Enablers and Barriers to the Utilization of Antenatal Care Services in India

 , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Outcome Variable
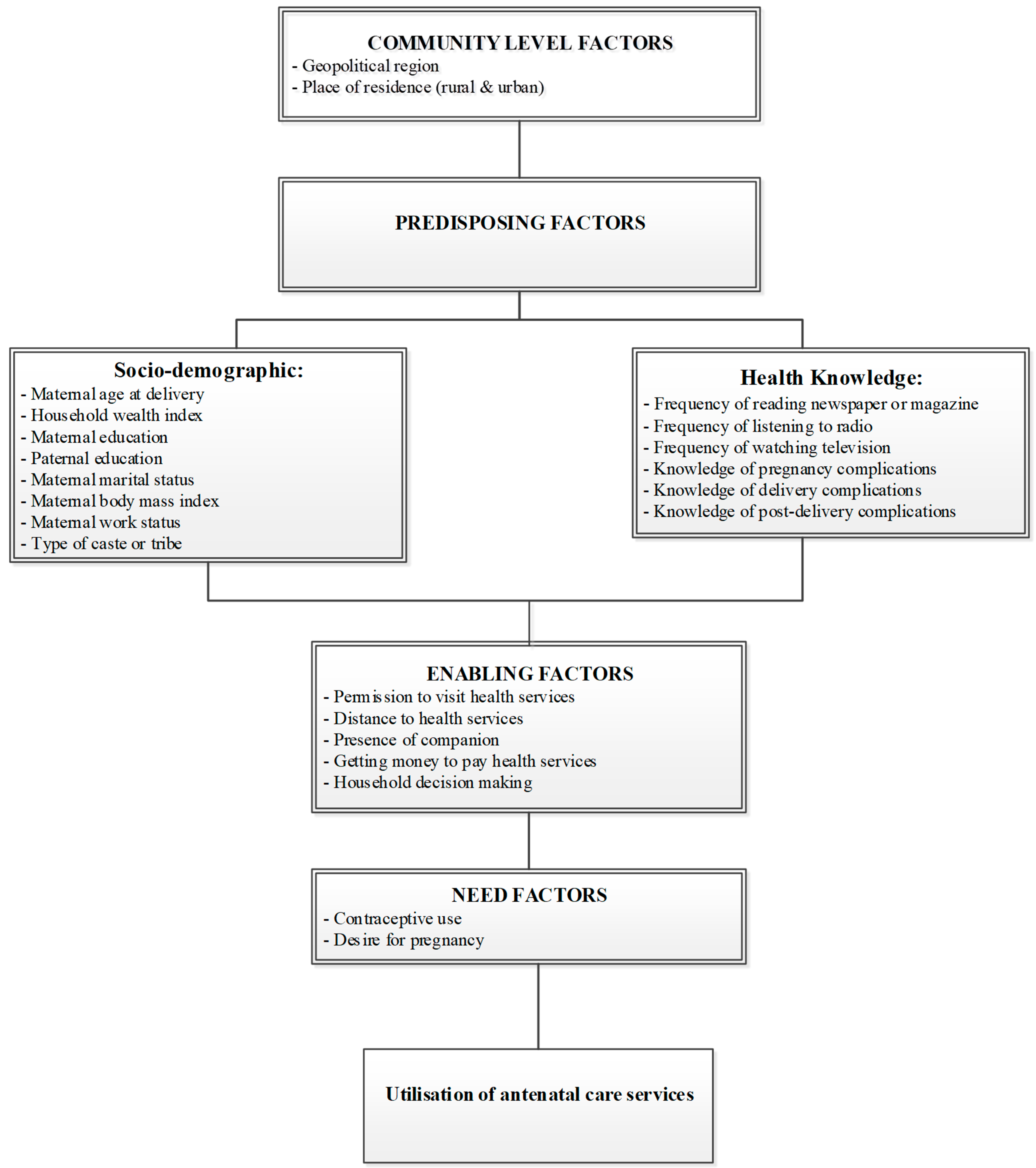
2.3. Study Factors
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Distribution of ANC Service Use by Study Factors
3.2. Factors Associated with ANC Use (1–3 Visits)
3.3. Factors Associated with ANC Use (≥4 Visits)
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Maternal mortality Online: World Health Organisation. 2019. Available online: https://www.who.int/en/news-room/fact-sheets/detail/maternal-mortality (accessed on 20 August 2019).
