Burden of Disease Assessment of Ambient Air Pollution and Premature Mortality in Urban Areas: The Role of Socioeconomic Status and Transportation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Definitions
2.2. Input Data
2.2.1. Population, Socioeconomic, and Geographic Data
2.2.2. Mortality Data
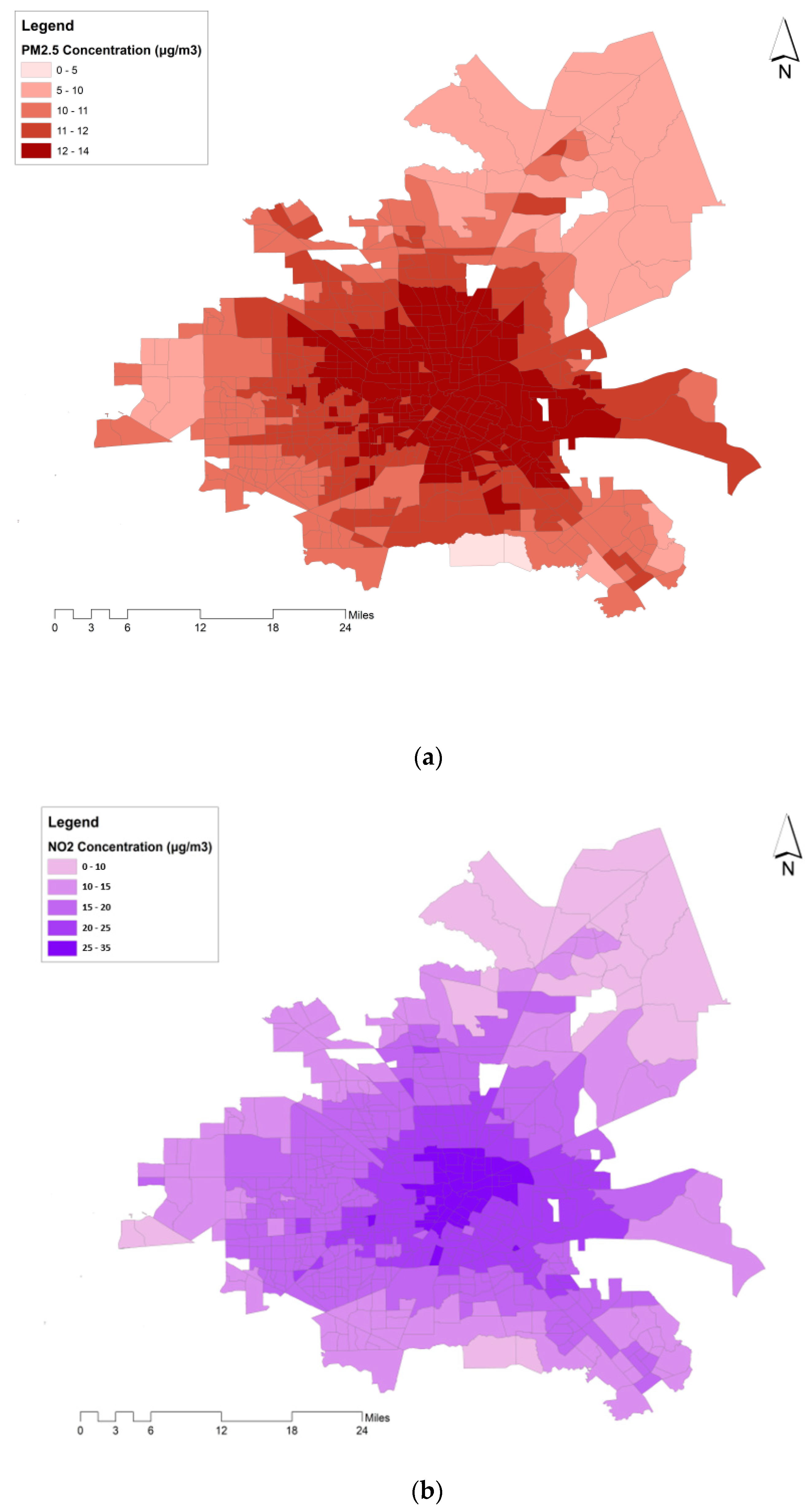
2.2.3. Air Pollution Data
2.2.4. Road Traffic
