Horticultural Therapy Program for People with Mental Illness: A Mixed-Method Evaluation


Abstract
:1. Introduction
2. Materials and Methods
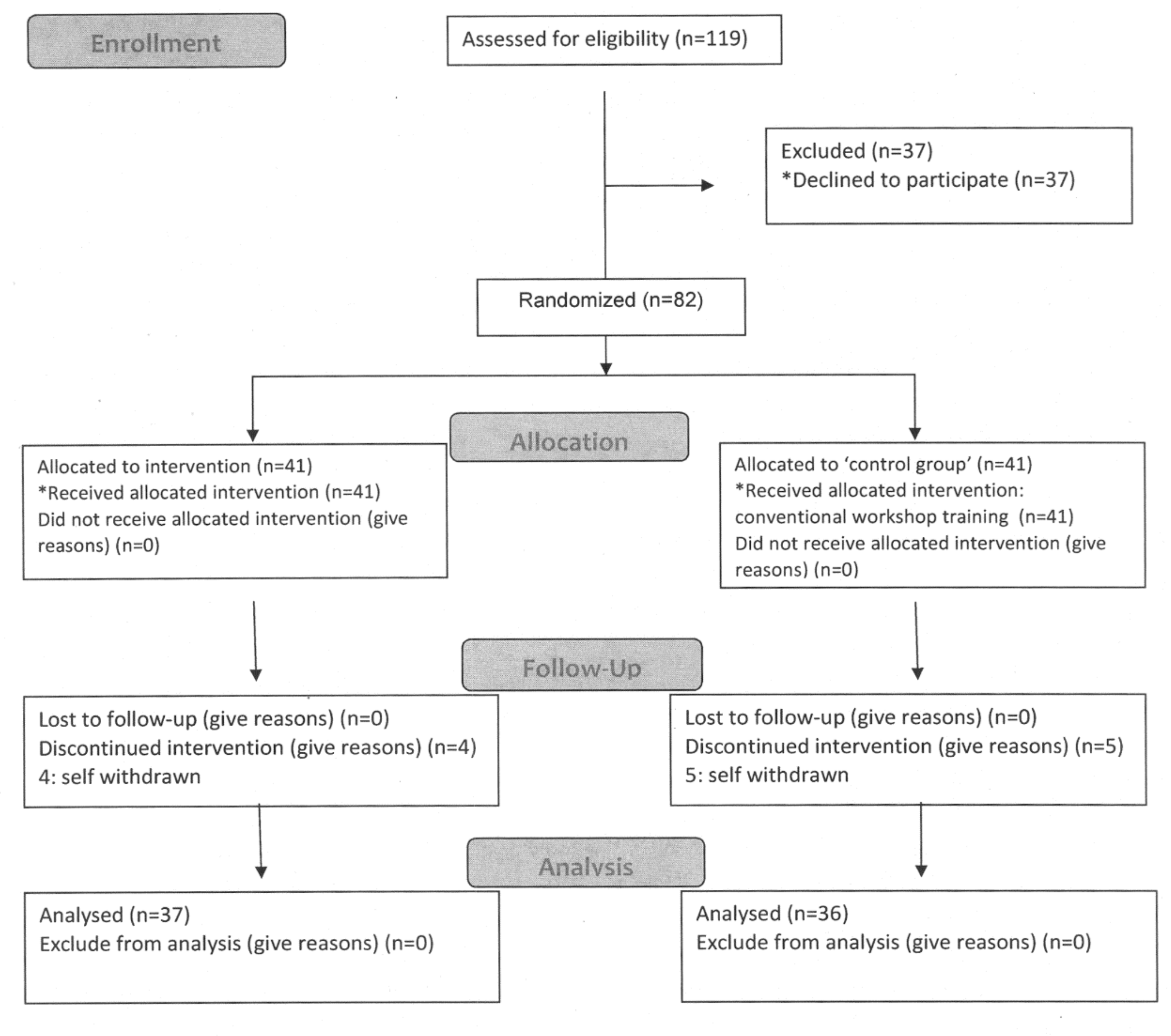
2.1. Participants
2.2. Horticultural Therapy Program
2.3. Instruments
2.4. Procedures
2.5. Focus Group Evaluation
2.6. Quantitative Data Analysis
2.7. Qualitative Data Analysis
3. Results
3.1. Profile of Participants
3.2. Quantitative Evaluation
3.3. Focus Group Evaluation
4. Discussion
4.1. Outcomes and Processes of Horticultural Therapy
4.2. Contributions and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Horticultural Therapy Association. American Horticultural Therapy Association Definitions and Positions. 2012. Available online: http://ahta.org/sites/default/files/DefinitionsandPositions.pdf (accessed on 1 December 2018).
