What is the Co-Creation of New Knowledge? A Content Analysis and Proposed Definition for Health Interventions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation Phase
2.1.1. Unit of Analysis and Data Collection Method
2.1.2. Sampling Strategy
2.1.3. Constructing a Controlled List of Search Terms
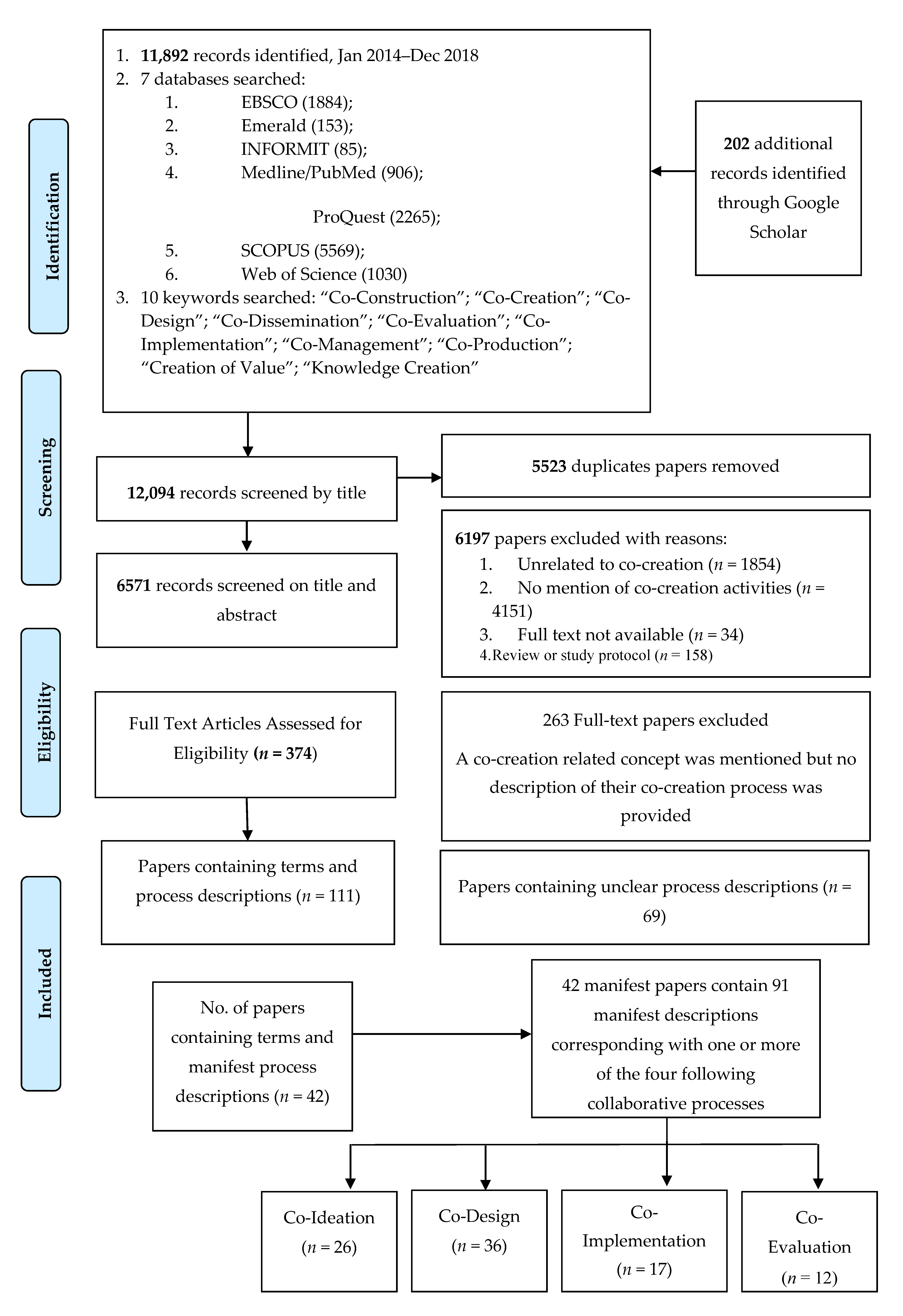
2.1.4. Search Protocol and Screening of Records
2.2. Organization Phase
3. Reporting and Results Phase
3.1. Variability of Terms and Description of Co-Creation Activities
3.2. Trustworthiness
3.3. Results
4. Discussion
4.1. Implications for Service Delivery and Policy Implementation
4.2. Implications for Future Research
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Milat, A.; Li, B. Narrative review of frameworks for translating research evidence into policy and practice. Public Health Res. Pract. 2017, 27, e2711704. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, D.H.; Ridenour, T.A.; Stahl, M.; Sussman, S. The full translational spectrum of prevention science: Facilitating the transfer of knowledge to practices and policies that prevent behavioral health problems. Translat. Behavior. Med. 2016, 6, 516. [Google Scholar] [CrossRef] [Green Version]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implem. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castleden, H.; Morgan, V.S.; Lamb, C. “I spent the first year drinking tea”: Exploring canadian university researchers’ perspectives on community-based participatory research involving indigenous peoples. Can. Geogr. /Le Géographe Can. 2012, 56, 160–179. [Google Scholar] [CrossRef]
- Cox, A.; Dudgeon, P.; Holland, C.; Kelly, K.; Scrine, C.; Walker, R. Using participatory action research to prevent suicide in aboriginal and torres strait islander communities. Aust. J. Prim. Health 2014, 20, 345–349. [Google Scholar] [CrossRef]
- Spears, J.C.; Kraemer, D.A.; Arcury, T. Participation levels in 25 Community-based participatory research projects. Health Educ. Res. 2016, 31, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Glasziou, P.; Altman, D.G.; Bossuyt, P.; Boutron, I.; Clarke, M.; Julious, S.; Michie, S.; Moher, D.; Wager, E. Reducing waste from incomplete or unusable reports of biomedical research. Lancet 2014, 383, 267–276. [Google Scholar]
- Knight, A.; Shakeshaft, A.; Havard, A.; Maple, M.; Foley, C.; Shakeshaft, B. The quality and effectiveness of interventions that target multiple risk factors among young people: A systematic review. Aust. N. Z. J. Public Health 2017, 41, 54–60. [Google Scholar] [CrossRef]
- Calabria, B.; Shakeshaft, A.P.; Havard, A. A systematic and methodological review of interventions for young people experiencing alcohol-related harm. Addiction 2011, 106, 1406–1418. [Google Scholar] [CrossRef]
- Clifford, A.C.; Doran, C.M.; Tsey, K. A systematic review of suicide prevention interventions targeting indigenous peoples in Australia, United States, Canada and New Zealand. BMC Public Health 2013, 13, 463. [Google Scholar] [CrossRef] [Green Version]
- Calabria, B.; Clifford, A.; Shakeshaft, A.P.; Doran, C.M. A systematic review of family-based interventions targeting alcohol misuse and their potential to reduce alcohol-related harm in indigenous communities. J. Stud. Alcoh. Drug. 2012, 73, 477–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanson-Fisher, R.W.; Campbell, E.M.; Htun, A.T.; Bailey, L.J.; Millar, C.J. We are what we do: Research outputs of public health. Am. J. Prevent. Med. 2008, 35, 380–385. [Google Scholar] [CrossRef] [PubMed]
