Comparability of ActivPAL-Based Estimates of Meeting Physical Activity Guidelines for Preschool Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. activPAL Measures and Data Reduction
2.3. Anthropometric and Other Variables
2.4. Data Analysis
3. Results
3.1. Characteristics of the Participants
3.2. TPA, Daily Steps, and MVPA Derived from Counts and Step Rate
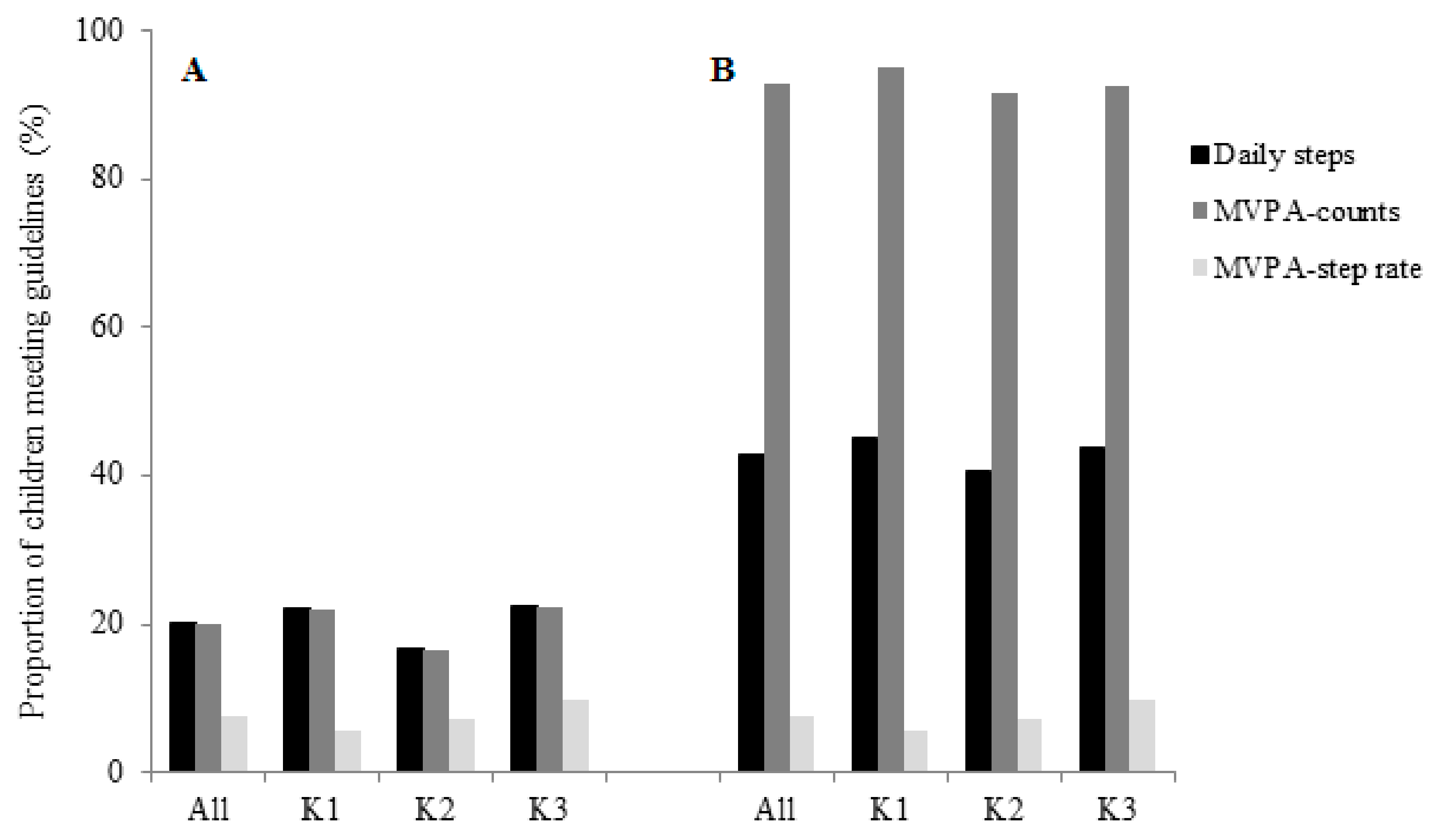
3.3. Agreement across the Three Methods (Daily Steps, MVPA Derived from Counts, and MVPA Derived from Step Rate) in Terms of Meeting the WHO PA Guidelines
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children Under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Dowd, K.P.; Harrington, D.M.; Bourke, A.K.; Nelson, J.; Donnelly, A.E. The measurement of sedentary patterns and behaviors using the activPAL Professional physical activity monitor. Physiol. Meas. 2012, 33, 1887–1899. [Google Scholar] [CrossRef] [PubMed]
- Dowd, K.P.; Harrington, D.M.; Donnelly, A.E. Criterion and concurrent validity of the activPAL professional physical activity monitor in adolescent females. PLoS ONE 2012, 7, e47633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyden, K.; Kozey Keadle, S.L.; Staudenmayer, J.W.; Freedson, P.S. Validity of two wearable monitors to estimate breaks from sedentary time. Med. Sci. Sports Exerc. 2012, 44, 2243–2252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Huang, W.Y.; Yu, J.J.; Sheridan, S.; Sit, C.H.; Wong, S.H. Compliance and Practical Utility of Continuous Wearing of activPAL in Adolescents. Pediatr. Exerc. Sci. 2019, 31, 363–369. [Google Scholar] [CrossRef]
- Sherry, A.P.; Pearson, N.; Ridgers, N.D.; Barber, S.E.; Bingham, D.D.; Nagy, L.C.; Clemes, S.A. activPAL-measured sitting levels and patterns in 9–10 years old children from a UK city. J. Public Health 2018, 1–8. [Google Scholar] [CrossRef]
