Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Introduction to the PAHCO Model
1.2. Distinguishing the Two Facets of Control Competence
1.3. From Basic Elements, via Control Competence, to Health Outcomes
1.4. Aims and Hypotheses
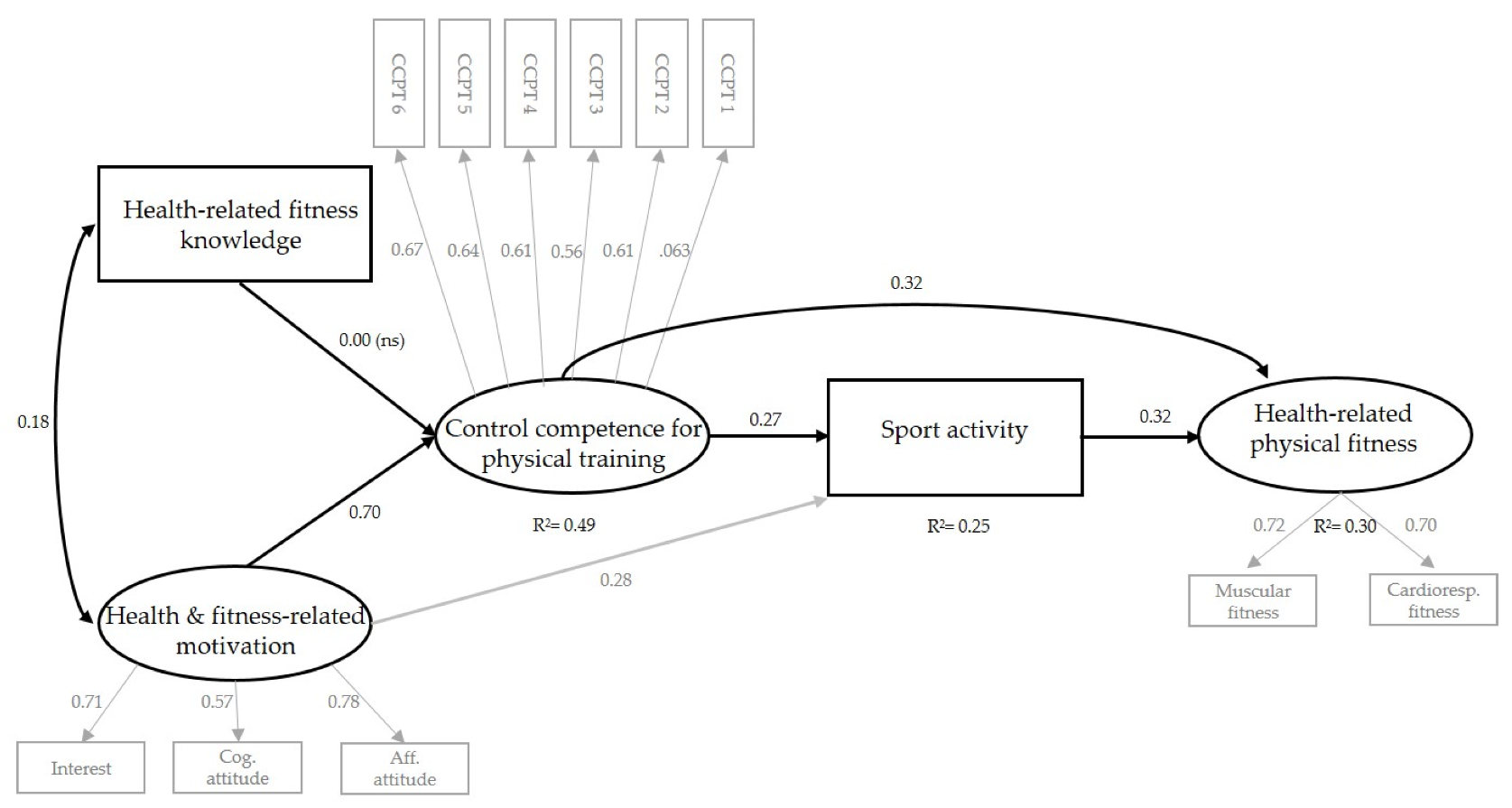
- (1)
- Domain-specific knowledge and domain-specific motivation are positively associated with control competence for physical training.
