Overweight in Young Athletes: New Predictive Model of Overfat Condition

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Body Composition Assessment
- Waist is taken at the narrowest level, or if this is not apparent, at the midpoint between the lowest rib and the top of the hip bone (iliac crest).
- Hip is taken over minimal clothing at the greatest protrusion of the gluteus muscles. The subject stands erect with their weight evenly distributed on both feet and legs slightly parted without tensing the muscles.
- Bicep circumference, with the arms relaxed, is taken at the level of the midpoint between the acromion and the olecranon processes.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maffetone, P.B.; Rivera-Dominguez, I.; Laursen, P.B. Overfat and Underfat: New Terms and Definitions Long Overdue. Front Public Health. 2016, 4, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, G.H. The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function. Obes. Facts. 2017, 10, 207–215. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Gratteri, S.; Gualtieri, P.; Cammarano, A.; Bertucci, P.; Di Renzo, L. Why Primary obesity is a Disease? J. Transl. Med. 2019, 17, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonnalagadda, S.S.; Skinner, R.; Moore, L. Overweight athlete: fact or fiction? Curr. Sports Med. Rep. 2004, 3, 198–205. [Google Scholar] [CrossRef] [PubMed]
- WHO, Obesity Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 18 September 2019).
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic Performance of Body Mass Index to Identify Obesity as Defined by Body Adiposity in Children and Adolescents: A Systematic Review and Meta-Analysis. Pediatr. Obes. 2015, 10, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Petri, C.; Mascherini, G.; Bini, V.; Anania, G.; Calà, P.; Toncelli, L.; Galanti, G. Integrated Total Body Composition Versus Body Mass Index in Young Athletes. Available online: https://europepmc.org/article/med/27057821 (accessed on 14 December 2019).
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Dahlqvist, L.O. Advanced Body Composition Assessment: from Body Mass Index to Body Composition Profiling. J. Investig. Med. 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Ackland, T.R.; Lohman, T.G.; Sundgot-Borgen, J.; Maughan, R.J.; Meyer, N.L.; Stewart, A.D.; Müller, W. Current Status of Body Composition Assessment in Sport: Review and Position Statement on Behalf of the Ad Hoc Research Working Group on Body Composition Health and performance, Under the Auspices of the I.O.C. Medical Commission. Sports Med. 2012, 42, 227–249. [Google Scholar] [CrossRef]
- Alves Junior, C.A.; Mocellin, M.C.; Gonçalves, E.C.A.; Silva, D.A.; Trindade, E.B. Anthropometric Indicators as Body Fat Discriminators in Children and Adolescents: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 718–727. [Google Scholar] [CrossRef] [Green Version]
- Roberts, C.; Freeman, J.; Samdal, O.; Schnohr, C.W.; de Looze, M.E.; Nic Gabhainn, S.; Iannotti, R.; Rasmussen, M.; International HBSC Study Group. The Health Behavior in School-Aged Children (HBSC) Study: Methodological Developments and Current Tensions. Int. J. Public Health 2009, 54, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Mascherini, G.; Petri, C.; Galanti, G. Integrated Total Body Composition and Localized Fat-Free Mass Assessment. Sport Sci. Health 2015, 11, 217. [Google Scholar] [CrossRef]
