Interventions to Improve the Quality of Life of Patients with Chronic Obstructive Pulmonary Disease: A Global Mapping During 1990–2018

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database and Search Strategy
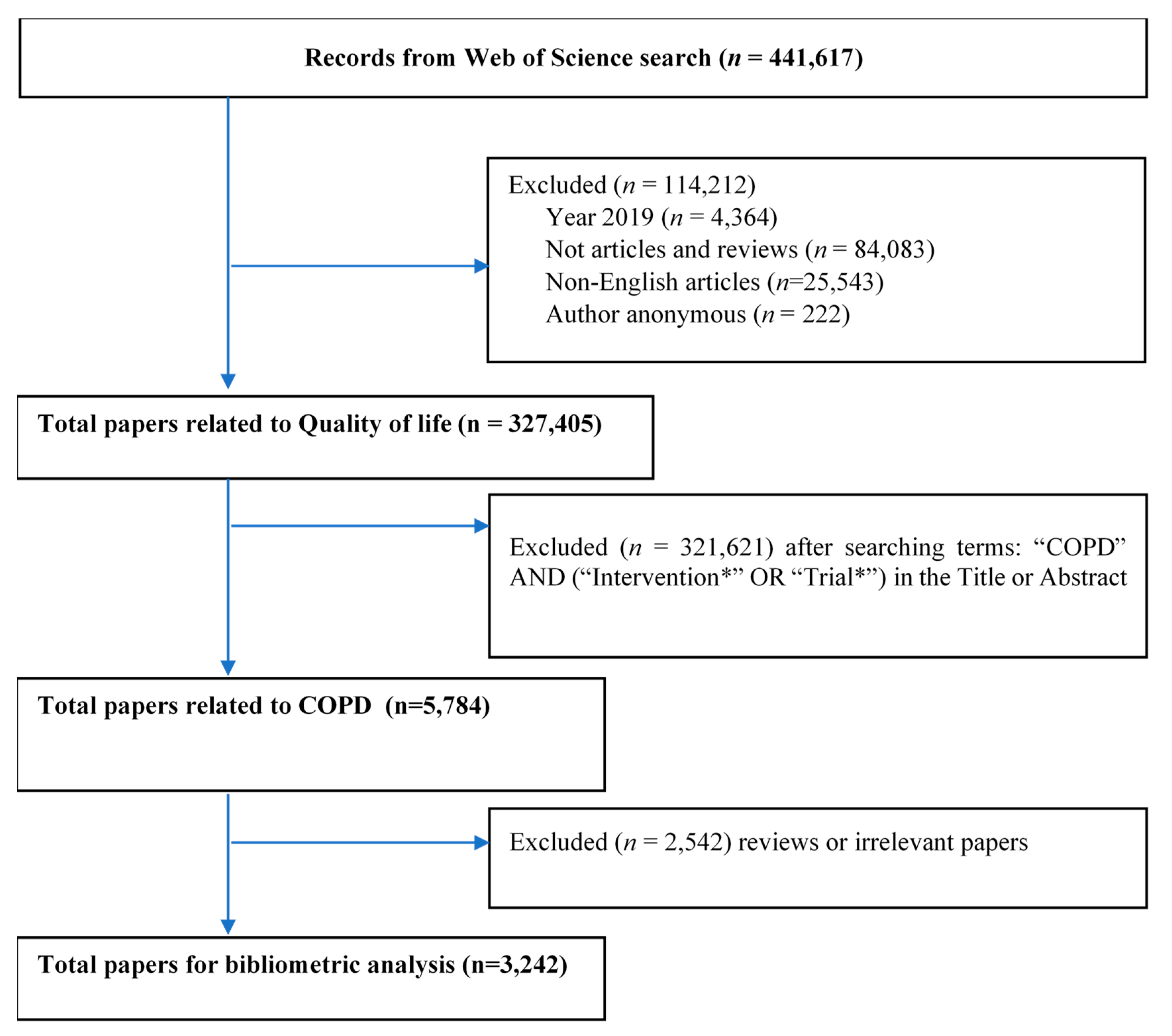
- Step 1: With the use of Boolean operators “OR”, the search query was developed to identify the number of published items related to “Quality of life” OR “well-being”. Only English research articles and research reviews were included, while grey literature, conference proceedings, or books/book chapters in any other language were excluded. Papers having anonymous authors and publications in 2019 were also limited. This research began in the middle of 2019; thus, this data could not reflect the research trend for the whole year. Data in WoS databases under text format was downloaded and imported to STATA version 15.0 (STATACorp., Texas, TX, USA) for further extraction. (See Table A1)
- Step 2: STATA syntax was applied to filter the papers in step 1 with the terms “Intervention” OR “Interventions” OR “trial” OR “trials” in titles or abstracts.