- World Health Organization. Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Downe, S.; Finlayson, K.; Tuncalp, Ö.; Metin Gülmezoglu, A. What matters to women: A systematic scoping review to identify the processes and outcomes of antenatal care provision that are important to healthy pregnant women. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Barber, R.M.; Bhutta, Z.A.; Dandona, L.; Gething, P.W.; Hay, S.I.; Lopez, A.D. Global, regional, and national levels of maternal mortality, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1775–1812. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Jassir, F.B.; Say, L.; Chou, D.; Mathers, C.; Lawn, J.E. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: A systematic analysis. Lancet Glob. Health 2016, 4, e98–e108. [Google Scholar] [CrossRef]
- International Institute for Population Sciences (IIPS). National Family Health Survey (NFHS-3), 2005–2006; International Institute for Population Sciences: Mumbai, India, 2007. [Google Scholar]
- International Institute for Population Sciences (IIPS). National Family Health Survey (NFHS-4), India; International Institute for Population Sciences: Mumbai, India, 2017. [Google Scholar]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.B.; Daniels, J.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Wang, H.; Bhutta, Z.A.; Coates, M.M.; Coggeshall, M.; Dandona, L.; Diallo, K.; Hay, S.I. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1725–1774. [Google Scholar] [CrossRef]
- Munuswamy, S.; Nakamura, K.; Seino, K.; Kizuki, M. Inequalities in Use of Antenatal Care and Its Service Components in India. J. Rural Med. 2014, 9, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.K.; Rai, R.K.; Alagarajan, M.; Singh, L. Determinants of maternity care services utilization among married adolescents in rural India. PLoS ONE 2012, 7, e31666. [Google Scholar] [CrossRef]
- Ram, F.; Singh, A. Is antenatal care effective in improving maternal health in rural Uttar Pradesh? Evidence from a district level household survey. J. Biosoc. Sci. 2006, 38, 433–448. [Google Scholar] [CrossRef]
- Mumbare, S.S.; Rege, R. Antenatal care services utilization, delivery practices and factors affecting them in tribal area of North Maharashtra. Indian J. Community Med. 2011, 36, 287. [Google Scholar] [CrossRef]
- Dandona, L.; Dandona, R.; Kumar, G.A.; Shukla, D.K.; Paul, V.K.; Balakrishnan, K.; Nandakumar, A. Nations within a nation: Variations in epidemiological transition across the states of India, 1990–2016 in the Global Burden of Disease Study. Lancet 2017, 390, 2437–2460. [Google Scholar] [CrossRef]
- Luke, N.; Munshi, K. Women as agents of change: Female income and mobility in India. J. Dev. Econ. 2011, 94, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Parmentier, M.J.C. The persistence of traditional gender roles in the information technology sector: A study of female engineers in India. Inf. Technol. Int. Dev. 2005, 2, 29–46. [Google Scholar] [CrossRef]
- Taneja, G.; Sridhar, V.S.R.; Mohanty, J.S.; Joshi, A.; Bhushan, P.; Jain, M.; Gera, R. India’s RMNCH+ A Strategy: Approach, learnings and limitations. BMJ Glob. Health 2019, 4, e001162. [Google Scholar] [CrossRef] [PubMed]
- Agho, K.E.; Ezeh, O.K.; Ogbo, F.A.; Enoma, A.I.; Raynes-Greenow, C. Factors associated with inadequate receipt of components and use of antenatal care services in Nigeria: A population-based study. Int. Health 2018, 10, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Ogbo, F.A.; Dhami, M.V.; Awosemo, A.O.; Olusanya, B.O.; Olusanya, J.; Osuagwu, U.L.; Agho, K.E. Regional prevalence and determinants of exclusive breastfeeding in India. Int. Breastfeed. J. 2019, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Senanayake, P.; O’Connor, E.; Ogbo, F.A. National and rural-urban prevalence and determinants of early initiation of breastfeeding in India. BMC Pub. Health 2019, 19, 896. [Google Scholar] [CrossRef] [PubMed]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Ugboma, Z.; Agho, K.E. Stunting and severe stunting among infants in India: The role of delayed introduction of complementary foods and community and household factors. Glob. Health Act. 2019, 12, 1638020. [Google Scholar] [CrossRef] [PubMed]
- Ogbo, F.A.; Ogeleka, P.; Awosemo, A.O. Trends and determinants of complementary feeding practices in Tanzania, 2004–2016. Trop. Med. Health 2018, 46, 40. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Dahiru, T.; Oche, O.M. Determinants of antenatal care, institutional delivery and postnatal care services utilization in Nigeria. Pan. Afr. Med. J. 2015, 21, 321. [Google Scholar] [CrossRef]
