Nurses’ Adherence to Patient Safety Principles: A Systematic Review

 ,
,  , , and
, , and 
Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Design
2.2. Search Methods
2.3. Search Outcome and Data Extraction
2.4. Quality Appraisal
2.5. Data Abstraction and Synthesis
3. Results
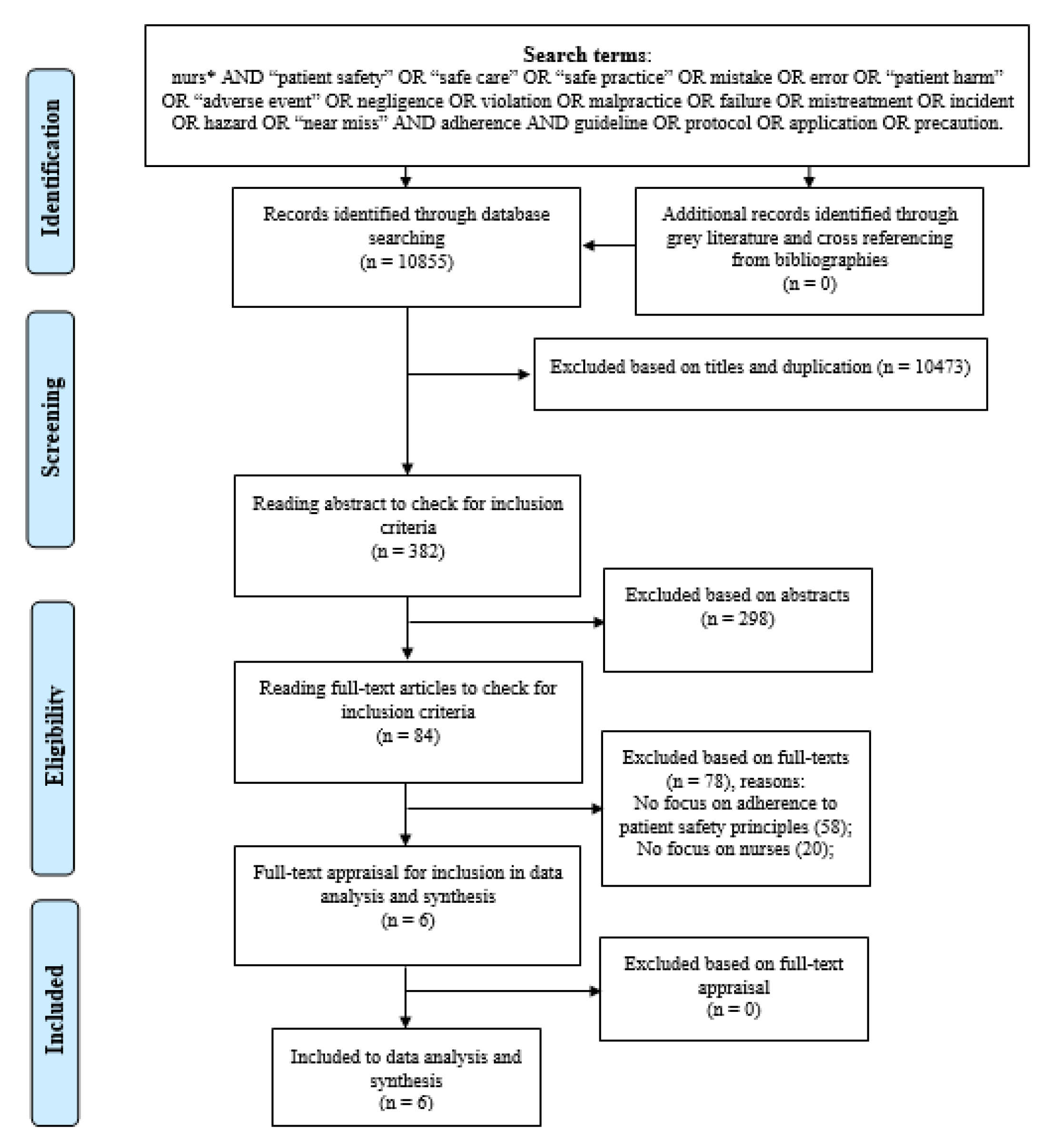
3.1. Search Results and Study Selections
3.2. General Characteristics of the Selected Studies
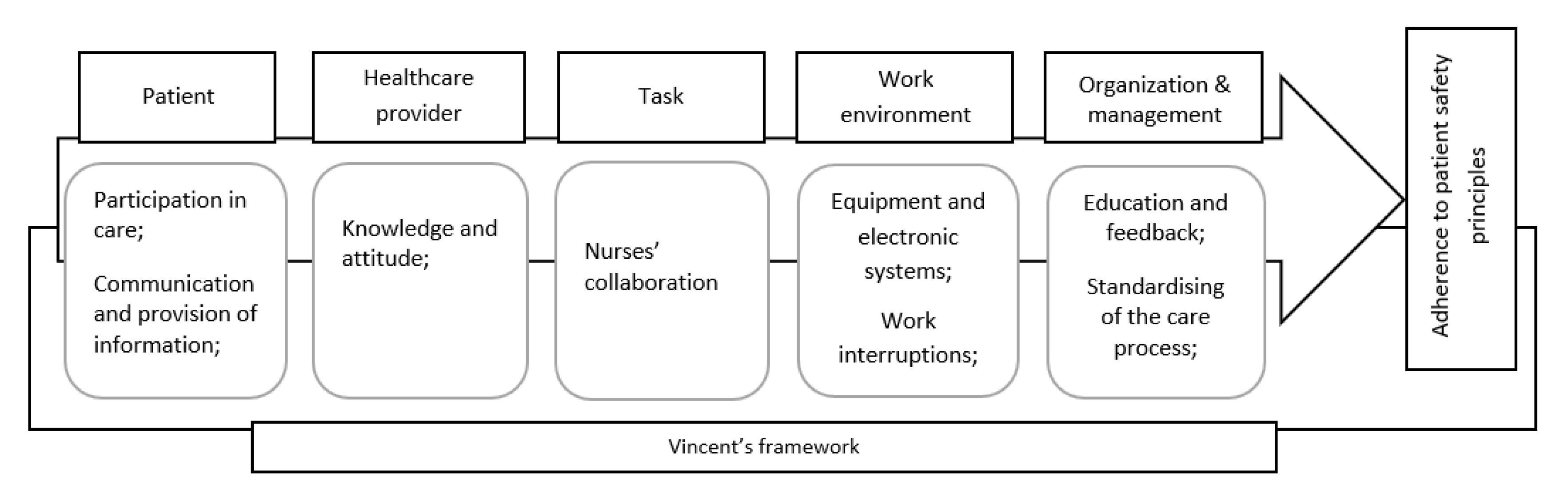
3.3. Findings of Studies with Connection to the Vincent’s Framework
3.3.1. Patient
3.3.2. Healthcare Provider
3.3.3. Task
3.3.4. Work Environment
3.3.5. Organisation and Management
4. Discussion
Limitations and Suggestions for Future Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Database | Total in Each Database | Selection Based on Title Reading | Selection Based on Abstract Reading | Selection Based on Full-Text Reading/Appraisal |
