Quality of Care for Patients with Acute Myocardial Infarction (AMI) in Pakistan: A Retrospective Study


Abstract
:1. Introduction
2. Methods
2.1. Data Source and Study Population
2.2. Quality Indicators
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Compliance Measurements
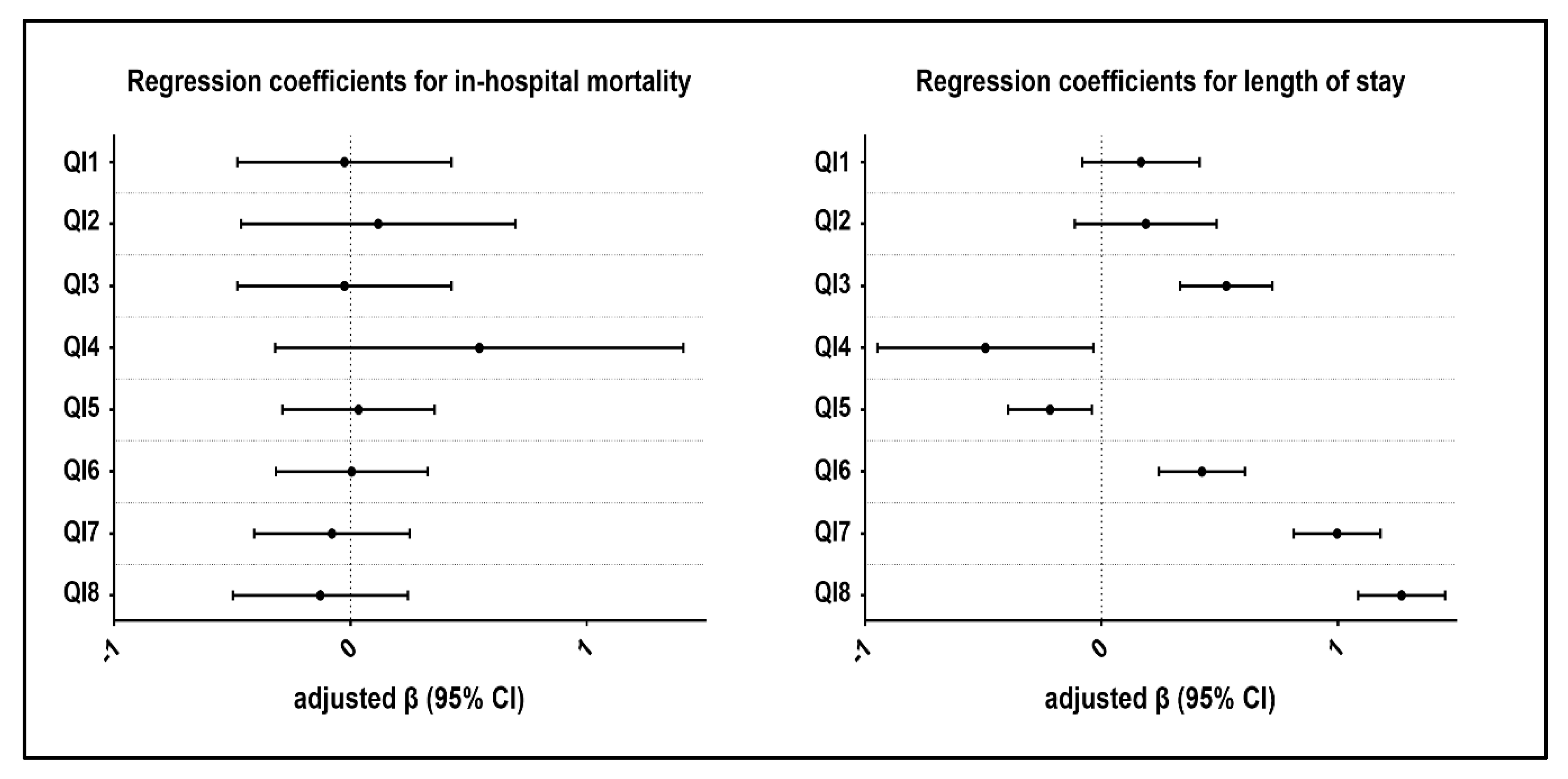
3.3. Association between Process Indicators and Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Califf, R.M.; Peterson, E.D.; Gibbons, R.J.; Garson, A.; Brindis, R.G.; Beller, G.A.; Smith, S.C. Integrating quality into the cycle of therapeutic development. J. Am. Coll. Cardiol. 2002, 40, 1895–1901. [Google Scholar] [CrossRef]
- Schiele, F.; Gale, C.P.; Simon, T.; Fox, K.A.A.; Bueno, H.; Lettino, M.; Tubaro, M.; Puymirat, E.; Ferrières, J.; Meneveau, N.; et al. Assessment of Quality Indicators for Acute Myocardial Infarction in the FAST-MI (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) Registries. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003336. [Google Scholar] [CrossRef] [PubMed]
- Kontos, M.C.; Rennyson, S.L.; Chen, A.Y.; Alexander, K.P.; Peterson, E.D.; Roe, M.T. The association of myocardial infarction process of care measures and in-hospital mortality: A report from the NCDR®. Am. Heart J. 2014, 168, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.D.; Roe, M.T.; Mulgund, J.; DeLong, E.R.; Lytle, B.L.; Brindis, R.G.; Smith, S.C.; Pollack, C.V.; Newby, L.K.; Harrington, R.A.; et al. Association Between Hospital Process Performance and Outcomes Among Patients With Acute Coronary Syndromes. JAMA 2006, 295, 1912. [Google Scholar] [CrossRef] [PubMed]
- Araújo, C.; Laszczyńska, O.; Viana, M.; Dias, P.; Maciel, M.J.; Moreira, I.; Azevedo, A. Quality of Care and 30-day Mortality of Women and Men With Acute Myocardial Infarction. Rev. Esp. Cardiol. 2019, 72, 543–552. [Google Scholar]
- Baldwin, L.M.; MacLehose, R.F.; Hart, L.G.; Beaver, S.K.; Every, N.; Chan, L. Quality of Care for Acute Myocardial Infarction in Rural Urban US Hospitals. J. Rural Health 2004, 20, 99–108. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Anderson, J.L.; Bachelder, B.L.; Fesmire, F.M.; Fihn, S.D.; Foody, J.M.; Ho, P.M.; Kosiborod, M.N.; Masoudi, F.A.; Nallamothu, B.K. ACC/AHA 2008 Performance Measures for Adults With ST-Elevation and Non-ST-Elevation Myocardial Infarction. Circulation 2008, 118, 2596–2648. [Google Scholar] [CrossRef]