- (2)
- Control competence for physical training mediates the association between domain-specific knowledge and domain-specific motivation and sport activity.
- (3)
- Control competence for physical training is related to health-related physical fitness, controlled for the level of sport activity.
2. Methods
2.1. Participants and Procedure
2.1.1. Study A
2.1.2. Study B
2.2. Data Collection
2.3. Measures
2.3.1. Facets of Control Competence (Studies A and B)
2.3.2. Domain-Specific Knowledge (Study B)
2.3.3. Domain-Specific Motivation (Study B)
2.3.4. Sport Activity (Study B)
2.3.5. Health-Related Physical Fitness (Study B)
2.4. Statistical Analyses
3. Results
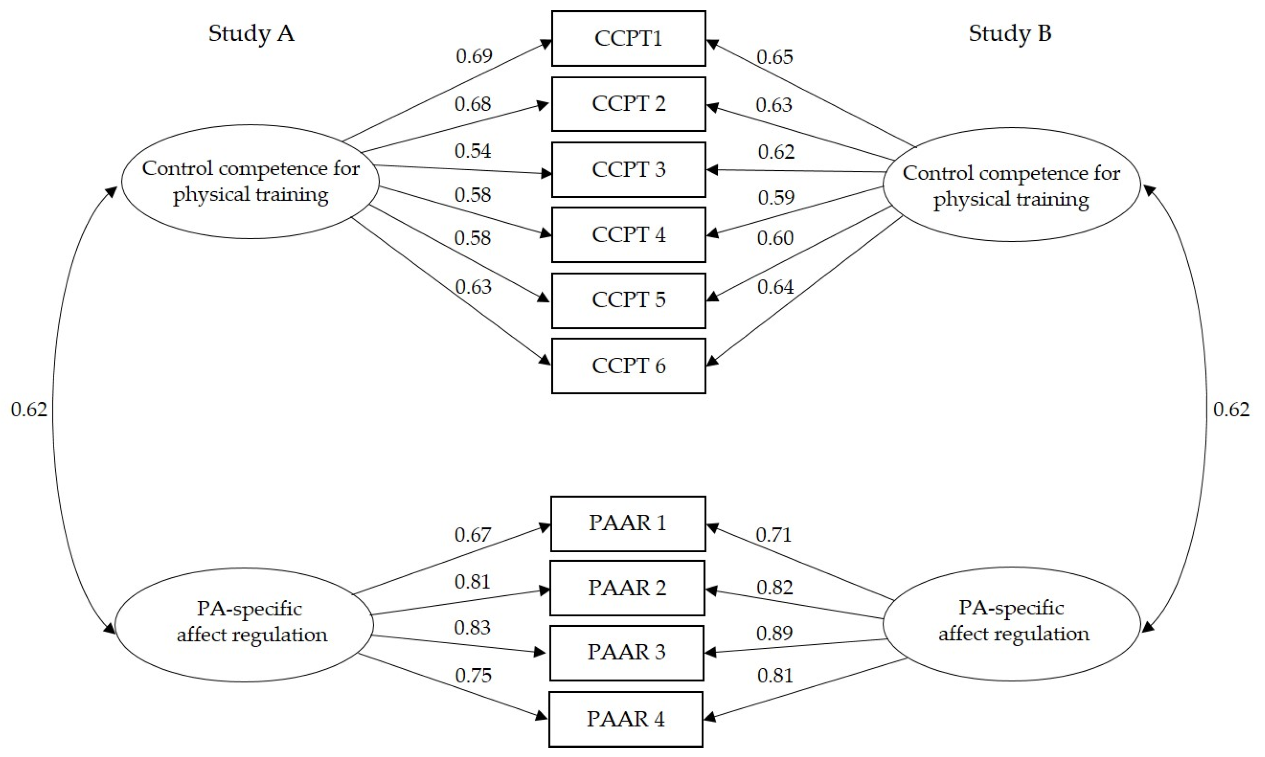
3.1. Confirmatory Factor Analysis of Control Competence
3.2. Path Model for Control Competence for Physical Training
4. Discussion
4.1. Distinguishing the Two Facets of Control Competence
4.2. Associations between Basic Elements, Control Competence for Physical Training, Sport Activity, and Health-Related Physical Fitness
4.2.1. Basic Elements, Control Competence for Physical Training, and Sport Activity
4.2.2. Control Competence, Sport Activity, and Health-Related Physical Fitness
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef] [PubMed]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, 197–239. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvenalo, M.; Tammelin, T.; Viikari, J.S.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exercise 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longmuir, P.E.; Tremblay, M. Top 10 Research Questions Related to Physical Literacy. Res. Q. Exerc. Sport 2016, 87, 28–35. [Google Scholar] [CrossRef]
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; HLS-EU. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Soellner, R.; Huber, S.; Lenartz, N.; Rudinger, G. Gesundheitskompetenz—Ein vielschichtiger Begriff [Health literacy—A complex term]. Z. Gesundheitspsychol. 2009, 17, 105–113. [Google Scholar] [CrossRef]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent health literacy and health behaviors: A systematic review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef]
- Edwards, L.C.; Bryant, A.S.; Keegan, R.J.; Morgan, K.; Jones, A.M. Definitions, foundations and associations of physical literacy: A systematic review. Sports Med. 2017, 47, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Costas-Bradstreet, C.; Barnes, J.D.; Bartlett, B.; Dampier, D.; Lalonde, C.; Leidl, R.; Longmuir, P.; McKee, M.; Patton, R.; et al. Canada’s Physical Literacy Consensus Statement: Process and outcome. BMC Public Health 2018, 18. [Google Scholar] [CrossRef]
