A Cross-Sectional Study of Age-Related Changes in Oral Function in Healthy Japanese Individuals

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Investigated Criteria
2.2.1. Degree of Tongue Coating
2.2.2. Oral Mucosal Wetness
2.2.3. Occlusal Force
2.2.4. Tongue–Lip Motor Function
2.2.5. Tongue Pressure
2.2.6. Masticatory Function
2.2.7. Swallowing Function
2.3. Statistical Analysis
2.3.1. Gender Differences
2.3.2. Analysis of Oral Function
2.3.3. Bivariate Correlation Analyses of the Criteria
3. Results
3.1. Participants’ Characteristics
3.2. Oral Function Criteria Results
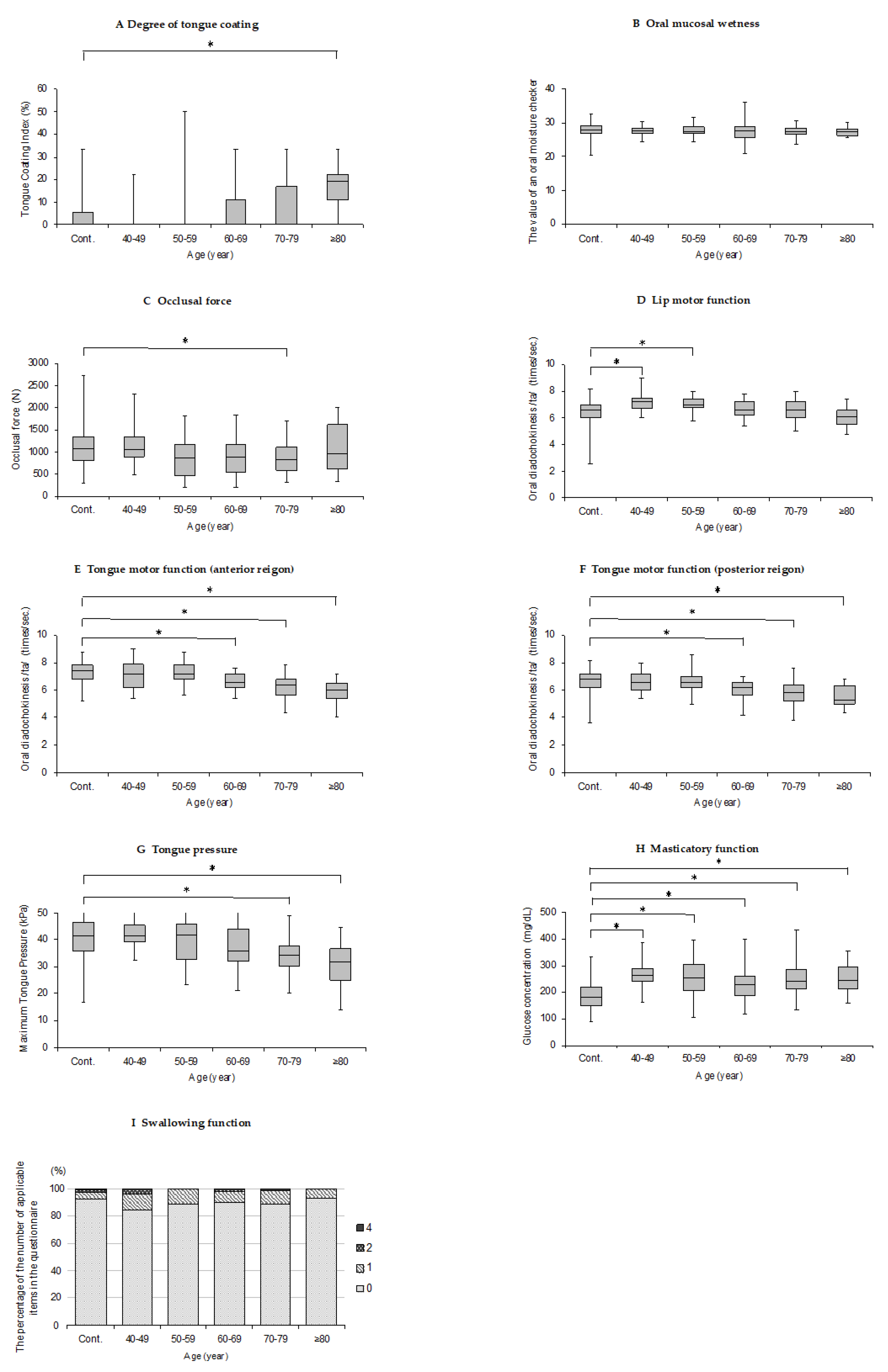
3.2.1. Degree of Tongue Coating
3.2.2. Oral Mucosal Wetness
3.2.3. Occlusal Force
3.2.4. Tongue–Lip Motor Function
3.2.5. Tongue Pressure
3.2.6. Masticatory Function
3.2.7. Swallowing Function
3.3. Bivariate Correlation Analyses of the Criteria
4. Discussion
4.1. Degree of Tongue Coating
4.2. Mucosal Wetness
4.3. Occlusal Force
4.4. Tongue–Lip Motor Function
4.5. Tongue Pressure
4.6. Masticatory Function
4.7. Swallowing Function
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Machida, N.; Tohara, H.; Hara, K.; Kumakura, A.; Wakasugi, Y.; Nakane, A.; Minakuchi, S. Effects of aging and sarcopenia on tongue pressure and jaw-opening force. Geriatri. Gerontol. Int. 2017, 17, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Akagi, J. Decreased tongue pressure is associated with sarcopenia and sarcopenic dysphagia in the elderly. Dysphagia 2015, 30, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Sumi, Y.; Miura, H.; Nagaya, M.; Nagaosa, S.; Umemura, O. Relationship between oral function and general condition among Japanese nursing home residents. Arch. Gerontol. Geriat. 2009, 48, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Hagglund, P.; Falt, A.; Hagg, M.; Wester, P.; Jaghagen, E.L. Swallowing dysfunction as risk factor for undernutrition in older people admitted to Swedish short-term care: A cross-sectional study. Aging Clin. Exp. Res. 2019, 31, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Amemiya, K.; Nakatsuka, M.; Nakamura, K.; Kasai, M.; Meguro, K. Impaired eating and swallowing function in older adults in the community: The Kurihara project. Int. J. Environ. Res. Public Health 2019, 16, 4040. [Google Scholar] [CrossRef] [Green Version]
- Buehring, B.; Hind, J.; Fidler, E.; Krueger, D.; Binkley, N.; Robbins, J. Tongue strength is associated with jumping mechanography performance and handgrip strength but not with classic functional tests in older adults. J. Am. Geriatr. Soc. 2013, 61, 418–422. [Google Scholar] [CrossRef]
- Hara, K.; Tohara, H.; Kenichiro, K.; Yamaguchi, K.; Ariya, C.; Yoshimi, K.; Nakane, A.; Minakuchi, S. Association between tongue muscle strength and masticatory muscle strength. J. Oral Rehabil. 2019, 46, 134–139. [Google Scholar] [CrossRef]