- Adewuyi, E.O.; Auta, A.; Khanal, V.; Bamidele, O.D.; Akuoko, C.P.; Adefemi, K.; Zhao, Y. Prevalence and factors associated with underutilization of antenatal care services in Nigeria: A comparative study of rural and urban residences based on the 2013 Nigeria demographic and health survey. PLoS ONE 2018, 13, e0197324. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, T.; Dune, T.; Perz, J.; Ogbo, F.A. Trends and Determinants of Antenatal Care Service Use in Ethiopia between 2000 and 2016. Int. J. Environ. Res. Pub. Health 2019, 16, 748. [Google Scholar] [CrossRef] [PubMed]
- Revankar, R.G. The Indian Constitution: A Case Study of Backward Classes; Fairleigh Dickinson Univ Press: Madison, NJ, USA, 1971. [Google Scholar]
- Yadav, N. Other backward classes: Then and now. Econ. Political Wkl. 2002, 37, 4495–4500. [Google Scholar]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Agho, K.E. Prevalence and factors associated with complementary feeding practices among children aged 6–23 months in India: A regional analysis. BMC Pub. Health 2019, 1, 1034. [Google Scholar] [CrossRef] [PubMed]
- Pathak, P.K.; Singh, A.; Subramanian, S.V. Economic inequalities in maternal health care: Prenatal care and skilled birth attendance in India, 1992–2006. PLoS ONE 2010, 5, e13593. [Google Scholar] [CrossRef] [PubMed]
- Rani, M.; Bonu, S.; Harvey, S. Differentials in the quality of antenatal care in India. Int. J. Qual. Health Care 2008, 20, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Banke-Thomas, O.E.; Banke-Thomas, A.O.; Ameh, C.A. Factors influencing utilisation of maternal health services by adolescent mothers in Low-and middle-income countries: A systematic review. BMC Pregnancy Childbirth 2017, 17, 65. [Google Scholar] [CrossRef]
- Simkhada, B.; Teijlingen, E.R.; Porter, M.; Simkhada, P. Factors affecting the utilization of antenatal care in developing countries: Systematic review of the literature. J. Adv. Nurs. 2008, 61, 244–260. [Google Scholar] [CrossRef]
- Singh, A.; Kumar, A.; Pranjali, P. Utilization of maternal healthcare among adolescent mothers in urban India: Evidence from DLHS-3. PeerJ 2014, 2, e592. [Google Scholar] [CrossRef]
- Zuhair, M.; Roy, R.B. Socioeconomic determinants of the utilization of antenatal care and child vaccination in India. Asia Pac. J. Pub. Health 2017, 29, 649–659. [Google Scholar] [CrossRef]
- Agha, S.; Williams, E. Quality of antenatal care and household wealth as determinants of institutional delivery in Pakistan: Results of a cross-sectional household survey. Reprod. Health 2016, 13, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magadi, M.A.; Madise, N.J.; Rodrigues, R.N. Frequency and timing of antenatal care in Kenya: Explaining the variations between women of different communities. Soc. Sci. Med. 2000, 51, 551–561. [Google Scholar] [CrossRef]
- Griffiths, P.; Stephenson, R. Understanding users’ perspectives of barriers to maternal health care use in Maharashtra, India. J. Biosoc. Sci. 2001, 33, 339–359. [Google Scholar] [CrossRef] [PubMed]
- Ponna, S.N.; Upadrasta, V.P.; Babu Geddam, J.J.; Dudala, S.R.; Sadasivuni, R.; Bathina, H. Regional variation in utilization of Antenatal care services in the state of Andhra Pradesh. J. Fam. Med. Prim. Care 2017, 6, 231–239. [Google Scholar] [CrossRef]
- Elmusharaf, K.; Byrne, E.; O’Donovan, D. Strategies to increase demand for maternal health services in resource-limited settings: Challenges to be addressed. BMC Pub. Health 2015, 15, 870. [Google Scholar] [CrossRef]
- Lim, S.S.; Dandona, L.; Hoisington, J.A.; James, S.L.; Hogan, M.C.; Gakidou, E. India’s Janani Suraksha Yojana, a conditional cash transfer programme to increase births in health facilities: An impact evaluation. Lancet 2010, 375, 2009–2023. [Google Scholar] [CrossRef]
- Goli, S.; Moradhvaj Rammohan, A.; Shruti Pradhan, J. High Spending on Maternity Care in India: What Are the Factors Explaining It? PLoS ONE 2016, 11, e0156437. [Google Scholar] [CrossRef]
- Government of India. The pradhan mantri surakshit matritva abhiyan. In Ministry of Health and Family Welfare—Maternal Health Division; Ministry of Health and Family Welfare: New Delhi, India, 2016. [Google Scholar]
- Ministry of Women and Child Development. Pradhan Mantri Matru Vandana Yojana Online: Ministry of Women and Child Development. 2019. Available online: http://www.wcd.nic.in/schemes/pradhan-mantri-matru-vandana-yojana (accessed on 20 January 2019).