- van Loo, C.M.; Okely, A.D.; Batterham, M.J.; Hinkley, T.; Ekelund, U.; Brage, S.; Reilly, J.J.; Jones, R.A.; Janssen, X.; Cliff, D.P. Validation of thigh-based accelerometer estimates of postural allocation in 5–12 year-olds. J. Sci. Med. Sport 2017, 20, 273–277. [Google Scholar] [CrossRef] [Green Version]
- Aminian, S.; Hinckson, E.A. Examining the validity of the ActivPAL monitor in measuring posture and ambulatory movement in children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 119. [Google Scholar] [CrossRef] [Green Version]
- Edwardson, C.L.; Winkler, E.A.H.; Bodicoat, D.H.; Yates, T.; Davies, M.J.; Dunstan, D.W.; Healy, G.N. Considerations when using the activPAL monitor in field-based research with adult populations. J. Sport Health Sci. 2017, 6, 162–178. [Google Scholar] [CrossRef] [Green Version]
- Janssen, X.; Cliff, D.P.; Reilly, J.J.; Hinkley, T.; Jones, R.A.; Batterham, M.; Ekelund, U.; Brage, S.; Okely, A.D. Validation and calibration of the activPAL for estimating METs and physical activity in 4-6 year olds. J. Sci. Med. Sport 2014, 17, 602–606. [Google Scholar] [CrossRef] [Green Version]
- Ellis, Y.G.; Cliff, D.P.; Janssen, X.; Jones, R.A.; Reilly, J.J.; Okely, A.D. Sedentary time, physical activity and compliance with IOM recommendations in young children at childcare. Prev. Med. Rep. 2017, 7, 221–226. [Google Scholar] [CrossRef]
- van Loo, C.M.; Okely, A.D.; Batterham, M.; Hinkley, T.; Ekelund, U.; Brage, S.; Reilly, J.J.; Peoples, G.E.; Jones, R.; Janssen, X.; et al. Predictive Validity of a Thigh-Worn Accelerometer METs Algorithm in 5- to 12-Year-old Children. J. Phys. Act. Health 2016, 13, S78–S83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paltechnologies Activpal Operating Guide. Available online: http://www.paltechnologies.com/ (accessed on 30 July 2019).