- Chew, D.P.; Scott, I.A.; Cullen, L.; French, J.K.; Briffa, T.G.; Tideman, P.A.; Woodruffe, S.; Kerr, A.; Branagan, M.; Aylward, P.E.G. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Med. J. Aust. 2016, 205, 128–133. [Google Scholar] [CrossRef]
- Tu, J.V.; Khalid, L.; Donovan, L.R.; Ko, D.T. Indicators of quality of care for patients with acute myocardial infarction. Cmaj 2008, 179, 909–915. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli−Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC); Steg, P.G.; James, S.K.; Atar, D.; Badano, L.P.; Blömstrom-Lundqvist, C.; Borger, M.A.; Di Mario, C.; Dickstein, K.; Ducrocq, G.; et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2012, 33, 2569–2619. [Google Scholar] [CrossRef] [PubMed]
- Jneid, H.; Addison, D.; Bhatt, D.L.; Fonarow, G.C.; Gokak, S.; Grady, K.L.; Green, L.A.; Heidenreich, P.A.; Ho, P.M.; Jurgens, C.Y.; et al. 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J. Am. Coll. Cardiol. 2017, 70, 2048–2090. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.T.; Welsh, R.C.; Ohinmaa, A.; Thanh, N.X.; Bagai, A.; Kaul, P. Quality of Acute Myocardial Infarction Care in Canada: A 10-Year Review of 30-Day In-Hospital Mortality and 30-Day Hospital Readmission. Can. J. Cardiol. 2017, 33, 1319–1326. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Executive summary: Heart disease and stroke statistics-2016 update: A Report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Khursheed, M.; Fayyaz, J.; Feroze, A.; Shakeel, N.; Bhatti, J.A. Time to treatment in patients of suspected acute coronary syndrome in Pakistan: A clinical audit. Hear. Lung J. Acute Crit. Care 2015, 44, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Jafary, M.H.; Samad, A.; Ishaq, M.; Jawaid, S.A.; Ahmad, M.; Vohra, E.A. Profile of Acute Myocardial Infarction (AMI) in Pakistan. Pakistan J. Med. Sci. 2007, 23, 485–489. [Google Scholar]
- Malik, S.M.; Bhutta, Z.A. Reform of primary health care in Pakistan. Lancet 2018, 392, 1375–1377. [Google Scholar] [CrossRef]
- Kutz, A.; Gut, L.; Ebrahimi, F.; Wagner, U.; Schuetz, P.; Mueller, B. Association of the Swiss Diagnosis-Related Group Reimbursement System With Length of Stay, Mortality, and Readmission Rates in Hospitalized Adult Patients. JAMA Netw. Open 2019, 2, e188332. [Google Scholar] [CrossRef]
- Statistics, P.B. of Pakistan Bureau of Statistics. Available online: http://www.pbs.gov.pk/publications.