- Step 3: The COPD keywords were formed by COPD specialists and reviewing some papers and MeSH term library of PubMed. These terms were used to search in the title and keyword fields among papers in step 2 (see Table A1), and there were 5784 papers for further screening.
- Step 4: Two researchers separately screened the titles and abstracts of 5784 papers to exclude papers not related to COPD. A group discussion with a senior researcher was conducted if there were any contradictions. A total of 3242 papers were imported to STATA for further analysis. (See Figure A1).
2.2. Data Analysis
3. Results
Overall Growth and Essential Characteristics of Research
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Search Query | Search Result |
|---|---|---|
| # 1 | TS = (“quality of life”) | 355,541 |
| # 2 | TS = (“well-being”) | 104,048 |
| # 3 | #2 OR #1 | 441,617 |
| # 4 | #2 OR #1 | 437,253 |
| Refined by: [excluding] Publication Years: (2019) | ||
| # 5 | #2 OR #1 | 353,171 |
| Refined by: [excluding] Publication Years: (2019) AND [excluding] Document Types: ( Meeting Abstract Or Proceedings Paper Or Editorial Material Or Book Chapter Or Letter Or Book Review Or Correction Or Note Or News Item Or Book Or Reprint Or Early Access Or Retracted Publication Or Biographical Item Or Correction Addition Or Discussion Or Data Paper Or Retraction Or Bibliography Or Fiction Creative Prose Or Item About An Individual Or Poetry Or Software Review) | ||
| # 6 | #2 OR #1 | 353,170 |
| Refined by: [excluding] Publication Years: (2019) AND [excluding] Document Types: ( Meeting Abstract Or Proceedings Paper Or Editorial Material Or Book Chapter Or Letter Or Book Review Or Correction Or Note Or News Item Or Book Or Reprint Or Early Access Or Retracted Publication Or Biographical Item Or Correction Addition Or Discussion Or Data Paper Or Retraction Or Bibliography Or Fiction Creative Prose Or Item About An Individual Or Poetry Or Software Review ) AND [excluding] Document Types: (Tv Review Radio Review) | ||
| # 7 | #2 OR #1 | 327,627 |
| Refined by: [excluding] Publication Years: (2019) AND [excluding] Document Types: (Meeting Abstract Or Proceedings Paper Or Editorial Material Or Book Chapter Or Letter Or Book Review Or Correction Or Note Or News Item Or Book Or Reprint Or Early Access Or Retracted Publication Or Biographical Item Or Correction Addition Or Discussion Or Data Paper Or Retraction Or Bibliography Or Fiction Creative Prose Or Item About An Individual Or Poetry Or Software Review) AND [excluding] Document Types: (Tv Review Radio Review) AND [excluding]Languages: (German Or Spanish Or French Or Portuguese Or Russian Or Turkish Or Polish Or Italian Or Korean Or Czech Or Hungarian Or Croatian Or Greek Or Dutch Or Japanese Or Slovenian Or Slovak Or Lithuanian Or Serbian Or Persian Or Malay Or Romanian Or Chinese Or Icelandic Or Arabic Or Afrikaans Or Norwegian Or Ukrainian Or Danish Or Catalan Or Swedish Or Estonian Or Bulgarian Or Serbo Croatian Or Galician Or Georgian Or Esperanto Or Finnish Or Hebrew Or Indonesian Or Welsh) | ||
| # 8 | AU = (“Anonymous” OR “anonymous”) | 1,406,800 |
| # 9 | #7 NOT #8 | 327,405 |

References
- World Health Organization. Chronic obstructive pulmonary disease: Definition. Available online: https://www.who.int/respiratory/copd/definition/en/ (accessed on 12 July 2019).
- OECD/EUROPEAN UNION 2016. Asthma and COPD prevalence. In Health at a Glance: Europe 2016–State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016. [Google Scholar] [CrossRef]
- Group, R.C.W. COPD prevalence in 12 Asia–Pacific countries and regions: Projections based on the COPD prevalence estimation model. Respirology 2003, 8, 192–198. [Google Scholar]
- National Center for Chronic Disease Prevention and Health Promotion. COPD Prevalence in the United States. Available online: https://www.cdc.gov/copd/data.html (accessed on 12 July 2019).