- Stewart, A.D.; Marfell-Jones, M.; Olds, T.J.; De Ridder, H. Skinfolds in International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Glasgow, UK, 2011. [Google Scholar]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical Impedance Analysis—Part I: Review of Principles and Methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Marini, E.; Campa, F.; Buffa, R.; Stagi, S.; Matia, C.N.; Toselli, S.; Sardinha, L.S.; Silva, A.M. Phase Angle and Bioelectrical Impedance Vector Analysis in the Evaluation of Body Composition in Athletes. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.D.; Cole, T.J.; Fry, T.; Jebb, S.A.; Prentice, A.M. Body Fat Reference Curves for Children. Int. J. Obes. (Lond.) 2006, 30, 598–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Lobstein, T. Extended International (IOTF) Body Mass Index Cut-Offs for Thinness, Overweight and Obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the Accuracy of Diagnostic Systems. Science 1998, 240, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Demsar, J.; Curk, T.; Erjavec, A.; Gorup, C.; Hocevar, T.; Milutinovic, M.; Možina, M.; Polajnar, M.; Toplak, M.; Starič, A.; et al. Orange: Data Mining Toolbox in Python. J. Mach. Learn. Res. 2013, 14, 2349–2353. [Google Scholar]
- Sardinha, L.B.; Going, S.B.; Teixeira, P.J.; Lohman, T.G. Receiver Operating Characteristic Analysis of Body Mass Index, Triceps Skinfold Thickness, and Arm Girth for Obesity Screening in Children and Adolescents. Am. J. Clin. Nutr. 1999, 70, 1090–1095. [Google Scholar] [CrossRef] [Green Version]
- Hoshikawa, Y.; Muramatsu, M.; Iida, T.; Uchiyama, A.; Nakajima, Y.; Kanehisa, H. Event-Related Differences in the Cross-Sectional Areas and Torque Generation Capabilities of Quadriceps Femoris and Hamstrings in Male High School Athletes. J. Physiol. Anthropol. 2010, 29, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Tsunawake, N.; Tahara, Y.; Yukawa, K.; Katsuura, T.; Harada, H.; Kikuchi, Y. Classification of Body Shape of Male Athletes by Factor Analysis. Ann. Physiol. Anthropol. 1994, 13, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Horan, M.; Gibney, E.; Molloy, E.; McAuliffe, F. Methodologies to Assess Paediatric Adiposity. Ir. J. Med. Sci. 2015, 184, 53–68. [Google Scholar] [CrossRef]
- Reilly, J.; Wilson, J.; Durnin, J. Determination of Body Composition From Skinfold Thickness: A Validation Study. Arch. Dis. Child. 1975, 73, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Sinning, W.E.; Dolny, D.G.; Little, K.D.; Cunningham, L.N.; Racaniello, A.; Siconolfi, S.F.; Sholes, J.L. Validity of ‘‘Generalised’’ Equations for Body Composition Analysis in Male Athletes. Med. Sci. Sports Exerc. 1985, 17, 124–130. [Google Scholar]
- Wells, J.C. A Critique of the Expression of Paediatric Body Composition Data. Arch. Dis. Child. 2001, 85, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Krebs, N.F.; Himes, J.H.; Jacobson, D.; Nicklas, T.A.; Guilday, P.; Styne, D. Assessment of Child and Adolescent Overweight and Obesity. Pediatrics 2007, 120, S193–S228. [Google Scholar] [CrossRef] [Green Version]
- Mascherini, G.; Castizo-Olier, J.; Irurtia, A.; Petri, C.; Galanti, G. Differences between the Sexes in Athletes’ Body Composition and Lower Limb Bioimpedance Values. Muscles Ligaments Tendons J. 2018, 7, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Mascherini, G.; Petri, C.; Calà, P.; Bini, V.; Galanti, G. Lifestyle and Resulting Body Composition in Young Athletes. Available online: https://europepmc.org/article/med/28006893 (accessed on 18 November 2019).