|---|---|---|---|---|
| ProQuest | 3169 | 0 | 0 | 0 |
| CINAHL | 4271 | 40 | 8 | 1 |
| EBSCO | 673 | 7 | 5 | 0 |
| PubMed [including Medline] | 33 | 27 | 20 | 1 |
| PsycINFO | 442 | 42 | 6 | 0 |
| Scopus | 1387 | 203 | 33 | 2 |
| Web of Science | 856 | 62 | 11 | 1 |
| Norwegian databases | ||||
| Oria | 4 | 0 | 0 | 0 |
| Idunn | 0 | 0 | 0 | 0 |
| Norart | 0 | 0 | 0 | 0 |
| Helsebiblioteket.no | 1 | 0 | 0 | 0 |
| Cristin | 4 | 0 | ||
| Finnish database—Medic | 15 | 1 | 1 | 1 |
| Manual search/backtracking references | 0 | 0 | 0 | 0 |
| Total of databases | 10855 | 382 | 84 | 6 |
References
- World Heath Organization (WHO). Patient Safety. 2019. Available online: https://www.who.int/patientsafety/en/ (accessed on 24 December 2019).
- Harvard Global Health Institute. Patient Safety: A Major Public Health Challenge. Available online: https://globalhealth.harvard.edu/qualitypowerpoint (accessed on 8 March 2020).