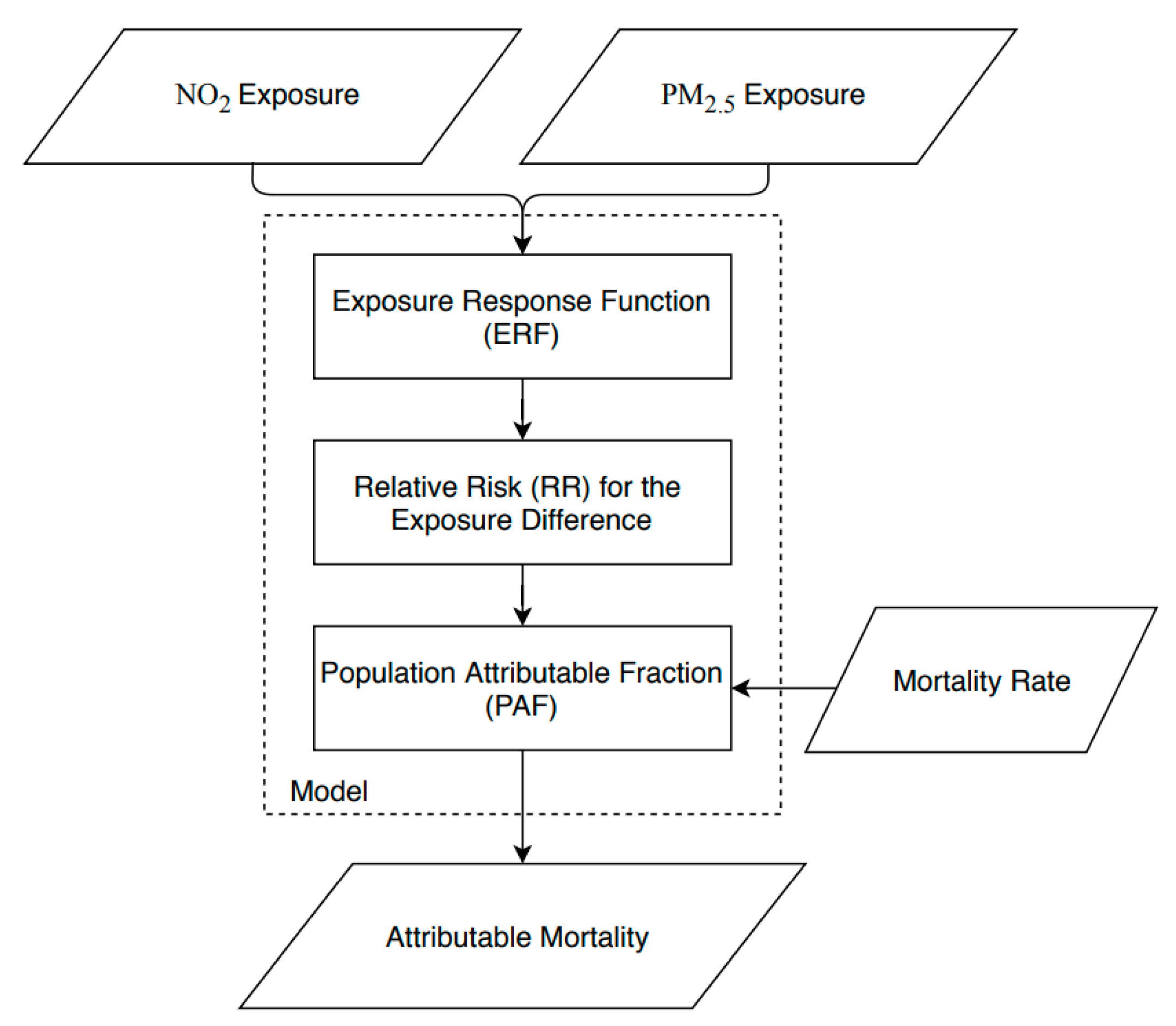
2.3. Burden of Disease Assessment Model
2.4. Exposure-Response Functions
2.5. Counterfactual Scenario
- Zero-exposure of the population to air pollution,
- Air pollution concentrations complying with the WHO air quality guideline values, where in exceedance.
- Air pollution concentrations complying with the the US NAAQS, where in exceedance.