- McCalman, J.; Tsey, K.; Clifford, A.; Earles, W.; Shakeshaft, A.; Bainbridge, R. Applying what works: A systematic search of the transfer and implementation of promising Indigenous Australian health services and programs. BMC Public Health 2012, 12, 600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanson-Fisher, R.W.; Bonevski, B.; Green, L.W.; D’Este, C. Limitations of the randomized controlled trial in evaluating population-based health interventions. Am. J. Prevent. Med. 2007, 33, 155–161. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. How to make more published research true. PLoS Med. 2014, 11, e1001747. [Google Scholar] [CrossRef] [Green Version]
- McCormack, L.; Sheridan, S.; Lewis, M.; Boudewyns, V.; Melvin, C.L.; Kistler, C.; Cullen, K.; Lohr, K. Communication and dissemination strategies to facilitate the use of health-related evidence. Evid. Rep. Technol. Assess. 2013, 213, 1–520. [Google Scholar]
- Guttmacher, S.; Kelly, P.J.; Ruiz-Janecko, Y. Community-Based Health Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Sabater-Hernández, D.; Tudball, J.; Ferguson, C.; Franco-Trigo, L.; Hossain, L.N.; Benrimoj, S.I. A stakeholder co-design approach for developing a community pharmacy service to enhance screening and management of atrial fibrillation. BMC Health Ser. Res. 2018, 18, 145. [Google Scholar] [CrossRef]
- Brosens, D.; De Donder, L.; Dury, S.; Verte, D. Building a research partnership in a prison context: From collaboration to co-construction. Sociolog. Res. Online 2015, 20, 79–93. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving research impact through co-creation in community-based health services: Literature review and case study. Milbank Quarter. 2016, 94, 392–429. [Google Scholar] [CrossRef] [Green Version]
- Jull, J.; Giles, A.; Graham, I.D. Community-based participatory research and integrated knowledge translation: Advancing the co-creation of knowledge. Implement. Sci. 2017, 12, 150. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Foster, M.; Freeman, C.; Scott, I.A. A multifaceted intervention to reduce inappropriate polypharmacy in primary care: Research co-creation opportunities in a pilot study. Medical J. Australia 2016, 204, S41–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donetto, S.; Pierri, P.; Tsianakas, V.; Robert, G. Experience-based co-design and healthcare improvement: Realizing participatory design in the public sector. Design J. 2015, 18, 227–248. [Google Scholar] [CrossRef] [Green Version]
- Hafford-Letchfield, T.; Formosa, M. Mind the gap! An exploration of the role of lifelong learning in promoting co-production and citizenship within social care for older people. European J. Res. Educ. Learn. Adult. 2016, 7, 237–252. [Google Scholar] [CrossRef] [Green Version]
- Voorberg, W.H.; Bekkers, V.J.J.M.; Tummers, L.G. A systematic review of co-creation and co-production: Embarking on the social innovation journey. Public Manag. Rev. 2015, 17, 1333–1357. [Google Scholar] [CrossRef] [Green Version]
- Brandsen, T.; Honingh, M. Distinguishing different types of coproduction: A conceptual analysis based on the classical definitions. Public Adm. Rev. 2016, 76, 427–435. [Google Scholar] [CrossRef]
- McGeechan, G.; Woodall, D.; Anderson, L.; Wilson, L.; O’Neill, G.; Newbury-Birch, D. A coproduction community based approach to reducing smoking prevalence in a local community setting. J. Environ. Public Health 2016, 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Mehrpouya, H.; Maxwell, D.; Zamora, D. Reflections on co-creation: An open source approach to co-creation. Participations 2013, 10, 172–182. [Google Scholar]