- Furuya, H.; Tamura, F.; Yoshida, M.; Hirano, H.; Iijima, K.; Kikutani, T. Tongue muscle mass and strength relate to whole-body muscle in the community-dwelling elderly. Jpn. J. Dysphagia Rehabil. 2016, 29, 1–9. (In Japanese) [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. Med. J. 1965, 14, 56–61. [Google Scholar]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). A. Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [Green Version]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Shimizu, T.; Ueda, T.; Sakurai, K. New method for evaluation of tongue-coating status. J. Oral Rehabil. 2007, 34, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Uesugi, H.; Shiga, H. Relationship between masticatory performance using a gummy jelly and masticatory movement. J. Prosthodont. Res. 2017, 61, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Okuma, R.; Fujishima, I.; Kojima, S.; Hojo, K.; Takehara, I.; Motohashi, Y. Development of a questionnaire to screen dysphagia. Jpn. J. Dysphagia Rehabil. 2002, 6, 3–8. (In Japanese) [Google Scholar]
- Ralph, W.J. Hygiene of the tongue. Gerodontics 1987, 3, 169–170. [Google Scholar]
- Yaegaki, K.; Sanada, K. Biochemical and clinical factors influencing oral malodor in periodontal patients. J. Periodontol. 1992, 63, 783–789. [Google Scholar] [CrossRef]
- Kikutani, T.; Tamura, F.; Nishiwaki, K.; Suda, M.; Kayanaka, H.; Machida, R.; Yoshida, M.; Akagawa, Y. The degree of tongue-coating reflects lingual motor function in the elderly. Gerodontology 2009, 26, 291–296. [Google Scholar] [CrossRef]
- Pedersen, W.; Schubert, M.; Izutsu, K.; Mersai, T.; Truelove, E. Age-dependent decreases in human submandibular-gland flow-rates as measured under resting and post-stimulation conditions. J. Dent. Res. 1985, 64, 822–825. [Google Scholar] [CrossRef]
- Gandara, B.K.; Izutsu, K.T.; Truelove, E.L.; Ensign, W.Y.; Sommers, E.E. Age-related salivary flow-rate changes in controls and patients with oral lichen planus. J. Dent. Res. 1985, 64, 1149–1151. [Google Scholar] [CrossRef]
- Baum, B.J. Evaluation of stimulated parotid-saliva flow-rate in different age-groups. J. Dent. Res. 1981, 60, 1292–1296. [Google Scholar] [CrossRef] [PubMed]
- Benaryeh, H.; Shalev, A.; Szargel, R.; Laor, A.; Laufer, D.; Gutman, D. The salivary flow-rate and composition of whole and parotid resting and stimulated saliva in young and old healthy-subjects. Biochem. Med. Metab. Biol. 1986, 36, 260–265. [Google Scholar] [CrossRef]
- Scully, C.; Felix, D.H. Oral Medicine—Update for the dental practitioner. Dry mouth and disorders of salivation. Brit. Dent. J. 2005, 199, 423–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, B.J.; Bodner, L. Aging and oral motor function—Evidence for altered performance among older persons. J. Dent. Res. 1983, 62, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Bakke, M.; Holm, B.; Jensen, B.L.; Michler, L.; Moller, E. Unilateral, isometric bite force in 8–68-year-old women and men related to occlusal factors. Scand. J. Dent. Res. 1990, 98, 148–158. [Google Scholar] [CrossRef]
- Iinuma, T.; Arai, Y.; Fukumoto, M.; Takayama, M.; Abe, Y.; Asakura, K.; Nishiwaki, Y.; Takebayashi, T.; Iwase, T.; Komiyama, K.; et al. Maximum occlusal force and physical performance in the oldest old: The Tokyo oldest old survey on total health. J. Am. Geriatr. Soc. 2012, 60, 68–76. [Google Scholar] [CrossRef]
- Shinogaya, T.; Bakke, M.; Thomsen, C.E.; Vilmann, A.; Sodeyama, A.; Matsumoto, M. Effects of ethnicity, gender and age on clenching force and load distribution. Clin. Oral. Investig. 2001, 5, 63–68. [Google Scholar] [CrossRef]
