Effects of HIV-Related Discrimination on Psychosocial Syndemics and Sexual Risk Behavior among People Living with HIV


Abstract
:1. Introduction
1.1. Syndemic Theory
1.2. HIV and Discrimination in Hong Kong
1.3. The Present Study
2. Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
3.1. HIV-Related Discrimination and Psychosocial Syndemics
3.2. Condom Use with Steady and Casual Partners
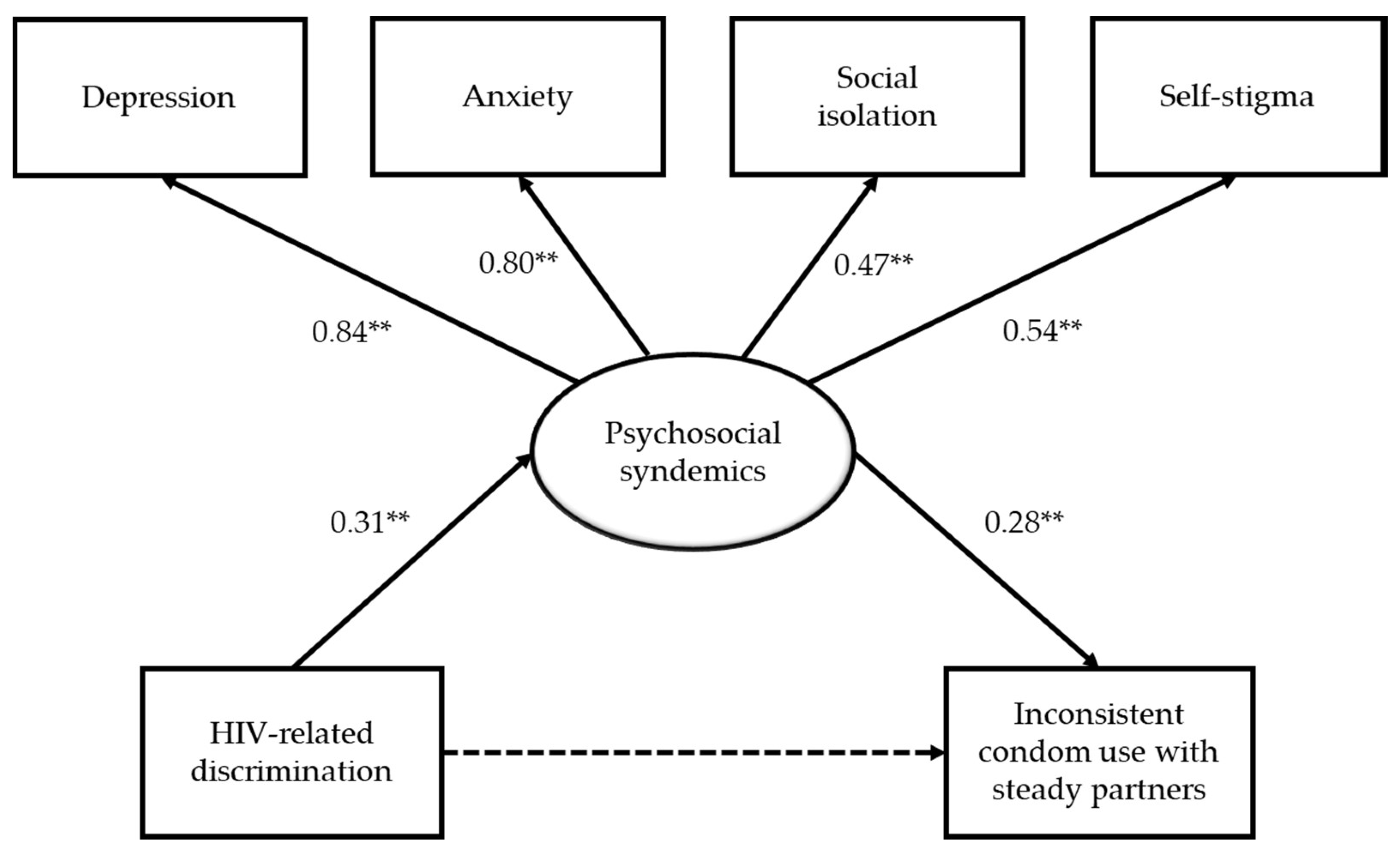
3.3. A Mediation Model of HIV-Related Discrimination on Sexual Risk Behavior
4. Discussion
4.1. Relevance to Local Context
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dos Santos, M.M.; Kruger, P.; Mellors, S.E.; Wolvaardt, G.; Van Der Ryst, E. An exploratory survey measuring stigma and discrimination experienced by people living with HIV/AIDS in South Africa: The People Living with HIV Stigma Index. BMC Public Health 2014, 14, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simbayi, L.C.; Kalichman, S.; Strebel, A.; Cloete, A.; Henda, N.; Mqeketo, A. Internalized stigma, discrimination, and depression among men and women living with HIV/AIDS in Cape Town, South Africa. Soc. Sci. Med. 2007, 64, 1823–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxton, S.; Gonzales, G.; Uppakaew, K.; Abraham, K.; Okta, S.; Green, C.; Nair, K.; Parwati Merati, T.; Thephthien, B.; Marin, M. AIDS-related discrimination in Asia. AIDS Care 2005, 17, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Morroni, C.; Zuniga, J.M.; Sherer, R.; Beyrer, C.; Solomon, S.; Schechter, M.; Rockstroh, J. HIV-related stigma, isolation, discrimination, and serostatus disclosure: A global survey of 2035 HIV-infected adults. J. Int. Assoc. Physicians AIDS Care 2012, 11, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Wingood, G.M.; DiClemente, R.J.; Mikhail, I.; McCree, D.H.; Davies, S.L.; Hardin, J.W.; Peterson, S.H.; Hook, E.W.; Saag, M. HIV discrimination and the health of women living with HIV. Women Health 2007, 46, 99–112. [Google Scholar] [CrossRef]
- Stutterheim, S.E.; Pryor, J.B.; Bos, A.E.; Hoogendijk, R.; Muris, P.; Schaalma, H.P. HIV-related stigma and psychological distress: The harmful effects of specific stigma manifestations in various social settings. AIDS 2009, 23, 2353–2357. [Google Scholar] [CrossRef]