- Morse, J.M.; Hupcey, J.E.; Cerdas, M. Criteria for concept evaluation. J. Adv. Nurs. 1996, 24, 385–390. [Google Scholar] [CrossRef]
- Jo, S.; Nabatchi, T. Getting back to basics: Advancing the study and practice of coproduction. Int. J. Public Adm. 2016, 39, 1101–1108. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Manimozhi, G.; Srinivasan, P. A meta synthesis of content analysis approaches. Am. J. Educ. Res. 2018, 6, 632–637. [Google Scholar]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurs. Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Sánchez de la Guía, L.; Puyuelo, C.M.; de-Miguel-Molina, B. Terms and meanings of “participation” in product design: From “user involvement” to “co-design”. Design J. 2017, 20, S4539–S4551. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Hackett, C.L.; Mulvale, G.; Miatello, A. Co-designing for quality: Creating a user-driven tool to improve quality in youth mental health services. Health Expect. 2018, 21, 1013–1023. [Google Scholar] [CrossRef]
- Knowles, S.; Hays, R.; Senra, H.; Bower, P.; Locock, L.; Protheroe, J.; Sanders, C.; Daker-White, G. Empowering people to help speak up about safety in primary care: Using codesign to involve patients and professionals in developing new interventions for patients with multimorbidity. Health Expect. 2018, 21, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, Y.S.; Guba, E.G. Establishing trustworthiness. Natural. Inqu. 1985, 289, 289–327. [Google Scholar]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. 2016, 6, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, A.K.; Rahman, Z. Roles and resource contributions of customers in value co-creation. Int. Strat. Manag. Rev. 2015, 3, 144–160. [Google Scholar] [CrossRef] [Green Version]
- Podgórniak-Krzykacz, A. Co-production for local public services—A case study of the cooperative Hallenbad Nörten-Hardenberg eG. Zarz. Publiczne. 2015, 30, 167–178. [Google Scholar]
- Wang, W.; Bryan-Kinns, N.; Ji, T. Using community engagement to drive co-creation in rural China. Int. J. Design. 2016, 10, 37–52. [Google Scholar]
- Bryan-Kinns, N.; Wang, W.; Ji, T. Exploring interactivity and co-creation in rural China. Int. Comput. 2018, 30, 273–292. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Zhao, X.; Voss, C.; Zhu, G. Innovating through services, co-creation and supplier integration cases from China. Int. J. Product. Econ. 2016, 171, 289–300. [Google Scholar] [CrossRef]
- Lapolla, K.; Sanders, E.B.N. Using cocreation to engage everyday creativity in reusing and repairing apparel. Cloth.Text. Res. J. 2015, 33, 183–198. [Google Scholar] [CrossRef]
- Jamin, G.; Luyten, T.; Delsing, R.; Braun, S. The process of co-creating the interface for VENSTER, an interactive artwork for nursing home residents with dementia. Disab. Rehabilit. Assist. Tech. 2018, 13, 809–818. [Google Scholar] [CrossRef]
- Broadley, C.; Smith, P. Co-design at a distance: Context, participation, and ownership in geographically distributed design processes. Design J. 2018, 21, 395–415. [Google Scholar] [CrossRef]
- Hjelmfors, L.; Stromberg, A.; Friedrichsen, M.; Sandgren, A.; Martensson, J.; Jaarsma, T. Using co-design to develop an intervention to improve communication about the heart failure trajectory and end-of-life care. BMC Palliat. Care 2018, 17, 85. [Google Scholar] [CrossRef] [Green Version]