- Sun, H.; Liu, M.; Hou, S. Quality indicators for acute myocardial infarction care in China. Int. J. Qual. Health Care 2011, 23, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: Executive summary: A report of the american college of cardiology/american heart association task force on practice guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef]
- Rublee, D.A. The Quality of Care: How Can It Be Assessed? JAMA J. Am. Med. Assoc. 1989, 261, 1151. [Google Scholar] [CrossRef]
- Donabedian, A. Methods for deriving criteria for assessing the quality of medical care. Med. Care Rev. 1980, 37, 653. [Google Scholar] [PubMed]
- Jacobs, R.; Goddard, M.; Smith, P.C. Composite Performance Measures in the Public Sector; Centre for Health Economics, University of York: York, UK, 2007; Volume 16. [Google Scholar]
- Wang, Y.; Fu, R.; Wang, Z.; Bao, H.; Chen, Y.; Yang, F.; Luo, X.; Liu, M. Assessing the Quality of Care for Patients with Acute Myocardial Infarction in China. Clin. Cardiol. 2015, 38, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Jafary, F.H.; Faruqui, A.M.; Rasool, S.I.; Hatcher, J.; Chaturvedi, N.; Jafar, T.H. High prevalence of lack of knowledge of symptoms of acute myocardial infarction inPakistan and its contribution to delayed presentationto the hospital. BMC Public Health 2007, 7, 284. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.J.; Antman, E.M.; Brooks, N.H.; Califf, R.M.; Hillis, L.D.; Hiratzka, L.F.; Rapaport, E.; Riegel, B.; Russell, R.O.; Smith, E.E. 1999 update: ACC/AHA guidelines for the management of patients with acute myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infar. J. Am. Coll. Cardiol. 1999, 34, 890–911. [Google Scholar] [CrossRef]
- Lee, D.S.; Tran, C.; Flintoft, V.; Grant, F.C.; Liu, P.P.; Tu, J.V. Canadian Cardiovascular Outcomes Research Team/Canadian Cardiovascular Society Heart Failure Quality Indicator Panel CCORT/CCS quality indicators for congestive heart failure care. Can. J. Cardiol. 2003, 19, 357–364. [Google Scholar]
- Meghani, S.H.; Buck, H.G.; Dickson, V.V.; Hammer, M.J.; Rabelo−Silva, E.R.; Clark, R.; Naylor, M.D. The Conceptualization and Measurement of Comorbidity: A Review of the Interprofessional Discourse. Nurs. Res. Pract. 2013, 2013, 192782. [Google Scholar] [CrossRef]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- Lu, S.F.; Lu, L.X.; Smith, S.C.; Dai, X. Acute Myocardial Infarction in Patients with Paraplegia: Characteristics, Management, and Outcomes. Am. J. Med. 2018, 131, 574.e1–574.e11. [Google Scholar] [CrossRef]
- Patel, R.S.; Shrestha, S.; Saeed, H.; Raveendranathan, S.; Isidahome, E.E.; Ravat, V.; Fakorede, M.O.; Patel, V. Comorbidities and Consequences in Hospitalized Heart Failure Patients with Depression. Cureus 2018, 10, e3193. [Google Scholar] [CrossRef] [Green Version]