- Petri, C.; Mascherini, G.; Bini, V.; Toncelli, L.; Armentano, N.; Calà, P.; Galanti, G. Evaluation of Physical Activity and Dietary Behaviors in Young Athletes: A Pilot Study. Minerva Pediatr. 2017, 69, 463–469. [Google Scholar] [CrossRef]
- Fairchild, T.J.; Klakk, H.; Heidemann, M.S.; Andersen, L.B.; Wedderkopp, N. Exploring the Relationship between Adiposity and Fitness in Young Children. Med. Sci. Sports Exerc. 2016, 48, 1708–1714. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Male (n = 620) | Female (n = 426) | p Value |
|---|---|---|---|
| Age (y) | 13.87 ± 2.42 | 12.74 ± 2.33 | <0.001 |
| Height (m) | 1.64 ± 0.14 | 1.55 ± 0.12 | <0.001 |
| Weight (kg) | 55.71 ± 15.24 | 48.97 ± 13.19 | <0.001 |
| BMI (kg/m2) | 20.23 ± 3.33 | 20.04 ± 3.33 | 0.076 |
| Waist circ. (cm) | 68.34 ± 8.88 | 64.22 ± 8.67 | <0.001 |
| Hip circ. (cm) | 85.18 ± 10.07 | 83.85 ± 13.41 | 0.057 |
| Hip/waist | 0.807 ± 0.14 | 0.809 ± 0.46 | <0.001 |
| WHR | 0.52 ± 0.04 | 0.54 ± 0.07 | <0.001 |
| Biceps Circ. (cm) | 24.40 ± 4.30 | 25.08 ± 29.41 | 0.001 |
| Biceps fold (mm) | 6.07 ± 3.50 | 8.54 ± 3.87 | <0.001 |
| Triceps fold (mm) | 11.57 ± 5.48 | 16.47 ± 5.74 | <0.001 |
| Subscapular fold (mm) | 9.16 ± 5.18 | 12.28 ± 8.11 | <0.001 |
| Supra iliac fold (mm) | 11.08 ± 7.06 | 15.10 ± 7.37 | <0.001 |
| Axilla fold (mm) | 8.06 ± 5.25 | 10.68 ± 6.81 | <0.001 |
| Pectoral fold (mm) | 7.85 ± 4.96 | 11.03 ± 5.05 | <0.001 |
| Abdomen fold (mm) | 12.51 ± 8.02 | 17.14 ± 7.98 | <0.001 |
| Quadriceps fold (mm) | 15.29 ± 9.54 | 22.10 ± 6.51 | <0.001 |
| Sum fold (mm) | 81.58 ± 42.66 | 91.25 ± 38.95 | <0.001 |
| Fat Mass from Skinfold (%) | 16.85 ± 7.22 | 23.62 ± 7.56 | <0.001 |
| RZ (Ω) | 566.85 ± 89.97 | 623.62 ± 69.18 | <0.001 |
| XC (Ω) | 61.62 ± 8.07 | 66.22 ± 25.74 | <0.001 |