- Elford, J.; Ibrahim, F.; Bukutu, C.; Anderson, J. HIV-related discrimination reported by people living with HIV in London, UK. AIDS Behav. 2008, 12, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Bogart, L.M.; Wagner, G.J.; Galvan, F.H.; Landrine, H.; Klein, D.J.; Sticklor, L.A. Perceived discrimination and mental health symptoms among Black men with HIV. Cult. Divers. Ethn. Minor. Psychol. 2011, 17, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Préau, M.; Bouhnik, A.D.; Peretti-Watel, P.; Obadia, Y.; Spire, B.; Group, A.E.V. Suicide attempts among people living with HIV in France. AIDS Care 2008, 20, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Mak, W.W.; Cheung, R.Y. Self-stigma among concealable minorities in Hong Kong: Conceptualization and unified measurement. Am. J. Orthopsychiatry 2010, 80, 267–281. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Watson, A.C. The paradox of self-stigma and mental illness. Clin. Psychol. Sci. Pract. 2002, 9, 35–53. [Google Scholar] [CrossRef]
- Mak, W.W.; Cheung, R.Y.; Law, R.W.; Woo, J.; Li, P.C.; Chung, R.W. Examining attribution model of self-stigma on social support and psychological well-being among people with HIV+/AIDS. Soc. Sci. Med. 2007, 64, 1549–1559. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Spire, B.; Obadia, Y.; Moatti, J.P.; Group, V. Discrimination against HIV-infected people and the spread of HIV: Some evidence from France. PLoS ONE 2007, 2, 411. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Fernandez, V.I.; Miranda, S.M.; Jacobson, J.O.; Mendoza, S.; Paredes, M.A.; Danaval, D.C.; Mabey, D.; Monterroso, E. Unsafe sexual behaviors among HIV-positive men and women in Honduras: The role of discrimination, condom access, and gender. Sex. Transm. Dis. 2012, 39, 35–41. [Google Scholar] [CrossRef]
- Singer, M.; Clair, S. Syndemics and public health: Reconceptualizing disease in bio-social context. Med. Anthropol. Q. 2003, 17, 423–441. [Google Scholar] [CrossRef]
- Singer, M. AIDS and the health crisis of the US urban poor; the perspective of critical medical anthropology. Soc. Sci. Med. 1994, 39, 931–948. [Google Scholar] [CrossRef] [Green Version]
- Mustanski, B.; Garofalo, R.; Herrick, A.; Donenberg, G. Psychosocial health problems increase risk for HIV among urban young men who have sex with men: Preliminary evidence of a syndemic in need of attention. Ann. Behav. Med. 2007, 34, 37–45. [Google Scholar] [CrossRef]
- Tsai, A.C.; Burns, B.F. Syndemics of psychosocial problems and HIV risk: A systematic review of empirical tests of the disease interaction concept. Soc. Sci. Med. 2015, 139, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Batchelder, A.W.; Lounsbury, D.W.; Palma, A.; Carrico, A.; Pachankis, J.; Schoenbaum, E.; Gonzalez, J.S. Importance of substance use and violence in psychosocial syndemics among women with and at-risk for HIV. AIDS Care 2016, 28, 1316–1320. [Google Scholar] [CrossRef] [Green Version]