- Titaley, C.R.; Dibley, M.J.; Roberts, C.L. Factors associated with underutilization of antenatal care services in Indonesia: Results of Indonesia Demographic and Health Survey 2002/2003 and 2007. BMC Pub. Health 2010, 10, 485. [Google Scholar] [CrossRef]
- Rahman, A.; Nisha, M.K.; Begum, T.; Ahmed, S.; Alam, N.; Anwar, I. Trends, determinants and inequities of 4+ ANC utilisation in Bangladesh. J. Health Popul. Nutr. 2017, 36, 2. [Google Scholar] [CrossRef]
- Celik, Y.; Hotchkiss, D.R. The socio-economic determinants of maternal health care utilization in Turkey. Soc. Sci. Med. 2000, 50, 1797–1806. [Google Scholar] [CrossRef]
- United Nations. Sustainable Development Goals Online: United Nations. 2016. Available online: http://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed on 28 July 2018).
- Sunita Kishor, K.G. Gender Equality and Women’s Empowerment in India; International Institute for Population Sciences: Mumbai, India, 2009; p. 132. [Google Scholar]
- King-Schultz, L.; Jones-Webb, R. Multi-method approach to evaluate inequities in prenatal care access in Haiti. J. Health Care Poor Underserved 2008, 19, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Titaley, C.R.; Hunter, C.L.; Heywood, P.; Dibley, M.J. Why don’t some women attend antenatal and postnatal care services? A qualitative study of community members’ perspectives in Garut, Sukabumi and Ciamis districts of West Java Province, Indonesia. BMC Pregnancy Childbirth 2010, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Gabrysch, S.; Campbell, O.M. Still too far to walk: Literature review of the determinants of delivery service use. BMC Pregnancy Childbirth 2009, 9, 34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Antenatal Care (ANC) Visits | No ANC Visits | ANC (1–3) Visits | ANC (≥4) Visits | |||
|---|---|---|---|---|---|---|
| Variable | n * | PR (95% CI) | n * | PR (95% CI) | n * | PR (95% CI) |
| Outcomes | 30,449 | 16.6 (16.3–17.0) | 58,082 | 31.7 (31.3–32.2) | 94,560 | 51.7 (51.1–52.2) |
| Community-level factors | ||||||
| Residence type | ||||||
| Urban | 5074 | 16.6 (15.5–17.8) | 12,799 | 22.0 (21.0–23.1) | 36,410 | 38.5 (37.3–39.6) |
| Rural | 25,375 | 83.3 (82.1–84.4) | 45,283 | 77.9 (76.9–78.9) | 58,150 | 61.5 (60.3–62.6) |
| Geopolitical region | ||||||
| North | 2705 | 8.9 (8.2–9.5) | 8254 | 14.2 (13.7–14.7) | 11,765 | 12.4 (12.0–12.9) |
| South | 1977 | 6.5 (5.7–7.3) | 5255 | 9.0 (8.4–9.7) | 26,886 | 28.4 (27.7–29.1) |
| East | 11,994 | 39.3 (38.1–40.6) | 15,102 | 26.0 (25.3–26.6) | 19,518 | 20.6 (19.9–21.3) |
| West | 2337 | 7.7 (6.9–8.4) | 4334 | 7.4 (6.7–8.2) | 17,390 | 18.3 (17.6–19.1) |
| Central | 10,532 | 34.6 (33.4–35.7) | 22,475 | 38.7 (37.9–39.4) | 15,540 | 16.4 (15.9–16.8) |
| Northeast | 904 | 2.9 (2.7–3.2) | 2661 | 4.5 (4.3–4.8) | 3461 | 3.6 (3.5–3.8) |
| Socio-demographic factors | ||||||
| Household wealth index | ||||||
| Poor | 22,029 | 72.3 (71.3–73.3) | 31,517 | 54.2 (53.4–55.0) | 28,107 | 29.7 (29.0–30.4) |
| Middle | 4136 | 13.5 (13.0–14.1) | 11,295 | 19.4 (18.9–19.9) | 21,004 | 22.2 (21.7–22.7) |
| Rich | 4284 | 14.0 (13.2–14.9) | 15,270 | 26.2 (25.5–27.0) | 45,449 | 48.0 (47.2–48.8) |
| Mother’s education | ||||||
