Cohort Profile: Effectiveness of a 12-Month Patient-Centred Medical Home Model Versus Standard Care for Chronic Disease Management among Primary Care Patients in Sydney, Australia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
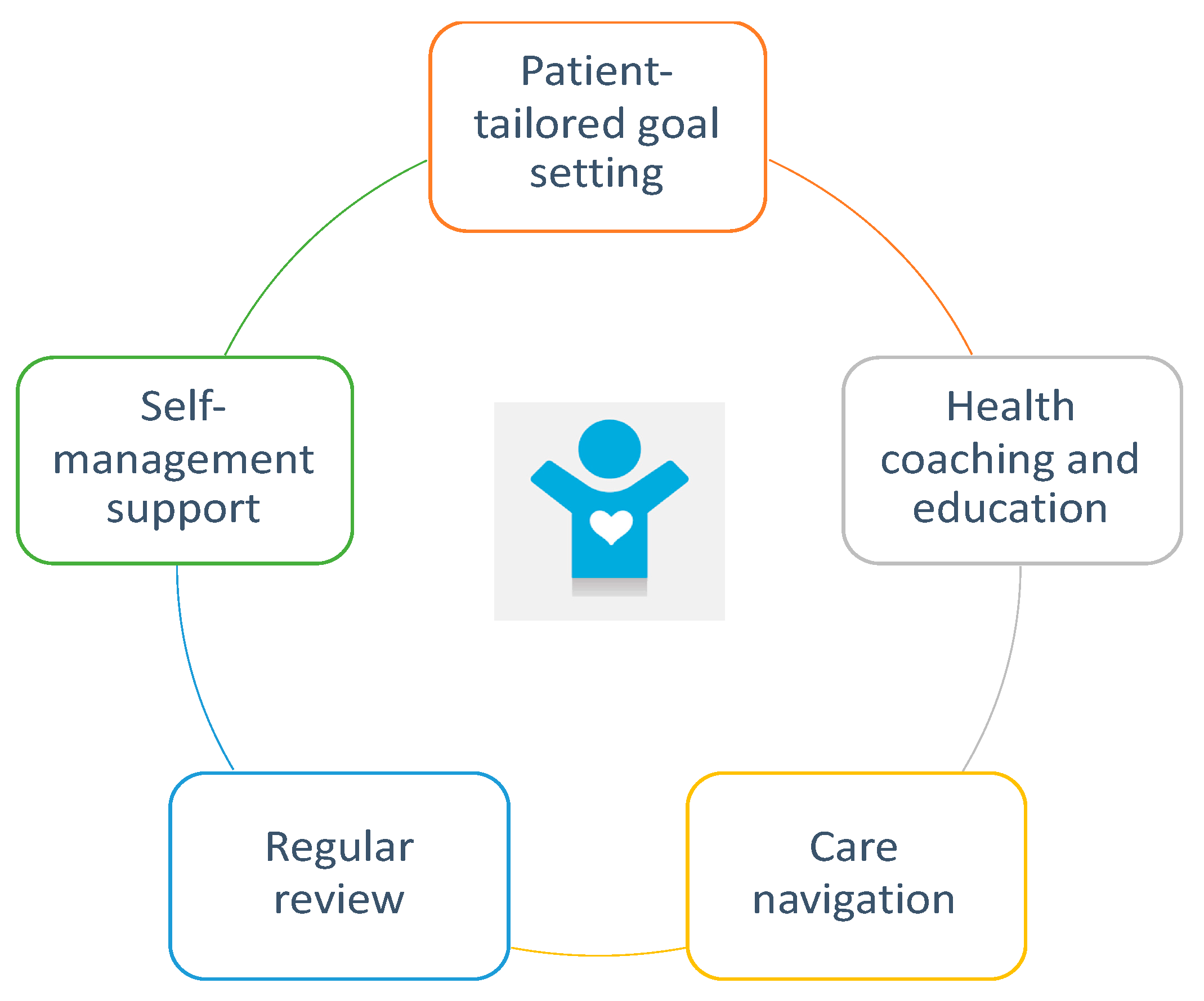
2.1. Design of the WellNet Chronic Disease Management (CDM) Program
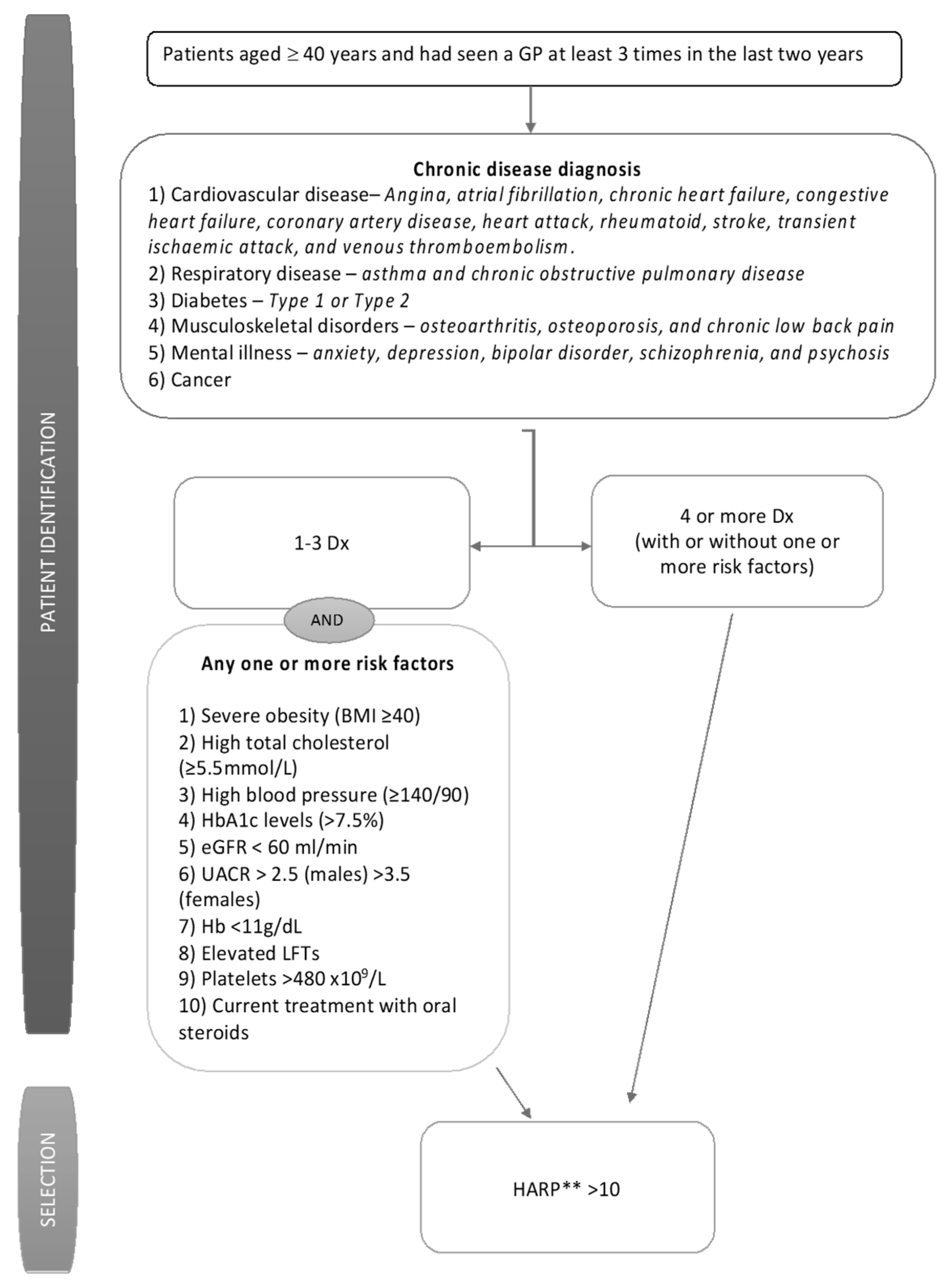
- Patient identification and enrolment;
- Patient centred integrated care;
- Outcomes-based program philosophy;
- Data analytics, risk assessment and patient stratification;
- Evidence-based interventions;