- Nehl, E.J.; Klein, H.; Sterk, C.E.; Elifson, K.W. Prediction of HIV sexual risk behaviors among disadvantaged African American adults using a syndemic conceptual framework. AIDS Behav. 2016, 20, 449–460. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; He, Y.; Pham, R.; Ravelo, G.J.; Rojas, P.; Rodriguez, P.; Castro, G.; Barengo, N.C.; Acuña, J.M.; Cyrus, E. Analyzing the association between depression and high-risk sexual behavior among adult Latina immigrant farm workers in Miami-Dade County. Int. J. Environ. Res. Public Health 2019, 16, 1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Operario, D.; Yang, M.F.; Reisner, S.L.; Iwamoto, M.; Nemoto, T. Stigma and the syndemic of HIV-related health risk behaviors in a diverse sample of transgender women. J. Community Psychol. 2014, 42, 544–557. [Google Scholar] [CrossRef]
- Biello, K.B.; Colby, D.; Closson, E.; Mimiaga, M.J. The syndemic condition of psychosocial problems and HIV risk among male sex workers in Ho Chi Minh City, Vietnam. AIDS Behav. 2014, 18, 1264–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, X.; Sun, Q.; Fang, F.; Rao, Z.; Li, X.; Lv, Y.; Li, T.; Lin, A. The prevalence of depression associated with the infection status and sexual behaviors among men who have sex with men in Shenzhen, China: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulter, R.W.; Kinsky, S.M.; Herrick, A.L.; Stall, R.D.; Bauermeister, J.A. Evidence of syndemics and sexuality-related discrimination among young sexual-minority women. LGBT Health 2015, 2, 250–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrick, A.; Stall, R.; Egan, J.; Schrager, S.; Kipke, M. Pathways towards risk: Syndemic conditions mediate the effect of adversity on HIV risk behaviors among young men who have sex with men (YMSM). J. Urban Health 2014, 91, 969–982. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, J.J.; Fernández, M.I.; Fava, J.L.; Operario, D.; Rudy, B.J.; Wilson, P.A. Using syndemics theory to investigate risk and protective factors associated with condomless sex among youth living with HIV in 17 US cities. AIDS Behav. 2017, 21, 833–844. [Google Scholar] [CrossRef] [Green Version]
- Virtual AIDS Office of Hong Kong, Department of Health, The Government of the Hong Kong Special Administrative Region. HIV Surveillance and Epidemiology. Available online: http://www.info.gov.hk/aids/english/surveillance/latest_stat.htm (accessed on 20 May 2019).