2.6. Sensitivity Analysis
3. Results
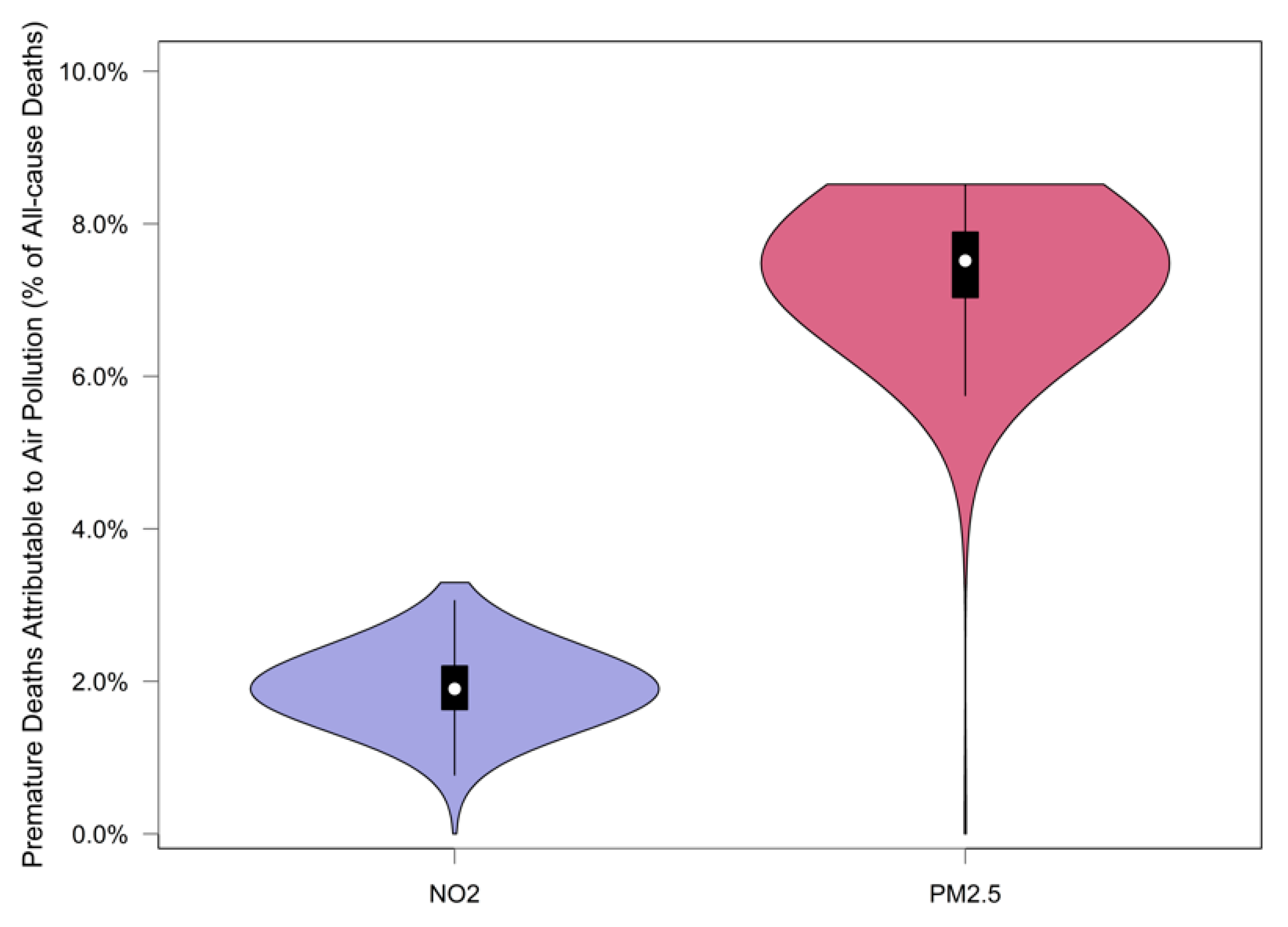
3.1. Premature Deaths Attributable to Air Pollution
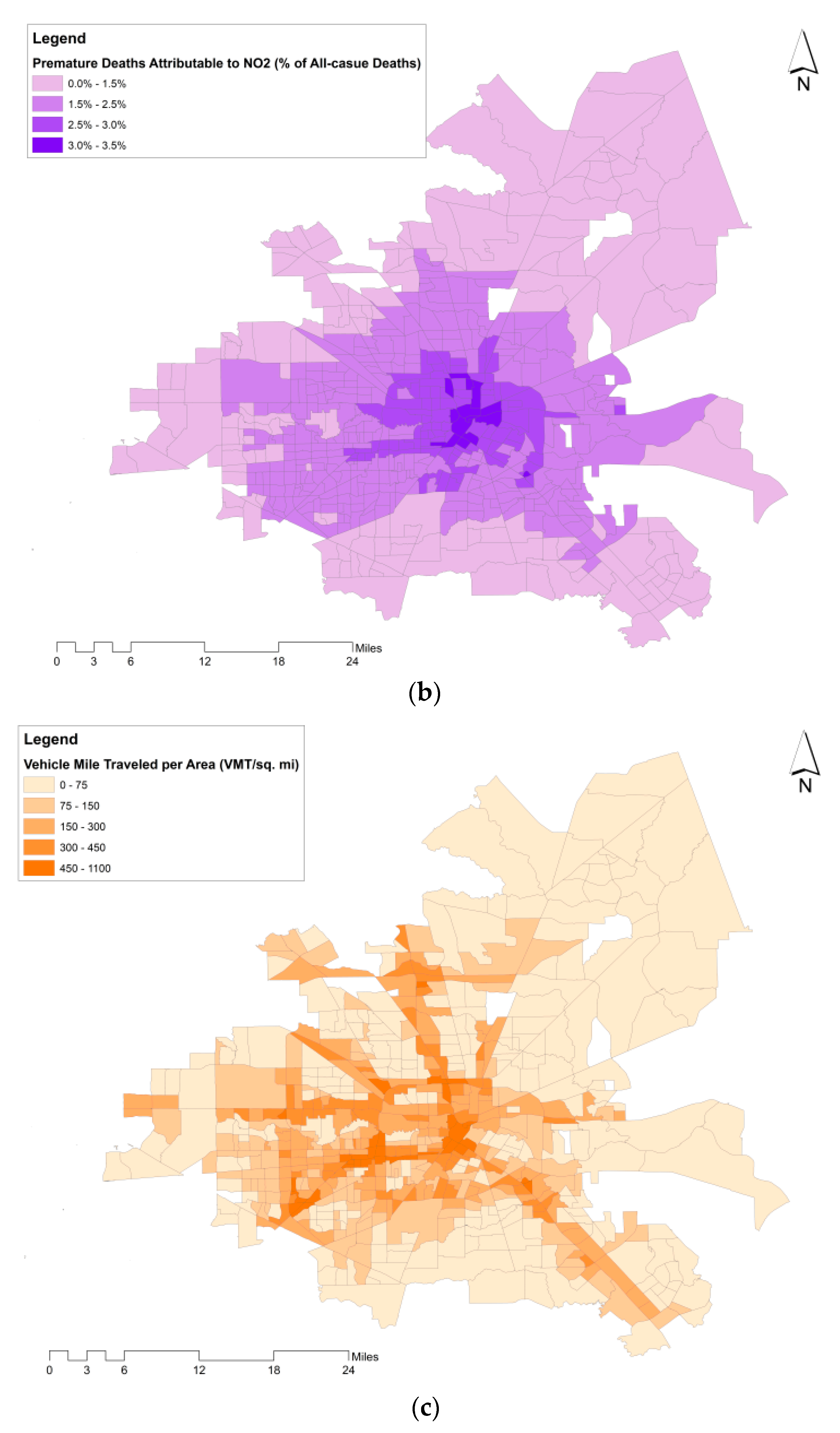
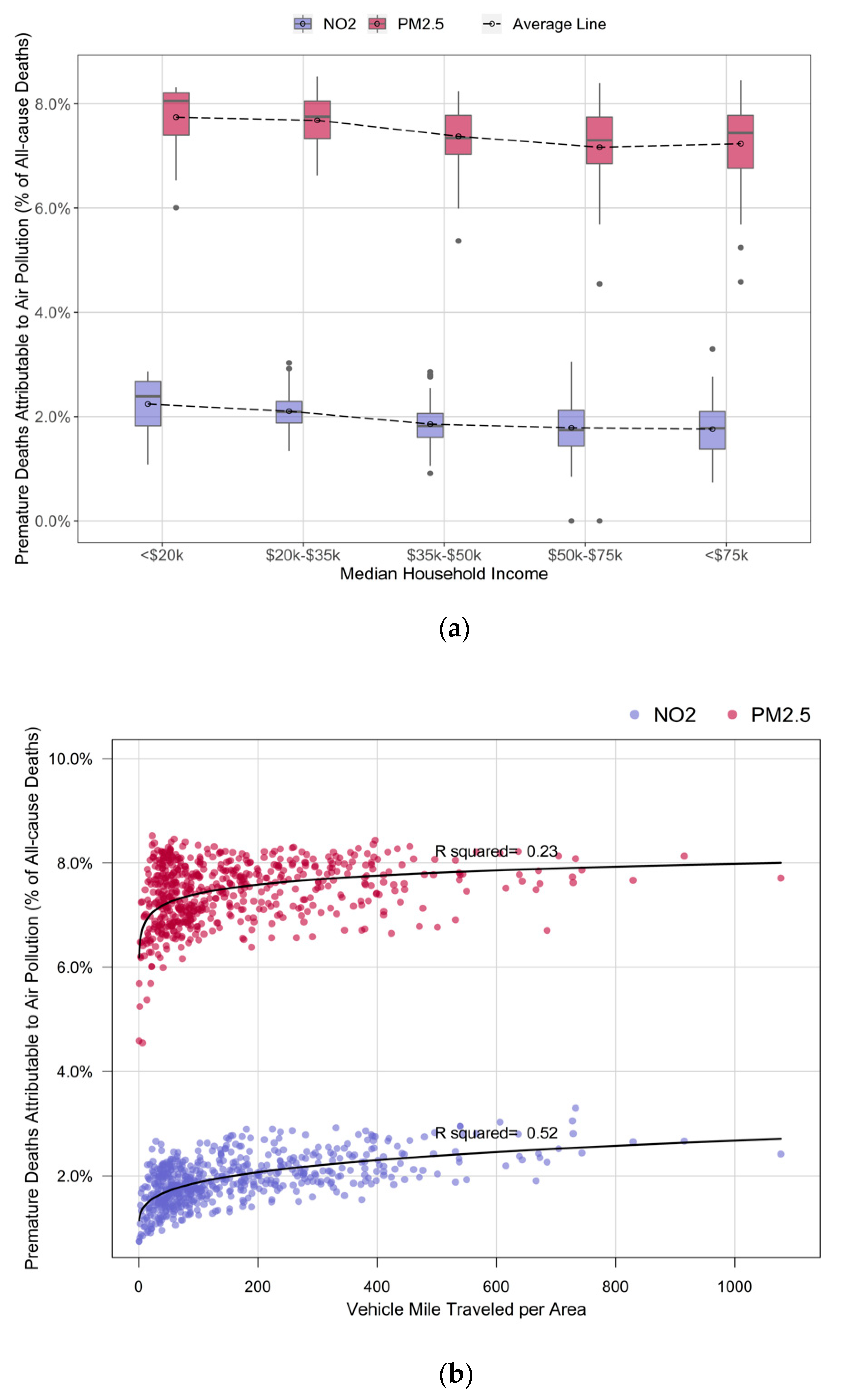
3.2. Premature Deaths Attributable to Air Pollution by Household Income and Road Traffic
3.3. Sensitivity Analysis
4. Discussion
4.1. Key Findings
4.2. Strengths and Limitations
4.3. Policy and Research Recommendations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. World Urbanization Prospects: The 2014 Revision-Highlights; United Nations: Geneva, Switzerland, 2014; Available online: https://population.un.org/wup/Publications/Files/WUP2018-KeyFacts.pdf (accessed on 20 July 2020).
- Wheeler, S.M.; Beatley, T. Sustainable Urban Development Reader; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Robert, K.W.; Parris, T.M.; Leiserowitz, A.A. What