- Adler, L.; Yi, D.; Li, M.; McBroom, B.; Hauck, L.; Sammer, C.; Jones, C.; Shaw, T.; Classen, D. Impact of Inpatient Harms on Hospital Finances and Patient Clinical Outcomes. J. Patient Saf. 2018, 14, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Slawomirski, L.; Auraaen, A.; Klazinga, N.S. The Economics of Patient Safety. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/social-issues-migration-health/the-economics-of-patient-safety_5a9858cd-en (accessed on 19 March 2020).
- Rodziewicz, T.L.; Hipskind, J.E. Medical Error Prevention. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Emanuel, L.; Berwick, D.; Conway, J.; Combes, J.; Hatlie, M.; Leape, L.; Reason, P.; Schyve, P.; Vincent, C.; Walton, M. What Exactly is Patient Safety. In Advances in Patient Safety: New Directions and Alternative Approaches; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Sibal, A.; Uberoi, R.S.; Malani, A. An approach to improve patient safety and quality beyond accreditation. World Hosp. Health Serv. 2016, 52, 10–12. [Google Scholar] [PubMed]
- Mitchell, P. Defining Patient Safety and Quality Care. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Kanerva, A.; Kivinen, T.; Lammintakanen, J. Collaborating with nurse leaders to develop patient safety practices. Leadersh Health Serv. 2017, 30, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M. Why is Patient Safety so Hard? A Selective Review of Ethnographic Studies. J. Health Serv. Res. Policy 2010, 15, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Gillespie, B.M.; Chaboyer, W.; Li, Y.; Whitelock, K.; Morley, N.; Morrissey, S.; O’Callaghan, F.; Marshall, A.P. Preventing surgical site infections: Facilitators and barriers to nurses’ adherence to clinical practice guidelines—A qualitative study. J. Clin. Nurs. 2019, 28, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Sermeus, W. Understanding the role of nurses in patient safety: From evidence to policy with RN4CAST. BMC Nurs. 2016, 15, 1. [Google Scholar]
- Henneman, E.A. Recognizing the Ordinary as Extraordinary: Insight into the “Way We Work” to Improve Patient Safety Outcomes. Am. J. Crit. Care 2017, 26, 272–277. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jordan, S.; Kangasniemi, M. Patient participation in patient safety and nursing input—a systematic review. J. Clin. Nurs. 2015, 24, 627–639. [Google Scholar] [CrossRef] [Green Version]
- International Council of Nurses (ICN). Patient Safety-ICN Position. 2019. Available online: https://www.icn.ch/sites/default/files/inline-files/D05_Patient_Safety_0.pdf (accessed on 24 December 2019).
- Rashvand, F.; Ebadi, A.; Vaismoradi, M.; Salsali, M.; Yekaninejad, M.S.; Griffiths, P.; Sieloff, C. The assessment of safe nursing care: Development and psychometric evaluation. J. Nurs. Manag. 2017, 25, 22–36. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Salsali, M.; Turunen, H.; Bondas, T. A qualitative study on Iranian nurses’ experiences and perspectives on how to provide safe care in clinical practice. J. Res. Nurs. 2013, 18, 351–365. [Google Scholar] [CrossRef]
- Efstathiou, G.; Papastavrou, E.; Raftopoulos, V.; Merkouris, A. Factors influencing nurses’ compliance with Standard Precautions in order to avoid occupational exposure to microorganisms: A focus group study. BMC Nurs. 2011, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, R.B.; Sackett, D.L.; Taylor, D.W. Compliance in Health Care; John Hopkins University Press: Baltimore, MD, USA, 1979. [Google Scholar]
- Playle, J.F.; Keeley, P. Non-compliance and professional power. J. Adv. Nurs. 1998, 27, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Hessels, A.J.; Larson, E.L. Relationship between patient safety climate and standard precaution adherence: A systematic review of the literature. J. Hosp. Infect. 2016, 92, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Jam, R.; Mesquida, J.; Hernández, Ó.; Sandalinas, I.; Turégano, C.; Carrillo, E.; Pedragosa, R.; Valls, J.; Parera, A.; Ateca, B.; et al. Nursing workload and compliance with non-pharmacological measures to prevent ventilator-associated pneumonia: A multicentre study. Nurs. Crit. Care 2018, 23, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Jimmieson, N.L.; Tucker, M.K.; White, K.M.; Liao, J.; Campbell, M.; Brain, D.; Page, K.; Barnett, A.G.; Graves, N. The role of time pressure and different psychological safety climate referents in the prediction of nurses’ hand hygiene compliance. Saf. Sci. 2016, 82, 29–43. [Google Scholar] [CrossRef]
