’ quality of life and the moderating role of social exclusion. J. Serv. Res. 2015, 18, 369–383. [Google Scholar] [CrossRef]
- Guo, S.; Guo, X.; Fang, Y.; Vogel, D. How doctors gain social and economic returns in online Health-Care communities: A professional capital perspective. J. Manag. Inf. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Liu, X.; Guo, X.; Wu, H.; Wu, T. The impact of individual and organizational reputation on physicians’ appointments online. Int. J. Electron. Commer. 2016, 20, 551–577. [Google Scholar] [CrossRef]
- Zhou, J.; Amo, L.; Ye, C.; Kai, S. Using reputation to predict online psychological counselor appointment: Evidence from a chinese website. In Proceedings of the 2018 ACM SIGMIS Conference on Computers and People Research, Buffalo, NY, USA, 18–20 June 2018. [Google Scholar]
- Gentles, S.J.; Lokker, C.; McKibbon, K.A. Health information technology to facilitate communication involving health care providers, caregivers, and pediatric patients: A scoping review. J. Med. Internet Res. 2010, 12, e22. [Google Scholar] [CrossRef] [PubMed]
- Van der Eijk, M.; Faber, M.J.; Aarts, J.W.; Kremer, J.A.; Munneke, M.; Bloem, B.R. Using online health communities to deliver patient-centered care to people with chronic conditions. J. Med. Internet Res. 2013, 15, e115. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Maramba, I.; Wheeler, S. Wikis, blogs and podcasts: A new generation of Web-based tools for virtual collaborative clinical practice and education. BMC Med. Educ. 2006, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Ciesielka, D. Using a wiki to meet graduate nursing education competencies in collaboration and community health. J. Nurs. Educ. 2008, 47, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. EHealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.S.; Prestin, A.; Lyons, C.; Wen, K. Web 2.0 for health promotion: Reviewing the current evidence. Am. J. Public Health 2013, 103, e9–e18. [Google Scholar] [CrossRef] [PubMed]
- Korda, H.; Itani, Z. Harnessing social media for health promotion and behavior change. Health Promot. Pract. 2013, 14, 15–23. [Google Scholar] [CrossRef]
- Balatsoukas, P.; Kennedy, C.M.; Buchan, I.; Powell, J.; Ainsworth, J. The role of social network technologies in online health promotion: A narrative review of theoretical and empirical factors influencing intervention effectiveness. J. Med. Internet Res. 2015, 17, e141. [Google Scholar] [CrossRef]
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Zhou, J. Factors influencing people’s personal information disclosure behaviors in online health communities: A pilot study. Asia Pac. J. Public Health 2018, 30, 286–295. [Google Scholar] [CrossRef]
- Nambisan, P. Information seeking and social support in online health communities: Impact on patients’ perceived empathy. J. Am. Med. Inf. Assoc. 2011, 18, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.A.; Hu, X.; Orrange, S.E.; Kravitz, R.L. Lingering questions and doubts: Online information-seeking of support forum members following their medical visits. Patient Educ. Couns. 2011, 85, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Bodie, G.D.; Dutta, M.J. Understanding health literacy for strategic health marketing: EHealth literacy, health disparities, and the digital divide. Health Mark. Q. 2008, 25, 175–203. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, N.; Kindratt, T.B.; Pagels, P.; Foster, B.; Gimpel, N.E. Health literacy, health information seeking behaviors and internet use among patients attending a private and public clinic in the same geographic area. J. Community Health 2014, 39, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Knapp, C.; Madden, V.; Wang, H.; Sloyer, P.; Shenkman, E. Internet use and eHealth literacy of low-income parents whose children have special health care needs. J. Med. Internet Res. 2011, 13, e75. [Google Scholar] [CrossRef] [PubMed]
- Paek, H.; Hove, T. Social cognitive factors and perceived social influences that improve adolescent eHealth literacy. Health Commun. 2012, 27, 727–737. [Google Scholar] [CrossRef]
- Robb, M.; Shellenbarger, T. Influential factors and perceptions of eHealth literacy among undergraduate college students. Online J. Nurs. Inform. 2014, 18. [Google Scholar] [CrossRef]
- Hsu, W.; Chiang, C.; Yang, S. The effect of individual factors on health behaviors among college students: The mediating effects of eHealth literacy. J. Med. Internet Res. 2014, 16, e287. [Google Scholar] [CrossRef]
- Milne, R.A.; Puts, M.T.; Papadakos, J.; Le, L.W.; Milne, V.C.; Hope, A.J.; Catton, P.; Giuliani, M.E. Predictors of high eHealth literacy in primary lung cancer survivors. J. Cancer Educ. 2015, 30, 685–692. [Google Scholar] [CrossRef]
- Chang, F.; Chiu, C.; Chen, P.; Miao, N.; Lee, C.; Chiang, J.; Pan, Y. Relationship between parental and adolescent eHealth literacy and online health information seeking in Taiwan. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 618–624. [Google Scholar] [CrossRef]
- Dashti, S.; Peyman, N.; Tajfard, M.; Esmaeeli, H. E-Health literacy of medical and health sciences university students in Mashhad, Iran in 2016: A pilot study. Electron. Physician 2017, 9, 3966. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W. The effect of age on electronic health literacy: Mixed-Method study. JMIR Hum. Factors 2019, 6, e11480. [Google Scholar] [CrossRef] [PubMed]
- Levin-Zamir, D.; Bertschi, I. Media health literacy, eHealth literacy, and the role of the social environment in context. Int. J. Environ. Res. Public Health 2018, 15, 1643. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Wang, D. The role of online communities in reducing urban-rural health disparities in china. J. Am. Soc. Inf. Sci. Technol. 2018, 69, 890–899. [Google Scholar] [CrossRef]
- Kreps, G.L.; Neuhauser, L. New directions in eHealth communication: Opportunities and challenges. Patient Educ. Couns. 2010, 78, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Neuhauser, L.; Kreps, G.L. EHealth communication and behavior change: Promise and performance. Soc. Semiot. 2010, 20, 9–27. [Google Scholar] [CrossRef]
- Graffigna, G.; Barello, S.; Triberti, S.; Wiederhold, B.K.; Bosio, A.C.; Riva, G. Enabling eHealth as a pathway for patient engagement: A toolkit for medical practice. In Annual Review of Cybertherapy and Telemedicine; Wiederhold, B.K., Riva, G., Eds.; IOS Press: Amsterdam, The Netherlands, 2014; pp. 13–21. [Google Scholar]
- Abraham, C.; Conner, M.; Norman, P. Health Promotion from the Perspective of Social Cognitive Theory. In Understanding and Changing Health Behaviour; Psychology Press: London, UK, 2013; pp. 315–356. [Google Scholar]