is sustainable development? Goals, indicators, values, and practice. Environ. Sci. Policy Sustain. Dev. 2005, 47, 8–21. [Google Scholar] [CrossRef]
- Colvile, R.; Kaur, S.; Britter, R.; Robins, A.; Bell, M.; Shallcross, D.; Belcher, S. Sustainable development of urban transport systems and human exposure to air pollution. Sci. Total Environ. 2004, 334, 481–487. [Google Scholar] [CrossRef]
- Liu, Q.; Baumgartner, J.; de Foy, B.; Schauer, J.J. A global perspective on national climate mitigation priorities in the context of air pollution and sustainable development. City Environ. Interact. 2019, 1, 100003. [Google Scholar] [CrossRef]
- World Health Organization. Who Global Urban Ambient Air Pollution Database (Update 2016); World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/phe/health_topics/outdoorair/databases/cities/en/ (accessed on 20 July 2019).
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B. Air pollution and lung cancer incidence in 17 european cohorts: Prospective analyses from the european study of cohorts for air pollution effects (escape). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Kurt, O.K.; Zhang, J.; Pinkerton, K.E. Pulmonary health effects of air pollution. Curr. Opin. Pulm. Med. 2016, 22, 138. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, K.; Shotten, M.; Cohen, A.; Brauer, M.; Shahraz, S.; Burnett, R.; Leach-Kemon, K.; Freedman, G.; Murray, C. Transport for Health: The Global Burden of Disease from Motorized Road Transport; World Bank Group: Washington, DC, USA, 2014; Available online: http://documents.worldbank.org/curated/en/984261468327002120/Transport-for-health-the-global-burden-of-disease-from-motorized-road-transport (accessed on 7 February 2020).