- Relf, P.D. Theoretical models for research and program development in agriculture and health care. In Farming for Health; Hassink, J., VanDijk, M., Eds.; Springer: Dordrecht, The Netherlands, 2006; pp. 1–20. [Google Scholar]
- Clatworthy, J.; Hinds, J.; MCamic, P. Gardening as a mental health intervention: A review. Ment. Health Rev. J. 2013, 18, 214–225. [Google Scholar] [CrossRef]
- Sempik, J.; Aldridgem, J.; Becker, S. Social and Therapeutic Horticulture: Evidence and Messages from Research; Centre for Child and Family Research, Loughborough University: Loughborough, UK, 2003. [Google Scholar]
- Eling, M. People-plant interaction: The physiological, psychological and sociological effects of plants on people. In Farming for Health; Hassink, J., VanDijk, M., Eds.; Springer: Dordrecht, The Netherlands, 2006; pp. 43–55. [Google Scholar]
- Parkinson, S.; Lowe, C.; Vecsey, T. The therapeutic benefits of horticulture in a mental health service. Br. J. Occup. Ther. 2011, 74, 525–534. [Google Scholar] [CrossRef]
- Han, A.R.; Park, S.A.; Ahn, B.E. Reduced stress and improved physical functional ability in elderly with mental health problems following a horticultural therapy program. Complementary Ther. Med. 2018, 38, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Kam, M.C.Y.; Siu, A.M.H. Evaluation of a horticultural activity programme for persons with psychiatric illness. Hong Kong J. Occup. Ther. 2010, 20, 80–86. [Google Scholar] [CrossRef]
- Wichrowski, M.; Whiteson, J.; Haas, F.; Mola, A.; Rey, M.J. Effects of horticultural therapy on mood and heart rate in patients participating in an inpatient cardiopulmonary rehabilitation program. J. Cardiopulm. Rehabil. Prev. 2005, 25, 270–274. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Fjeld, T.; Veiersted, B.; Sandvik, L.; Riise, G.; Levy, F. The effect of indoor foliage plants on health and discomfort symptoms among office workers. Indoor Built Environ. 1998, 7, 204–209. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989; pp. 177–200. [Google Scholar]
- Wiesinger, G.; Neuhauser, F.; Putz, M. Farming for health in Austrian Farms, horticultural therapy, animal-assisted therapy. In Farming for Health: Green-Care Farming Across Europe and the United States of America; Hassink, J., Dijk, M., Eds.; Springer: Dordrecht, The Netherlands, 2006; pp. 233–248. [Google Scholar]
- Perrins-Margalis, N.M.; Rugletic, J.; Schepis, N.M.; Stepanski, H.R.; Walsh, M.A. The immediate effects of a group-based horticulture experience on the quality of life of persons with chronic mental illness. Occup. Ther. Ment. Health 2000, 16, 15–32. [Google Scholar] [CrossRef]
- Diamant, E.; Waterhouse, A. Gardening and belonging: Reflections on how social and therapeutic horticulture may facilitate health, wellbeing and inclusion. Br. J. Occup. Ther. 2010, 73, 84–88. [Google Scholar] [CrossRef]
- Gonzalez, M.T.; Hartig, T.; Patil, G.G.; Martinsen, E.W.; Kirkevold, M. A prospective study of group cohesiveness in therapeutic horticulture for clinical depression. Int. J. Ment. Health Nurs. 2011, 20, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Lohr, V.I.; Pearson-Mims, C.H.; Goodwin, G.K. Interior plants may improve worker productivity and reduce stress in windowless environments. J. Environ. Hortic. 1996, 14, 97–100. [Google Scholar]
- Best, L.J.; Still, M.; Cameron, G. Supported education: Enabling course completion for people experiencing mental illness. Aust. Occup. Ther. J. 2008, 55, 65–68. [Google Scholar] [CrossRef]
- Kamioka, H.; Tsutani, K.; Yamada, M.; Park, H.; Okuizumi, H.; Honda, T.; Okada, S.; Park, S.J.; Kitayuguchi, J.; Abe, T.; et al. Effectiveness of horticultural therapy: A systematic review of randomized controlled trials. Complementary Ther. Med. 2014, 22, 930–943. [Google Scholar] [CrossRef] [PubMed]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.; Bradley, A.J. Horticultural therapy for schizophrenia. Cochrane Database Syst. Rev. 2011, 11, CD009413. [Google Scholar] [CrossRef]
- New Life Psychiatric Rehabilitation Association. Annual Report of New Life Psychiatric Rehabilitation Association; New Life Psychiatric Rehabilitation Association: Hong Kong, China, 2014. [Google Scholar]
- Cipriani, J.; Benz, A.; Holmgren, A.; Kinter, D.; McGarry, J.; Rufino, G. A systematic review of the effects of horticultural therapy on persons with mental health conditions. Occup. Ther. Ment. Health 2017, 33, 47–69. [Google Scholar] [CrossRef]
- Shorten, A.; Smith, J. Mixed methods research: Expanding the evidence base. Evid. Based Nurs. 2017, 74–75. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.B.; Onwuegbuzie, A.J.; Turner, L.A. Toward a definition of mixed methods research. J. Mix. Methods Res. 2007, 1, 112–133. [Google Scholar] [CrossRef]
- Hintze, J. PASS 12; NCSS, LLC: Kaysville, UT, USA, 2013; Available online: www.ncss.com (accessed on 1 December 2018).