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Zhang, X.; Liu, S.; Deng, Z.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Hum. Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Tsai, C. Integrating social capital theory, social cognitive theory, and the technology acceptance model to explore a behavioral model of telehealth systems. Int. J. Environ. Res. Public Health 2014, 11, 4905–4925. [Google Scholar] [CrossRef]
- Shu, Q.; Tu, Q.; Wang, K. The impact of computer self-efficacy and technology dependence on computer-related technostress: A social cognitive theory perspective. Int. J. Hum. Comput. Interact. 2011, 27, 923–939. [Google Scholar] [CrossRef]
- Baranowski, T.; Perry, C.L.; Parcel, G.S. How individuals, environments, and health behavior interact. In Health Behavior and Health Education: Theory, Research, and Practice, 3rd ed.; Glanz, K., Rimer, B.K., Lewis, F.M., Eds.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 165–184. [Google Scholar]
- Zhou, J.; Zuo, M.; Yu, Y.; Chai, W. How fundamental and supplemental interactions affect users’ knowledge sharing in virtual communities? A social cognitive perspective. Internet Res. 2014, 24, 566–586. [Google Scholar] [CrossRef]
- Chiu, C.M.; Hsu, M.H.; Wang, E.T.G. Understanding knowledge sharing in virtual communities: An integration of social capital and social cognitive theories. Decis. Support Syst. 2006, 42, 1872–1888. [Google Scholar] [CrossRef]
- Yan, Y.; Davison, R.M. Exploring behavioral transfer from knowledge seeking to knowledge contributing: The mediating role of intrinsic motivation. J. Am. Soc. Inf. Sci. Technol. 2013, 64, 1144–1157. [Google Scholar] [CrossRef]
- Alleman, J.R. Online counseling: The internet and mental health treatment. Psychother. Theory Res. Pract. Train. 2002, 39, 199–209. [Google Scholar] [CrossRef]
- Dennis, A.R.; Fuller, R.M.; Valacich, J.S. Media, tasks, and communication processes: A theory of media synchronicity. MIS Q. 2008, 32, 575–600. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; SAGE Publications: London, UK, 1991. [Google Scholar]



{kind=link}
{kind=link}
| Sources | Context/Objective | Independent Variables | Dependent Variables | Findings |
|---|---|---|---|---|
| [26] | Internet, 2371 parents | e-health literacy | parent’s gender; parent’s race/ethnicity; parental language spoken at home; parent’s educational attainment; parent’s marital status; household type; child’s health; age | Exception of parent’s gender, parent’s marital status, and household type, all other factors have positive effects |
| [27] | Internet, 182 middle schoolers | e-health literacy | outcome expectations; training involvement; health motivation; perceived injunctive norm; perceived descriptive norm; subjective norm; personal norm | Exception of health motivation, all other factors have positive effects |
| [28] | 59 college students | levels of e-health literacy | race, age, class standing, college major, final course grades, use of the Internet, time spent on the Internet | Only the effect of use of the Internet is significant and positive |
| [29] | 525 valid college students | e-health literacy (as a mediator) | health status; degree of health concern | All effects are significant and positive |
| [30] | 83 lung cancer survivors | e-health literacy | age; gender; living situation; overall health; overall quality of life; histology; education; access to e-resources | Only the effects of education and access to e-resources are significant and positive |