- Shared electronic health records; and
- Patient education and teaching self-management skills.
2.2. Specific and Broader Aims and Rationale of Study Design
2.3. Patient Characteristics
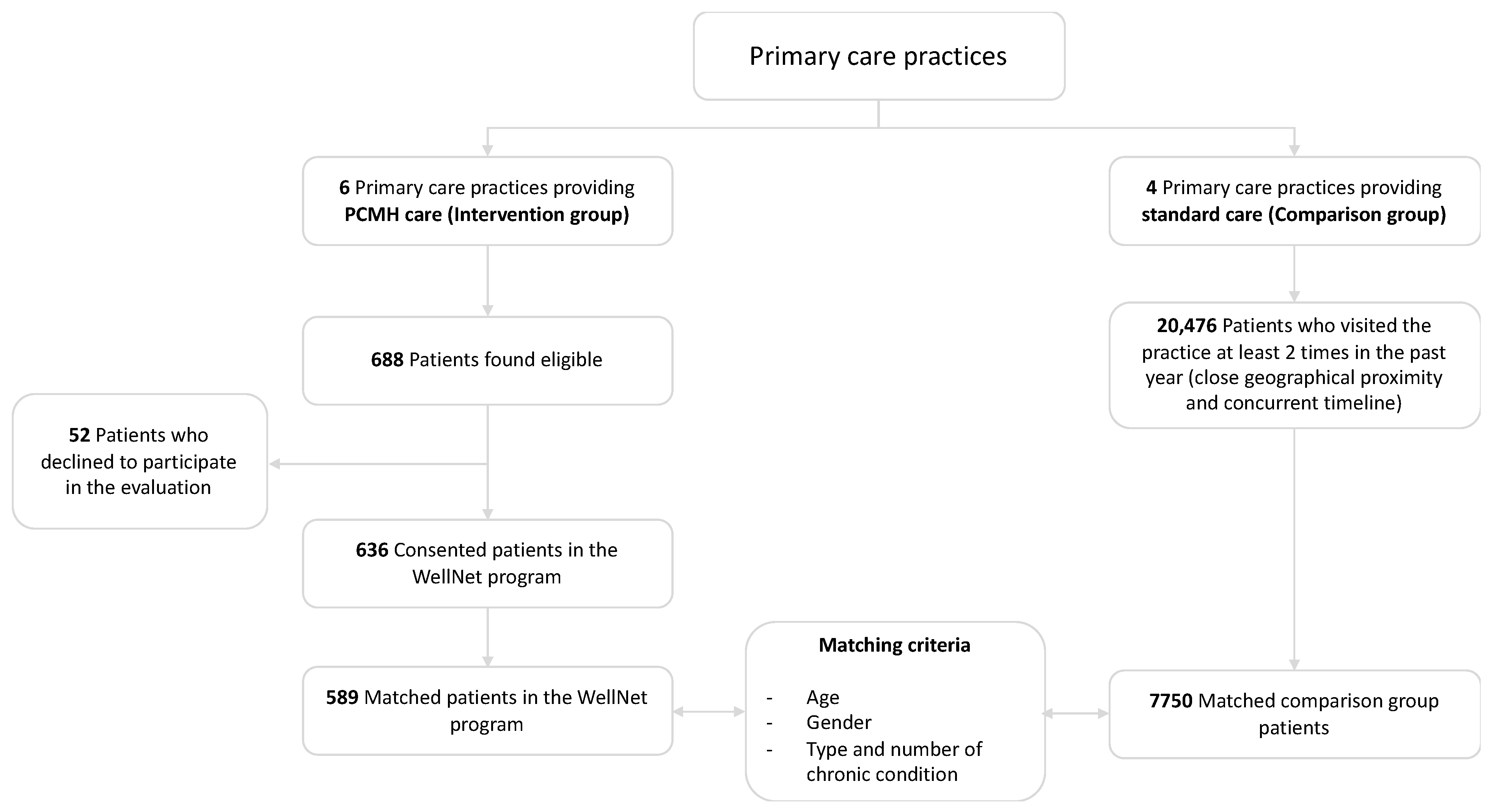
2.3.1. Treatment Group—Enrolment Methods and Outcome
2.3.2. Comparison Group—Matching Iterations and Outcomes
2.4. Provider Characteristics
2.5. Follow-Up
2.6. Data Collection
- (a)
- health-related quality of life,
- (b)
- level of health engagement and activation,
- (c)
- self-management of their health,
- (d)
- other disease-specific risk assessments.