- Olszowy, D.R. Horticulture for the Disabled: Principles of Horticultural Therapy; Thomas: Springfield, IL, USA, 1978; pp. 9–43. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Taouk, M.; Lovibond, P.F.; Laube, R. Psychometric Properties of a Chinese Version of the Short Depression Anxiety Stress Scales (DASS21) (Report for New South Wales Transcultural Mental Health Centre); Cumberland Hospital: Sydney, Australia, 2001. [Google Scholar]
- Brown, S.S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, S.S.W.; Lo, A.W.Y.; Leung, T.K.S.; Chan, F.S.M.; Wong, A.T.Y.; Lam, R.W.T.; Tsang, D.K.Y. Translation and validation of the Chinese version of the Short Warwick-Edinburgh Mental Well-Being Scale for Patients with Mental Illness in Hong Kong. East Asian Arch. Psychiatry 2014, 24, 3–9. [Google Scholar] [PubMed]
- Eakman, A.M.; Carlson, M.; Clark, F. The Meaningful Activity Participation Assessment: A measure of engagement in personally valued activities. Int. J. Aging Hum. Dev. 2010, 70, 299–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, B.; Brintnell, E.S.; Goldberg, J. The relationship between engagement in meaningful activities and quality of life in persons disabled by mental illness. Occup. Ther. Ment. Health 2002, 18, 17–44. [Google Scholar] [CrossRef]
- Gigliotti, C.M.; Jarrott, S. Effects of horticulture therapy on engagement and affect. Can. J. Aging 2005, 24, 367–377. [Google Scholar] [CrossRef]
- Brown, L.D.; Tang, X.; Hollman, R.L. The Structure of social exchange in self-help support groups: Development of a measure. Am. J. Community Psychol. 2014, 53, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Rabiee, F. Focus-group interview and data analysis. Proc. Nutr. Soc. 2004, 63, 655–660. [Google Scholar] [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature based solution for improving mental health and well-being in urban areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [CrossRef]
- Whear, R.; Coon, J.T.; Bethel, A.; Abbott, R.; Stein, K.; Garside, R. What is the impact of using outdoor spaces such as gardens on the physical and mental well-being of those with dementia? A systematic review of quantitative and qualitative evidence. J. Am. Med. Dir. Assoc. 2014, 15, 697–705. [Google Scholar] [CrossRef] [Green Version]
- Noone, S.; Innes, A.; Kelly, F.; Mayers, A. ‘The nourishing soil of the soul’: The role of horticultural therapy in promoting well-being in community-dwelling people with dementia. Dementia 2017, 16, 897–910. [Google Scholar] [CrossRef]
- Detweiler, M.B.; Self, J.A.; Lane, S.; Spencer, L.; Lutgens, B.; Kim, D.Y.; Halling, M.H.; Rudder, T.F.; Lehmann, L. Horticultural therapy: A pilot study on modulating cortisol levels and indices of substance craving, posttraumatic stress disorder, depression, and quality of life in veterans. Altern. Ther. Health Med. 2015, 21, 36–41. [Google Scholar] [PubMed]
- Green, M.F.; Horan, W.P.; Lee, J. Social cognition in schizophrenia. Nat. Rev. Neurosci. 2015, 16, 620. [Google Scholar] [CrossRef] [PubMed]
- Kring, A.M.; Elis, O. Emotion deficits in people with schizophrenia. Annu. Rev. Clin. Psychol. 2013, 9, 409–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sempik, J.; Rickhuss, C.; Beeston, A. The effects of social and therapeutic horticulture on aspects of social behaviour. Br. J. Occup. Ther. 2014, 77, 313–319. [Google Scholar] [CrossRef]


{kind=link}
| Session Title | Session Objectives |
|---|---|
| Growth with Hope: Transplant Sprouting Seedling Activity | To learn and practice transplantation. To share the objectives and expectations of the HT sessions. |