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; de Faire, U.; Erbel, R.; Eriksen, K.T. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the escape project. BMJ 2014, 348, f7412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesaroni, G.; Badaloni, C.; Gariazzo, C.; Stafoggia, M.; Sozzi, R.; Davoli, M.; Forastiere, F. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in rome. Environ. Health Perspect. 2013, 121, 324–331. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Fact Sheet: Ambient (Outdoor) Air Quality and Health. 2018. Available online: https://www.who.int/en/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 1 May 2019).
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367. [Google Scholar] [CrossRef]
- Tainio, M. Burden of disease caused by local transport in warsaw, poland. J. Transp. Health 2015, 2, 423–433. [Google Scholar] [CrossRef] [Green Version]
- Holnicki, P.; Tainio, M.; Kałuszko, A.; Nahorski, Z. Burden of mortality and disease attributable to multiple air pollutants in warsaw, poland. Int. J. Environ. Res. Public Health 2017, 14, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sá, T.H.; Tainio, M.; Goodman, A.; Edwards, P.; Haines, A.; Gouveia, N.; Monteiro, C.; Woodcock, J. Health impact modelling of different travel patterns on physical activity, air pollution and road injuries for são paulo, brazil. Environ. Int. 2017, 108, 22–31. [Google Scholar]
- Zhang, C.; Ding, R.; Xiao, C.; Xu, Y.; Cheng, H.; Zhu, F.; Lei, R.; Di, D.; Zhao, Q.; Cao, J. Association between air pollution and cardiovascular mortality in Hefei, China: A time-series analysis. Environ. Pollut. 2017, 229, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Rojas-Rueda, D.; Khreis, H.; Cirach, M.; Milà, C.; Espinosa, A.; Foraster, M.; Mceachan, R.R.; Kelly, B.; Wright, J. Socioeconomic inequalities in urban and transport planning related exposures and mortality: A health impact assessment study for bradford, UK. Environ. Int. 2018, 121, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martinez, D. Urban and transport planning related exposures and mortality: A health impact assessment for cities. Environ. Health Perspect. 2016, 125, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Khreis, H.; de Hoogh, K.; Nieuwenhuijsen, M.J. Full-chain health impact assessment of traffic-related air pollution and childhood asthma. Environ. Int. 2018, 114, 365–375. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martínez, D. Health impacts related to urban and transport planning: A burden of disease assessment. Environ. Int. 2017, 107, 243–257. [Google Scholar] [CrossRef] [Green Version]
- Kheirbek, I.; Haney, J.; Douglas, S.; Ito, K.; Matte, T. The contribution of motor vehicle emissions to ambient fine particulate matter public health impacts in new york city: A health burden assessment. Environ. Health 2016, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Tainio, M.; de Nazelle, A.J.; Götschi, T.; Kahlmeier, S.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; de Sá, T.H.; Kelly, P.; Woodcock, J. Can air pollution negate the health benefits of cycling and walking? Prev. Med. 2016, 87, 233–236. [Google Scholar] [CrossRef] [Green Version]
- Khreis, H.; Warsow, K.M.; Verlinghieri, E.; Guzman, A.; Pellecuer, L.; Ferreira, A.; Jones, I.; Heinen, E.; Rojas-Rueda, D.; Mueller, N. The health impacts of traffic-related exposures in urban areas: Understanding real effects, underlying driving forces and co-producing future directions. J. Transp. Health 2016, 3, 249–267. [Google Scholar] [CrossRef]
- Brønnum-Hansen, H.; Bender, A.M.; Andersen, Z.J.; Sørensen, J.; Bønløkke, J.H.; Boshuizen, H.; Becker, T.; Diderichsen, F.; Loft, S. Assessment of impact of traffic-related air pollution on morbidity and mortality in copenhagen municipality and the health gain of reduced exposure. Environ. Int. 2018, 121, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Goodkind, A.L.; Tessum, C.W.; Coggins, J.S.; Hill, J.D.; Marshall, J.D. Fine-scale damage estimates of particulate matter air pollution reveal opportunities for location-specific mitigation of emissions. Proc. Natl. Acad. Sci. USA 2019, 116, 8775–8780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Effects Institute. Traffic-related Air Pollution: A Critical Review of the Literature on Emissions, Exposure, and Health Effects; Health Effects Institute: Boston, MA, USA, 2010. [Google Scholar]
- World Population Review. Houston, Texas Population. 2019. Available online: http://worldpopulationreview.com/us-cities/houston-population/ (accessed on 1 May 2019).