2.7. Statistical Analyses
2.7.1. Analysis Conducted to Date
2.7.2. Ongoing Analysis
2.8. Ethical Considerations
3. Results and Discussion
3.1. Recruitment Outcomes
3.2. Sociodemographic Characteristics
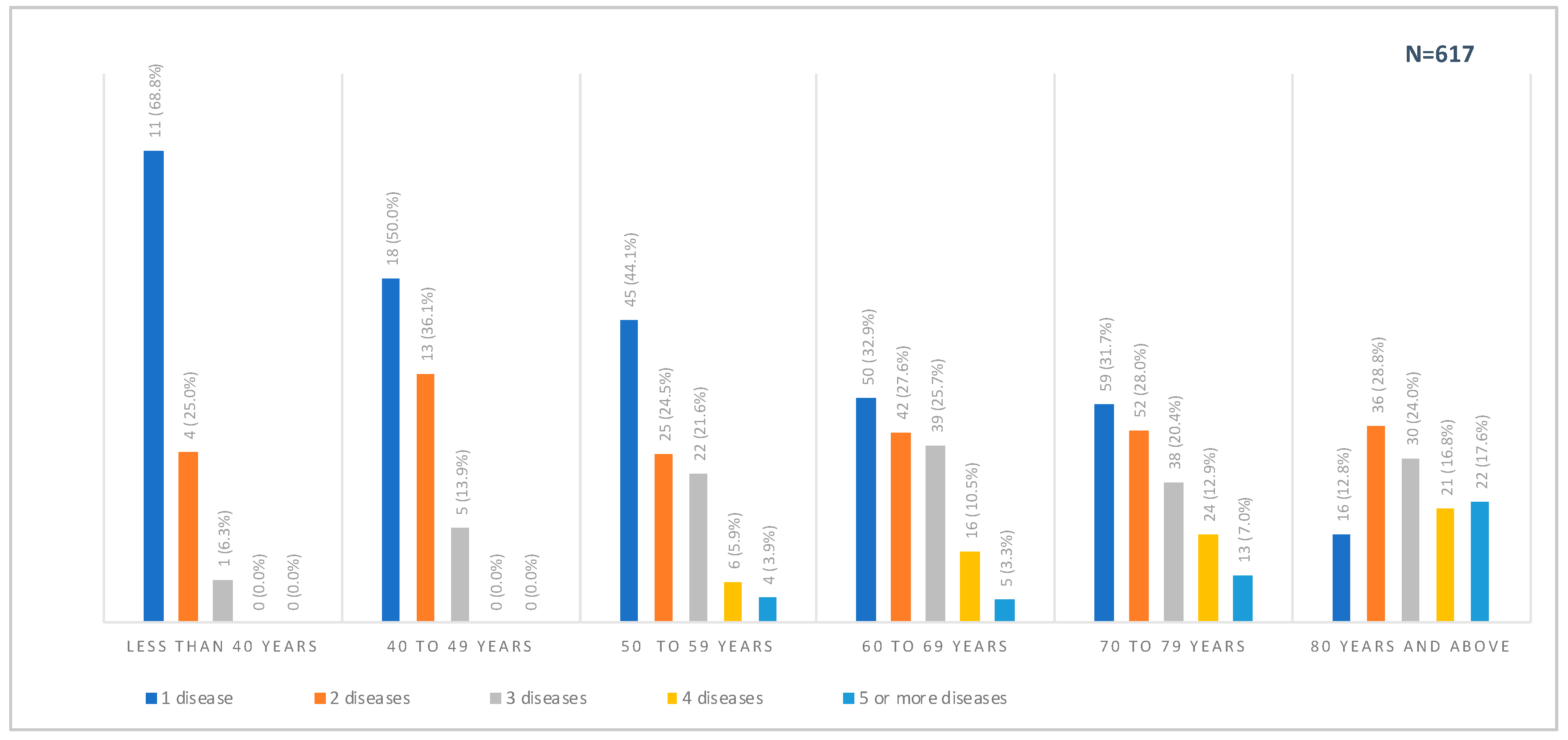
3.3. Chronic Disease Diagnosis and Clinical Indicators
3.4. Self-Reported Health Assessments
3.5. Provider-Level Findings
3.5.1. Provider-Level Baseline Characteristics
3.5.2. GPs Perspectives on Chronic Disease Management
3.5.3. GPs Perspectives on WellNet Study
3.5.4. GPs Perspectives on PCMH Model
3.6. Factors Affecting Reproducibility of Study Findings
3.7. Study Strengths
3.8. Study Limitations
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare: Australia’s health 2018. Available online: https://www.aihw.gov.au/getmedia/fe037cf1-0cd0-4663-a8c0-67cd09b1f30c/aihw-aus-222.pdf.aspx?inline=true (accessed on 10 June 2019).
- Australian Bureau of Statistics: Causes of Death, Australia 2017. Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/3303.0 (accessed on 22 June 2019).
- Australian Bureau of Statistics: National Health Survey: First results 2014–15 2015. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/CDA852A349B4CEE6CA257F150009FC53/$File/national%20health%20survey%20first%20results,%202014-15.pdf (accessed on 15 June 2019).