- Motegi, E.; Nomura, M.; Tachiki, C.; Miyazaki, H.; Takeuchi, F.; Takaku, S.; Abe, Y.; Miyatani, M.; Ogai, T.; Fuma, A.; et al. Occlusal force in people in their sixties attending college for elderly. Bull. Tokyo Dent. Coll. 2009, 50, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Helkimo, E.; Carlsson, G.E.; Helkimo, M. Bite force and state of dentition. Acta Odontol. Scand. 1977, 35, 297–303. [Google Scholar] [CrossRef]
- Noro, A.; Hosokawa, S.; Takahashi, J.; Akihiro, Y.; Nishimoto, Y.; Hosokawa, I.; Makiishi, T.; Hirai, Y. Basic and clinical subjects of myofunctional therapy using a new oral rehabilitation apparatus Part.2 Evaluation of chronological changes of ‘‘labial-closure-strength” from youth to adults. Jpn. J. Conserv. Dent. 2002, 45, 817–828. (In Japanese) [Google Scholar]
- Hara, S.; Miura, H.; Yamasaki, K. Oral diadochokinesis among Japanese aged over 55 years: Analysis of standard values. Jpn. J. Geriatr. 2013, 50, 258–263. (In Japanese) [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikutani, T.; Tamura, F.; Nishiwaki, K.; Kodama, M.; Suda, M.; Fukui, T.; Takahashi, N.; Yoshida, M.; Akagawa, Y.; Kimura, M. Oral motor function and masticatory performance in the community-dwelling elderly. Odontology 2009, 97, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Fei, T.; Polacco, R.C.; Hori, S.E.; Molfenter, S.M.; Peladeau-Pigeon, M.; Tsang, C.; Steele, C.M. Age-related differences in tongue-palate pressures for strength and swallowing tasks. Dysphagia 2013, 28, 575–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, D.; Visser, M.; deMeersman, R.E.; Sepulveda, D.; Baumgartner, R.N.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. Appendicular skeletal muscle mass: Effects of age, gender, and ethnicity. J. Appl. Physiol. 1997, 83, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Kimura, M.; Nakamura, E.; Masuo, Y.; Oda, S. Limb muscle mass decrease with aging in Japanese men and women aged 15–97 yr. Jpn. J. Phys. Fit. Sports Med. 2007, 56, 461–471. (In Japanese) [Google Scholar] [CrossRef]
- Yamada, A.; Kanazawa, M.; Komagamine, Y.; Minakuchi, S. Association between tongue and lip functions and masticatory performance in young dentate adults. J. Oral Rehabil. 2015, 42, 833–839. [Google Scholar] [CrossRef]
- Ikeda, Y.; Shioda, Y.; Narita, T.; Kondo, Y.; Ikeda, T.; Sato, J.; Ito, T.; Gionhaku, N. Age related changes of masticatory ability—Occlusal force, Occlusal contact area, Amount of glucose discharge, Temporal phage of masticatory movement-. J. Jpn. Soc. Masticatory Sci. and Health Prom. 2014, 24, 59–66. (In Japanese) [Google Scholar]
- Furuta, M.; Komiya-Nonaka, M.; Akifusa, S.; Shimazaki, Y.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Interrelationship of oral health status, swallowing function, nutritional status, and cognitive ability with activities of daily living in Japanese elderly people receiving home care services due to physical disabilities. Community Dent. Oral Epidemiol. 2013, 41, 173–181. [Google Scholar] [CrossRef]