- Zhang, S.; Kong, X.; Lamb, K.V.; Wu, Y. High nursing workload is a main associated factor of poor hand hygiene adherence in Beijing, China: An observational study. Int. J. Nurs. Pract. 2019, 25, e12720. [Google Scholar] [CrossRef]
- Schutijser, B.; Klopotowska, J.E.; Jongerden, I.; Spreeuwenberg, P.; Wagner, C.; de Bruijne, M. Nurse compliance with a protocol for safe injectable medication administration: Comparison of two multicentre observational studies. BMJ Open 2018, 8, e019648. [Google Scholar] [CrossRef] [Green Version]
- Jun, J.; Kovner, C.T.; Stimpfel, A.W. Barriers and facilitators of nurses’ use of clinical practice guidelines: An integrative review. Int. J. Nurs. Stud. 2016, 60, 54–68. [Google Scholar] [CrossRef]
- Vincent, C.; Taylor-Adams, S.; Stanhope, N. Framework for analysing risk and safety in clinical medicine. BMJ 1998, 316, 1154–1157. [Google Scholar] [CrossRef] [Green Version]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef] [Green Version]
- van Beuzekom, M.; Boer, F.; Akerboom, S.; Hudson, P. Patient safety: Latent risk factors. BJA Br. J. Anaesth. 2010, 105, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Vincent, C.; Burnett, S.; Carthey, J. Safety measurement and monitoring in healthcare: A framework to guide clinical teams and healthcare organisations in maintaining safety. BMJ Qual. Saf. 2014, 23, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Kutney-Lee, A.; Kelly, D. The effect of hospital electronic health record adoption on nurse-assessed quality of care and patient safety. J. Nurs. Adm. 2011, 41, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Strudwick, G.; Reisdorfer, E.; Warnock, C.; Kalia, K.; Sulkers, H.; Clark, C.; Booth, R. Factors Associated With Barcode Medication Administration Technology That Contribute to Patient Safety: An Integrative Review. J. Nurs. Care Qual. 2018, 33, 79–85. [Google Scholar] [CrossRef]
- Hessels, A.J.; Wurmser, T. Relationship among safety culture, nursing care, and Standard Precautions adherence. Am. J. Infect. Control 2019. [Google Scholar] [CrossRef]
- Evans, D. Systematic reviews of nursing research. Intensive Crit. Care Nurs. 2001, 17, 51–57. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S.E. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1 [updated March 2011]. 2011. Available online: http://handbook-5-1.cochrane.org/ (accessed on 19 March 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Gardner, C.L. Adherence: A concept analysis. Int. J. Nurs. Knowl. 2015, 26, 96–101. [Google Scholar] [CrossRef]
- Brown, M.T.; Bussell, J.; Dutta, S.; Davis, K.; Strong, S.; Mathew, S. Medication Adherence: Truth and Consequences. Am. J. Med. Sci. 2016, 351, 387–399. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.M.; Suarez-Cuervo, C.; Berger, Z.; Lee, J.; Gayleard, J.; Rosenberg, C.; Nagy, N.; Weeks, K.; Dy, S. Evaluation of Patient and Family Engagement Strategies to Improve Medication Safety. Patient 2018, 11, 193–206. [Google Scholar] [CrossRef]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. Biomed. Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [Green Version]
- Roter, D.L.; Wolff, J.; Wu, A.; Hannawa, A.F. Patient and family empowerment as agents of ambulatory care safety and quality. BMJ Qual. Saf. 2017, 26, 508–512. [Google Scholar] [CrossRef]
- Sharma, A.E.; Rivadeneira, N.A.; Barr-Walker, J.; Stern, R.J.; Johnson, A.K.; Sarkar, U. Patient Engagement in Health Care Safety: An Overview Of Mixed-Quality Evidence. Health Aff. 2018, 37, 1813–1820. [Google Scholar] [CrossRef]
- Bissonnette, J.M. Adherence: A concept analysis. J. Adv. Nurs. 2008, 63, 634–643. [Google Scholar] [CrossRef]
- Kyngäs, H.; Duffy, M.E.; Kroll, T. Conceptual analysis of compliance. J. Clin. Nurs. 2000, 9, 5–12. [Google Scholar] [CrossRef]
- EQUATOR Network. Enhancing the QUAlity and Transparency of health Research. 2019. Available online: http://www.equator-network.org/ (accessed on 4 November 2019).