- Wang, L.; Palmer, A.J.; Cocker, F.; Sanderson, K. Multimorbidity and health-related quality of life (HRQoL) in a nationally representative population sample: Implications of count versus cluster method for defining multimorbidity on HRQoL. Health Qual. Life Outcomes 2017, 15, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atlantis, E.; Sullivan, T.; Sartorius, N.; Almeida, O.P. Changes in the prevalence of psychological distress and use of antidepressants or anti-anxiety medications associated with comorbid chronic diseases in the adult Australian population, 2001–2008. Aust. NZJ Psychiatry 2012, 46, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, K.I.; McQueenie, R.; Nicholl, B.; Jani, B.D.; Lee, D.; Mair, F.S. Risk factors and mortality associated with multimorbidity in people with stroke or transient ischaemic attack: A study of 8,751 UK Biobank participants. JOC 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Condelius, A.; Edberg, A.-K.; Jakobsson, U.; Hallberg, I.R. Hospital admissions among people 65+ related to multimorbidity, municipal and outpatient care. Arch. Gerontol. Geriat. 2008, 46, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Int. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef]
- Vyas, A.; Pan, X.; Sambamoorthi, U. Chronic condition clusters and polypharmacy among adults. Int. J. Famiy. Med. 2012, 193168, 1–8. [Google Scholar] [CrossRef]
- Atlantis, E.; Lange, K.; Wittert, G.A. Chronic disease trends due to excess body weight in Australia. Obes. Rev. 2009, 10, 543–553. [Google Scholar] [CrossRef]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; McGaughey, M.; Pletcher, M.A. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories using data from the Global Burden of Disease Study 2016. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Capewell, S. Proportion of the decline in cardiovascular mortality disease due to prevention versus treatment: Public health versus clinical care. Annu. Rev. Public Health 2011, 32, 5–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunenfeld, B.; Stratton, P. The clinical consequences of an ageing world and preventive strategies. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 643–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Camacho, E.M.; Davies, L.M.; Hann, M.; Small, N.; Bower, P.; Chew-Graham, C.; Baguely, C.; Gask, L.; Dickens, C.M.; Lovell, K. Long-term clinical and cost-effectiveness of collaborative care (versus usual care) for people with mental–physical multimorbidity: Cluster-randomised trial. Br. J. Psychiatry 2018, 213, 456–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coventry, P.; Lovell, K.; Dickens, C.; Bower, P.; Chew-Graham, C.; McElvenny, D.; Hann, M.; Cherrington, A.; Garrett, C.; Gibbons, C.J. Integrated primary care for patients with mental and physical multimorbidity: Cluster randomised controlled trial of collaborative care for patients with depression comorbid with diabetes or cardiovascular disease. BMJ 2015, 350, h638. [Google Scholar] [CrossRef] [Green Version]
- O’Loughlin, M.; Mills, J.; McDermott, R.; Harriss, L. Review of patient-reported experience within Patient-Centered Medical Homes: Insights for Australian Health Care Homes. Aust. J. Prim. Health 2017, 23, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Australian Nursing Federation. Primary health care in Australia: A nursing and midwifery consensus view 2009. Available online: https://anmf.org.au/documents/reports/PHC_Australia.pdf (accessed on 1 June 2019).
- Department of Health. National Primary Health Care Strategic Framework 2013. Available online: https://www.health.gov.au/internet/main/publishing.nsf/Content/6084A04118674329CA257BF0001A349E/$File/NPHCframe.pdf (accessed on 3 August 2019).
- Commonwealth of Australia: National primary health care strategic framework 2016. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/6084A04118674329CA257BF0001A349E/$File/NPHCframe.pdf (accessed on 11 August 2019).
- Department of Health: Australian Primary Care Collaboratives Programme 2014. Available online: https://www.health.gov.au/internet/main/publishing.nsf/Content/health-pcd-programs-apccp-index.htm (accessed on 10 August 2019).
- Canaway, R.; Boyle, D.I.; Manski-Nankervis, J.A.E.; Bell, J.; Hocking, J.S.; Clarke, K.; Clark, M.; Gunn, J.M.; Emery, J.D. Gathering data for decisions: Best practice use of primary care electronic records for research. Med. J. Aust. 2019, 210, S12–S16. [Google Scholar] [CrossRef] [Green Version]
- Winzenberg, T.M.; Gill, G.F. Prioritising general practice research. Med. J. Aust. 2016, 205, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Jackson, G.L.; Powers, B.J.; Chatterjee, R.; Bettger, J.P.; Kemper, A.R.; Hasselblad, V.; Dolor, R.J.; Irvine, R.J.; Heidenfelder, B.L.; Kendrick, A.S. The patient-centered medical Home: A Systematic review. Ann. Intern. Med. 2013, 158, 169–178. [Google Scholar] [CrossRef]
- Australian Medical Association. AMA Position Statement on the Medical Home 2015. Available online: https://ama.com.au/position-statement/ama-position-statement-medical-home (accessed on 13 June 2019).
- Bodenheimer, T.; Ghorob, A.; Willard-Grace, R.; Grumbach, K. The 10 building blocks of high-performing primary care. Ann. Fam. Med. 2014, 12, 166–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berk-Clark, C.; Doucette, E.; Rottnek, F.; Manard, W.; Prada, M.A.; Hughes, R.; Lawrence, T.; Schneider, F.D. Do Patient-Centered Medical Homes Improve Health Behaviors, Outcomes, and Experiences of Low-Income Patients? A Systematic Review and Meta-Analysis. Health Serv. Res. 2018, 53, 1777–1798. [Google Scholar] [CrossRef] [PubMed]
- Maeng, D.D.; Graf, T.R.; Davis, D.E.; Tomcavage, J.; Bloom Jr, F.J. Can a patient-centered medical home lead to better patient outcomes? The quality implications of Geisinger’s ProvenHealth Navigator. Am. J. Med. Qual. 2012, 27, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Bitton, A.; Martin, C.; Landon, B.E. A Nationwide Survey of Patient Centered Medical Home Demonstration Projects. J. Gen. Intern. Med. 2010, 25, 584–592. [Google Scholar] [CrossRef] [Green Version]
- DeVries, A.; Li, C.-H.W.; Sridhar, G.; Hummel, J.R.; Breidbart, S.; Barron, J.J. Impact of medical homes on quality, healthcare utilization, and costs. Am. J. Manag. Care 2012, 18, 534–544. [Google Scholar]
- Peikes, D.; Chen, A.; Schore, J.; Brown, R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among medicare beneficiaries: 15 randomized trials. JAMA 2009, 301, 603–618. [Google Scholar] [CrossRef]
- Reid, R.J.; Fishman, P.A.; Yu, O.; Ross, T.R.; Tufano, J.T.; Soman, M.P.; Larson, E.B. Patient-centered medical home demonstration: A prospective, quasi-experimental, before and after evaluation. Am. J. Manag. Care 2009, 15, e71–e87. [Google Scholar] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease: Global Strategy for Diagnosis, Management, and Prevention of COPD 2016. Available online: https://goldcopd.org/global-strategy-diagnosis-management-prevention-copd-2016/ (accessed on 10 May 2019).