- Westhorp, G.; Stevens, K.; Rogers, P.J. Using realist action research for service redesign. Evaluation 2016, 22, 361–379. [Google Scholar] [CrossRef]
- Kwon, S.M.; Wardrip, P.S.; Gomez, L.M. Co-design of interdisciplinary projects as a mechanism for school capacity growth. Improv. School. 2014, 17, 54–71. [Google Scholar] [CrossRef]
- Taffe, S. The hybrid designer/end-user: Revealing paradoxes in co-design. Design Stud. 2015, 40, 39–59. [Google Scholar] [CrossRef]
- Durl, J.; Trischler, J.; Dietrich, T. Co-designing with young consumers—reflections, challenges and benefits. Young Consum. 2017, 18, 439–455. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.E.; De Brun, A.; Beirne, D.; Conway, C.; Cunningham, U.; English, A.; Fitzsimmons, J.; Furlong, E.; Kane, Y.; Kelly, A.; et al. Using co-design to develop a collective leadership intervention for healthcare teams to improve safety culture. Int. J. Environ. Res. Public Health 2018, 15, 1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, B.; Dearden, A. Enhancing service development and service delivery through co-design. Volunt. Sector Rev. 2015, 6, 61–80. [Google Scholar] [CrossRef] [Green Version]
- De Jans, S.; Van Geit, K.; Cauberghe, V.; Hudders, L.; De Veirman, M. Using games to raise awareness: How to co-design serious mini-games? Comput. Educ. 2017, 110, 77–87. [Google Scholar] [CrossRef]
- Candi, M.; van den Ende, J.; Gemser, G. Benefits of customer codevelopment of new products: The moderating effects of utilitarian and hedonic radicalness. J. Produ. Innovat. Manag. 2016, 33, 418–434. [Google Scholar] [CrossRef]
- Sharma, S.; Conduit, J. Cocreation culture in health care organizations. J. Serv. Res. 2016, 19, 438–457. [Google Scholar] [CrossRef]
- Barbera, C.; Sicilia, M.; Steccolini, I. What Mr. Rossi Wants in Participatory Budgeting: Two R’s (Responsiveness and Representation) and Two I’s (Inclusiveness and Interaction). Int. J. Public Adm. 2016, 39, 1088–1100. [Google Scholar]
- Sicilia, M.; Guarini, E.; Sancino, A.; Andreani, M.; Ruffini, R. Public services management and co-production in multi-level governance settings. Int. Rev. Adm. Sci. 2016, 82, 8–27. [Google Scholar] [CrossRef]
- Strokosch, K.; Osborne, S.P. Asylum seekers and the co-production of public services: Understanding the implications for social inclusion and citizenship. J. Soc. Poli. 2016, 45, 673–690. [Google Scholar] [CrossRef] [Green Version]
- Dunn, V. Young people, mental health practitioners and researchers co-produce a Transition Preparation Programme to improve outcomes and experience for young people leaving Child and Adolescent Mental Health Services (CAMHS). BMC Health Ser. Res. 2017, 17, 293. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Madden, K.; Fletcher, A.; Midgley, L.; Grant, A.; Cox, G.; Moore, L.; Campbell, R.; Murphy, S.; Bonnell, G.; et al. Development of a framework for the co-production and prototyping of public health interventions. BMC Public Health 2017, 17, 689. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, J.; Caluwaerts, D.; Brans, M. Coproduction in health planning: Challenging the need for “open” policy-making processes. Int. J. Public Adm. 2016, 39, 1056–1066. [Google Scholar]
- Thijssen, P.; Van Dooren, W. Who you are/where you live: Do neighbourhood characteristics explain co-production? Int. Rev. Adm. Sci. 2016, 82, 88–109. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, R.B. Value co-creation in industrial cities: A strategic source of competitive advantages. J. Strat. Market. 2016, 24, 144–167. [Google Scholar] [CrossRef]