- Okamoto, N.; Tomioka, K.; Saeki, K.; Iwamoto, J.; Morikawa, M.; Harano, A.; Kurumatani, N. Relationship between swallowing problems and tooth loss in community-dwelling independent elderly adults: The Fujiwara-kyo study. J. Am. Geriatr. Soc. 2012, 60, 849–853. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Hirano, H.; Arai, H.; Morishita, S.; Ohara, Y.; Edahiro, A.; Murakami, M.; Shimada, H.; Kikutani, T.; Suzuki, T. Relationship between frailty and oral function in community-dwelling elderly adults. J. Am. Geriatr. Soc. 2017, 65, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, Y.; Horii, N.; Sakuramoto-Sadakane, A.; Nagai, K.; Ono, T.; Sawada, T.; Shinmura, K.; Kishimoto, H. Is a history of falling related to oral function? A cross-sectional survey of elderly subjects in rural Japan. Int. J. Environ. Res. Public Health 2019, 16, 3843. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Age Group | Cont. | 40–49 | 50–59 | 60–69 | 70–79 | ≥80 |
|---|---|---|---|---|---|---|
| n (men/women) | 92 (52/40) | 25 (10/15) | 35 (9/26) | 39 (18/21) | 63 (21/42) | 13 (7/6) |
| Age (year) | 23.4 ± 2.1 | 44.2 ± 3.0 | 53.6 ± 2.8 | 65.4 ± 3.2 | 74.8 ± 2.5 | 83.7 ± 3.0 |
| Number of remaining teeth | 28.3 ± 1.8 | 27.6 ± 2.5 | 26.8 ± 2.0 | 25.6 ± 2.8 | 26.3 ± 2.4 | 25.1 ± 3.8 |
| Percentage of denture users (%) | 0 | 4.0 | 0 | 15.4 | 17.5 | 23.1 |
| Age | TCI | Mucosal Wetness | Occlusal Force | OD/pa/ | OD /ta/ | OD/ka/ | Tongue Pressure | Masticatory Function | Swallowing Function | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 1 | 0.335 * | −0.089 | −0.054 | −0.423 * | −0.480 * | −0.426 * | −0.485 * | −0.089 | −0.019 |
| TCI | 1 | −0.078 | 0.078 | −0.106 | −0.127 | −0.149 | −0.218 * | 0.090 | 0.063 | |
| Mucosal wetness | 1 | −0.025 | 0.079 | 0.078 | 0.032 | 0.003 | −0.135 | 0.082 | ||
| Occlusal force | 1 | −0.001 | 0.063 | 0.023 | 0.231 * | 0.314 * | 0.088 | |||
| OD /pa/ | 1 | 0.776 * | 0.765 * | 0.332 * | 0.160 * | −0.110 | ||||
| OD /ta/ | 1 | 0.836 * | 0.343 * | 0.182 * | −0.091 | |||||
| OD /ka/ | 1 | 0.294 * | 0.166 * | −0.096 | ||||||
| Tongue pressure | 1 | 0.214 * | 0.034 | |||||||
| Masticatory function | 1 | −0.021 | ||||||||
| Swallowing function | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyota, K.; Mizutani, S.; Oku, S.; Asao, M.; Futatsuki, T.; Inoue, R.; Imai, Y.; Kashiwazaki, H. A Cross-Sectional Study of Age-Related Changes in Oral Function in Healthy Japanese Individuals. Int. J. Environ. Res. Public Health 2020, 17, 1376. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041376
Iyota K, Mizutani S, Oku S, Asao M, Futatsuki T, Inoue R, Imai Y, Kashiwazaki H. A Cross-Sectional Study of Age-Related Changes in Oral Function in Healthy Japanese Individuals. International Journal of Environmental Research and Public Health. 2020; 17(4):1376. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041376
Chicago/Turabian StyleIyota, Kiyomi, Shinsuke Mizutani, Saori Oku, Misa Asao, Toshiko Futatsuki, Ryosuke Inoue, Yuko Imai, and Haruhiko Kashiwazaki. 2020. "A Cross-Sectional Study of Age-Related Changes in Oral Function in Healthy Japanese Individuals" International Journal of Environmental Research and Public Health 17, no. 4: 1376. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041376