- Lampe, L. Drug treatment for anxiety. Aust. Prescr. 2013, 36, 186–189. [Google Scholar] [CrossRef] [Green Version]
- National Heart Foundation of Australia: Guide to management of hypertension (2008 updated 2010) 2010. Available online: https://www.healthylivingnt.org.au/system/files/f/HypertensionGuidelines2008QRG2010Update.pdf (accessed on 1 May 2019).
- National Heart Foundation of Australia: Guideline for the diagnosis and management of hypertension in adults 2016. Available online: https://www.heartfoundation.org.au/images/uploads/publications/PRO-167_Hypertension-guideline-2016_WEB.pdf (accessed on 11 June 2019).
- National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Guidelines for the prevention, detection and management of chronic heart failure in Australia 2011. Available online: https://www.heartfoundation.org.au/images/uploads/publications/Chronic_Heart_Failure_Guidelines_2011.pdf (accessed on 11 June 2019).
- National Institute for Health and Care Excellence: Hypertension in adults: Diagnosis and management 2011. Available online: https://www.nice.org.uk/guidance/cg127 (accessed on 13 June 2019).
- National Institute for Health and Care Excellence: Type 1 diabetes in adults: Diagnosis and management 2015. Available online: https://www.nice.org.uk/guidance/ng17 (accessed on 12 June 2019).
- National Institute for Health and Care Excellence: Chronic heart failure in adults: Diagnosis and management 2018. Available online: https://www.nice.org.uk/guidance/ng106 (accessed on 11 June 2019).
- National Institute for Health and Care Excellence: Recognition, assessment and initial management of depression in adults 2018. Available online: http://pathways.nice.org.uk/pathways/depression (accessed on 10 June 2019).
- National Prescribing Service. Managing Blood Pressure based on Absolute Risk 2016. Available online: https://www.nps.org.au/medical-info/clinical-topics/blood-pressure (accessed on 16 June 2019).
- National Prescribing Service. Blood pressure treatment targets 2016. Available online: www.nps.org.au/conditions/heart-blood-and-blood-vessel-conditions/blood-pressure/for-health-professionals/managing-blood-pressure-based-on-absolute-risk/bp-treatment-targets (accessed on 14 June 2019).
- National Prescribing Service. Non-pharmacological management of depression 2016. Available online: https://www.nps.org.au/news/medicinewise-news-exploring-non-drug-options-in-depression (accessed on 11 June 2019).
- National Prescribing Service. Understanding high blood pressure 2017. Available online: www.nps.org.au/conditions/heart-blood-and-blood-vessel-conditions/blood-pressure/for-individuals/understanding-high-blood-pressure (accessed on 10 June 2019).
- National Vascular Disease Prevention Alliance: Guidelines for the management of absolute cardiovascular disease risk 2012. Available online: https://www.heartfoundation.org.au/images/uploads/publications/Absolute-CVD-Risk-Full-Guidelines.pdf (accessed on 18 June 2019).
- The Royal Australian College of General Practitioners: General practice management of type 2 diabetes: 2016–18. East Melbourne 2016. Available online: https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/5d3298b2-abf3-487e-9d5e-0558566fc242.pdf (accessed on 11 June 2019).
- Yang, I.; Brown, J.; George, J.; Jenkins, S.; McDonald, C.; McDonald, V.; Smith, B.; Zwar, N.; Dabscheck, E. The COPD-X Plan: Australian and New Zealand Guidelines for the management of Chronic Obstructive Pulmonary Disease. Med. J. Aust. 2018, 207, 436–442. [Google Scholar] [CrossRef] [Green Version]
- Department of Health: Evaluation Report of the Diabetes Care Project 2015. Available online: https://www.health.gov.au/internet/main/publishing.nsf/Content/302DF0372F537A43CA257E35000138E8/$File/DCP%20Evaluation%20Report.pdf (accessed on 17 June 2019).
- Primary Health Care Advisory Group: Better Outcomes for People with Chronic and Complex Health Conditions 2016. Available online: https://www.health.gov.au/internet/main/publishing.nsf/Content/76B2BDC12AE54540CA257F72001102B9/$File/Primary-Health-Care-Advisory-Group_Final-Report.pdf (accessed on 11 June 2019).