- Mainz, J. Developing evidence-based clinical indicators: a state of the art methods primer. Int. J. Qual. Health Care 2003, 15, i5–i11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Characteristics | Frequency (%) | In-Hospital Mortality | LOS (day) | ||
|---|---|---|---|---|---|
| N (%) | p Value | mean ± SD | p Value | ||
| Age | |||||
| ~50 | 316 (11.87) | 26 (8.23) | 0.8170 | 6.07 ± 3.05 | <0.0001 |
| 50–60 | 414 (15.55) | 32 (7.73) | 7.27 ± 2.50 | ||
| 60–70 | 736 (27.64) | 61 (8.29) | 7.64 ± 2.29 | ||
| 70~ | 1197 (44.95) | 109 (9.11) | 7.41 ± 2.50 | ||
| Sex | |||||
| Male | 1859 (69.81) | 159 (8.55) | 0.9803 | 7.33 ± 2.55 | 0.6370 |
| Female | 804 (30.19) | 69 (8.58) | 7.29 ± 2.59 | ||
| Obese | |||||
| No | 2314 (86.89) | 201 (8.69) | 0.5544 | 7.37 ± 2.53 | 0.0045 |
| Yes | 349 (13.11) | 27 (7.74) | 6.96 ± 2.69 | ||
| Insurance | |||||
| Government | 673 (25.27) | 60 (8.92) | 0.9177 | 7.16 ± 2.77 | 0.0040 |
| Private | 341 (12.81) | 28 (8.21) | 7.49 ± 2.78 | ||
| Uninsured | 1649 (61.92) | 140 (8.49) | 7.70 ± 2.46 | ||
| Smoking | |||||
| No | 1162 (43.63) | 95 (8.18) | 0.5308 | 7.32 ± 2.57 | 0.2555 |
| Yes | 1501 (56.37) | 133 (8.86) | 7.31 ± 2.55 | ||
| Family history of IHD * | |||||
| No | 1536 (57.68) | 132 (8.59) | 0.9451 | 7.24 ± 2.58 | 0.1109 |
| Yes | 1127 (42.32) | 96 (8.52) | 7.42 ± 2.53 | ||
| Prior MI/CAD | |||||
| No | 1693 (63.57) | 153 (9.04) | 0.2467 | 7.23 ± 2.58 | 0.0214 |
| Yes | 970 (36.43) | 75 (7.73) | 7.46 ± 2.58 | ||
| History Of DM | |||||
| No | 1754 (65.87) | 151 (8.61) | 0.9039 | 7.26 ± 2.62 | 0.2349 |
| Yes | 909 (34.13) | 77 (8.47) | 7.41 ± 2.42 | ||
| History of Hypertension | |||||
| No | 1611 (60.50) | 130 (8.07) | 0.2612 | 7.20 ± 2.40 | 0.0151 |
| Yes | 1052 (39.50) | 98 (9.32) | 7.48 ± 2.48 | ||
| MI | |||||
| NSTEMI | 1209 (45.40) | 124 (10.26) | 0.0044 | 6.09 ± 2.65 | <0.0001 |
| STEMI | 1454 (54.60) | 104 (7.15) | 8.33 ± 1.96 | ||
| Hospital type | |||||
| Specialized | 1034 (38.83) | 103 (9.96) | 0.0397 | 7.08 ± 2.64 | <0.0001 |
| Generalized | 1629 (61.17) | 125 (7.67) | 7.46 ± 2.49 | ||
| Comorbidities | Frequency (%) | In-Hospital Mortality | LOS (day) | ||
|---|---|---|---|---|---|
| N (%) | p Value | Mean ± SD | p Value | ||
| Rheumatic heart disease | |||||
| no | 2655 (99.70) | 226 (8.51) | 0.0002 | 7.32 ± 2.56 | 0.8367 |
| yes | 8 (0.30) | 2 (25.00) | 6.88 ± 3.18 | ||
| Heart Failure | |||||
| no | 2615 (98.20) | 222 (8.49) | 0.3251 | 7.31 ± 2.56 | 0.9827 |
| yes | 48 (1.80) | 6 (12.50) | 7.35 ± 2.37 | ||
| Cardiogenic Shock | |||||
| no | 2392 (89.82) | 204 (8.53) | 0.8550 | 7.27 ± 2.57 | 0.0137 |
| yes | 271 (10.18) | 24 (8.86) | 7.68 ± 2.43 | ||
| Hypertension | |||||
| no | 1998 (75.03) | 167 (8.36) | 0.5155 | 7.30 ± 2.57 | 0.8212 |
| yes | 665 (24.97) | 61 (9.17) | 7.35 ± 2.53 | ||
| Cerebrovascular disease | |||||
