Trends in Hospital Admissions for Pertussis Infection: A Nationwide Retrospective Observational Study in Italy, 2002–2016



Abstract
:1. Background
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
List of Abbreviations
References
- Esposito, S. Prevention of pertussis: From clinical trials to Real World Evidence. J. Prev. Med. Hyg. 2018. [Google Scholar] [CrossRef]
- Stefanelli, P.; Buttinelli, G.; Vacca, P.; Tozzi, A.E.; Midulla, F.; Carsetti, R.; Fedele, G.; Villani, A.; Concato, C.; Pertussis Study Group. Severe pertussis infection in infants less than 6 months of age: Clinical manifestations and molecular characterization. Hum. Vaccin. Immunother. 2017. [Google Scholar] [CrossRef]
- Warfel, J.M.; Zimmerman, L.; Merkel, T.J. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc. Natl. Acad. Sci. USA 2014. [Google Scholar] [CrossRef]
- Wirsing von König, C.H.; Riffelman, M. Pertussis: An old disease in new clothes. Eurosurveillance 2007. [Google Scholar] [CrossRef] [PubMed]
- Guiso, N.; Wirsing von König, C.H.; Forsyth, K.; Tan, T.; Plotkin, S.A. The Global Pertussis Initiative: Report from a round table meeting to discuss the epidemiology and detection of pertussis, Paris, France, 11–12 January 2010. Vaccine 2011. [Google Scholar] [CrossRef] [PubMed]
- Gabutti, G.; Rota, M.C.; Bonato, B.; Pirani, R.; Turlà, G.; Cucchi, A.; Cavallaro, A. Hospitalizations for pertussis in Italy, 1999–2009: Analysis of the hospital discharge database. Eur. J. Pediatr. 2012. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Vaccination Schedule. Available online: http://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=4829&area=vaccinazioni&menu=vuoto (accessed on 15 February 2019).
- Esposito, S.; Principi, N. Prevention of pertussis: An unresolved problem. Hum. Vaccin. Immunother. 2018, 14, 2452–2459. [Google Scholar] [CrossRef]
- Di Mattia, G.; Nicolai, A.; Frassanito, A.; Petrarca, L.; Nenna, R.; Midulla, F. Pertussis: New preventive strategies for an old disease. Paediatr. Respir. Rev. 2019, 29, 68–73. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N.; European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Vaccine Study Group (EVASG)2. Immunization against pertussis in adolescents and adults. Clin. Microbiol. Infect. 2016. [Google Scholar] [CrossRef]
- Brindicci, G.; Carboni, D.; Genga, R.; Moschini, E.; Montorzi, G.; Viscogliosi, F.; Muratori, G.; Ripanti, G. Report on three cases of pertussis in the Urbino area (Italy). Infez. Med. 2018, 26, 85–88. [Google Scholar]
- Italian Institute of Statistics. Available online: http://demo.istat.it/ (accessed on 3 March 2019).
- Ministry of Health. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 7 March 2019).
- Palazzo, R.; Carollo, M.; Fedele, G.; Rizzo, C.; Rota, M.C.; Giammanco, A.; Iannazzo, S.; Ausiello, C.M.; Sero-Epidemiology Working Group. Evidence of increased circulation of Bordetella pertussis in the Italian adult population from seroprevalence data (2012–2013). J. Med. Microbiol. 2016, 65, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Dalby, T.; Forsyth, K.; Halperin, S.A.; Heininger, U.; Hozbor, D.; Plotkin, S.; Ulloa-Gutierrez, R.; Wirsing von König, C.H. Pertussis Across the Globe: Recent Epidemiologic Trends From 2000 to 2013. Pediatr. Infect. Dis. J. 2015. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global and Regional Immunization Profile: European Region. Available online: http://www.who.int/immunization/monitoring_surveillance/data/gs_eurprofile. pdf?ua=1 (accessed on 1 April 2019).