- Doughty, J. Mortality in terms of lost years of life. Can. J. Public Health/Revue Can. de Sante’e Publique 1951, 42, 134–141. [Google Scholar]
- Murphy, S.L.; Xu, J.; Kochanek, K.D. Deaths: Final Data for 2010. 2013. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_06.pdf (accessed on 20 July 2019).
- Alotaibi, R.; Bechle, M.; Marshall, J.D.; Ramani, T.; Zietsman, J.; Nieuwenhuijsen, M.J.; Khreis, H. Traffic related air pollution and the burden of childhood asthma in the contiguous united states in 2000 and 2010. Environ. Int. 2019, 127, 858–867. [Google Scholar] [CrossRef]
- WHO. Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Bechle, M.J.; Millet, D.B.; Marshall, J.D. National spatiotemporal exposure surface for NO2: Monthly scaling of a satellite-derived land-use regression, 2000–2010. Environ. Sci. Technol. 2015, 49, 12297–12305. [Google Scholar] [CrossRef]
- Beelen, R.; Hoek, G.; Pebesma, E.; Vienneau, D.; de Hoogh, K.; Briggs, D.J. Mapping of background air pollution at a fine spatial scale across the european union. Sci. Total Environ. 2009, 407, 1852–1867. [Google Scholar] [CrossRef]
- Hystad, P.; Setton, E.; Cervantes, A.; Poplawski, K.; Deschenes, S.; Brauer, M.; van Donkelaar, A.; Lamsal, L.; Martin, R.; Jerrett, M. Creating national air pollution models for population exposure assessment in canada. Environ. Health Perspect. 2011, 119, 1123–1129. [Google Scholar] [CrossRef]
- Vienneau, D.; de Hoogh, K.; Bechle, M.J.; Beelen, R.; van Donkelaar, A.; Martin, R.V.; Millet, D.B.; Hoek, G.; Marshall, J.D. Western european land use regression incorporating satellite-and ground-based measurements of NO2 and PM10. Environ. Sci. Technol. 2013, 47, 13555–13564. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Bechle, M.; Hankey, S.; Sheppard, L.; Aa, J.a.M.S. Parsimonious Approach for Estimating Ambient Concentrations of Criteria Pollutants in the Contiguous U.S. Unpublished Manuscript.
- World Health Organization. Review of Evidence on Health Aspects of Air Pollution–Revihaap Project: Final Technical Report; WHO European Centre for Environment and Health: Geneva, Switzerland, 2013. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK361807/ (accessed on 20 July 2019).
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 european cohorts within the multicentre escape project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- World Health Organization. Who Expert Meeting: Methods and Tools for Assessing the Health Risks of Air Pollution at Local, National and International Level; WHO Regional Office for Europe: Copenhagen, Denmark, 2014; Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/263629/WHO-Expert-Meeting-Methods-and-tools-for-assessing-the-health-risks-of-air-pollution-at-local,-national-and-international-level.pdf?ua=1 (accessed on 20 July 2019).
- Environmental Protection Agency. Primary and Secondary National Ambient Air Quality Standards for Oxides of Nitrogen and Sulfur, 36 Fed. Reg. 8186 (Final Rule 30 April 1971).
- Environmental Protection Agency. National Ambient Air Quality Standards for Particulate Matter, 78 Fed. Reg. 3085 (Final Rule 15 January 2013) (to be codified at 40 C.F.R. pts 50, 51, 52).
- Anderson, R.T.; Sorlie, P.; Backlund, E.; Johnson, N.; Kaplan, G.A. Mortality effects of community socioeconomic status. Epidemiology 1997, 8, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G.; Pickett, K.E. Income inequality and socioeconomic gradients in mortality. Am. J. Public Health 2008, 98, 699–704. [Google Scholar] [CrossRef]
- Hao, J.; Wu, Y.; Fu, L.; He, D.; He, K. Source contributions to ambient concentrations of co and nox in the urban area of beijing. J. Environ. Sci. Health Part A 2001, 36, 215–228. [Google Scholar] [CrossRef]
- Bhanarkar, A.; Goyal, S.; Sivacoumar, R.; Rao, C.C. Assessment of contribution of SO2 and NO2 from different sources in jamshedpur region, india. Atmos. Environ. 2005, 39, 7745–7760. [Google Scholar] [CrossRef]
- Sundvor, I.; Balaguer, N.C.; Viana, M.; Querol, X.; Reche, C.; Amato, F.; Mellios, G.; Guerreiro, C. Road traffic’s Contribution to Air Quality in European Cities. Etc/acm Technical Paper 2012/14 November 2012. The European Topic Centre on Air Pollution and Climate Change Mitigation (ETC/ACM) (a Consortium of European Institutes under Contract of the European Environment Agency). 2012. Available online: https://www.eionet.europa.eu/etcs/etc-atni/products/etc-atni-reports/etcacm_tp_2012_14_traffic_contribution_city_aq (accessed on 20 July 2019).