- International Physical Literacy Association. Physical Literacy Definition. Available online: https://www.physical-literacy.org.uk/ (accessed on 18 October 2019).
- Tremblay, M.S.; Lloyd, M. Physical literacy measurement—The missing piece. Phys. Health Educ. 2010, 76, 26–30. [Google Scholar]
- Whitehead, M. Physical Literacy throughout the Lifecourse; Routledge: London, UK, 2010. [Google Scholar]
- Dudley, D.; Cairney, J.; Wainwright, N.; Kriellaars, D.; Mitchell, D. Critical considerations for physical literacy policy in public health, recreation, sport, and education agencies. Quest 2017, 69, 436–452. [Google Scholar] [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical literacy, physical activity and health: Toward an evidence-informed conceptual model. Sports Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Sudeck, G.; Pfeifer, K. Physical activity-related health competence as an integrative objective in exercise therapy and health sports—Conception and validation of a short questionnaire. Sportwissenschaft 2016, 46, 74–87. [Google Scholar] [CrossRef]
- Thiel, C.; Pfeifer, K.; Sudeck, G. Pacing and perceived exertion in endurance performance in exercise therapy and health sports. Ger. J. Exerc. Sport Res. 2018, 48, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Klieme, E.; Hartig, J.; Rauch, D. The concept of competence in educational contexts. In Assessment of Competencies in Eeducational Contexts; Hartig, J., Klieme, E., Leutner, D., Eds.; Hogrefe Publishing GmbH: Göttingen, Germany, 2008; pp. 3–22. [Google Scholar]
- Weinert, F.E. Concept of competence: A conceptual clarification. In Defining and Selecting Key Competencies; Rychen, D.S., Salganik, L.H., Eds.; Hogrefe & Huber: Seattle, WA, USA, 2001; pp. 45–65. [Google Scholar]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J. Appl. Soc. Psych. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Baartman, L.; de Bruijn, E. Integrating knowledge, skills and attitudes: Conceptualising learning processes towards vocational competence. Educ. Res. Rev. 2011, 6, 125–134. [Google Scholar] [CrossRef]
- Lenartz, N. Gesundheitskompetenz und Selbstregulation. Health Competence and Self-Regulation; Bonn University Press: Bonn, Germany, 2011. [Google Scholar]
- Franke, A. Modelle von Gesundheit und Krankheit [Models of health and illness], 2nd ed.; Verlag Hans Huber: Bern, Switzerland, 2010. [Google Scholar]