- Harrington, D.M.; Welk, G.J.; Donnelly, A.E. Validation of MET estimates and step measurement using the ActivPAL physical activity logger. J. Sports Sci. 2011, 29, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Lyden, K.; Keadle, S.K.; Staudenmayer, J.; Freedson, P.S. The activPALTM Accurately Classifies Activity Intensity Categories in Healthy Adults. Med. Sci. Sports Exerc. 2017, 49, 1022–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, D.M.; Dowd, K.P.; Tudor-Locke, C.; Donnelly, A.E. A steps/minute value for moderate intensity physical activity in adolescent females. Pediatr. Exerc. Sci. 2012, 24, 399–408. [Google Scholar] [CrossRef] [Green Version]
- Tudor-Locke, C.; Craig, C.L.; Beets, M.W.; Belton, S.; Cardon, G.M.; Duncan, S.; Hatano, Y.; Lubans, D.R.; Olds, T.S.; Raustorp, A.; et al. How many steps/day are enough? for children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 78. [Google Scholar] [CrossRef] [Green Version]
- De Craemer, M.; De Decker, E.; De Bourdeaudhuij, I.; Verloigne, M.; Manios, Y.; Cardon, G. The translation of preschoolers’ physical activity guidelines into a daily step count target. J. Sports Sci. 2015, 33, 1051–1057. [Google Scholar] [CrossRef]
- Vale, S.; Trost, S.G.; Duncan, M.J.; Mota, J. Step based physical activity guidelines for preschool-aged children. Prev. Med. 2015, 70, 78–82. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Coyle, J.; Kelly, L.; Burke, G.; Grant, S.; Paton, J.Y. An objective method for measurement of sedentary behavior in 3- to 4-year olds. Obes. Res. 2003, 11, 1155–1158. [Google Scholar] [CrossRef]
- Lee, L.F.R.; Dall, P.M. Concurrent agreement between ActiGraph and activPAL in measuring moderate to vigorous intensity physical activity for adults. Med. Eng. Phys. 2019, 74, 82–88. [Google Scholar] [CrossRef]
- Department of Health, The Government of the Hong Kong Special Administrative Region. Physical Activity Guideline for Children Aged 2 to 6; Department of Health, The Government of the Hong Kong Special Administrative Region: Hong Kong, China, 2018.
- Dowd, K.P.; Harrington, D.M.; Hannigan, A.; Donnelly, A.E. Light-Intensity Physical Activity Is Associated with Adiposity in Adolescent Females. Med. Sci. Sports Exerc. 2014, 46, 2295–2300. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.Y.; Wong, S.H. Time use clusters in children and their associations with sociodemographic factors. J. Public Health 2016, 38, e106–e113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Almeida, M.J.; McIver, K.L.; Pfeiffer, K.A.; Dowda, M. Validation and calibration of an accelerometer in preschool children. Obesity 2006, 14, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberghe, E.; Labarque, V.; Trost, S.G.; de Bourdeaudhuij, I.; Cardon, G. Calibration and comparison of accelerometer cut points in preschool children. Int. J. Pediatr. Obes. 2011, 6, e582–e589. [Google Scholar] [CrossRef] [PubMed]
- Gabel, L.; Proudfoot, N.A.; Obeid, J.; MacDonald, M.J.; Bray, S.R.; Cairney, J.; Timmons, B.W. Step count targets corresponding to new physical activity guidelines for the early years. Med. Sci. Sports Exerc. 2013, 45, 314–318. [Google Scholar] [CrossRef]
- Huang, W.Y.; Wong, S.H.; Wong, M.C.; Sit, C.H.; Sum, R.K.; He, G. Results From Hong Kong’s 2016 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2016, 13, S169–S175. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Ezeugwu, V.E.; Tamana, S.K.; Chikuma, J.; Lefebvre, D.L.; Azad, M.B.; Moraes, T.J.; Subbarao, P.; Becker, A.B.; Turvey, S.E.; et al. Associations between meeting the Canadian 24-Hour Movement Guidelines for the Early Years and behavioral and emotional problems among 3-year-olds. J. Sci. Med. Sport 2019, 22, 797–802. [Google Scholar] [CrossRef]
- De Craemer, M.; McGregor, D.; Androutsos, O.; Manios, Y.; Cardon, G. Compliance with 24-h Movement Behaviour Guidelines among Belgian Pre-School Children: The ToyBox-Study. Int. J. Environ. Res. Public Health 2018, 15, 2171. [Google Scholar] [CrossRef] [Green Version]
