Positive Orientation and Strategies for Coping with Stress as Predictors of Professional Burnout among Polish Nurses



Abstract
:1. Introduction
- Do selected sociodemographic variables, that is, age, work experience, and financial situation significantly differentiate a positive orientation among nurses?
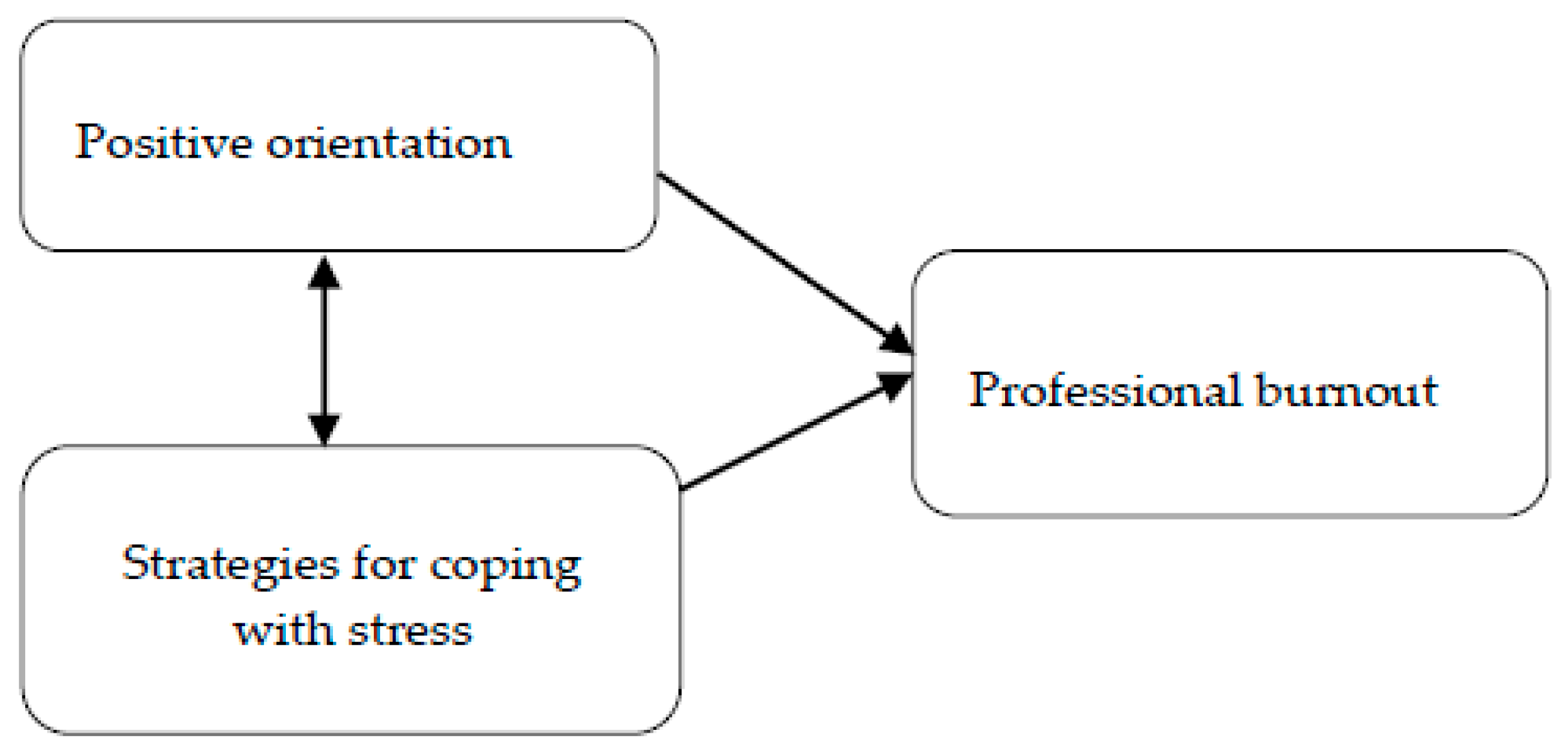
- What is the relationship between the level of positive orientation of nurses and their strategies of coping with stress and personal burnout, work-related burnout, and burnout in contact with patients?
- What is the role of positive orientation, coping strategies, and selected sociodemographic variables of nurses in the prediction of personal burnout, work-related burnout, and burnout in contact with patients?