| No education | 16,481 | 54.1 (53.1–55.0) | 19,914 | 34.2 (33.6–34.9) | 14,276 | 15.1 (14.6–15.5) |
| Primary | 4299 | 14.1 (13.6–14.6) | 9081 | 15.6 (15.2–16.0) | 11,271 | 11.9 (11.5–12.2) |
| Secondary or higher | 9669 | 31.7 (30.8–32.7) | 29,087 | 50.0 (49.3–50.7) | 69,014 | 72.9 (72.4–73.5) |
| Mother’s working status | ||||||
| Did not work | 3971 | 13.0 (12.3–13.7) | 7920 | 13.6 (13.1–14.1) | 14,756 | 15.6 (15.0–16.1) |
| Worked | 913 | 2.9 (2.7–3.2) | 1569 | 2.7 (2.5–2.9) | 2728 | 2.8 (2.6–3.0) |
| Mother’s age | ||||||
| 15–19 years | 927 | 3.0 (2.7–3.3) | 1910 | 3.2 (3.1–3.4) | 3402 | 3.5 (3.3–3.8) |
| 20–34 years | 24,677 | 81.0 (80.4–81.6) | 50,646 | 87.2 (86.8–87.5) | 84,389 | 89.2 (88.9–89.5) |
| 35–49 years | 4845 | 15.9 (15.3–16.4) | 5526 | 9.5 (9.2–9.8) | 6769 | 7.1 (6.8–7.4) |
| Maternal BMI kg/m2 | ||||||
| ≤18 | 6616 | 21.7 (21.1–22.3) | 11,793 | 20.3 (19.8–20.7) | 14,948 | 15.8 (15.4–16.2) |
| 19–24 | 20,543 | 67.4 (66.7–68.1) | 38,719 | 66.6 (66.1–67.1) | 58,416 | 61.7 (61.2–62.3) |
| ≥25 | 2745 | 9.0 (8.5–9.5) | 6758 | 11.6 (11.2–12.0) | 19,093 | 20.1 (19.7–20.6) |
| Type of caste or tribe | ||||||
| Scheduled caste | 6988 | 22.9 (22.1–23.8) | 12,820 | 22.0 (21.4–22.6) | 19,030 | 20.1 (19.5–20.7) |
| Scheduled tribe | 3750 | 12.3 (11.6–12.9) | 6342 | 10.9 (10.4–11.4) | 8669 | 9.1 (8.7–9.5) |
| Other backward class | 14,243 | 46.7 (45.7–47.8) | 26,788 | 46.1 (45.3–46.9) | 38,831 | 41.0 (40.3–41.7) |
| Others # | 5468 | 17.9 (17.1–18.8) | 12,132 | 20.8 (20.2–21.6) | 28,030 | 29.6 (28.9–30.3) |
| Marital status | ||||||
| Currently married | 29,926 | 98.2 (98.0–98.4) | 57,365 | 98.7 (98.6–98.8) | 93,289 | 98.6 (98.5–98.7) |
| Formerly married (divorced/separated/widowed) | 465 | 1.5 (1.3–1.7) | 670 | 1.1 (1.0–1.2) | 1194 | 1.2 (1.1–1.3) |
| Partner education | ||||||
| No education | 1614 | 5.3 (4.9–5.7) | 1852 | 3.1 (2.9–3.4) | 1776 | 1.8 (1.7–2.0) |
| Primary | 2950 | 9.6 (9.1–10.2) | 6515 | 11.2 (10.7–11.6) | 12,192 | 12.8 (12.4–13.3) |
| Secondary or higher | 299 | 0.9 (0.8–1.1) | 1089 | 1.8 (1.7–2.0) | 3471 | 3.6 (3.4–3.9) |
| Religion | ||||||
| Hindu | 23,825 | 78.2 (77.1–79.2) | 46,598 | 80.2 (79.4–80.9) | 74,029 | 78.2 (77.5–79.0) |
| Muslim | 5679 | 18.6 (17.6–19.6) | 9233 | 15.9 (15.1–16.6) | 14,511 | 15.3 (14.6–16.0) |
| Christian and others | 945 | 3.1 (2.7–3.5) | 2250 | 3.8 (3.6–4.1) | 6020 | 6.3 (5.9–6.7) |
| Health knowledge factors | ||||||
| Reads newspaper or magazine | ||||||
| Not all | 25,657 | 84.2 (83.5–84.9) | 41,835 | 72.0 (71.2–72.7) | 51,812 | 54.7 (54.1–55.4) |
| Yes | 4792 | 15.7 (15.0–16.4) | 16,246 | 27.9 (27.2–28.7) | 42,749 | 45.2 (44.5–45.8) |
| Listens to radio | ||||||
| Not all | 26,365 | 86.5 (85.9–87.2) | 50,716 | 87.3 (86.7–87.8) | 80,818 | 85.4 (85.0–85.9) |
| Yes | 4084 | 13.4 (12.7–14.0) | 7366 | 12.6 (12.1–13.2) | 13,742 | 14.5 (14.0–14.9) |
| Watches television | ||||||
| Not all | 17,496 | 57.4 (56.4–58.4) | 21,168 | 36.4 (35.7–37.1) | 13,841 | 14.6 (14.2–15.0) |
| Yes | 12,953 | 42.5 (41.5–43.5) | 36,914 | 63.5 (62.8–64.2) | 80,719 | 85.3 (84.9–85.7) |
| Told about delivery complications | ||||||
| Any complications | 0 | 0 | 30,726 | 52.9 (52.1–53.6) | 66,918 | 70.7 (70.1–71.3) |