- Mooi, F.R.; van Loo, I.H.; van Gent, M.; He, Q.; Bart, M.J.; Heuvelman, K.J.; de Greeff, S.C.; Diavatopoulos, D.; Teunis, P.; Nagelkerke, N.; et al. Bordetella pertussis strains with increased toxin production associated with pertussis resurgence. Emerg. Infect. Dis. 2009. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, S.H.; Nadi, E.; Hajilooi, M.; Seif-Rabiei, M.A.; Samaei, A. High Seroprevalence of Bordetella pertussis in Patients with Chronic Obstructive Pulmonary Disease: A Case-Control Study. Tanaffos 2015, 14, 172–176. [Google Scholar] [PubMed]
- Loconsole, D.; De Robertis, A.L.; Morea, A.; Metallo, A.; Lopalco, P.L.; Chironna, M. Resurgence of Pertussis and Emergence of the Ptxp3 Toxin Promoter Allele in South Italy. Pediatr. Infect. Dis. J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bonanni, P.; Ferro, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.G.; Rizzuto, E.; Signorelli, C. Vaccine coverage in Italy and assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39 (Suppl. S1), 146–158. [Google Scholar]
- Hickler, B.; Guirguis, S.; Obregon, R. Vaccine special issue on vaccine hesitancy. Vaccine 2015, 33, 4155–4156. [Google Scholar] [CrossRef]
- Burioni, R.; Odone, A.; Signorelli, C. Lessons from Italy’s policy shift on immunization. Nature 2018, 555, 30. [Google Scholar] [CrossRef]
- Berti, E.; Chiappini, E.; Orlandini, E.; Galli, L.; de Martino, M. Pertussis is still common in a highly vaccinated infant population. Acta Paediatr. 2014. [Google Scholar] [CrossRef]
- Giles, M.L.; Krishnaswamy, S.; Wallace, E.M. Maternal immunisation: What have been the gains? Where are the gaps? What does the future hold? F1000Research 2018. [Google Scholar] [CrossRef]
- Saji, F.; Samejima, Y.; Kamiura, S.; Koyama, M. Dynamics of immunoglobulins at the feto-maternal interface. Rev. Reprod. 1999, 4, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Abu Raya, B.; Srugo, I.; Kessel, A.; Peterman, M.; Bader, D.; Peri, R.; Ashtamker, N.; Gonen, R.; Bamberger, E. The induction of breast milk pertussis specific antibodies following gestational tetanus-diphtheria-acellular pertussis vaccination. Vaccine 2014. [Google Scholar] [CrossRef] [PubMed]
- Gabutti, G.; Conforti, G.; Tomasi, A.; Kuhdari, P.; Castiglia, P.; Prato, R.; Memmini, S.; Azzari, C.; Rosati, G.V.; Bonanni, P. Why, when and for what diseases pregnant and new mothers “should” be vaccinated. Hum. Vaccin. Immunother. 2017. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, A.E.; Vitali Rosati, G.; Ciarrocchi, G.; Ferrera, G.; Gabutti, G.; Giuffrida, S.; Locuratolo, F.; Marchetti, F.; Mereu, G.; Pellegrino, A.; et al. Riduzione del rischio di pertosse nel neonato mediante vaccinazione: La strategia cocoon in Italia. Riv. Immunol. Allergol. Pediatr. 2012, 2, 1–14. [Google Scholar]
- Gabutti, G.; Azzari, C.; Bonanni, P.; Prato, R.; Tozzi, A.E.; Zanetti, A.; Zuccotti, G. Pertussis: Current perspectives on epidemiology and prevention. Hum. Vaccin. Immunother. 2015. [Google Scholar] [CrossRef] [PubMed]