2. Materials and Methods
2.1. Settings and Design
2.2. Participants
2.3. Research Instruments
2.3.1. The Polish Adaptation of the Positive Orientation Scale
2.3.2. The Polish Adaptation of the Mini-COPE
2.3.3. Copenhagen Burnout Inventory (CBI)
2.4. Statistical Analysis
3. Results
4. Discussion
Implications for the Nursing Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Manzano-García, G.; Ayala, J.C. Insufficiently studied factors related to burnout in nursing: Results from an e-Delphi study. PLoS ONE 2017, 12, e0175352. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.S.; Will, G.T. Low morale and mutual withdrawal on a mental hospital ward. Psychiatry 1953, 16, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Walkiewicz, M.; Sowińska, K.; Tartas, M. Wypalenie zawodowe wśród personelu medycznego-przegląd literatury. Burnout in the medical profession—A literature review. Przegląd Lek. 2014, 71, 263–269. [Google Scholar]
- Lin, F.; St John, W.; McVeigh, C. Burnout among hospital nurses in China. J. Nurs. Manag. 2009, 17, 294–301. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Kitaoka-Higashiguchi, K.; Morikawa, Y.; Nakagawa, H. Relationship between stress coping and burnout in Japanese hospital nurses. J. Nurs. Manag. 2009, 17, 359–365. [Google Scholar] [CrossRef]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Borritz, M.; Rugulies, R.; Bjorner, J.B.; Villadsen, E.; Mikkelsen, O.A.; Kristensen, T.S. Burnout among employees in human service work: Design and baseline findings of the PUMA study. Scand. J. Public Health 2006, 34, 49–58. [Google Scholar] [CrossRef]
- Vargas, C.; Cañadas, G.; Aguayo, R.; Fernandez, R.; de la Fuente, E. Which occupational risk factors are associated with burnout in nursing? A meta-analytic study. IJCHP 2014, 14, 28–38. [Google Scholar] [CrossRef]
- Garrosa, E.; Rainho, C.; Moreno-JimeÂnez, B.; Monteiro, M.J. The relationship between job stressors, hardy personality, coping resources and burnout in a sample of nurses: A correlational study at two time points. Int. J. Nurs. Stud. 2010, 47, 205–215. [Google Scholar] [CrossRef]
- Nie, Z.; Jin, Y.; He, L.; Chen, Y.; Ren, X.; Yu, J.; Yao, Y. Correlation of burnout with social support in hospital nurses. Int. J. Clin. Exp. Med. 2015, 8, 19144–19149. [Google Scholar]
- Juczyński, Z.; Ogińska–Bulik, N. Narzędzia Pomiaru Stresu i Radzenia Sobie ze Stresem [Tools for Measuring Stress and Coping with Stress]; Pracownia Testów Psychologicznych: Warsaw, Poland, 2009. [Google Scholar]
- Ogińska-Bulik, N. The role of personal and social resources in preventing adverse health outcomes in employees of uniformed professions. Int. J. Occup. Med. Environ. Health 2005, 18, 233–240. [Google Scholar] [PubMed]
- Ogińska–Bulik, N.; Juczyński, Z. Osobowościowe wyznaczniki satysfakcji z życia [Personality determinants of satisfaction with life]. In Psychologia Zdrowia–w Poszukiwaniu Pozytywnych Inspiracji [Health Psychology-in Search of Positive Inspiration]; Heszen, I., Życińska, J., Eds.; Wydawnictwo SWPS Academica: Warsaw, Poland, 2008; pp. 117–134. [Google Scholar]
- Seligman, M.E.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Caprara, G.V. Positive orientation: Turning potentials into optimal functioning. Eur. Health Psychologist. 2009, 11, 46–48. [Google Scholar]
- Caprara, G.V.; Steca, P.; Alessandri, G.; Abela, J.R.; McWhinnie, C.M. Positive orientation: Explorations on what is common to life satisfaction, self-esteem, and optimism. Epidemiol. Psych. Sci. 2010, 19, 63–71. [Google Scholar] [CrossRef]
- Caprara, G.V.; Alessandri, G.; Barbaranelli, C. Optimal functioning: The contribution of self efficacy beliefs to positive orientation. Psychother. Psychosom. 2010, 79, 328–330. [Google Scholar] [CrossRef]