- Bryan, A.D.; Magnan, R.E.; Nilsson, R.; Marcus, B.H.; Tompkins, S.A.; Hutchison, K.E. The big picture of individual differences in physical activity behavior change: A transdisciplinary approach. Psychol. Sport Exerc. 2011, 12, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Ekkekakis, P.; Parfitt, G.; Petruzzello, S. The pleasure and displeasure people feel when they exercise at different intensities: Decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Med. 2011, 41, 641–671. [Google Scholar] [CrossRef]
- Sudeck, G.; Jeckel, S.; Schubert, T. Individual differences in the competence for physical-activity-related affect regulation moderate the activity–affect association in real-life situations. J. Sport Exerc. Psychol. 2018, 40, 196–205. [Google Scholar] [CrossRef]
- Ennis, C.D. Knowledge, transfer, and innovation in physical literacy curricula. J. Sport Health Sci. 2015, 4, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAuley, E.; Blissmer, B. Self-efficacy determinants and consequences of physical activity. Exerc. Sport Sci. Rev. 2000, 28, 85–88. [Google Scholar] [PubMed]
- Chen, A. Operationalizing physical literacy for learners: Embodying the motivation to move. J. Sport Health Sci. 2015, 4, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Shi, Y.; Zeng, Q.; Wang, Y.; Du, W.; Wei, N.; Xie, R.; Chang, C. Determinants of health literacy and health behavior regarding infectious respiratory diseases: A pathway model. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paakkari, L.T.; Torppa, M.P.; Paakkari, O.-P.; Välimaa, R.S.; Ojala, K.S.; Tynjälä, J.A. Does health literacy explain the link between structural stratifiers and adolescent health? Eur. J. Public Health 2019. [Google Scholar] [CrossRef]
- Fuchs, R.; Klaperski, S.; Gerber, M.; Seelig, H. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen. Eine methodische Zwischenbilanz. [Measurement of physical activity and sport activity with the BSA questionnaire]. Z. Gesundheitspsychol. 2015, 23, 60–76. [Google Scholar] [CrossRef]
- Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Trautwein, U.; Sudeck, G. Promotion of physical activity-related health competence in physical education: Study protocol for the GEKOS cluster randomized controlled trial. BMC Public Health 2019, 19. [Google Scholar] [CrossRef]
- Volk, C.; Haible, S.; Demetriou, Y.; Thiel, A.; Wagner, W.; Sudeck, G.; Höner, O. Health-related fitness knowledge in adolescence: Development and evaluation of a test considering different methodological approaches. manuscript submitted.