| None | 30,449 | 100 | 27,356 | 47.1 (46.3–47.8) | 27,642 | 29.2 (28.6–29.8) |
| Knowledge of post-delivery complications | ||||||
| Yes | 4911 | 16.1 (15.4–16.8) | 20,235 | 34.8 (34.1–35.5) | 42,506 | 44.9 (44.2–45.6) |
| None | 25,537 | 83.8 (83.1–84.5) | 37,847 | 65.1 (64.4–65.8) | 52,054 | 55.0 (54.3–55.7) |
| Enabling factors | ||||||
| Household decision making | ||||||
| Mother involved | 3621 | 11.8 (11.2–12.5) | 7566 | 13.0 (12.5–13.5) | 14,721 | 15.5 (15.0–16.1) |
| Mother not involved | 26,828 | 88.1 (87.4–88.7) | 50,516 | 86.9 (86.4–87.4) | 79,839 | 84.4 (83.8–84.9) |
| Seek permission to visit health services | ||||||
| No problem | 13,533 | 44.4 (43.4–45.4) | 31,658 | 54.5 (53.7–55.2) | 58,785 | 62.1 (61.4–62.8) |
| Big problem | 9207 | 30.2 (29.3–31.2) | 12,447 | 21.4 (20.8–22.0) | 14,468 | 15.3 (14.8–15.8) |
| Not a big problem | 7709 | 25.3 (24.5–26.1) | 13,977 | 24.0 (23.4–24.7) | 21,307 | 22.5 (21.9–23.1) |
| Getting money to pay health services | ||||||
| No problem | 9186 | 30.1 (29.2–31.0) | 23,053 | 39.6 (38.9–40.4) | 45,309 | 47.9 (47.1–48.6) |
| Big problem | 11,842 | 38.8 (37.9–39.8) | 16,742 | 28.8 (28.1–29.4) | 21,002 | 22.2 (21.6–22.8) |
| Not a big problem | 9421 | 30.9 (30.1–31.7) | 18,287 | 31.4 (30.8–32.1) | 28,249 | 29.8 (29.2–30.4) |
| Distance to health facility | ||||||
| No problem | 6485 | 21.3 (20.4–22.1) | 16,546 | 28.4 (27.8–29.1) | 38,332 | 40.5 (39.8–41.2) |
| Big problem | 13,823 | 45.4 (44.3–46.4) | 20,906 | 35.9 (35.2–36.7) | 24,232 | 25.6 (25.0–26.2) |
| Not a big problem | 10,141 | 33.3 (32.4–34.1) | 20,629 | 35.5 (34.9–36.1) | 31,996 | 33.8 (33.2–34.4) |
| Accompany to health facility | ||||||
| No problem | 9796 | 32.1 (31.2–33.1) | 23,339 | 40.1 (39.5–40.8) | 49,195 | 52.0 (51.3–52.7) |
| Big problem | 10,163 | 33.3 (32.4–34.3) | 14,285 | 24.5 (23.9–25.2) | 15,511 | 16.4 (15.9–16.8) |
| Not a big problem | 10,490 | 34.4 (33.6–35.3) | 20,458 | 35.2 (34.5–35.8) | 29,854 | 31.5 (30.9–32.1) |
| Need factors | ||||||
| Contraceptive use | ||||||
| Yes | 8264 | 27.1 (26.3–27.9) | 23,147 | 39.8 (39.2–40.4) | 46,599 | 49.2 (48.6–49.8) |
| No | 22,179 | 72.8 (72.0–73.6) | 34,926 | 60.1 (59.5–60.7) | 47,942 | 50.7 (50.1–51.3) |
| Wanted pregnancy at the time | ||||||
| Then | 25,844 | 84.8 (84.2–85.5) | 52,189 | 89.8 (89.5–90.2) | 88,139 | 93.2 (92.9–93.4) |
| Later | 1280 | 4.2 (3.8–4.5) | 2631 | 4.5 (4.3–4.7) | 3582 | 3.7 (3.5–3.9) |
| No more | 3223 | 10.5 (10.0–11.1) | 3261 | 5.6 (5.3–5.8) | 2839 | 3.0 (2.8–3.1) |
| Study Factors | Antenatal Care (1–3) Visits | Antenatal Care (≥4) Visits | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| COR | (95% CI) | p Value | aOR | (95% CI) | p Value | COR | (95% CI) | p Value | aOR | (95% CI) | p Value | |
| Community-level factors | ||||||||||||
| Geopolitical region | ||||||||||||
| North | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| South | 0.80 | 0.74–1.02 | 0.097 | 0.72 | 0.54–0.97 | 0.035 | 3.12 | 2.68–3.65 | p < 0.001 | 2.41 | 1.83–3.16 | p < 0.001 |
| East | 0.41 | 0.37–0.45 | p < 0.001 | 0.47 | 0.39–0.56 | p < 0.001 | 0.37 | 0.33–0.41 | p < 0.001 | 0.40 | 0.33–0.48 | p < 0.001 |