- Hong Kong Advisory Council on AIDS. Recommended HIV/AIDS Strategies for Hong Kong 2017–2021. 2017. Available online: http://www.aca.gov.hk/english/strategies/pdf/strategies17-21.pdf (accessed on 20 May 2019).
- Lau, J.; Kim, J.; Lau, M.; Tsui, H. HIV related behaviours and attitudes among Chinese men who have sex with men in Hong Kong: A population based study. Sex. Transm. Infect. 2004, 80, 459–465. [Google Scholar] [CrossRef]
- Chan, W. AIDS and the Law: The Hong Kong Experience; Hong Kong Advisory Council on AIDS, the Government of the Hong Kong Special Administrative Region: Hong Kong, China, 1997.
- Mak, W.W.; Mo, P.K.; Cheung, R.Y.; Woo, J.; Cheung, F.M.; Lee, D. Comparative stigma of HIV/AIDS, SARS, and tuberculosis in Hong Kong. Soc. Sci. Med. 2006, 63, 1912–1922. [Google Scholar] [CrossRef]
- Lau, J.; Tsui, H.; Li, C.; Chung, R.; Chan, M.; Molassiotis, A. Needs assessment and social environment of people living with HIV/AIDS in Hong Kong. AIDS Care 2003, 15, 699–706. [Google Scholar] [CrossRef]
- Equal Opportunities Commission. Baseline Survey on Public Attitudes towards Persons with a Disability. 2010. Available online: http://www.eoc.org.hk/EOC/Upload/UserFiles/File/ResearchReport/201109/DisabilityReport(eng).pdf (accessed on 20 May 2019).
- Zhou, Y.R. “If you get AIDS You have to endure it alone”: Understanding the social constructions of HIV/AIDS in China. Soc. Sci. Med. 2007, 65, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Au, A.; Chan, I.; Li, P.; Chung, R.; Po, L.M.; Yu, P. Stress and health–related quality of life among HIV-infected persons in Hong Kong. AIDS Behav. 2004, 8, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, D.M. Does internalized heterosexism moderate the link between heterosexist events and lesbians’ psychological distress? Sex Roles 2006, 54, 227–234. [Google Scholar] [CrossRef]
- Veit, C.T.; Ware, J.E. The structure of psychological distress and well-being in general populations. J. Consult. Clin. Psychol. 1983, 51, 730–742. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Kuhns, L.M.; Hotton, A.L.; Garofalo, R.; Muldoon, A.L.; Jaffe, K.; Bouris, A.; Voisin, D.; Schneider, J. An index of multiple psychosocial, syndemic conditions is associated with antiretroviral medication adherence among HIV-positive youth. AIDS Patient Care STDs 2016, 30, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizuno, Y.; Purcell, D.W.; Knowlton, A.R.; Wilkinson, J.D.; Gourevitch, M.N.; Knight, K.R. Syndemic vulnerability, sexual and injection risk behaviors, and HIV continuum of care outcomes in HIV-positive injection drug users. AIDS Behav. 2015, 19, 684–693. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Social Sciences, 2nd ed.; Erlbaum: New York, NY, USA, 1988. [Google Scholar]
- Flora, D.B.; Curran, P.J. An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychol. Methods 2004, 9, 466–491. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.Y. Evaluating Cut off Criteria of Model Fit Indices for Latent Variable Models with Binary and Continuous Outcomes. Ph.D. Thesis, University of California, Los Angeles, CA, USA, 2002. [Google Scholar]
- George, D.; Mallery, M. SPSS for Windows Step by Step: A Simple Guide and Reference, 10th ed.; Pearson: Boston, MA, USA, 2010. [Google Scholar]