- Hawker, S.; Payne, S.; Kerr, C.; Hardey, M.; Powell, J. Appraising the evidence: Reviewing disparate data systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Vincent, C. Patient Safety, 2nd ed.; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar]
- Graan, S.M.; Botti, M.; Wood, B.; Redley, B. Nursing handover from ICU to cardiac ward: Standardised tools to reduce safety risks. Aust. Crit. Care 2016, 29, 165–171. [Google Scholar] [CrossRef]
- Rintala, E.; Laurikainen, E.; Kaarto, A.-M.; Routamaa, M. Adherence to surgical hand rubbing directives in a hospital district of Southwest Finland. Suomen Lääkärilehti 2014. [Google Scholar] [CrossRef]
- Fålun, N.; Oterhals, K.; Pettersen, T.; Brørs, G.; Olsen, S.S.; Norekvål, T.M.; TELMON-NOR Investigators. Cardiovascular nurses’ adherence to practice standards in in-hospital telemetry monitoring. Nurs. Crit. Care 2020, 25, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.-H.; Ahn, J.-W.; Son, Y.-J. Association between Hospital Nurses’ Perception of Patient Safety Management and Standard Precaution Adherence: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 4744. [Google Scholar] [CrossRef] [Green Version]
- Förberg, U.; Wallin, L.; Johansson, E.; Ygge, B.-M.; Backheden, M.; Ehrenberg, A. Relationship between work context and adherence to a clinical practice guideline for peripheral venous catheters among registered nurses in pediatric care. Worldviews Evid. Based Nurs. 2014, 11, 227–239. [Google Scholar] [CrossRef]
- Alsulami, Z.; Choonara, I.; Conroy, S. Paediatric nurses’ adherence to the double-checking process during medication administration in a children’s hospital: An observational study. J. Adv. Nurs. 2014, 70, 1404–1413. [Google Scholar] [CrossRef]
- Ijkema, R.; Langelaan, M.; van de Steeg, L.; Wagner, C. Do patient characteristics influence nursing adherence to a guideline for preventing delirium? J. Nurs. Scholarsh. 2014, 46, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Tobiano, G.; Bucknall, T.; Marshall, A.; Guinane, J.; Chaboyer, W. Nurses’ views of patient participation in nursing care. J. Adv. Nurs. 2015, 71, 2741–2752. [Google Scholar] [CrossRef] [Green Version]
- Malfait, S.; Eeckloo, K.; Van Biesen, W.; Van Hecke, A. The effectiveness of bedside handovers: A multilevel, longitudinal study of effects on nurses and patients. J. Adv. Nurs. 2019, 75, 1690–1701. [Google Scholar] [CrossRef]
- Cathro, H. Navigating Through Chaos: Charge Nurses and Patient Safety. J. Nurs. Adm. 2016, 46, 208–214. [Google Scholar] [CrossRef]
- Gaffney, T.A.; Hatcher, B.J.; Milligan, R. Nurses’ role in medical error recovery: An integrative review. J. Clin. Nurs. 2016, 25, 906–917. [Google Scholar] [CrossRef]
- Ribeiro, L.; Fernandes, G.C.; Souza, E.G.d.; Souto, L.C.; Santos, A.S.P.D.; Bastos, R.R. Safe surgery checklist: Filling adherence, inconsistencies, and challenges. Rev. Col. Bras. Cir. 2019, 46, e20192311. [Google Scholar] [CrossRef] [Green Version]
- Simons, P.A.M.; Houben, R.; Benders, J.; Pijls-Johannesma, M.; Vandijck, D.; Marneffe, W.; Backes, H.; Groothuis, S. Does compliance to patient safety tasks improve and sustain when radiotherapy treatment processes are standardized? Eur. J. Oncol. Nurs. 2014, 18, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Manser, T. Teamwork and patient safety in dynamic domains of healthcare: A review of the literature. Acta Anaesthesiol. Scand. 2009, 53, 143–151. [Google Scholar] [CrossRef]
- O’Brien, B.; Graham, M.M.; Kelly, S.M. Exploring nurses’ use of the WHO safety checklist in the perioperative setting. J. Nurs. Manag. 2017, 25, 468–476. [Google Scholar] [CrossRef]
- Massey, D.; Chaboyer, W.; Anderson, V. What factors influence ward nurses’ recognition of and response to patient deterioration? An integrative review of the literature. Nurs. Open 2016, 4, 6–23. [Google Scholar] [CrossRef] [Green Version]
- Ross, C.; Rogers, C.; King, C. Safety culture and an invisible nursing workload. Collegian 2019, 26, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Tunlind, A.; Granström, J.; Engström, Å. Nursing care in a high-technological environment: Experiences of critical care nurses. Intensive Crit. Care Nurs. 2015, 31, 116–123. [Google Scholar] [CrossRef]