| West | 0.60 | 0.51–0.71 | p < 0.001 | 0.49 | 0.37–0.65 | p < 0.001 | 1.71 | 1.49–1.95 | p < 0.001 | 1.13 | 0.87–1.47 | 0.324 |
| Central | 0.69 | 0.63–0.76 | p < 0.001 | 0.76 | 0.64–0.91 | 0.003 | 0.34 | 0.30–0.37 | p < 0.001 | 0.36 | 0.30–0.44 | p < 0.001 |
| North East | 0.96 | 0.85–1.09 | 0.568 | 1.08 | 0.84–1.39 | 0.506 | 0.88 | 0.77–1.00 | 0.057 | 0.78 | 0.60–1.01 | 0.068 |
| Socio-demographic factors | ||||||||||||
| Household wealth index | ||||||||||||
| Poor | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Middle | 1.90 | 1.80–2.02 | p < 0.001 | 1.28 | 1.11–1.48 | 0.001 | 3.98 | 3.74–4.22 | p < 0.001 | 1.86 | 1.61–2.15 | p < 0.001 |
| Rich | 2.49 | 2.30–2.68 | P < 0.001 | 1.56 | 1.29–1.88 | p < 0.001 | 8.31 | 7.71–8.96 | p < 0.001 | 2.99 | 2.47–3.62 | p < 0.001 |
| Mother education | ||||||||||||
| No education | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Primary | 1.74 | 1.65–1.84 | p < 0.001 | 1.48 | 1.29–1.70 | p < 0.001 | 3.02 | 2.85–3.21 | p < 0.001 | 2.03 | 1.75–2.36 | p < 0.001 |
| Secondary and higher | 2.49 | 2.36–2.61 | p < 0.001 | 1.77 | 1.57–2.00 | p < 0.001 | 8.24 | 7.81–8.69 | p < 0.001 | 3.42 | 3.01–3.87 | p < 0.001 |
| Type of caste or tribe | ||||||||||||
| Scheduled caste | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Scheduled tribe | 0.92 | 0.85–0.99 | 0.039 | 1.16 | 0.98–1.38 | 0.071 | 0.84 | 0.78–0.92 | p < 0.001 | 1.28 | 1.05–1.54 | 0.110 |
| Other backward class | 1.02 | 0.96–1.08 | 0.381 | 1.03 | 0.91–1.17 | 0.556 | 1.00 | 0.94–1.06 | 0.970 | 0.88 | 0.77–1.00 | 0.058 |
| Others | 1.20 | 1.12–1.30 | p < 0.001 | 1.18 | 0.99–1.40 | 0.055 | 1.88 | 1.74–2.03 | p < 0.001 | 1.60 | 1.34–1.91 | p < 0.001 |
| Partner education | ||||||||||||
| No education | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Primary | 1.92 | 1.73–2.14 | p < 0.001 | 1.32 | 1.19–1.48 | p < 0.001 | 3.75 | 3.35–4.20 | p < 0.001 | 1.55 | 1.37–1.75 | p < 0.001 |
| Secondary and higher | 3.17 | 2.55–3.95 | p < 0.001 | 1.62 | 1.28–2.04 | p < 0.001 | 10.55 | 8.47–13.13 | p < 0.001 | 2.51 | 1.98–3.18 | p < 0.001 |
| Health knowledge factors | ||||||||||||
| Reads newspaper or magazine | ||||||||||||
| Not all | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Yes | 2.07 | 1.95–2.21 | p < 0.001 | 1.18 | 1.00–1.38 | 0.042 | 4.41 | 4.17–4.67 | p < 0.001 | 1.27 | 1.08–1.50 | 0.003 |
| Listens to radio | ||||||||||||
| Not all | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Yes | 0.93 | 0.87–1.00 | 0.080 | 0.67 | 0.57–0.78 | p < 0.001 | 1.09 | 1.02–1.17 | 0.005 | 0.65 | 0.55–0.77 | p < 0.001 |
| Watches television | ||||||||||||
| Not all | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Yes | 2.35 | 2.24–2.46 | p < 0.001 | 1.42 | 1.27–1.59 | p < 0.001 | 7.87 | 7.47–8.30 | p < 0.001 | 2.56 | 2.26–2.89 | p < 0.001 |
| Enabling factors | ||||||||||||
| Household decision making | ||||||||||||
| Mother involved | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Mother not involved | 0.90 | 0.84–0.96 | 0.002 | 0.84 | 0.74–0.95 | 0.007 | 0.73 | 0.68–0.78 | p < 0.001 | 0.68 | 0.59–0.78 | p < 0.001 |
| Seeking permission to visit health services | ||||||||||||