| [31] | 1917 parents and 1417 students | e-health literacy | parent: age; education; marital status; household poverty; area; parent Internet skill confidence; parent Internet skills adolescent: sex; grade; academic performance; adolescent health information literacy | Parent: Exception of age, marital status, and area, all other factors have positive effects Adolescent: Exception of sex, all other factors have positive effects |
| [32] | 192 participants | e-health literacy | gender; department; education level; health status; monthly income; website preference categories | All effects are positive and significant |
| [33] | 65 traditional college students and 143 older adult students | overall e-health literacy; functional e-health literacy | age | Age difference does exist between different groups |
| [2] | 1162 patients who use the Internet | e-health literacy | age; self-rated health; Internet use frequency; online health information seeking frequency; types of health information sought | Age difference exists. All other effects are positive and significant |
| Variables | n | % |
|---|---|---|
| Gender | ||
| Male | 112 | 33.6 |
| Female | 221 | 66.4 |
| Age (years) | ||
| < 16 | 1 | 0.3 |
| 16–25 | 86 | 25.8 |
| 26–35 | 82 | 24.6 |
| 36–45 | 69 | 20.7 |
| 46–55 | 66 | 19.8 |
| > 55 | 29 | 8.7 |
| Education | ||
| High school and below | 80 | 24 |
| College | 73 | 21.9 |
| Bachelor | 110 | 33 |
| Master and above | 70 | 21 |
| City | ||
| First tier | 112 | 33.6 |
| Second tier | 113 | 33.9 |
| Others | 108 | 32.4 |
| Prior Internet Experience (years) | ||
| < 1 | 14 | 4.2 |
| 1–2 | 17 | 5.1 |
| 2–3 | 32 | 9.6 |
| 3–4 | 132 | 39.6 |
| 4–5 | 5 | 1.5 |
| > 5 | 133 | 39.9 |
| Tenure (years) | ||
| < 1 | 139 | 41.7 |
| 1–2 | 106 | 31.8 |
| 2–3 | 44 | 13.2 |
| 3–4 | 24 | 7.2 |
| 4–5 | 3 | 0.9 |
| > 5 | 17 | 5.1 |
| Constructs | Items | HKS | SIT | EHL |
|---|---|---|---|---|
| Health knowledge seeking | I often use this online health community (OHC) to seek knowledge | 0.817 | 0.140 | 0.145 |
| I frequently use this OHC to seek knowledge | 0.873 | 0.252 | 0.152 | |
| I spend a lot of time using this OHC to seek knowledge | 0.773 | 0.319 | 0.071 | |
| Social interaction ties | I maintain close social relationships with some members in this OHC | 0.277 | 0.844 | 0.055 |
| I spend a lot of time interacting with some members in this OHC | 0.295 | 0.840 | 0.091 | |
| I know some members in this OHC on a personal level | 0.179 | 0.879 | 0.118 | |
| I have frequent communication with some members in this OHC | 0.130 | 0.926 | 0.109 | |
| E-health literacy | I know how to find helpful health resources on the Internet | 0.179 | 0.010 | 0.795 |
| I know how to use the Internet to answer my health questions | 0.181 | 0.023 | 0.841 | |
| I know what health resources are available on the Internet | 0.183 | 0.036 | 0.852 | |
| I know where to find helpful health resources on the Internet | 0.177 | 0.102 | 0.831 | |
| I know how to use the health information I find on the Internet to help me | 0.158 | 0.139 | 0.825 | |
| I have the skills I need to evaluate the health resources I find on the Internet | 0.067 | 0.169 | 0.780 | |
| I can tell high-quality from low-quality health resources on the Internet | 0.044 | 0.157 | 0.781 | |