- Brandes, M.; Steenbock, B.; Wirsik, N. Energy Cost of Common Physical Activities in Preschoolers. J. Phys. Act. Health 2018, 15, 233–238. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Schuna, J.M., Jr.; Han, H.; Aguiar, E.J.; Larrivee, S.; Hsia, D.S.; Ducharme, S.W.; Barreira, T.V.; Johnson, W.D. Cadence (steps/min) and intensity during ambulation in 6-20 year olds: the CADENCE-kids study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Dall, P.M.; McCrorie, P.R.; Granat, M.H.; Stansfield, B.W. Step accumulation per minute epoch is not the same as cadence for free-living adults. Med. Sci. Sports Exerc. 2013, 45, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Han, H.; Aguiar, E.J.; Barreira, T.V.; Schuna, J.M., Jr.; Kang, M.; Rowe, D.A. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: A narrative review. Br. J. Sports Med. 2018, 52, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Rose-Jacobs, R. Development of gait at slow, free, and fast speeds in 3- and 5-year-old children. Phys. Ther. 1983, 63, 1251–1259. [Google Scholar] [CrossRef] [Green Version]
- Dobell, A.P.; Eyre, E.L.J.; Tallis, J.; Chinapaw, M.J.M.; Altenburg, T.M.; Duncan, M.J. Examining accelerometer validity for estimating physical activity in pre-schoolers during free-living activity. Scand. J. Med. Sci. Sports 2019, 29, 1618–1628. [Google Scholar] [CrossRef]
- Hagenbuchner, M.; Cliff, D.P.; Trost, S.G.; Van Tuc, N.; Peoples, G.E. Prediction of activity type in preschool children using machine learning techniques. J. Sci. Med. Sport 2015, 18, 426–431. [Google Scholar] [CrossRef]
- Cliff, D.P.; Reilly, J.J.; Okely, A.D. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J. Sci. Med. Sport 2009, 12, 557–567. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Whole Sample (n = 149) | Analytical Sample (n = 114) |
|---|---|---|
| Sex (% boys) | 60.4 | 61.4 |
| Age (years) | 4.9 (0.8) | 4.9 (0.8) |
| Body mass index, BMI (kg⋅m2) | 15.5 (1.7) | 15.3 (1.5) |
| Number of valid wear days | 3.8 (2.6) | 4.8 (2.0) |
| Sex of responding parent (% mother) | 74.8 | 70.8 |
| Parental age (years) | 36.9 (7.0) | 36.7 (7.2) |
| Parental education (%) | ||
| Lower secondary or less | 27.3 | 25.0 |
| Completed secondary | 46.5 | 47.9 |
| Tertiary | 27.2 | 27.1 |
| Variables | TPA (Hour/Day) | Daily Steps (Steps/Day) | MVPA-Counts (Hour/Day) | MVPA-Step Rate (Hour/Day) |
|---|---|---|---|---|
| All | 2.33 (0.75) | 10,691 (3894) | 1.95 (0.72) | 0.47 (0.31) |
| Sex | ||||
| Boys | 2.35 (0.79) | 10,754 (4123) | 1.98 (0.77) | 0.47 (0.33) |
| Girls | 2.29 (0.69) | 10,597 (3526) | 1.90 (0.65) | 0.48 (0.27) |
| Grade | ||||
| K1 | 2.38 (0.74) | 10,739 (3795) | 2.14 (0.72) | 0.44 (0.28) |
| K2 | 2.28 (0.75) | 10,565 (3828) | 1.86 (0.71) * | 0.48 (0.29) |
| K3 | 2.34 (0.76) | 10,794 (4051) | 1.90 (0.72) * | 0.50 (0.34) |
| Body weight status | ||||
| Non-overweight | 2.33 (0.75) | 10,713 (3913) | 1.95 (0.73) | 0.47 (0.30) |
| Overweight | 2.19 (0.75) | 10,350 (3743) | 1.86 (0.69) | 0.52 (0.37) |
| Variables | TPA (Hour/Day) | Daily Steps (Steps/Day) | MVPA-Counts (Hour/Day) | MVPA-Step Rate (Hour/Day) |
|---|---|---|---|---|
| TPA (hour/day) | - | 0.957 | 0.948 | 0.733 |
| Daily steps (steps/day) | - | - | 0.920 | 0.869 |
| MVPA-counts (hour/day) | - | - | - | 0.726 |
| Variables | Daily Steps vs. MVPA-Counts | Daily Steps vs. MVPA-Step Rate | MVPA-Counts vs. MVPA-Step Rate |
|---|---|---|---|
| All | 1.00 | 0.41 (0.31, 0.51) | 0.41 (0.31, 0.51) |
| Grade | |||
| K1 | 1.00 | 0.23 (0.06, 0.41) | 0.23 (0.06, 0.41) |
| K2 | 1.00 | 0.42 (0.25, 0.60) | 0.42 (0.25, 0.60) |
| K3 | 1.00 | 0.51 (0.36, 0.67) | 0.51 (0.36, 0.67) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.Y.; Lee, E.-Y. Comparability of ActivPAL-Based Estimates of Meeting Physical Activity Guidelines for Preschool Children. Int. J. Environ. Res. Public Health 2019, 16, 5146. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245146
Huang WY, Lee E-Y. Comparability of ActivPAL-Based Estimates of Meeting Physical Activity Guidelines for Preschool Children. International Journal of Environmental Research and Public Health. 2019; 16(24):5146. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245146
Chicago/Turabian StyleHuang, Wendy Yajun, and Eun-Young Lee. 2019. "Comparability of ActivPAL-Based Estimates of Meeting Physical Activity Guidelines for Preschool Children" International Journal of Environmental Research and Public Health 16, no. 24: 5146. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245146