- Lau, J.T.; Tsui, H.; Ho, S.P.; Wong, E.; Yang, X. Prevalence of psychological problems and relationships with condom use and HIV prevention behaviors among Chinese female sex workers in Hong Kong. AIDS Care 2010, 22, 659–668. [Google Scholar] [CrossRef]
- Starks, T.J.; Millar, B.M.; Parsons, J.T. Predictors of condom use with main and casual partners among HIV-positive men over 50. Health Psychol. 2015, 34, 1116–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauermeister, J.A.; Hickok, A.M.; Meadowbrooke, C.; Veinot, T.; Loveluck, J. Self-efficacy among young men who have sex with men: An exploratory analysis of HIV/AIDS risk behaviors across partner types. AIDS Behav. 2014, 18, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kesteren, N.M.; Hospers, H.J.; van Empelen, P.; Van Breukelen, G.; Kok, G. Sexual decision-making in HIV-positive men who have sex with men: How moral concerns and sexual motives guide intended condom use with steady and casual sex partners. Arch. Sex. Behav. 2007, 36, 437–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auerbach, J.D. Principles of positive prevention. J. Acquir. Immune Defic. Syndr. 2004, 37, 122–125. [Google Scholar] [CrossRef]
- Yeo, T.E.D.; Chu, T.H. Social-cultural factors of HIV-related stigma among the Chinese general population in Hong Kong. AIDS Care 2017, 29, 1255–1259. [Google Scholar] [CrossRef]
- Kan, R.; Au, K.; Chan, W.; Cheung, L.; Lam, C.; Liu, H.; Ng, L.; Wong, M.; Wong, W. Homophobia in medical students of the University of Hong Kong. Sex Educ. 2009, 9, 65–80. [Google Scholar] [CrossRef]
- Yip, B.H.K.; Sheng, X.T.; Chan, V.W.Y.; Wong, L.H.L.; Lee, S.W.Y.; Abraham, A.A. ‘Let’s talk about sex’—A knowledge, attitudes and practice study among paediatric nurses about teen sexual health in Hong Kong. J. Clin. Nurs. 2015, 24, 2591–2600. [Google Scholar] [CrossRef]
- Hong Kong Advisory Council on AIDS. Recommended HIV/AIDS Strategies for Hong Kong 2012–2016. 2012. Available online: http://www.chp.gov.hk/files/pdf/spp_g253.pdf (accessed on 20 May 2019).
- Hankivsky, O.; Grace, D.; Hunting, G.; Giesbrecht, M.; Fridkin, A.; Rudrum, S.; Ferlatte, O.; Clark, N. An intersectionality-based policy analysis framework: Critical reflections on a methodology for advancing equity. Int. J. Equity Health 2014, 13, 119. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.C.H.; Mak, W.W.S. Cognitive, regulatory, and interpersonal mechanisms of HIV stigma on the mental and social health of men who have sex with men living with HIV. Am. J. Men’s Health 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Ferlatte, O.; Salway, T.; Trussler, T.; Oliffe, J.L.; Gilbert, M. Combining intersectionality and syndemic theory to advance understandings of health inequities among Canadian gay, bisexual and other men who have sex with men. Crit. Public Health 2018, 28, 509–521. [Google Scholar] [CrossRef]
- Watkins-Hayes, C. Intersectionality and the sociology of HIV/AIDS: Past, present, and future research directions. Annu. Rev. Sociol. 2014, 40, 431–457. [Google Scholar] [CrossRef]
- Mustanski, B.; Phillips, G.; Ryan, D.T.; Swann, G.; Kuhns, L.; Garofalo, R. Prospective effects of a syndemic on HIV and STI incidence and risk behaviors in a cohort of young men who have sex with men. AIDS Behav. 2017, 21, 845–857. [Google Scholar] [CrossRef] [Green Version]