- Łaguna, M.; Oleś, P.; Filipiuk, D. Orientacja pozytywna i jej pomiar: Polska adaptacja skali orientacji pozytywnej [Positive orientation and its measurement: Polish adaptation of positive orientation scale]. Stud. Psychol. 2011, 49, 47–54. [Google Scholar] [CrossRef]
- Alessandri, G.; Caprara, G.V.; Tisak, J. The unique contribution of positive orientation to optimal functioning: Farther explorations. Eur. Psychol. 2012, 17, 44–54. [Google Scholar] [CrossRef]
- Sobol–Kwapińska, M. Orientacja pozytywna–koncepcje teoretyczne i przegląd badań [Positive orientatio –theoretical cancepts and studies review]. Stud. Psychol. 2014, 52, 77–90. [Google Scholar] [CrossRef]
- Alessandri, G.; Vecchione, M.; Tisak, J.; Deiana, G.; Caria, S.; Caprara, G.V. The utility of positive orientation in predicting job performance and organizational citizenship behaviors. Appl. Psychol. 2012, 61, 669–698. [Google Scholar] [CrossRef]
- Oleś, P.K.; Alessandri, G.; Oleś, M.; Bąk, W.; Jankowski, T.; Laguna, M.; Caprara, G.V. Positive orientation and generalized self-efficacy. Stud. Psychol. 2013, 55, 47–59. [Google Scholar] [CrossRef]
- Miciuk, Ł.R.; Jankowski, T.; Laskowska, A.; Oleś, P. Positive Orientation and the Five-Factor Model. Pol. Psychol. Bull. 2016, 47, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Watkins, P.C. Gratitude and the Good Life: Toward a Psychology of Appreciation; Springer: New York, NY, USA, 2013. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Carver, C.S.; Scheier, M.F. Situational Coping and Coping Dispositions in a Stressful Transaction. J. Pers. Soc. Psychol. 1994, 66, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Endler, N.S.; Parker, J.D. Multidimensional assessment of coping: A critical evaluation. J. Pers. Soc. Psychol. 1990, 58, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing Coping Strategies: A Theoretically Based Approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef]
- Pusz, P.; Zaręba, L. Metody Statystyczne Analizy Danych [Statistical Methods of Data Analysis]; Mitel: Rzeszów, Poland, 2013. [Google Scholar]
- Nowakowska, I. Zarządzanie Jakością Pracy Zespołu Pielęgniarskiego w Szpitalu [Work Quality of a Hospital Nursing Team-Dissertation]; Uniwersytet Medyczny im. K. Marcinkowskiego w Poznaniu: Poznań, Poland, 2011. [Google Scholar]
- Alessandri, G.; Caprara, G.V.; Tisak, J. A Unified Latent Curve, Latent State-Trait Analysis of the Developmental Trajectories and Correlates of Positive Orientation. Multivar. Behav. Res. 2012, 47, 341–368. [Google Scholar] [CrossRef]
- Lorenz, V.R.; Benatti, M.C.C.; Sabino, M.O. Burnout and stress among nurses in a university tertiary hospital. Rev. Lat. Am. Enfermagem. 2010, 18, 1084–1091. [Google Scholar] [CrossRef]
- Hsu, H.Y.; Chen, S.-H.; Yu, H.-Y.; Lou, J.H. Job stress, achievement motivation and occupational burnout among male nurses. J. Adv. Nurs. 2010, 66, 1592–1601. [Google Scholar] [CrossRef]
- Hamaideh, S.H.; Mrayyan, M.T.; Mudallal, R.; Faouri, I.G.; Khasawneh, N.A. Jordanian nurses’ job stressors and social support. Int. Nurs. Rev. 2008, 55, 40–47. [Google Scholar] [CrossRef]
- Akbar, R.E.; Elahi, N.; Mohammadi, E.; Khoshknab, M.F. What Strategies Do the Nurses Apply to Cope with Job Stress? A Qualitative Study. Glob. J. Health Sci. 2016, 8, 55–64. [Google Scholar] [CrossRef]