- Teichmann, K.; Scholl-Grissemann, U.; Stokburger-Sauer, N.E. The power of codesign to bond customers to products and companies: The role of toolkit support and creativity. J. Inter. Market. 2016, 36, 15–30. [Google Scholar] [CrossRef]
- Hetrick, S.E.; Robinson, J.; Burge, E.; Blandon, R.; Mobilio, B.; Rice, S.M.; Simmons, M.; Alvarez-Jimenez, M.; Goodrich, S.; Davey, C. Youth codesign of a mobile phone app to facilitate self-monitoring and management of mood symptoms in young people with major depression, suicidal ideation, and self-harm. JMIR Mental Health 2018, 5, e9. [Google Scholar] [CrossRef]
- Bessant, J.; Farthing, R.; Watts, R. Co-designing a civics curriculum: Young people, democratic deficit and political renewal in the EU. J. Curricu. Stud. 2016, 48, 271–289. [Google Scholar] [CrossRef]
- Merickova, B.M.; Nemec, J.; Svidronova, M. Co-creation in local public services delivery innovation: Slovak experience. Lex Localis-J. Local Self-Governm. 2015, 13, 521–535. [Google Scholar] [CrossRef]
- Hahn-Goldberg, S.; Damba, C.; Solomon, R.; Okrainec, K.; Abrams, H.; Tai, H. Using co-design methods to create a patient-oriented discharge summary. J. Clin. Outcom. Manag. 2016, 23, 321–328. [Google Scholar]
- Cui, A.S.; Wu, F. Utilizing customer knowledge in innovation: Antecedents and impact of customer involvement on new product performance. J. Acade. Market. Sci. 2016, 44, 516–538. [Google Scholar] [CrossRef]
- Tommasetti, A.; Troisi, O.; Vesci, M. Measuring customer value co-creation behavior: Developing a conceptual model based on service-dominant logic. J. Ser. Theory Pract. 2017, 27, 930–950. [Google Scholar] [CrossRef]
- Oyner, O.; Korelina, A. The influence of customer engagement in value co-creation on customer satisfaction. Worldw. Hosp. Tour. Themes 2016, 8, 327–345. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Hsiao, S.H.; Yang, Z.; Hajli, N. The impact of sellers’ social influence on the co-creation of innovation with customers and brand awareness in online communities. Industr. Market. Manag. 2016, 54, 56–70. [Google Scholar] [CrossRef]
- Tu, X. Conditions for the co-production of new immigrant services in Hong Kong. Int. J. Public Adm. 2016, 39, 1067–1076. [Google Scholar] [CrossRef]
- Vennik, F.D.; van de Bovenkamp, H.M.; Putters, K.; Grit, K.J. Co-production in healthcare: Rhetoric and practice. Int. Rev. Adm. Sci. 2016, 82, 150–168. [Google Scholar] [CrossRef]
- Wherton, J.; Sugarhood, P.; Procter, R.; Hinder, S.; Greenhalgh, T. Co-production in practice: How people with assisted living needs can help design and evolve technologies and services. Implement. Sci. 2015, 10, 75. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, C.; Jayme, B. Community knowledge co-creation through participatory video. Act. Res.: Spe. Edit. Knowl. Democr. 2015, 13, 298–314. [Google Scholar] [CrossRef]
- Janamian, T.; Crossland, L.; Wells, L. On the road to value co-creation in health care: The role of consumers in defining the destination, planning the journey and sharing the drive. Med. J. Australia 2016, 204, S12–S14. [Google Scholar] [CrossRef]
- Lwembe, S.; Green, S.A.; Chigwende, J.; Ojwang, T.; Dennis, R. Co-production as an approach to developing stakeholder partnerships to reduce mental health inequalities: An evaluation of a pilot service. Primary Health Care Res. Develop (Cambridge University Press/UK) 2017, 18, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Anderl, E.; Marz, A.; Schumann, J.H. Nonmonetary customer value contributions in free e-services. J. Strat. Market. 2016, 24, 175–189. [Google Scholar] [CrossRef]