| no | 2253 (84.60) | 205 (9.10) | 0.0022 | 7.29 ± 2.60 | 0.5060 |
| yes | 410 (15.40) | 23 (5.61) | 7.43 ± 2.32 | ||
| Gastrointestinal disease | |||||
| no | 2620 (98.39) | 226 (8.63) | 0.3555 | 7.32 ± 2.56 | 0.5060 |
| yes | 43 (1.61) | 2 (4.65) | 7.05 ± 2.54 | ||
| Type-I DM | |||||
| no | 2307 (86.63) | 200 (8.67) | 0.6138 | 7.29 ± 2.60 | 0.5357 |
| yes | 356 (13.37) | 28 (7.87) | 7.48 ± 2.26 | ||
| Type-II DM | |||||
| no | 2322 (87.19) | 197 (8.48) | 0.7084 | 7.33 ± 2.56 | 0.4519 |
| yes | 341 (12.81) | 31 (9.09) | 7.23 ± 2.52 | ||
| Renal failure | |||||
| no | 2451 (92.04) | 206 (8.40) | 0.3247 | 7.34 ± 2.54 | 0.3972 |
| yes | 212 (7.96) | 22 (10.38) | 7.00 ± 2.71 | ||
| Dysrhythmia | |||||
| no | 2485 (93.32) | 216 (8.69) | 0.3689 | 7.29 ± 2.57 | 0.1766 |
| yes | 178 (6.68) | 12 (6.74) | 7.66 ± 2.69 | ||
| Peripheral Vascular Disease | |||||
| no | 2389 (89.71) | 201 (8.41) | 0.4196 | 7.30 ± 2.58 | 0.9493 |
| yes | 274 (10.29) | 27 (9.85) | 7.41 ± 2.32 | ||
| COPD | |||||
| no | 2525 (94.82) | 215 (8.51) | 0.7113 | 7.30 ± 2.56 | 0.1561 |
| yes | 138 (5.18) | 13 (9.42) | 7.61 ± 2.43 | ||
| Liver disease | |||||
| no | 2615 (98.20) | 224 (8.57) | 0.9545 | 7.31 ± 2.56 | 0.4408 |
| yes | 48 (1.80) | 4 (8.33) | 7.60 ± 2.44 | ||
| Hypercholesterolemia | |||||
| no | 1614 (60.61) | 140 (8.67) | 0.7972 | 7.22 ± 2.59 | 0.0499 |
| yes | 1049 | 88 (8.39) | 7.46 ± 2.50 | ||
| Thyroid Disorder | |||||
| no | 1950 | 175 (8.97) | 0.2082 | 7.19 ± 2.62 | <0.0001 |
| yes | 713 | 53 (7.43) | 7.65 ± 2.34 | ||
| Quality Indicators (QI) | Eligible Patients, No. (%) a | Overall Adherence, % | Hospital Variation, Range (%) |
|---|---|---|---|
| QI1: Aspirin prescribed within 3h of hospital arrival | 1549 (58.17) | 73.08 | 62.11–85.81 |
| QI2: Beta-blockers within 12h of arrival | 785 (23.69) | 38.98 | 32.89–45.45 |
| QI3: Clopidogrel within 12h of arrival | 2408 (90.42) | 67.86 | 62.68–73.27 |
| QI4: Thrombolytics received within 30 min of hospital arrival | 971 (36.46) | 7.52 | 3.57–11.43 |
| QI5: ECG within 10 min of hospital arrival | 2663 (100.00) | 62.49 | 57.74–71.84 |
| QI6: Left ventricular function assessment | 2663 (100.00) | 62.79 | 56.33–67.53 |
| QI7: Coronary angiography performed during hospital stay | 2663 (100.00) | 66.35 | 60.85–71.78 |
| QI8: Primary PCI | 2366 (88.85) | 37.36 | 29.52–43.59 |
| Prescription filled post-discharge | |||
| QI9: Aspirin | 1549 (58.17) | 47.97 | 38.51–61.29 |
| QI10: Beta-blocker | 785 (29.48) | 22.29 | 10.94–34.21 |
| QI11: Clopidogrel | 2408 (90.42) | 45.35 | 35.36–53.59 |
| QI12: Statin | 2020 (75.85) | 36.39 | 30.11–41.76 |
| QI13: ACE inhibitor | 2567 (96.40) | 38.02 | 29.70–45.54 |
| Outcome indicators | |||
| In-hospital mortality | 2663 (100.00) | 8.56 | 5.56–12.50 |
| Quality Indicators* | In−Hospital Mortality | Length of Stay | ||
|---|---|---|---|---|