- McTiernan, K.; McDonald, N. Occupational stressors, burnout and coping strategies between hospital and community psychiatric nurses in a Dublin region. J. Psychiatr. Ment. Health Nurs. 2015, 22, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, S. How nurses can cope with stress and avoid burnout. Emerg. Nurs. 2014, 22, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Chan, H.J. Optimism and proactive coping in relation to burnout among nurses. J. Nurs. Manag. 2015, 23, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Geuens, N.; Braspenning, M.; Van Bogaert, P.; Franck, E. Individual vulnerability to burnout in nurses: The role of Type D personality within different nursing specialty areas. Burn. Res. 2015, 2, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Bakhamis, L.; Paul, D.; Smith, H.; Coustasse, A. Still an Epidemic: The Burnout Syndrome in Hospital Registered Nurses. Health Care Manag. 2019, 38, 3–10. [Google Scholar] [CrossRef]
- Wang, L.; Tao, H.; Bowers, B.; Brown, R.; Zhang, Y. Influence of Social Support and Self-Efficacy on Resilience of Early Career Registered Nurses. West. J. Nurs. Res. 2018, 40, 648–664. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y. Work stress, perceived social support, self-efficacy and burnout among Chinese registered nurses. J. Nurs. Manag. 2019, 27, 1445–1453. [Google Scholar] [CrossRef]
- Yestiana, Y.; Kurniati, T.; Hidayat, A.A.A. Predictors of burnout in nurses working in inpatient rooms at a public hospital in Indonesia. Pan Afr. Med. J. 2019, 33, 148. [Google Scholar] [CrossRef]
- Sampson, M.; Melnyk, B.M.; Hoying, J. Intervention Effects of the MINDBODYSTRONG Cognitive Behavioral Skills Building Program on Newly Licensed Registered Nurses’ Mental Health, Healthy Lifestyle Behaviors, and Job Satisfaction. J. Nurs. Adm. 2019, 49, 487–495. [Google Scholar] [CrossRef]


{kind=link}
| Positive Orientation Scale | Kruskal–Wallis Test (H) | Chi-Square Test (χ2) | Spearman’s Rank Correlation Coefficient (R) | ||||
|---|---|---|---|---|---|---|---|
| H | p-Value | χ2 | p-Value | R | t(N-2) | p-Value | |
| Age | 3.46 | n.s. | 7.87 | n.s. | −0.008 | −0.38 | n.s. |
| Work experience | 1.17 | n.s. | 11.26 | n.s. | −0.02 | −0.98 | n.s. |
| Financial situation | 152.83 | 0.001 | 155.23 | 0.001 | 0.28 | 12.45 | 0.001 |
| Strategies for Coping with Stress (Mini-COPE) | Positive Orientation | |||
|---|---|---|---|---|
| Spearman’s (R) | T(N-2) | p-Value | ||
| 1. | Active coping | 0.22 | 9.71 | 0.001 |
| 2. | Planning | 0.27 | 12.10 | 0.001 |
| 3. | Positive revalidation | 0.25 | 11.09 | 0.001 |
| 4. | Acceptance | 0.19 | 8.11 | 0.001 |
| 5. | Sense of humor | 0.06 | 2.38 | n.s. |
| 6. | Turn to religion | 0.03 | 1.12 | n.s |
| 7. | Seeking emotional support | 0.27 | 12.01 | 0.001 |
| 8. | Seeking instrumental support | 0.19 | 8.09 | 0.001 |
| 9. | Taking care of something else | 0.06 | 2.50 | 0.01 |
| 10. | Denial | −0.10 | −4.42 | 0.001 |
| 11. | Discharge | −0.09 | −3.74 | 0.001 |
| 12. | Use of psychoactive substances | −0.09 | −3.79 | 0.001 |
| 13. | Cessation of actions | −0.21 | −8.96 | 0.001 |
| 14. | Self-blaming | −0.26 | −11.63 | 0.001 |
| Variables | Personal Burnout | Work-Related Burnout | Burnout in Contacts with Patients | ||||
|---|---|---|---|---|---|---|---|
| Spearman’s (R) | p-Value | Spearman’s (R) | p-Value | Spearman’s (R) | p-Value | ||
| Positive orientation | −0.39 | 0.001 | −0.31 | 0.001 | −0.30 | 0.001 | |
| Strategies for coping with stress (Mini-COPE) | |||||||
| 1. | Active coping | −0.17 | 0.001 | −0.18 | 0.001 | −0.15 | 0.001 |
| 2. | Planning | −0.13 | 0.001 | −0.13 | 0.001 | −0,13 | 0.001 |
| 3. | Positive revalidation | −0.08 | 0.001 | −0.06 | 0.01 | −0.07 | 0.001 |
| 4. | Acceptance | −0.09 | 0.001 | −0.10 | 0.001 | −0.10 | 0.001 |
| 5. | Sense of humor | 0.03 | n.s. | 0.04 | n.s. | 0.03 | n.s. |