- Hurley, E.; Trischler, J.; Dietrich, T. Exploring the application of co-design to transformative service research. J. Ser Market. 2018. [Google Scholar] [CrossRef] [Green Version]
- Lam, B.Z.T.; Kelemen, M.; Hoo, N.J. Unearth hidden assets through community co-design and co-production. Design J. 2017, 20, 3601. [Google Scholar] [CrossRef]
- Dietrich, T.T.J.; Schuster, L.; Rundle-Thiele, S. Co-designing services with vulnerable consumers. J. Ser. Theory Pract. 2017, 27, 663–688. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, R.V.S.; Picciolli, P.; Landini, A.; Annarumma, C.; Manna, R. Fostering organizational change through co-production. Insights from an Italian experience. Int. Rev. Public Nonpr. Market. 2018, 15, 371–391. [Google Scholar] [CrossRef]
- Knight, A.; Havard, A.; Shakeshaft, A.; Maple, M.; Snijder, M.; Shakeshaft, B. The feasibility of embedding data collection into the routine service delivery of a multi-component program for high-risk young people. Int. J. Environ. Res. Public Health 2017, 14, 208. [Google Scholar] [CrossRef] [Green Version]
- Fiore, L.D.; Lavori, P.W. Integrating randomized comparative effectiveness research with patient care. New England J. Med. 2016, 374, 2152–2158. [Google Scholar] [CrossRef]
- Snijder, M.; Shakeshaft, A.; Wagemakers, A.; Stephens, A.; Calabria, B. A systematic review of studies evaluating Australian indigenous community development projects: The extent of community participation, their methodological quality and their outcomes. BMC Public Health 2015, 15, 1154. [Google Scholar] [CrossRef] [Green Version]
- Sol, J.; Beers, P.J.; Oosting, S.; Geerling-Eiff, F. Action research in a regional development setting: Students as boundary workers in a learning multi-actor network. In Knowledge in Action; Springer: Manhattan, NY, USA, 2011; pp. 133–152. [Google Scholar]
- Wagemakers, A.; Corstjens, R.; Koelen, M.; Vaandrager, L.; van’t Riet, H.; Dijkshoorn, H. Participatory approaches to promote healthy lifestyles among Turkish and Moroccan women in Amsterdam. Promot. Educ. 2008, 15, 17–23. [Google Scholar] [CrossRef]
- Wagemakers, A.; van Husen, G.; Barrett, J.B.; Koelen, M.A. Amsterdam’s STI/HIV programme: An innovative strategy to achieve and enhance the participation of migrant community-based organisations. Health Educ. J. 2015, 74, 411–423. [Google Scholar] [CrossRef]
- Campbell, H.; Vanderhoven, D. Knowledge that Matters: Realising the Potential of Co-production; N8 Research Partnership: Manchester, UK, 2016; pp. 1–70. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropract. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| 1.1 | Terms Identified during Snowball Search of Google Scholar | No. of Terms |
| “co-creation (would also retrieve “value co-creation”, “resonant co-creation” and “co-creation of knowledge”), “co-assessment”, “co-commissioning”, “co-conception”, “co-construction”, “co-delivery”, “co-design”, “co-development”, “co-dissemination”, “co-evaluation”, “co-ideation”, “co-implementation”, “co-initiation”, “co-innovation”, “co-learning”, “co-management”, “co-planning”, “co-possibility”, “co-production”, “co-testing”, “knowledge creation” and “knowledge co-production” | 22 | |
| 1.2 | Most Frequently Used Keywords Appearing in Electronic Databases (>50 Records Retrieved) | No. of Terms |
| “co-construction” OR “co-creation” OR “co-design” OR “co-dissemination” OR “co-evaluation” OR “co-implementation” OR “co-management” OR “co-production” OR “creation of value/value creation” OR “knowledge creation” | 10 | |