- Leelani, K. Impact on diabetes management of general practice management plans, team care arrangements and reviews. Med. J. Aust. 2013, 199, 261–265. [Google Scholar]
- Lacus, S.M.; King, G.; Porro, G. Causal inference without balance checking: Coarsened exact matching. Political. Anal. 2012, 20, 1–24. [Google Scholar]
- Andrews, G.; Slade, T. Interpreting scores on the Kessler psychological distress scale (K10). Aust. NZJ Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Magliano, D.J.; Balkau, B.; Colagiuri, S.; Zimmet, P.Z.; Tonkin, A.M.; Mitchell, P.; Phillips, P.J.; Shaw, J.E. AUSDRISK: An Australian Type 2 Diabetes Risk Assessment Tool based on demographic, lifestyle and simple anthropometric measures. Med. J. Aust. 2010, 192, 197. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Re.s 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.; Leidy, N.K. Development and first validation of the COPD Assessment Test. Eur. Resp. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Lyman, S.; Lee, Y.-Y.; Franklin, P.D.; Li, W.; Cross, M.B.; Padgett, D.E. Validation of the KOOS, JR: A short-form knee arthroplasty outcomes survey. Clin. Orthop. Relat. Res. 2016, 474, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Lyman, S.; Lee, Y.-Y.; Franklin, P.D.; Li, W.; Mayman, D.J.; Padgett, D.E. Validation of the HOOS, JR: A short-form hip replacement survey. Clin. Orthop. Relat. Res. 2016, 474, 1472–1482. [Google Scholar] [CrossRef] [Green Version]
- Sager, M.A.; Rudberg, M.A.; Jalaluddin, M.; Franke, T.; Inouye, S.K.; Landefeld, C.S.; Siebens, H.; Winograd, C.H. Hospital admission risk profile (HARP): Identifying older patients at risk for functional decline following acute medical illness and hospitalization. J. Am. Geriatr. Soc. 1996, 44, 251–257. [Google Scholar] [CrossRef]
- Stevens, R.J.; Kothari, V.; Adler, A.I.; Stratton, I.M.; Holman, R.R. The UKPDS risk engine: A model for the risk of coronary heart disease in Type II diabetes (UKPDS 56). Clin. Sci. 2001, 101, 671–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brett, T.; Arnold-Reed, D.E.; Popescu, A.; Soliman, B.; Bulsara, M.K.; Fine, H.; Bovell, G.; Moorhead, R.G. Multimorbidity in Patients Attending 2 Australian Primary Care Practices. Ann Fam Med 2013, 11, 535–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britt, H.C.; Harrison, C.M.; Miller, G.C.; Knox, S.A. Prevalence and patterns of multimorbidity in Australia. Med. J. Aust. 2008, 189, 72–77. [Google Scholar] [CrossRef]
- Heyworth, I.T.; Hazell, M.L.; Linehan, M.F.; Frank, T.L. How do common chronic conditions affect health-related quality of life? Br. J. Gen. Pract. 2009, 59, e353–e358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Z.; Liang, Y.; Liu, S.; Cao, W.; Tu, H.; Guo, L.; Xu, Y. Health-related quality of life as measured with EQ-5D among populations with and without specific chronic conditions: A population-based survey in Shaanxi Province, China. PLoS One 2013, 8, e65958. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Matching Iteration Number | Matching Variables | Treatment (Overall n = 636) | Comparison (overall n = 20478) | N (Matched Treatment: Comparison) | N (Unmatched Treatment: Comparison) |
|---|---|---|---|---|---|
| 1 | Age (continuous), gender, type of chronic disease (cardiovascular disease, respiratory disease, diabetes, musculoskeletal disease, mental illness, and cancer) and number of chronic diseases. | 617 * | 20478 * | 589:7750 | 28:12728 |
| 2 | Age (continuous), gender, type of chronic disease (cardiovascular disease, respiratory disease, diabetes, musculoskeletal disease, mental illness, and cancer), systolic, and total cholesterol: HDL-C ratio. | 447 ** | 3899 ** | 228:604 | 219:3205 |
| 3 | Age categories (breaks = 10 years), gender, (cardiovascular disease, respiratory disease, diabetes, musculoskeletal disease, mental illness, and cancer), systolic, and total cholesterol: HDL-C ratio. | 447 ** | 3899 ** | 260:749 | 260:749 |
| 4 | Age (continuous), gender, type of chronic disease (cardiovascular disease, respiratory disease, diabetes, musculoskeletal disease, mental illness, and cancer), systolic (breaks = 2 mmHg), and total cholesterol: HDL-C ratio. | 447 ** | 3899 ** | 202:517 | 245:3292 |
| 5 | Age categories (breaks = 10 years), gender, (cardiovascular disease, respiratory disease, diabetes, musculoskeletal disease, mental illness, and cancer), systolic (breaks = 2 mmHg), and total cholesterol: HDL-C ratio. | 447 ** | 3899 ** | 242:735 | 205:3074 |
| Type of Data | Time of Data Collection | Variables Measured |
|---|---|---|
| Socio-demographic data | Baseline | Age and gender |
| Private health insurance membership | Baseline | Private insurance status and name of the insurance provider |
| Diagnosis of chronic condition | Baseline | Diagnosis of arthritis, asthma, back pain, cancer, cardiovascular diseases (CVD), chronic obstructive pulmonary disease (COPD), diabetes, mental illness and kidney diseases. |
| Clinical assessments | Baseline 6-month 12-month | Height, weight, waist circumference, Body Mass Index (BMI), blood pressure (BP), blood sample - cholesterol [serum total cholesterol, high density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C)], triglycerides, glycated haemoglobin (HbA1c), estimated glomerular filtration rate (eGFR), and urine albumin-creatinine ratio (UACR). |