| 6. | Turn to religion | 0.01 | n.s. | −0.04 | n.s. | −0.02 | n.s. |
| 7. | Seeking emotional support | −0.15 | 0.001 | −0.13 | 0.001 | −0.14 | 0.001 |
| 8. | Seeking instrumental support | −0.01 | n.s | −0.04 | n.s | −0.04 | n.s |
| 9. | Taking care of something else | 0.05 | 0.05 | 0.03 | n.s | 0.03 | n.s |
| 10. | Denial | 0.16 | 0.001 | 0.14 | 0.001 | 0.12 | 0.001 |
| 11. | Discharge | 0.16 | 0.001 | 0.11 | 0.001 | 0.09 | 0.001 |
| 12. | Use of psychoactive substances | 0.13 | 0.001 | 0.11 | 0.001 | 0.09 | 0.001 |
| 13. | Cessation of actions | 0.20 | 0.001 | 0.18 | 0.001 | 0.17 | 0.001 |
| 14. | Self-blaming | 0.19 | 0.001 | 0.11 | 0.001 | 0.10 | 0.001 |
| Age | 0.04 | n.s. | 0.10 | 0.001 | 0.06 | 0.01 | |
| Work experience | 0.06 | 0.05 | 0.13 | 0.001 | 0.08 | 0.001 | |
| Financial situation | −0.24 | 0.001 | −0.22 | 0.001 | −0.21 | 0.001 | |
| Variables | R2 | β-Standardized | β | Error β | t | p-Value |
|---|---|---|---|---|---|---|
| Constant value | 67.65 | 3.25 | 20.78 | 0.001 | ||
| Positive orientation | 0.16 | −0.32 | −1.22 | 0.09 | −14.28 | 0.001 |
| Financial situation | 0.18 | 0.15 | 2.72 | 0.39 | 6.93 | 0.001 |
| Discharge | 0.19 | 0.10 | 2.41 | 0.55 | 4.38 | 0.001 |
| Denial | 0.20 | 0.07 | 1.53 | 0.49 | 3.14 | 0.001 |
| Active coping | 0.21 | −0.06 | −1.64 | 0.57 | −2.88 | 0.001 |
| Use of psychoactive substances | 0.21 | 0.06 | 1.89 | 0.69 | 2.74 | 0.01 |
| Work experience | 0.21 | 0.05 | 0.09 | 0.04 | 2.60 | 0.01 |
| R = 0.46; R2 = 0.21; Corrected R2 = 0.21 | ||||||
| Variables | R2 | β-Standardized | β | Error β | t | p-Value |
|---|---|---|---|---|---|---|
| Constant value | 75.43 | 2.832 | 26.64 | 0.001 | ||
| Positive orientation | 0.10 | −0.23 | −0.85 | 0.086 | −9.88 | 0.001 |
| Financial situation | 0.12 | −0.15 | −2.56 | 0.392 | −6.53 | 0.001 |
| Work experience | 0.14 | 0.13 | 0.21 | 0.035 | 6.04 | 0.001 |
| Cessation of actions | 0.15 | 0.07 | 1.64 | 0.541 | 3.03 | 0.001 |
| Active coping | 0.15 | −0.10 | −2.47 | 0.570 | −4.34 | 0.001 |
| Discharge | 0.16 | 0.08 | 1.93 | 0.527 | 3.67 | 0.001 |
| R = 0.39; R2 = 0.16; Corrected R2 = 0.16 | ||||||
| Variables | R2 | β-Standardized | β | Error β | t | p-Value |
|---|---|---|---|---|---|---|
| Constant value | 82.26 | 3.40 | 24.18 | 0.001 | ||
| Positive orientation | 0.09 | −0.22 | −0.97 | 0.10 | −9.23 | 0.001 |
| Financial situation | 0.11 | −0.14 | −2.98 | 0.47 | −6.33 | 0.001 |
| Cessation of actions | 0.12 | 0.07 | 2.00 | 0.65 | 3.07 | 0.001 |
| Work experience | 0.13 | 0.09 | 0.17 | 0.04 | 4.01 | 0.001 |
| Active coping | 0.14 | −0.07 | −2.23 | 0.71 | −3.14 | 0.001 |
| Discharge | 0.14 | 0.07 | 2.03 | 0.64 | 3.16 | 0.001 |
| Acceptance | 0.14 | −0.05 | −1.39 | 0.65 | −2.14 | 0.01 |
| R = 0.37; R2 = 0.14; Corrected R2 = 0.14 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kupcewicz, E.; Jóźwik, M. Positive Orientation and Strategies for Coping with Stress as Predictors of Professional Burnout among Polish Nurses. Int. J. Environ. Res. Public Health 2019, 16, 4264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214264
Kupcewicz E, Jóźwik M. Positive Orientation and Strategies for Coping with Stress as Predictors of Professional Burnout among Polish Nurses. International Journal of Environmental Research and Public Health. 2019; 16(21):4264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214264
Chicago/Turabian StyleKupcewicz, Ewa, and Marcin Jóźwik. 2019. "Positive Orientation and Strategies for Coping with Stress as Predictors of Professional Burnout among Polish Nurses" International Journal of Environmental Research and Public Health 16, no. 21: 4264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214264