| Range of Terms | Industry | Papers | Total Number of Manifest Descriptions | |||
|---|---|---|---|---|---|---|
| Community Based | Business & Marketing | Health & Welfare | Public Policy | |||
| Co-Ideation (n = 9 terms) | n = 26 | |||||
| Co-Ideation | ✓[41] | Agrawal & Rahman [41] | 1 | |||
| Co-Commissioning | ✓[42] | Podgórniak-Krzykacz [42] | 1 | |||
| Co-Creation | ✓[43,44] | ✓[45,46] | ✓[47] | Bryan-Kinns [44]; Jamin [47]; Wang [43]; Zhang [45]; Lapolla & Sanders [46] | 5 | |
| Co-Design | ✓[48,49,50,51,52] | ✓[52,53] | ✓[49,54] | ✓[55] | Broadley & Smith [48]; Hjelmfors [49]; Ward [54]; De Jans [56]; Durl [53]; Westhorp [50]; Lam & Dearden [55]; Taffe [52]; Kwon [51] | 9 |
| Co-Development | ✓[57] | Candi [57] | 1 | |||
| Co-Learning | ✓[58] | Sharma & Conduit [58] | 1 | |||
| Co-Planning | ✓[59,60] | Barbera [59]; Sicilia [60] | 2 | |||
| Co-Production | ✓[61] | ✓[62,63,64] | ✓[65] | Dunn [62]; Hawkins [63]; Strokosch & Osborne [61]; Van Damme [64]; Thijssen & Van Doreen [65] | 5 | |
| Co-Reflection | ✓[66] | Mostafa [66] | 1 | |||
| Co-Design (n = 7 terms) | n = 36 | |||||
| Co-Design | ✓[48,50,51] | ✓[41,56,52,53,66,67] | ✓[49,54,68] | ✓[60,69,70,71] | Broadley & Smith [48]; Hetrick [68]; Hjelmfors [49]; Ward [54]; De Jans [56]; Durl [53]; Agrawal & Rahman [41]; Bessant [69]; Hahn-Goldberg [71]; Mostafa [66]; Sicilia [60]; Teichmann [67]; Westhorp [50]; Merickova [70]; Taffe [52]; Kwon [51] | 16 |
| Co-Development | ✓[57,72] | Candi [57]; Cui & Wu [72] | 2 | |||
| Co-Creation | ✓[44] | ✓[45,46,73,74] | ✓[47] | Bryan-Kinns [44]; Jamin [47]; Tommasetti [73]; Oyner & Korelina [74]; Zhang [45]; Lapolla & Sanders [46] | 6 | |
| Co-Innovation | ✓[75] | Wang [75] | 1 | |||
| Co-Production | ✓[61,76] | ✓[58,62,63,64,77,78] | ✓[42] | Hawkins [63]; Dunn [62]; Sharma & Conduit [58]; Strokosch & Osborne [61]; Tu [76]; Van Damme [64]; Vennik [77]; Podgórniak-Krzykacz [42]; Wherton [78] | 9 | |
| Knowledge Co-Creation | ✓[79] | Tremblay & Jayme [79] | 1 | |||
| Value Co-Creation | ✓[80] | Janamian [80] | 1 | |||
| Co-Implementation (n = 5 terms) | n = 17 | |||||
| Co-Implementation | ✓[42,70,76] | Tu [76]; Podgórniak-Krzykacz [42]; Merickova [70] | 3 | |||
| Co-Creation | ✓[43,44] | ✓[46] | ✓[58] | Bryan-Kinns [44]; Sharma & Conduit [58]; Wang [43]; Lapolla & Sanders [46] | 4 | |
| Co-Delivery | ✓[81] | ✓[59,60] | Lwembe [81]; Barbera [59]; Sicilia [60] | 3 | ||
| Co-Design | ✓[55,50] | ✓[73] | Tommasetti [73]; Westhorp [50]; Lam & Dearden [55] | 3 | ||
| Co-Planning | ✓[65] | Thijssen & Van Dooren [65] | 1 | |||
| Co-Production | ✓[61,62] | Dunn [62]; Strokosch & Osborne [61] | 2 | |||
| Knowledge Creation | ✓[79] | Tremblay & Jayne [79] | 1 | |||
| Co-Evaluation (n = 7 terms) | n = 12 | |||||
| Co-Creation | ✓[47] | Jamin [47] | 1 | |||
| Co-Design | ✓[56,50] | De Jans [56]; Westhorp [50] | 2 | |||
| Co-Evaluation | ✓[41] | ✓[60] | Sicilia [60]; Agrawal & Rahman [41] | 2 | ||
| Co-Management | ✓[82] | Anderl [82] | 1 | |||
| Co-Production | ✓[61] | ✓[63,64] | ✓[42] | Hawkins [63]; Strokosch & Osborne [61]; Van Damme [64]; Podgórniak-Krzykacz [42] | 4 | |
| Co-Recovery | ✓[66] | Mostafa [66] | 1 | |||
| Knowledge Co-Creation | ✓[79] | Tremblay & Jayme [79] | 1 | |||
| Total terms used/industry | 23 | 28 | 23 | 17 | n = 91 | |
| Categories | Sub-Categories | Examples from the Literature |
|---|---|---|