| No problem | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Big problem | 0.57 | 0.54–0.61 | p < 0.001 | 0.74 | 0.64–0.86 | p < 0.001 | 3.62 | 0.34–0.38 | p < 0.001 | 0.53 | 0.45–0.63 | p < 0.001 |
| Not a big problem | 0.77 | 0.73–0.82 | p < 0.001 | 0.79 | 0.69–0.90 | 0.001 | 0.63 | 0.60–0.67 | p < 0.001 | 0.65 | 0.56–0.76 | p < 0.001 |
| Getting money to pay health services | ||||||||||||
| No problem | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Big problem | 0.56 | 0.53–0.59 | p < 0.001 | 0.99 | 0.84–1.17 | 0.996 | 0.36 | 0.33–0.38 | p < 0.001 | 1.08 | 0.89–1.29 | 0.406 |
| Not a big problem | 0.77 | 0.73–0.81 | p < 0.001 | 0.91 | 0.79–1.05 | 0.223 | 0.60 | 0.57–0.64 | p < 0.001 | 0.90 | 0.78–1.05 | 0.215 |
| Distance to health facility | ||||||||||||
| No problem | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Big problem | 0.59 | 0.55–0.63 | p < 0.001 | 0.99 | 0.85–1.16 | 0.934 | 0.29 | 0.27–0.31 | p < 0.001 | 0.85 | 0.71–1.01 | 0.068 |
| Not a big problem | 0.79 | 0.75–0.84 | p < 0.001 | 0.97 | 0.83–1.14 | 0.779 | 0.53 | 0.50–0.56 | p < 0.001 | 0.91 | 0.76–1.08 | 0.284 |
| Accompanied to health facility | ||||||||||||
| No problem | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Big problem | 0.59 | 0.55–0.62 | p < 0.001 | 0.90 | 0.77–1.06 | 0.222 | 0.30 | 0.28–0.32 | p < 0.001 | 0.78 | 0.65–0.94 | 0.011 |
| Not a big problem | 0.81 | 0.77–0.86 | p < 0.001 | 1.06 | 0.92–1.21 | 0.385 | 0.56 | 0.53–0.59 | p < 0.001 | 0.92 | 0.79–1.06 | 0.279 |
| Need factors | ||||||||||||
| Contraceptive use | ||||||||||||
| Yes | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| No | 0.56 | 0.53–0.58 | p < 0.001 | 0.70 | 0.63–0.78 | p < 0.001 | 0.38 | 0.36–0.40 | p < 0.001 | 0.51 | 0.45–0.57 | p < 0.001 |
| Wanted pregnancy at the time | ||||||||||||
| Then | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Later | 1.01 | 0.92–1.12 | 0.712 | 1.02 | 0.80–1.31 | 0.822 | 0.82 | 0.74–0.90 | p < 0.001 | 0.94 | 0.73–1.21 | 0.655 |
| No more | 0.50 | 0.46–0.53 | p < 0.001 | 0.72 | 0.61–0.87 | 0.001 | 0.25 | 0.23–0.28 | p < 0.001 | 0.51 | 0.41–0.64 | p < 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogbo, F.A.; Dhami, M.V.; Ude, E.M.; Senanayake, P.; Osuagwu, U.L.; Awosemo, A.O.; Ogeleka, P.; Akombi, B.J.; Ezeh, O.K.; Agho, K.E. Enablers and Barriers to the Utilization of Antenatal Care Services in India. Int. J. Environ. Res. Public Health 2019, 16, 3152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173152
Ogbo FA, Dhami MV, Ude EM, Senanayake P, Osuagwu UL, Awosemo AO, Ogeleka P, Akombi BJ, Ezeh OK, Agho KE. Enablers and Barriers to the Utilization of Antenatal Care Services in India. International Journal of Environmental Research and Public Health. 2019; 16(17):3152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173152
Chicago/Turabian StyleOgbo, Felix Akpojene, Mansi Vijaybhai Dhami, Ebere Maureen Ude, Praween Senanayake, Uchechukwu L. Osuagwu, Akorede O. Awosemo, Pascal Ogeleka, Blessing Jaka Akombi, Osita Kingsley Ezeh, and Kingsley E. Agho. 2019. "Enablers and Barriers to the Utilization of Antenatal Care Services in India" International Journal of Environmental Research and Public Health 16, no. 17: 3152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173152