- Warm, T.A. Weighted likelihood estimation of ability in item response theory. Psychometrika 1989, 54, 427–450. [Google Scholar] [CrossRef]
- Demetriou, Y. Health Promotion in Physical Education. Development and Evaluation of the Eight Week PE Programme “HealthyPEP” for Sixth Grade Students in Germany; Czwalina: Hamburg, Germany, 2013. [Google Scholar]
- Organisation for Economic Co-operation and Development. PISA 2006 Technical Report; OECD Publishing: Paris, France, 2009. [Google Scholar]
- Cattuzzo, M.T.; dos Santos Henrique, R.; Ré, A.H.N.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Montoro-Escaño, J.; Merino-Marban, R.; Viciana, J. Effects of a physical education-based programme on health-related physical fitness and its maintenance in high school students: A cluster-randomized controlled trial. Eur. Phys. Ed. Rev. 2016, 22, 243–259. [Google Scholar] [CrossRef]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe. Eurofit: Handbook for the Eurofit Tests of Physical Fitness; Council of Europe: Rome, Italy, 1988. [Google Scholar]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; LeBlanc, A.G.; Belanger, K.; Ortega, F.B.; Léger, L. International normative 20 m shuttle run values from 1, 142, 026 children and youth representing 50 countries. Br. J. Sports Med. 2017, 51, 1545–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woll, A.; Kurth, B.M.; Opper, E.; Worth, A.; Bös, K. The ‘Motorik-Modul’ (MoMo): Physical fitness and physical activity in german children and adolescents. Eur. J. Pediatr. 2011, 170, 1129–1142. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Bagozzi, R.; Yi, Y. Specification, evaluation, and interpretation of structural equation models. J. Acad. Mark. Sci. 2012, 40, 8–34. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- West, S.G.; Finch, J.F.; Curran, P.J. Structural equation models with nonnormal variables: Problems and remedies. In Structural Equation Modeling: Concepts, Issues, and Applications; Hoyle, R.H., Ed.; Sage: Thousand Oaks, CA, USA, 1995; pp. 56–75. [Google Scholar]
- Fisher, J.D.; Fisher, W.A.; Amico, K.R.; Harman, J.J. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006, 25, 462–473. [Google Scholar] [CrossRef]
- Kelly, S.; Melnyk, B.M.; Belyea, M. Predicting physical activity and fruit and vegetable intake in adolescents: A test of the information, motivation, behavioral skills model. Res. Nurs. Health 2012, 35, 146–163. [Google Scholar] [CrossRef]
- Schön, D. The Reflective Practitioner; Maurice Temple Smith Ltd.: London, UK, 1983. [Google Scholar]
- Demetriou, Y.; Sudeck, G.; Thiel, A.; Höner, O. The effects of school-based physical activity interventions on students’ health-related fitness knowledge: A systematic review. Educ. Res. Rev. 2015, 16, 19–40. [Google Scholar] [CrossRef]
- Ajzen, I.; Joyce, N.; Sheikh, S.; Cote, N.G. Knowledge and the prediction of behavior: The role of information accuracy in the theory of planned behavior. Basic Appl. Soc. Psych. 2011, 33, 101–117. [Google Scholar] [CrossRef]
- Edwards, L.C.; Bryant, A.S.; Keegan, R.J.; Morgan, K.; Cooper, S.-M.; Jones, A.M. ‘Measuring’ physical literacy and related constructs: A systematic review of empirical findings. Sports Med. 2018, 48, 659–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garfinkel, S.N.; Seth, A.K.; Barrett, A.B.; Suzuki, K.; Critchley, H.D. Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 2015, 104, 65–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quennerstedt, M. Physical education and the art of teaching: Transformative learning and teaching in physical education and sports pedagogy. Sport Educ. Soc. 2019, 24, 611–623. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Models | χ2 | p(df) | χ2/df | CFI | RMSEA | 90% CI | SRMR |
|---|---|---|---|---|---|---|---|
| Study A: 1 factor | 421.58 | <0.001 (35) | 12.05 | 0.82 | 0.12 | 0.11, 0.13 | 0.08 |
| Study A: 2 factors | 67.78 | <0.001 (34) | 1.99 | 0.98 | 0.04 | 0.02, 0.05 | 0.03 |
| Study B: 1 factor | 510.50 | <0.001 (35) | 14.59 | 0.83 | 0.13 | 0.12, 0.14 | 0.09 |
| Study B: 2 factors | 74.09 | <0.001 (34) | 2.18 | 0.99 | 0.04 | 0.03, 0.05 | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Sudeck, G. Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 39. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010039
Haible S, Volk C, Demetriou Y, Höner O, Thiel A, Sudeck G. Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(1):39. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010039
Chicago/Turabian StyleHaible, Stephanie, Carmen Volk, Yolanda Demetriou, Oliver Höner, Ansgar Thiel, and Gorden Sudeck. 2020. "Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents" International Journal of Environmental Research and Public Health 17, no. 1: 39. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010039