- Mustanski, B.; Andrews, R.; Herrick, A.; Stall, R.; Schnarrs, P.W. A syndemic of psychosocial health disparities and associations with risk for attempting suicide among young sexual minority men. Am. J. Public Health 2014, 104, 287–294. [Google Scholar] [CrossRef]
- Chou, K.L. Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Personal. Individ. Differ. 2000, 28, 299–307. [Google Scholar] [CrossRef]
- Liang, J.; Wu, S.C.; Krause, N.M.; Chiang, T.L.; Wu, H.Y. The structure of the mental health inventory among Chinese in Taiwan. Med. Care 1992, 30, 659–676. [Google Scholar] [CrossRef] [PubMed]
- Rojas, P.; Huang, H.; Li, T.; Ravelo, G.J.; Sanchez, M.; Dawson, C.; Brook, J.; Kanamori, M.; De La Rosa, M. Sociocultural determinants of risky sexual behaviors among adult Latinas: A longitudinal study of a community-based sample. Int. J. Environ. Res. Public Health 2016, 13, 1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosby, R.A.; DiClemente, R.J.; Salazar, L.F.; Wingood, G.M.; McDermott-Sales, J.; Young, A.M.; Rose, E. Predictors of consistent condom use among young African American women. AIDS Behav. 2013, 17, 865–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H. Antiretroviral therapy for the prevention of HIV-1 transmission. N. Engl. J. Med. 2016, 375, 830–839. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Characteristics | n (%)/M (SD) |
|---|---|
| Gender | |
| Male | 277 (95.8%) |
| Female | 12 (4.2%) |
| Age | 41.8 years (11.1 years) |
| Ethnicity | |
| Chinese | 271 (94.8%) |
| South Asian | 6 (2.1%) |
| Caucasian | 6 (2.1%) |
| Others | 3 (1.0%) |
| Education | |
| Secondary education or less | 138 (48.3%) |
| Tertiary education | 133 (46.5%) |
| Employment status | |
| Full-time employment | 183 (63.3%) |
| Part-time or irregular employment | 46 (15.9%) |
| Unemployed | 36 (12.5%) |
| Others | 24 (8.3%) |
| Marital status | |
| Single | 194 (67.4%) |
| Cohabiting/Married | 76 (26.4%) |
| Separated/Divorced/Widowed | 20 (6.9%) |
| Sexual orientation | |
| Heterosexual | 68 (23.7%) |
| Gay | 141 (49.1%) |
| Bisexual | 70 (24.4%) |
| Questioning | 8 (2.8%) |
| Length of being diagnosed with HIV infection | 5.25 years (4.70 years) |
| Use of antiretroviral therapy | |
| Yes | 254 (90.1%) |
| No | 28 (9.9%) |
| Number of psychosocial syndemic problem(s) | |
| 0 | 86 (29.6%) |
| 1 | 126 (43.3%) |
| 2 | 54 (18.6%) |
| 3 | 21 (7.2%) |
| 4 | 4 (1.4%) |
| Condom use with steady partners | |
| Consistent condom use | 28 (25.9%) |
| Inconsistent condom use | 80 (74.1%) |
| Condom use with casual partners | |
| Consistent condom use | 20 (18.7%) |
| Inconsistent condom use | 87 (81.3%) |
| Variable | All Participants (N = 291) | Had HIV-Related Discrimination (n = 94) | Did not Have HIV-Related Discrimination (n = 197) | Independent Samples t-Test | Pearson Correlation Coefficients | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Skewness | Kurtosis | Mean (SD) | Mean (SD) | t-Value | Cohen’s d | 1 | 2 | 3 | 4 | |
| 1. Depression (1–6) | 2.41 | 0.90 | 0.79 | 1.34 | 2.70 (0.95) | 2.28 (0.84) | 3.81 ** | 0.47 | - | |||