- Lee, T.-Y.; Sun, G.-T.; Kou, L.-T.; Yeh, M.-L. The use of information technology to enhance patient safety and nursing efficiency. Technol. Health Care 2017, 25, 917–928. [Google Scholar] [CrossRef]
- Pirinen, H.; Kauhanen, L.; Danielsson-Ojala, R.; Lilius, J.; Tuominen, I.; Díaz Rodríguez, N.; Salanterä, S. Registered Nurses’ Experiences with the Medication Administration Process. Adv. Nurs. 2015, 941589. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zheng, J.; Liu, K.; Baggs, J.G.; Liu, J.; Wu, Y.; You, L. Hospital nursing organizational factors, nursing care left undone, and nurse burnout as predictors of patient safety: A structural equation modeling analysis. Int. J. Nurs. Stud. 2018, 86, 82–89. [Google Scholar] [CrossRef]
- Usher, K.; Woods, C.; Parmenter, G.; Hutchinson, M.; Mannix, J.; Power, T.; Chaboyer, W.; Latimer, S.; Mills, J.; Siegloff, L.; et al. Self-reported confidence in patient safety knowledge among Australian undergraduate nursing students: A multi-site cross-sectional survey study. Int. J. Nurs. Stud. 2017, 71, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Schutijser, B.C.F.M.; Klopotowska, J.E.; Jongerden, I.P.; Spreeuwenberg, P.M.M.; De Bruijne, M.C.; Wagner, C. Interruptions during intravenous medication administration: A multicentre observational study. J. Adv. Nurs. 2019, 75, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Havaei, F.; MacPhee, M.; Lee, S.E. The effect of violence prevention strategies on perceptions of workplace safety: A study of medical-surgical and mental health nurses. J. Adv. Nurs. 2019, 75, 1657–1666. [Google Scholar] [CrossRef]
- Manapragada, A.; Bruk-Lee, V.; Thompson, A.H.; Heron, L.M. When safety climate is not enough: Examining the moderating effects of psychosocial hazards on nurse safety performance. J. Adv. Nurs. 2019, 75, 1207–1218. [Google Scholar] [CrossRef]
- Kim, J.; Bates, D.W. Medication administration errors by nurses: Adherence to guidelines. J. Clin. Nurs. 2013, 22, 590–598. [Google Scholar] [CrossRef]
- Aveling, E.-L.; Parker, M.; Dixon-Woods, M. What is the role of individual accountability in patient safety? A multi-site ethnographic study. Sociol. Health Illn. 2016, 38, 216–232. [Google Scholar] [CrossRef] [Green Version]
- DiCuccio, M.H. The Relationship Between Patient Safety Culture and Patient Outcomes: A Systematic Review. J. Patient Saf. 2015, 11, 135–142. [Google Scholar] [CrossRef]
- Gurková, E.; Zeleníková, R.; Friganovic, A.; Uchmanowicz, I.; Jarošová, D.; Papastavrou, E.; Žiaková, K. Hospital safety climate from nurses’ perspective in four European countries. Int. Nurs. Rev. 2019. [Google Scholar] [CrossRef]
- Hessels, A.J.; Genovese-Schek, V.; Agarwal, M.; Wurmser, T.; Larson, E.L. Relationship between patient safety climate and adherence to standard precautions. Am. J. Infect. Control 2016, 44, 1128–1132. [Google Scholar] [CrossRef] [Green Version]
- Doronina, O.; Jones, D.; Martello, M.; Biron, A.; Lavoie-Tremblay, M. A Systematic Review on the Effectiveness of Interventions to Improve Hand Hygiene Compliance of Nurses in the Hospital Setting. J. Nurs. Scholarsh. 2017, 49, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Martos-Cabrera, M.B.; Mota-Romero, E.; Martos-García, R.; Gómez-Urquiza, J.L.; Suleiman-Martos, N.; Albendín-García, L.; Cañadas-De la Fuente, G.A. Hand Hygiene Teaching Strategies among Nursing Staff: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3039. [Google Scholar] [CrossRef] [Green Version]
- Shimoni, Z.; Kama, N.; Mamet, Y.; Glick, J.; Dusseldorp, N.; Froom, P. Empowering surgical nurses improves compliance rates for antibiotic prophylaxis after caesarean birth. J. Adv. Nurs. 2009, 65, 2345–2349. [Google Scholar] [CrossRef]
- Leotsakos, A.; Zheng, H.; Croteau, R.; Loeb, J.M.; Sherman, H.; Hoffman, C.; Morganstein, L.; O’Leary, D.; Bruneau, C.; Lee, P.; et al. Standardization in patient safety: The WHO High 5s project. Int. J. Qual. Health Care 2014, 26, 109–116. [Google Scholar] [CrossRef] [Green Version]