| Risk of hospital admission | Baseline 12-month | Hospital Admission Risk Profile (HARP) score to estimate the risk of hospitalisation in the next 12 months |
| Health utility data | Baseline 12-month | Medication–drug name, dosage and frequency of use and number of prescriptions. |
| Patient activation, engagement and readiness to change | Baseline 12-month | Patient Activation Measure (PAM) scores to evaluate patient self-efficacy and self-management behaviours |
| Patient self-reported health-related quality of life | Baseline 12-month | EuroQol 5 Dimensions 5 Levels (EQ-5D-5L) to assess patient’s heath related quality of life |
| Disease-specific risk assessments | Baseline 12-month | Absolute Cardiovascular Disease Risk (CVDR), Australian Type 2 Diabetes Risk Tool (AusDrisk) scores, UK Prospective Diabetes Risk Engine (UKPDS), Chronic Obstructive Pulmonary Disease Assessment Test (CAT) scores, Kessler Psychological Distress scale (K10) scale, Depression Anxiety Stress Scale (DASS21), short versions of Knee Injury and Osteoarthritis Outcome Score (KOOS), Hip Disability and Osteoarthritis Outcome Score (HOOS). |
| Patient experience survey | 12-month | Patient satisfaction survey on quality of care outcomes; patient-provider relationship, communication, and empowerment outcomes; and access to information technology outcomes. |
| Feasibility outcomes | 12-month |
Recruitment: number of patients’ who potentially met the program’s inclusion criteria;
Retention rates: number of completed and dropouts; Treatment compliance: rates of adherence to overall protocol. |
| Criteria | Success Rate |
|---|---|
| Age | |
| 40 years and above | 97.5% |
| Number of chronic diseases | |
| Number of patients with 1 to 3 chronic diseases | 93.4% |
| Number of patients with 4 or more chronic diseases | 6.6% |
| Risk factors | |
| Patients with 1 chronic disease (n = 227) | |
| 1 risk factor | 47.6% |
| >1 risk factor | 31.7% |
| Patients with 2 chronic diseases (n = 237) | |
| 1 risk factor | 42.6% |
| >1 risk factor | 27.4% |
| Patients with 3 chronic diseases (n = 115) | |
| 1 risk factor | 40% |
| >1 risk factor | 35.7% |
| Patients with 4 or more chronic diseases (n = 38) | |
| 1 risk factor | 44.7% |
| >1 risk factor | 26.3% |
| HARP score >10 | 97.7% |
| Determinants | WellNet Treatment Group (N = 589) | WellNet Comparison Group (N = 7750) | p-Value |
|---|---|---|---|
| N (%) | N (%) | ||
| Age groups | 0.798 | ||
| 40–44 years | 7 (1.2) | 141 (1.8) | |
| 45–54 years | 57 (9.7) | 722 (9.3) | |
| 55–64 years | 118 (20.0) | 1580 (20.4) | |
| 65–74 years | 188 (31.9) | 2360 (30.4) | |
| 75–84 years | 156 (26.5) | 2029 (26.2) | |
| ≥85 years | 63 (10.7) | 918 (11.8) | |
| Mean (SD) | 70.05 (11.59) | 69.95 (11.86) | |
| Sex | 0.936 | ||
| Male | 293 (49.7) | 3842 (49.6) | |
| Female | 296 (50.3) | 3908 (50.4) | |
| Smoking status | |||
| Ex–smoker | 237 (42.1) | 2274 (36.4) | <0.001 |
| Non–smoker | 280 (49.7) | 3655 (58.6) | |
| Smoker | 46 (8.2) | 309 (5.0) | |
| Unknown | 26 (4.4) | 1512 (19.5) | |
| Drinking status | |||
| Drinker | 256 (43.5) | 1465 (18.9) | <0.001 |
| Non–drinker | 176 (29.9) | 147 (1.9) | |
| Unknown | 156 (26.5) | 6138 (79.2) | |
| Private insurance status | |||
| Yes | 404 (68.7) | NA | – |
| No | 184 (31.3) | ||
| Missing | 1 (0.2) | ||
| Prevalence of chronic conditions | 1.000 | ||
| Diseases of the circulatory system | 411 (69.8) | 5408 (69.8) | |
| Respiratory diseases | 169 (28.7) | 2224 (28.7) | |
| Musculoskeletal disorders | 256 (43.5) | 3368 (43.5) | |
| Diabetes | 279 (47.4) | 3671 (47.4) | |
| Mental illness | 111 (18.8) | 1461 (18.8) | |
| Cancer | 80 (13.6) | 1053 (13.6) | |
| Number of chronic conditions | 1.000 | ||
| 1 disease | 133 (22.6) | 1750 (22.6) | |
| 2 diseases | 249 (42.3) | 3276 (42.3) | |
| 3 diseases | 159 (27.0) | 2092 (27.0) | |
| 4 diseases | 42 (7.1) | 553 (7.1) | |
| ≥5 diseases | 6 (1.0) | 79 (1.0) |
| Clinical Measures | WellNet Treatment Group (N = 589) | WellNet Comparison Group (N = 7750) | p-Value |
|---|---|---|---|
| N (%) | N (%) | ||
| Systolic blood pressure (mmHg), Mean (SD) | 139.37 (19.30) | 135.96 (16.51) | <0.001 |
| Diastolic blood pressure (mmHg), Mean (SD) | 79.27 (10.32) | 76.02 (11.31) | <0.001 |
| Body Mass Index, Mean (SD) | 29.54 (6.36) | 29.12 (5.63) | 0.151 |
| Weight (kg)–Mean (SD) | 81.81 (20.72) | 81.73 (19.70) | 0.930 |
| Waist Circumference* (Males) (cm), Mean (SD) | 106.09 (15.63) | 104.30 (14.30) | 0.120 |
| Waist Circumference* (Females) (cm), Mean (SD) | 98.82 (14.62) | 93.15 (12.47) | <0.001 |
| HbA1c (%), Mean (SD) | 7.16 (1.41) | 6.71 (1.24) | <0.001 |
| HDL-C (mmol/L), Mean (SD) | 1.37 (0.40) | 1.40 (0.42) | 0.147 |
| LDL-C (mmol/L), Mean (SD) | 2.71 (1.08) | 2.52 (0.98) | <0.001 |
| Serum total cholesterol (mmol/L), Mean (SD) | 4.81 (1.38) | 4.60 (1.13) | <0.001 |
| Estimated Glomerular Filtration Rate (mL/min/1.73m2) | |||
| >90 mL/min/1.73 m2 | 109 (24.9) | 1467 (24.8) | 0.868 |
| 60–89 mL/min/1.73 m2 | 247 (56.5) | 3436 (58.2) | |
| 45–59 mL/min/1.73 m2 | 46 (10.5) | 622 (10.5) | |
| 30–44 mL/min/1.73 m2 | 26 (5.9) | 274 (4.6) | |