- U.S. Department of Transportation. Transporation Air Quality Selected Facts and Figures; U.S. Department of Transportation: Washington, DC, USA, 2016. Available online: https://www.fhwa.dot.gov/environment/air_quality/publications/fact_book/index.cfm (accessed on 20 July 2019).
- Christina, H.F.; Brugge, D. Environmental justice: Disproportionate impacts of transportation on vulnerable communities. In Traffic-Related Air Pollution: Emissions, Human Exposures, and Health; Khreis, H., Nieuwenhuijsen, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Clark, L.P.; Millet, D.B.; Marshall, J.D. Changes in transportation-related air pollution exposures by race-ethnicity and socioeconomic status: Outdoor nitrogen dioxide in the united states in 2000 and 2010. Environ. Health Perspect. 2017, 125, 097012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Zhong, B.; Vardoulakis, S.; Zhang, F.; Pilot, E.; Li, Y.; Yang, L.; Wang, W.; Krafft, T. Air quality strategies on public health and health equity in europe—A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 1196. [Google Scholar] [CrossRef] [Green Version]
- Gärling, T.; Schuitema, G. Travel demand management targeting reduced private car use: Effectiveness, public acceptability and political feasibility. J. Soc. Issues 2007, 63, 139–153. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Sample Size (Census Tracts) | Min | Median | Mean | Max |
|---|---|---|---|---|---|
| All-cause premature deaths (persons) | 592 | 1 | 14 | 15 | 61 |
| NO2 concentration (μg/m3) | 592 | 7.47 | 19.38 | 19.52 | 34.09 |
| PM2.5 concentration (μg/m3) | 592 | 6.80 | 11.61 | 11.41 | 13.30 |
| VMTA (veh.mi/mi2) | 592 | 0.72 | 99.27 | 163.04 | 1077.54 |
| Median household income (dollar) | 592 | 9926 | 43,352 | 52,857 | 214,861 |
| Counterfactual Scenario | Premature Deaths Cases (95% CI) | Air Pollutant | Counterfactual Concentration (μg/m3) | Adjusted RR Associated with 10 μg/m3 Increase (95% CI) | Attributable Premature Deaths (95% CI) | % of Attributable Premature Deaths to All-Cause Deaths (95% CI) |
|---|---|---|---|---|---|---|
| Zero-exposure scenario | 8667 (8499–8834) | PM2.5 | 0 | 1.07 (1.02–1.12) | 631 (366–809) | 7.3% (4.3%–9.2%) |
| NO2 | 0 | 1.01 (0.99–1.04) | 159 (0–609) | 1.8% (0.0%–6.9%) | ||
| Complying with WHO guidelines | 8667 (8499–8834) | PM2.5 | 10 | 1.07 (1.02–1.12) | 82 (42–95) | 0.9% (0.5%–1.1%) |
| NO2 | 40 | 1.01 (0.99–1.04) | 0 1 (0–0) | 0.0% (0.0%–0.0%) | ||
| Complying with NAAQS | 8667 (8499–8834) | PM2.5 | 12 | 1.07 (1.02–1.12) | 8 (6–10) | 0.1% (0.0%–0.1%) |
| NO2 | 99 | 1.01 (0.99–1.04) | 0 1 (0–0) | 0.0% (0.0%–0.0%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohrabi, S.; Zietsman, J.; Khreis, H. Burden of Disease Assessment of Ambient Air Pollution and Premature Mortality in Urban Areas: The Role of Socioeconomic Status and Transportation. Int. J. Environ. Res. Public Health 2020, 17, 1166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041166
Sohrabi S, Zietsman J, Khreis H. Burden of Disease Assessment of Ambient Air Pollution and Premature Mortality in Urban Areas: The Role of Socioeconomic Status and Transportation. International Journal of Environmental Research and Public Health. 2020; 17(4):1166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041166
Chicago/Turabian StyleSohrabi, Soheil, Joe Zietsman, and Haneen Khreis. 2020. "Burden of Disease Assessment of Ambient Air Pollution and Premature Mortality in Urban Areas: The Role of Socioeconomic Status and Transportation" International Journal of Environmental Research and Public Health 17, no. 4: 1166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041166