| The Lifecycle of Plants: Propagation by Cutting | To learn and practice propagation skills. To reflect on, appreciate nature, and share thoughts about the vitality of plants. |
| The Lifecycle of Plants (II): Propagation by Division | To learn and practice propagation skills. To reflect on, appreciate nature, and share thoughts about the vitality of plants. |
| Mindful Eating: Tasting Fruits | To experience mindfulness techniques during the activities. To share thoughts about using this experience in mindful eating, and its potential use as a relaxation activity. |
| Live Aroma: Introduction to Herbs | To introduce herbal plants to the users. To learn and practice a diaphragmatic breathing exercise.To share thoughts about the experience of using relaxation methods. |
| Self-Designed Pot Garden: Combination of Plants | To learn to design a pot garden using various plants and decorations. To share thoughts about the feeling of appreciation. |
| Natural Aroma: Herbal Bag Production | To experience the aromas of various kinds of dried natural materials. To revise the diaphragmatic breathing exercise. |
| Harvest Time: Vegetable Harvesting | To practice vegetable harvesting and cooking. To share the symbolic meaning of harvesting.To share overall feedback about the HT sessions. |
| If the therapy setting does not have an outdoor environment for vegetable growth, Sessions 1 and 8 will be changed to sessions entitled “Colorful Nature” and “Colorful World”, described below. | |
| Colorful Nature: Leaf Rubbing | To experience the natural colors of plants through a leaf rubbing exercise. To learn about the characteristics of plants. |
| 8. Colorful World: Pressed Flower Cards | To learn skills using pressed flowers. To share the symbolic meaning of pressed flowers. To share overall feedback about the HT sessions. |
| Variables | Group | χ2 | p | |||
|---|---|---|---|---|---|---|
| Treatment | Comparison | |||||
| n | % | n | % | |||
| Categorical Variables | ||||||
| Gender | ||||||
| Male | 20 | 54.1% | 17 | 45.9% | 0.44 | 0.51 |
| Female | 21 | 46.7% | 24 | 53.3% | ||
| Living Condition | ||||||
| Live with family | 11 | 36.7% | 19 | 63.3% | 8.78 | 0.01 |
| Hostel | 22 | 71.0% | 9 | 29.0% | ||
| Live alone | 8 | 38.1% | 13 | 61.9% | ||
| Diagnosis | ||||||
| Schizophrenia | 30 | 47.6% | 33 | 52.4% | 0.62 | 0.43 |
| Other psychiatric illness | 11 | 57.9% | 8 | 42.1% | ||
| Education | ||||||
| No formal education | 2 | 100.0% | 0 | 0.0% | 2.34 | 0.67 |
| Special education | 1 | 50.0% | 1 | 50.0% | ||
| Primary | 8 | 50.0% | 8 | 50.0% | ||
| Junior secondary | 13 | 44.8% | 16 | 55.2% | ||
| Senior secondary or above | 17 | 51.5% | 16 | 48.5% | ||
| Interval Variables | M | SD | M | SD | t | p |
| Age | 50.8 | 10.5 | 49.7 | 8.7 | 0.51 | 0.61 |
| Years from onset | 25.6 | 11.6 | 24.4 | 9.9 | 0.50 | 0.62 |
| Measures | T1 Pre-Test | T2 Post-Test | T3 Follow Up | Test Statistic | p |
|---|---|---|---|---|---|
| DASS | |||||
| Anxiety subscale | |||||
| Treatment | 0.59 (0.55) | 0.64 (0.54) | 0.72 (0.59) | 1.14 a | 0.29 |
| Comparison | 0.71 (0.47) | 0.79 (0.72) | 0.84 (0.68) | ||
| Stress subscale | |||||
| Treatment | 0.73 (0.66) | 0.71 (0.66) | 0.87 (0.68) | 0.85 | 0.36 |
| Comparison | 0.85 (0.48) | 0.84 (0.65) | 0.96 (0.66) | ||
| C-SWEMWBS | |||||
| Treatment | 3.10 (0.66) | --- | 3.30 (0.73) | 6.50 b | 0.01 |
| Comparison | 3.18 (0.71) | --- | 2.95 (0.70) | ||
| EMAS | |||||
| Treatment | 2.72 (0.62) | 2.74 (0.69) | --- | 3.53 b | 0.06 |
| Comparison | 2.58 (0.69) | 2.40 (0.74) | --- | ||
| AEC | |||||
| Affect | |||||
| Treatment | 0.035 (1.15) | 0.40 (1.07) | --- | 1.05 b | 0.31 |