| 2. Anxiety (1–6) | 2.57 | 0.87 | 0.37 | −0.06 | 2.76 (0.82) | 2.49 (0.88) | 2.50 * | 0.32 | 0.78 ** | - | ||
| 3. Social isolation (1–7) | 3.27 | 1.08 | 0.52 | 0.36 | 3.57 (1.14) | 3.12 (1.02) | 3.39 ** | 0.42 | 0.31 ** | 0.32 ** | - | |
| 4. Self-stigma (1–6) | 3.82 | 1.16 | −0.34 | −0.53 | 4.00 (1.19) | 3.74 (1.14) | 1.80 | 0.22 | 0.36 ** | 0.35 ** | 0.31 ** | - |
| Variable | Psychosocial Syndemics (N = 291) | Inconsistent Condom Use with Steady Partners (n = 108) | Inconsistent Condom Use with Casual Partners (n = 107) | |||
|---|---|---|---|---|---|---|
| IRR | (95% CI) | AOR | (95% CI) | AOR | (95% CI) | |
| HIV-related discrimination | ||||||
| Yes | 1.47 ** | (1.14, 1.89) | 5.40 * | (1.09, 26.70) | 3.24 | (0.70, 15.00) |
| No (reference category) | 1.00 | 1.00 | 1.00 | |||
| Psychosocial syndemics | - | - | 3.09 * | (1.22, 7.82) | 0.95 | (0.48, 1.90) |
| Gender | ||||||
| Male | 1.73 | (0.79, 3.78) | 14.54 | (0.40, 524.99) | - | - |
| Female (reference category) | 1.00 | 1.00 | - | - | ||
| Age | 1.00 | (0.99, 1.01) | 0.98 | (0.89, 1.07) | 1.05 | (0.97, 1.13) |
| Ethnicity | ||||||
| Chinese | 1.05 | (0.58, 1.89) | 0.32 | (0.02, 4.74) | - | - |
| Ethnic minority (reference category) | 1.00 | 1.00 | - | - | ||
| Education | ||||||
| Secondary education or less (reference category) | 1.00 | 1.00 | 1.00 | |||
| Tertiary education | 0.76 | (0.58, 1.00) | 2.62 | (0.52, 13.20) | 0.99 | (0.23, 4.36) |
| Employment status | ||||||
| Full-/part-time employment | 0.94 | (0.69, 1.27) | 0.30 | (0.05, 1.91) | 1.90 | (0.37, 9.68) |
| Not in employment | 1.00 | 1.00 | 1.00 | |||
| Marital status | ||||||
| Single (reference category) | 1.00 | 1.00 | 1.00 | |||
| Cohabiting/Married | 0.88 | (0.64, 1.22) | 0.11 * | (0.02, 0.58) | 0.24 * | (0.06, 0.99) |
| Separated/Divorced/Widowed | 0.98 | (0.57, 1.69) | 0.09 | (0.01, 1.19) | - | - |
| Sexual orientation | ||||||
| Heterosexual | 1.06 | (0.76, 1.50) | 0.13 * | (0.02, 0.94) | 1.33 | (.13, 13.79) |
| Sexual minority (reference category) | 1.00 | 1.00 | 1.00 | |||
| Length of being diagnosed with HIV infection | 1.00 | (1.00, 1.00) | 1.00 | (0.99, 1.02) | 0.98 * | (0.97, 1.00) |
| Antiretroviral medication use | ||||||
| Yes | 1.37 | (0.85, 2.20) | 3.98 | (0.38, 41.80) | 1.61 | (0.14, 18.41) |
| No (reference category) | 1.00 | 1.00 | 1.00 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, R.C.H.; Operario, D.; Mak, W.W.S. Effects of HIV-Related Discrimination on Psychosocial Syndemics and Sexual Risk Behavior among People Living with HIV. Int. J. Environ. Res. Public Health 2020, 17, 1924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061924
Chan RCH, Operario D, Mak WWS. Effects of HIV-Related Discrimination on Psychosocial Syndemics and Sexual Risk Behavior among People Living with HIV. International Journal of Environmental Research and Public Health. 2020; 17(6):1924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061924
Chicago/Turabian StyleChan, Randolph C. H., Don Operario, and Winnie W. S. Mak. 2020. "Effects of HIV-Related Discrimination on Psychosocial Syndemics and Sexual Risk Behavior among People Living with HIV" International Journal of Environmental Research and Public Health 17, no. 6: 1924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061924