| PA (°) | 6.29 ± 0.92 | 6.08 ± 2.17 | <0.001 |
| Fat Mass from BIA (%) | 18.25 ± 7.00 | 25.11 ± 6.34 | <0.001 |
| Fat Mass (Kg) | 10.43 ± 6.20 | 12.92 ± 6.35 | <0.001 |
| Free Fat Mass (Kg) | 45.28 ± 11.79 | 36.08 ± 7.72 | <0.001 |
| Anthropometric Variable | Area under the curve (%) |
|---|---|
| Waist circumference | 0.877 ± 0.011 |
| Waist/height | 0.882 ± 0.013 |
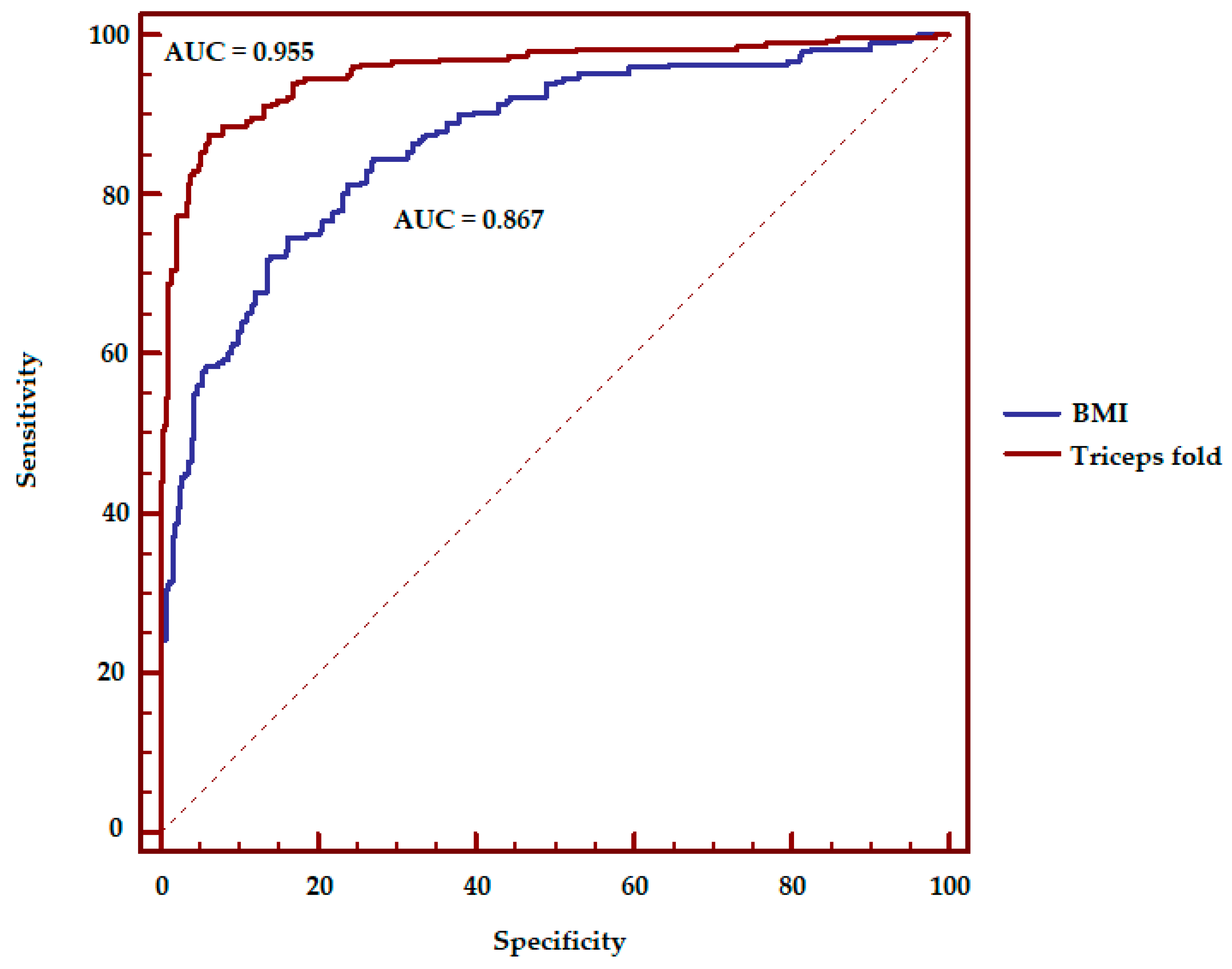
| Waist/hip | 0.867 ± 0.013 |
| Biceps circumference | 0.867 ± 0.013 |
| Triceps fold | 0.955 ± 0.008 |
| Sub scapula fold | 0.920 ± 0.010 |
| Supra ilium fold | 0.938 ± 0.009 |
| Mid axilla fold | 0.944 ± 0.009 |
| Pectoral fold | 0.946 ± 0.008 |
| Abdominal fold | 0.960 ± 0.007 |
| Quadriceps fold | 0.938 ± 0.008 |
| Skinfolds sum | 0.976 ± 0.006 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mascherini, G.; Petri, C.; Ermini, E.; Bini, V.; Calà, P.; Galanti, G.; Modesti, P.A. Overweight in Young Athletes: New Predictive Model of Overfat Condition. Int. J. Environ. Res. Public Health 2019, 16, 5128. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245128
Mascherini G, Petri C, Ermini E, Bini V, Calà P, Galanti G, Modesti PA. Overweight in Young Athletes: New Predictive Model of Overfat Condition. International Journal of Environmental Research and Public Health. 2019; 16(24):5128. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245128
Chicago/Turabian StyleMascherini, Gabriele, Cristian Petri, Elena Ermini, Vittorio Bini, Piergiuseppe Calà, Giorgio Galanti, and Pietro Amedeo Modesti. 2019. "Overweight in Young Athletes: New Predictive Model of Overfat Condition" International Journal of Environmental Research and Public Health 16, no. 24: 5128. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245128