| Comparison | −0.29 (0.72) | 0.22 (1.00) | --- | ||
| Engagement (%) | |||||
| Treatment | 97.06 (5.67) | 96.16 (7.06) | --- | 12.45 b | 0.001 |
| Comparison | 83.33 (21.91) | 81.00 (18.14) | --- | ||
| SESM | |||||
| Experiential knowledge provided | 2.98 (1.73) | 2.70 (1.72) | --- | 1.12 c | 0.27 |
| Emotional support provided | 3.63 (1.70) | 3.48 (1.63) | --- | 0.70 c | 0.49 |
| Experiential knowledge received | 3.15 (1.63) | 3.29 (1.48) | --- | 0.53 c | 0.60 |
| Emotional support received | 3.61 (1.70) | 3.95 (1.59) | --- | 1.53 c | 0.13 |
| Humor exchanged | 2.32 (1.64) | 2.28 (1.20) | --- | 0.12 c | 0.90 |
| Unwanted behavior received | 1.52 (1.13) | 1.54 (.94) | --- | 0.10 c | 0.92 |
| Theme | Quotations of Participants |
|---|---|
| 1. Enjoying End Products of Horticulture | I can grow and eat strawberries, if I am able to grow it. |
| I learn about the smell of different herbs | |
| I love herbal tea now. | |
| I learn to make herbal bags, they are beautiful, smells good, and could expel the insects. | |
| It is important to grow something that I can eat. | |
| I like to have produce from horticulture. | |
| Herbal could be used in seasoning | |
| I learn to press and preserve flowers and grass, for making small gifts. | |
| 2. Knowledge & Skill acquisition | I never know there are plants like this … such as “mini coconuts”. |
| I learn to grow tangerine from seeds. | |
| I want to learn more, eight sessions is not enough. | |
| I want to learn more about how to use fertilizers, and how to mix soils for different plants. | |
| There is so much to learn in horticulture. | |
| 3. Vitality and resilience of plants. | I remember our horticulture class was suspended due to typhoon that day, but the plants grow even bigger and stronger after the severe storm. |
| It is pleasurable to see the shoots growing into plants. | |
| Plants are amazing. | |
| Some plants and flowers will close at night, but re-open in the morning. | |
| I did not realize that plants are so resilient. | |
| 4. Serious leisure and potential career development | Horticulture could be a kind of play, but it also could be work. |
| After learning horticulture, I have more and more plants at home, such as tomatoes, cactus, etc. | |
| I see people working in gardens or parks, they must know about horticulture. I am interested in this kind of work. | |
| It may be good for me to open a flora store. Maybe we could run a stall at the annual Flower Market. | |
| 5. Psychosocial and health benefits | I can focus, put all my energy into it. |
| Horticulture helps me to stay calm, practice patience. | |
| Gives me lots of good memories | |
| Help me relieve stress | |
| I become more agile, I use my brain more. | |
| I took photos of my plants and share with friends and family. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siu, A.M.H.; Kam, M.; Mok, I. Horticultural Therapy Program for People with Mental Illness: A Mixed-Method Evaluation. Int. J. Environ. Res. Public Health 2020, 17, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030711
Siu AMH, Kam M, Mok I. Horticultural Therapy Program for People with Mental Illness: A Mixed-Method Evaluation. International Journal of Environmental Research and Public Health. 2020; 17(3):711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030711
Chicago/Turabian StyleSiu, Andrew M.H., Michael Kam, and Ide Mok. 2020. "Horticultural Therapy Program for People with Mental Illness: A Mixed-Method Evaluation" International Journal of Environmental Research and Public Health 17, no. 3: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030711