| Activity | Collaboration represented by the prefix “co” implying partnership and equality | Union/collaboration of stakeholders (researchers and non-researchers) [83,84];“mutual knowledge exchange” [44]; “common understanding” [66]; shared vision and decision-making; meaningful engagement with participants [47,62]; equal voice and a collective vision [54,60] |
| Activity | Ideation | “generate” [18,83], “explore” [85]; “brainstorm ideas” [49], “provoke discussion” [44,78]; reflect on how to meet community needs, solve problems and improve service delivery [58,61,62,86,87] |
| Activity | Designing | taking of ideas (generated in the co-ideation phase); planning of the production of concrete outcomes (products, services or programs) [41,66] |
| Activity | Implementing | participation of stakeholders in the delivery of services and programs [42] |
| Activity | Evaluating | usability testing of prototypes and products [47] and state actors and the public to assess the quality of public services [70,86]; provide constructive feedback on services, interventions or products to researchers [56]; feedback may be collected through the administration of pre- and post-initiative questionnaires or engagement in focus groups [53,59]; feedback is collected and used to improve services [56] |
| Core Principles | Definition | Operationalising Examples |
|---|---|---|
| 1. Rigorous research methods | Experimental or quasi experimental Evidence-based measures |
|
| 2. Embedded | Integration of best-evidence measures into routine data collection processes [87] Programs or policies implemented into routine practice |
|
| 3. Contains Four Processes | ||
| 3.i Co-ideation | Engaging in open dialogue to share new and creative ideas for the solving of problems relating to new products, services, policies and programs |
|
| 3.ii Co-design | Providing a description of the technical details of new products, services, procedures, policies or programs (prototype), as well as the research methods to be used (protocols). This process may include assessment of funding sources, availability of resources, research processes (e.g., ethics) and timelines. |
|
| 3. iii Co-implementation | Implementing the co-designed program, policy or clinical procedures in accordance with the research protocol. This process may be a one-time collaborative event or an arrangement over the longer term. |
|
| 3.iv Co-evaluation | Embedding data collection or other formal research techniques into the co-implementation process. Researchers with relevant bio-statistical skills undertake analyses. Co-interpretation of the meaning and implications of the results. |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearce, T.; Maple, M.; Shakeshaft, A.; Wayland, S.; McKay, K. What is the Co-Creation of New Knowledge? A Content Analysis and Proposed Definition for Health Interventions. Int. J. Environ. Res. Public Health 2020, 17, 2229. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072229
Pearce T, Maple M, Shakeshaft A, Wayland S, McKay K. What is the Co-Creation of New Knowledge? A Content Analysis and Proposed Definition for Health Interventions. International Journal of Environmental Research and Public Health. 2020; 17(7):2229. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072229
Chicago/Turabian StylePearce, Tania, Myfanwy Maple, Anthony Shakeshaft, Sarah Wayland, and Kathy McKay. 2020. "What is the Co-Creation of New Knowledge? A Content Analysis and Proposed Definition for Health Interventions" International Journal of Environmental Research and Public Health 17, no. 7: 2229. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072229