| Adjusted β (p Value) | Unadjusted β (p Value) | Adjusted β (p Value) | Unadjusted β (p Value) | |
| QI1 | −0.0258 (0.9014) | −0.0382 (0.8540) | 0.1668 (0.1880) | 0.2930 (0.0340) |
| QI2 | 0.1174 (0.6616) | 0.1079 (0.6856) | 0.1873 (0.2207) | 0.2337 (0.1456) |
| QI3 | 0.0238 (0.8831) | 0.0156 (0.9229) | 0.5278 (<0.0001) | 0.7994 (<0.0001) |
| QI4 | 0.5451 (0.1898) | 0.6093 (0.1457) | −0.4913 (0.0351) | −0.4994 (0.0328) |
| QI5 | 0.0342 (0.8177) | 0.0525 (0.7229) | −0.2179 (0.0159) | −0.2913 (0.0043) |
| QI6 | 0.0048 (0.9742) | −0.0636 (0.6647) | 0.4251 (<0.0001) | 0.8413 (<0.0001) |
| QI7 | −0.0786 (0.6057) | −0.1535 (0.3110) | 0.9974 (<0.0001) | 1.5171 (<0.0001) |
| QI8 | −0.1276 (0.4603) | −0.2174 (0.2102) | 1.2699 (<0.0001) | 1.7515 (<0.0001) |
| Factors | Regression Coefficient, 95%CI | p Value |
|---|---|---|
| STEMI vs. NSTEMI | 1.451 (1.026, 2.053) | 0.0379 |
| Generalized vs. Specialized Hospital | 0.877 (0.613, 1.254) | 0.4270 |
| Cerebra disease | 0.620 (0.355, 1.082) | 0.0849 |
| Rheumatic Heart Disease (RHD) | 2.346 (0.070, 78.121) | 0.4952 |
| Composite score (per 10%) | 1.003 (0.937, 1.073) | 0.9284 |
| Factors | Regression Coefficient, 95%CI | p Value |
|---|---|---|
| Age | ||
| 50–60 vs. ~50 | 0.481 (0.132, 0.829) | 0.0069 |
| 60–70 vs. ~50 | 0.751 (0.432, 1.071) | <0.0001 |
| 70~ vs. ~50 | 0.587 (0.282, 0.891) | 0.0002 |
| Insurance | ||
| Government vs. Uninsured | 0.147 (−0.059, 0.354) | 0.1623 |
| Private vs. Uninsured | 0.202 (−0.069, 0.474) | 0.1443 |
| Prior MI/CAD | 0.021 (−0.210, 0.251) | 0.8595 |
| History of Hypertension | 0.137 (−0.091, 0.365) | 0.2401 |
| STEMI vs. NSTEMI | 2.049 (1.871, 2.227) | <0.0001 |
| Generalized vs. Specialized hospital | 0.168 (−0.164, 0.499) | 0.3213 |
| thyroid | 0.257 (0.058, 0.455) | 0.011 |
| lipids | 0.179 (−0.001, 0.359) | 0.051 |
| Composite score (per 10%) | 0.258 (0.217, 0.299) | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehman, S.; Li, X.; Wang, C.; Ikram, M.; Rehman, E.; Liu, M. Quality of Care for Patients with Acute Myocardial Infarction (AMI) in Pakistan: A Retrospective Study. Int. J. Environ. Res. Public Health 2019, 16, 3890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203890
Rehman S, Li X, Wang C, Ikram M, Rehman E, Liu M. Quality of Care for Patients with Acute Myocardial Infarction (AMI) in Pakistan: A Retrospective Study. International Journal of Environmental Research and Public Health. 2019; 16(20):3890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203890
Chicago/Turabian StyleRehman, Shazia, Xi Li, Chao Wang, Muhammad Ikram, Erum Rehman, and Meina Liu. 2019. "Quality of Care for Patients with Acute Myocardial Infarction (AMI) in Pakistan: A Retrospective Study" International Journal of Environmental Research and Public Health 16, no. 20: 3890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203890