| I feel confident in using information from the Internet to make health decisions | 0.101 | 0.201 | 0.768 | |
| Cronbach’s α | 0.835 | 0.928 | 0.933 | |
| C.R. | 0.825 | 0.929 | 0.931 | |
| AVE | 0.662 | 0.767 | 0.630 |
| Variables | Mean | SD | Gender | Age | Edu. | City | Tenure | PIE | HKS | SIT | EHL |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | 1.660 | 0.473 | - | ||||||||
| Age | 3.600 | 1.303 | -0.018 | - | |||||||
| Edu. | 2.510 | 1.074 | −0.242 ** | −0.282 ** | - | ||||||
| City | 2.010 | 0.814 | −0.060 | −0.027 | 0.368 ** | - | |||||
| Tenure | 4.490 | 1.435 | −0.149 ** | 0.098 | 0.023 | −0.038 | - | ||||
| PIE | 2.090 | 1.316 | −0.289 ** | −0.333 ** | 0.553 ** | 0.235 ** | 0.280 ** | - | |||
| HKS | 3.382 | 0.945 | 0.084 | 0.250 ** | −0.250 ** | −0.337 ** | −0.084 | -0.154 ** | 0.813 | ||
| SIT | 2.728 | 1.020 | 0.038 | 0.204 ** | −0.335 ** | −0.305 ** | 0.001 | −0.236 ** | 0.502 ** | 0.876 | |
| EHL | 3.705 | 0.761 | 0.011 | 0.081 | −0.030 | −0.055 | −0.033 | 0.007 | 0.328 ** | 0.261 ** | 0.793 |
| Indices | χ2 | df | χ2/df | GFI | AGFI | NFI | CFI | RMSEA |
|---|---|---|---|---|---|---|---|---|
| Results | 229.840 | 84 | 2.736 | 0.915 | 0.878 | 0.943 | 0.963 | 0.072 |
| Criteria | - | - | < 3 | > 0.9 | > 0.8 | > 0.9 | > 0.9 | < 0.08 |
| Model 1 | Model 2 | Model 3 | VIF | ||||
|---|---|---|---|---|---|---|---|
| β | T Value | β | T Value | β | T Value | ||
| Control variables | |||||||
| Gender | 0.002 ns | 0.034 | 0.012 ns | 0.212 | 0.002 ns | 0.041 | 1.143 |
| Age | 0.078 ns | 1.273 | 0.018 ns | 0.302 | 0.034 ns | 0.590 | 1.269 |
| Edu. | 0.001 ns | 0.017 | 0.046 ns | 0.675 | 0.041 ns | 0.609 | 1.706 |
| City | 0.013 ns | 0.213 | 0.056 ns | 0.993 | 0.061 ns | 1.087 | 1.204 |
| Tenure | −0.034 ns | −0.564 | −0.028 ns | −0.496 | −0.017 ns | −0.308 | 1.183 |
| PIE | −0.023 ns | −0.305 | 0.069 ns | 0.969 | 0.058 ns | 0.820 | 1.884 |
| Main variables | |||||||
| HKS | 0.280 *** | 4.525 | 0.288 *** | 4.697 | 1.438 | ||
| SIT | 0.166 ** | 2.649 | 0.148 * | 2.380 | 1.475 | ||
| Interaction variables | |||||||
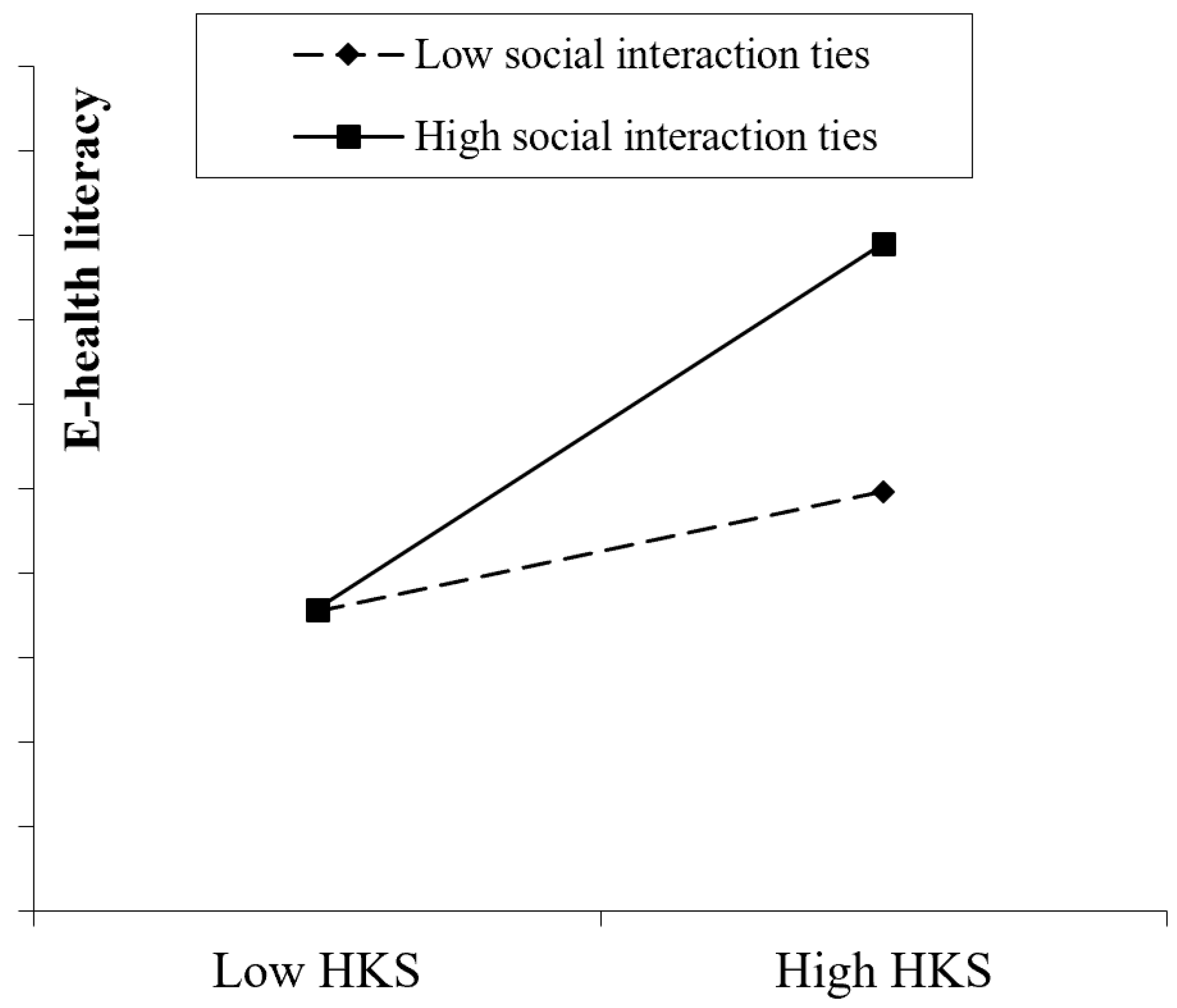
| SIT × HKS | 0.146 ** | 2.787 | 1.041 | ||||
| R2 | 0.009 | 0.133 | 0.153 | ||||
| Adjusted R2 | −0.009 | 0.111 | 0.130 | ||||
| △R2 | 0.009 | 0.124 | 0.020 | ||||
| F (df) | 0.479 (6) ns | 6.206 (8) *** | 6.495 (9) *** | ||||
| △F | 0.479 ns | 23.192 *** | 7.769 ** | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, J.; Fan, T. Understanding the Factors Influencing Patient E-Health Literacy in Online Health Communities (OHCs): A Social Cognitive Theory Perspective. Int. J. Environ. Res. Public Health 2019, 16, 2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142455
Zhou J, Fan T. Understanding the Factors Influencing Patient E-Health Literacy in Online Health Communities (OHCs): A Social Cognitive Theory Perspective. International Journal of Environmental Research and Public Health. 2019; 16(14):2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142455
Chicago/Turabian StyleZhou, Junjie, and Tingting Fan. 2019. "Understanding the Factors Influencing Patient E-Health Literacy in Online Health Communities (OHCs): A Social Cognitive Theory Perspective" International Journal of Environmental Research and Public Health 16, no. 14: 2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142455