- Skoff, T.H.; Kenyon, C.; Cocoros, N.; Liko, J.; Miller, L.; Kudish, K.; Baumbach, J.; Zansky, S.; Faulkner, A.; Martin, S.W. Sources of Infant Pertussis Infection in the United States. Pediatrics 2015. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, K.; Plotkin, S.; Tan, T.; Wirsing von König, C.H. Strategies to decrease pertussis transmission to infants. Pediatrics 2015. [Google Scholar] [CrossRef]
- Fiasca, F.; Necozione, S.; Fabiani, L.; Mastrodomenico, M.; Mattei, A. Measles-Related Hospitalizations in Italy, 2004–2016: The Importance of High Vaccination Coverage. Ann. Glob. Health 2019. [Google Scholar] [CrossRef]
- Fiasca, F.; Mattei, A.; Vittorini, P.; Necozione, S.; Appetiti, A.; Angelone, A.M.; Fabiani, L. Bacterial Meningitis Hospitalizations after the 2009 L’Aquila Earthquake: A Retrospective Observational Study. Asian J. Epidemiol. 2018. [Google Scholar] [CrossRef]
- Mattei, A.; Sbarbati, M.; Fiasca, F.; Angelone, A.M.; Mazzei, M.C.; di Orio, F. Temporal trends in hospitalization for rotavirus gastroenteritis: A nationwide study in Italy, 2005-2012. Hum. Vaccin. Immunother. 2016. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Investigated Variables | N = 9393 |
|---|---|
| Gender, n (%) | |
| Male | 4452 (47.40) |
| Female | 4941 (52.60) |
| Age (years), mean ± SD | 6.32 ± 20.57 |
| Age classes, n (%) | |
| <1 year | 5954 (63.39) |
| 1–4 years | 841 (8.95) |
| 5–14 years | 1718 (18.29) |
| ≥15 years | 880 (9.37) |
| Nationality, n (%) | |
| Italian | 8842 (94.13) |
| Immigrant | 551 (5.87) |
| Geographical location, n (%) | |
| North | 2630 (28.00) |
| Centre | 1835 (19.54) |
| South and Islands | 4928 (52.46) |
| Deaths, n (%) | |
| No | 9359 (99.64) |
| Yes | 34 (0.36) |
| Concomitant chronic respiratory diseases, n (%) | |
| No | 9020 (96.03) |
| Yes | 373 (3.97) |
| Lenght of hospital stay (days), mean ± SD | 6.59 ± 7.81 |
| Hospital charge (€), mean ± SD | 1806 ± 2236 |
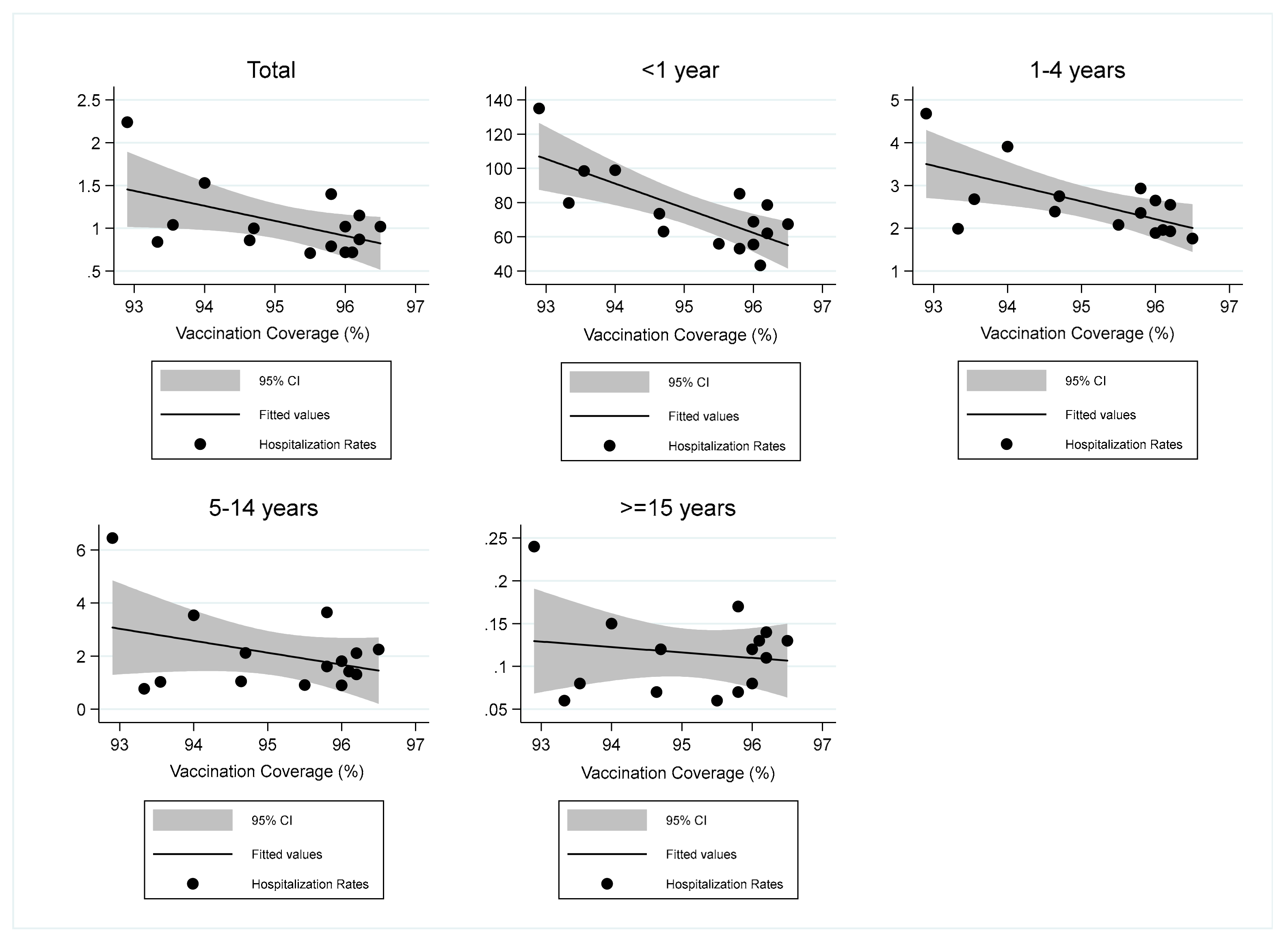
| Hospitalization Rates | Vaccination Coverage of 24 Months Old Children | ||
|---|---|---|---|
| Regression Coefficient | r2 | p-Value | |
| Total | −0.18 | 0.269 | 0.048 |
| <1 years | −14.40 | 0.555 | 0.001 |
| 1–4 years | −0.42 | 0.387 | 0.013 |
| 5–14 years | −0.45 | 0.129 | 0.189 |
| ≥15 years | −0.01 | 0.024 | 0.581 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiasca, F.; Gabutti, G.; Mattei, A. Trends in Hospital Admissions for Pertussis Infection: A Nationwide Retrospective Observational Study in Italy, 2002–2016. Int. J. Environ. Res. Public Health 2019, 16, 4531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224531
Fiasca F, Gabutti G, Mattei A. Trends in Hospital Admissions for Pertussis Infection: A Nationwide Retrospective Observational Study in Italy, 2002–2016. International Journal of Environmental Research and Public Health. 2019; 16(22):4531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224531
Chicago/Turabian StyleFiasca, Fabiana, Giovanni Gabutti, and Antonella Mattei. 2019. "Trends in Hospital Admissions for Pertussis Infection: A Nationwide Retrospective Observational Study in Italy, 2002–2016" International Journal of Environmental Research and Public Health 16, no. 22: 4531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224531