| <30 mL/min/1.73 m2 | 9 (2.0) | 106 (1.8) | |
| Missing | 152 (25.8) | 1845 (23.8) | |
| Albumin-Creatinine Ratio* (mg/mmol) (Males), Mean (SD) | 15.52 (67.54) | 13.08 (53.18) | 0.653 |
| Albumin-Creatinine Ratio* (mg/mmol) (Females), Mean (SD) | 7.53 (22.31) | 8.07 (32.12) | 0.878 |
| Patient Survey Questionnaires | WellNet Treatment Group (N = 635) |
|---|---|
| n (%) | |
| Hospital Admission risk profile (N = 628) | |
| Low risk (1–10) | 14 (2.2) |
| Medium risk (11–23) | 581 (92.5) |
| High risk (24–38) | 33 (5.3) |
| Missing | 7 (1.1) |
| Patient Activation Measure scores (N = 626) | |
| Not believing that activation is important (<47) | 121 (19.3) |
| A lack of knowledge and confidence to take action (47.1–55.1) | 236 (37.7) |
| Beginning to take action (55.2–67) | 138 (22.0) |
| Taking action (>67.1) | 131 (20.9) |
| Missing | 9 (1.4) |
| Mean EQ-5D-5L score (overall)–Mean (SD) | 0.79 (0.19) |
| EQ-5D-5L score percentage | |
| EQ-5D-5L mobility (N = 626) | |
| No problem | 298 (47.6) |
| Slight problem | 171 (27.3) |
| Moderate problem | 108 (17.3) |
| Severe problem | 47 (7.5) |
| Unable to walk | 2 (0.3) |
| Missing | 9 (1.4) |
| EQ-5D-5L self-care (N = 623) | |
| No problem | 521 (83.6) |
| Slight problem | 79 (12.7) |
| Moderate problem | 19 (3.0) |
| Severe problem | 4 (0.6) |
| Unable | 0 (0.0) |
| Missing | 12 (1.9) |
| EQ-5D-5L usual activities (N = 626) | |
| No problem | 312 (49.8) |
| Slight problem | 187 (29.9) |
| Moderate problem | 98 (15.7) |
| Severe problem | 26 (4.2) |
| Unable | 3 (0.5) |
| Missing | 9 (1.4) |
| EQ-5D-5L pain/discomfort (N = 627) | |
| No problem | 156 (24.9) |
| Slight problem | 246 (39.2) |
| Moderate problem | 165 (26.3) |
| Severe problem | 55 (8.8) |
| Extreme | 5 (0.8) |
| Missing | 8 (1.3) |
| EQ-5D-5L anxiety/depression (N = 629) | |
| No problem | 321 (51.0) |
| Slight problem | 190 (30.2) |
| Moderate problem | 94 (14.9) |
| Severe problem | 16 (2.5) |
| Extreme | 8 (1.3) |
| Missing | 6 (0.9) |
| DASS21 Scores (N = 331) | |
| DASS21–Depression scale | |
| Normal | 230 (69.5) |
| Mild | 26 (7.9) |
| Moderate | 40 (12.1) |
| Severe | 12 (3.6) |
| Extremely severe | 23 (6.9) |
| DASS21–Anxiety scale | |
| Normal | 211 (63.7) |
| Mild | 32 (9.7) |
| Moderate | 53 (16.0) |
| Severe | 14 (4.2) |
| Extremely severe | 21 (6.3) |
| DASS21–Stress scale | |
| Normal | 260 (78.5) |
| Mild | 29 (8.8) |
| Moderate | 20 (6.0) |
| Severe | 15 (4.5) |
| Extremely severe | 7 (2.1) |
| K10 scores (N = 302) | |
| Low level of psychological distress | 137 (45.4) |
| Moderate level of psychological distress | 88 (29.1) |
| High level of psychological distress | 49 (16.2) |
| Very high level of psychological distress | 28 (9.3) |
| UKPDS risk profile (N = 140) | |
| Coronary Heart Disease risk - mean percentage (SD) | 18.98 (14.11) |
| Fatal Coronary Heart Disease risk - mean percentage (SD) | 14.94 (16.14) |
| Stroke risk - mean percentage (SD) | 14.37 (15.10) |
| Fatal stroke risk - mean percentage (SD) | 2.33 (2.60) |
| Missing | 53 (27.5) |
| AusDRisk scores (N = 220) | |
| Low risk | 5 (2.3) |
| Intermediate risk | 34 (15.5) |
| High risk | 181 (82.3) |
| Missing | 137 (38.4) |
| Absolute cardiovascular risk (N = 370) | |
| Low risk | 167 (45.1) |
| Moderate risk | 84 (22.7) |
| High risk | 119 (32.2) |
| Missing | 48 (11.5) |
| COPD impact scores (N = 26) | |
| Normal | 2 (7.7) |
| Low | 4 (15.4) |
| Medium | 12 (46.2) |
| High | 3 (11.5) |
| Very high | 5 (19.2) |
| Missing | 38 (59.4) |
| HOOS score (N = 31) | |
| HOOS pain score - Mean (SD) | 64.92 (23.37) |
| HOOS function score - Mean (SD) | 68.95 (19.80) |
| HOOS symptoms score - Mean (SD) | 66.15 (17.23) |
| Missing | 168 (84.4) |
| KOOS score (N = 59) | |
| KOOS stiffness score - Mean (SD) | 61.86 (28.37) |
| KOOS pain score - Mean (SD) | 64.72 (22.01) |
| KOOS function score - Mean (SD) | 63.13 (25.58) |
| KOOS symptoms score - Mean (SD) | 63.09 (18.14) |
| Missing | 140 (70.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
John, J.R.; Jones, A.; Neville, A.M.; Ghassempour, S.; Girosi, F.; Tannous, W.K. Cohort Profile: Effectiveness of a 12-Month Patient-Centred Medical Home Model Versus Standard Care for Chronic Disease Management among Primary Care Patients in Sydney, Australia. Int. J. Environ. Res. Public Health 2020, 17, 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062164
John JR, Jones A, Neville AM, Ghassempour S, Girosi F, Tannous WK. Cohort Profile: Effectiveness of a 12-Month Patient-Centred Medical Home Model Versus Standard Care for Chronic Disease Management among Primary Care Patients in Sydney, Australia. International Journal of Environmental Research and Public Health. 2020; 17(6):2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062164
Chicago/Turabian StyleJohn, James Rufus, Amanda Jones, A. Munro Neville, Shima Ghassempour, Federico Girosi, and W. Kathy Tannous. 2020. "Cohort Profile: Effectiveness of a 12-Month Patient-Centred Medical Home Model Versus Standard Care for Chronic Disease Management among Primary Care Patients in Sydney, Australia" International Journal of Environmental Research and Public Health 17, no. 6: 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062164