| Authors, Year, Country | Aim | Method | Sample and Setting | Main Finding | Conclusion |
|---|---|---|---|---|---|
| Förberg et al., 2014, Sweden [52] | To investigate nurses’ adherence to the clinical practice guidelines regarding peripheral venous catheters and investigate their understandings of work context influencing it. | Survey | A children’s hospital with 245 beds, 373 nurses from 23 medical and surgical inpatient, intensive care, the operating, anaesthetic, advanced homecare, and outpatient wards. | The importance of the workplace condition in terms of information sharing and feedback. | The need for various strategies for improving adherence among nurses. |
| Rintala et al., 2014, Finland [49] | To evaluate adherence to surgical hand rubbing directives among operating room personnel, in public hospitals in Southwest Finland. | Observational before-after intervention | 11 surgical settings of four hospitals, 190 and 73 nurses in the first and second observation rounds, respectively. | The relative impact of the feedback intervention on adherence by nurses. | Necessity of effective educational methods and role models. |
| Alsulami et al., 2014, UK [53] | To explore the follow-up of double-checking policies by nurses and assess the identity of medication-administration errors despite double-checking. | Prospective observational | Medical and surgical wards, the PICU and NICU, observation of preparation and administration of 2000 drug doses to 876 children. | Deviations from the policies of medication administration. | Encouragement of double-checking steps during medication administration, and prevention of interruptions. |
| Graan et al., 2016, Australia [48] | To investigate the adoption of standardised nursing handover guidelines from the ICU to the cardiac ward in regard to understanding risks to patient safety before and after the implementation. | Three-stage, pre–post time series, and focus group interviews pre-and/or post-implementation. | A metropolitan private hospital with a 15-bed ICU and a 46-bed cardiac surgical ward; 20 consecutive episodes of ICU-to-ward handover and a further 20 post-implementation episodes; A purposive sample of 19 senior nurse managers and clinicians. | Unsafe practice of handover interventions and information gap. | The need for the adoption of standardised handover tools for reducing handover variabilities. |
| Fålun et al., 2019, Norway [50] | To study cardiovascular nurses’ knowledge of, and adherence to, practice standards for cardiac surveillance and their knowledge improvements over time, in years 2011 and 2017. | Survey | 363 nurses from 44 hospitals in 2011 and 38 hospitals in 2017. | Failure to fully adhere to cardiac telemetry monitoring standards. | Developing educational programmes regarding the safe practice of cardiac monitoring. |
| Lim et al., 2019, South Korea [51] | To investigate nurses’ adherence to standard precautions and its association with their perceptions of safe care. | Cross-sectional | 329 nurses working in a teaching hospital. | Intermediate adherence to standard precautions. | Devising integrative curricula to improve nurses’ transition to professional practice. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaismoradi, M.; Tella, S.; A. Logan, P.; Khakurel, J.; Vizcaya-Moreno, F. Nurses’ Adherence to Patient Safety Principles: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062028
Vaismoradi M, Tella S, A. Logan P, Khakurel J, Vizcaya-Moreno F. Nurses’ Adherence to Patient Safety Principles: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(6):2028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062028
Chicago/Turabian StyleVaismoradi, Mojtaba, Susanna Tella, Patricia A. Logan, Jayden Khakurel, and Flores Vizcaya-Moreno. 2020. "Nurses’ Adherence to Patient Safety Principles: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 6: 2028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062028