- Mehrotra, A.; Akanbi, M.O.; Gordon, S.B. The burden of COPD in Africa: A literature review and prospective survey of the availability of spirometry for COPD diagnosis in Africa. Trop. Med. Int. Health TM IH 2009, 14, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Basquill, C.; Papana, A.; Chan, K.Y.; Rudan, I.; Campbell, H. An estimate of the prevalence of COPD in Africa: A systematic analysis. Copd J. Chronic Obstr. Pulm. Dis. 2015, 12, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Peruzza, S.; Sergi, G.; Vianello, A.; Pisent, C.; Tiozzo, F.; Manzan, A.; Coin, A.; Inelmen, E.; Enzi, G. Chronic obstructive pulmonary disease (COPD) in elderly subjects: Impact on functional status and quality of life. Respir. Med. 2003, 97, 612–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agusti, À.; Soriano, J.B. COPD as a systemic disease. Copd J. Chronic Obstr. Pulm. Dis. 2008, 5, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Edwards, L.D.; Lomas, D.A.; MacNee, W.; Miller, B.E.; Rennard, S.; Silverman, E.K. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir. Res. 2010, 11, 122. [Google Scholar] [CrossRef]
- Restrepo, M.I.; Sibila, O.; Anzueto, A. Pneumonia in patients with chronic obstructive pulmonary disease. Tuberc. Respir. Dis. (Seoul) 2018, 81, 187–197. [Google Scholar] [CrossRef]
- Chaouat, A.; Naeije, R.; Weitzenblum, E. Pulmonary hypertension in COPD. Eur. Respir. J. 2008, 32, 1371–1385. [Google Scholar] [CrossRef]
- Quint, J. The Relationship between COPD and Cardiovascular Disease. Tanaffos 2017, 16, S16–S17. [Google Scholar]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A.; Anxiety, A.W.P.O.; Depression, C. Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest 2008, 134, 43S–56S. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.F.S.; Kunik, M.E.; Molinari, V.A.; Hillman, S.L.; Lalani, S.; Orengo, C.A.; Petersen, N.J.; Nahas, Z.; Goodnight-White, S. Functional impairment in COPD patients: The impact of anxiety and depression. Psychosomatics 2000, 41, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Vercoulen, J.H.; Sprangers, M.A.G.; Wouters, E.F.M. Fatigue in COPD: An important yet ignored symptom. Lancet Respir. Med. 2017, 5, 542–544. [Google Scholar] [CrossRef]
- Franssen, F.M.E.; Smid, D.E.; Deeg, D.J.H.; Huisman, M.; Poppelaars, J.; Wouters, E.F.M.; Spruit, M.A. The physical, mental, and social impact of COPD in a population-based sample: Results from the Longitudinal Aging Study Amsterdam. NPJ Prim. Care Respir. Med. 2018, 28, 30. [Google Scholar] [CrossRef]
- Price, D.; Small, M.; Milligan, G.; Higgins, V.; Gil, E.G.; Estruch, J. Impact of night-time symptoms in COPD: A real-world study in five European countries. Int. J. Chron. Obs. Pulmon. Dis. 2013, 8, 595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephenson, J.J.; Cai, Q.; Mocarski, M.; Tan, H.; Doshi, J.A.; Sullivan, S.D. Impact and factors associated with nighttime and early morning symptoms among patients with chronic obstructive pulmonary disease. Int. J. Chron. Obs. Pulmon. Dis. 2015, 10, 577. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHOQOL: Measuring Quality of Life. Available online: https://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/ (accessed on 21 April 2020).
- Gandhi, S.K.; Kong, S.X. Quality-of-life measures in the evaluation of antihypertensive drug therapy: Reliability, validity, and quality-of-life domains. Clin. Ther. 1996, 18, 1276–1295. [Google Scholar] [CrossRef]
- Taylor, S.H. Drug therapy and quality of life in angina pectoris. Am. Heart J. 1987, 114, 234–240. [Google Scholar] [CrossRef]
- Wright, E.K.; Kamm, M.A. Impact of drug therapy and surgery on quality of life in Crohn‘s disease: A systematic review. Inflamm. Bowel Dis. 2015, 21, 1187–1194. [Google Scholar] [CrossRef]
- Benzo, R.P.; Abascal-Bolado, B.; Dulohery, M.M. Self-management and quality of life in chronic obstructive pulmonary disease (COPD): The mediating effects of positive affect. Patient Educ. Couns. 2016, 99, 617–623. [Google Scholar] [CrossRef] [Green Version]
- Tran, B.X.; Harijanto, C.; Vu, G.T.; Ho, R.C. Global Mapping of Interventions to improve Quality of Life using Mind-body therapies during 1990–2018. Complementary Ther. Med. 2020, 49, 102350. [Google Scholar] [CrossRef]
- Hawthorne, G.; Richardson, J.; Osborne, R. The Assessment of Quality of Life (AQoL) instrument: A psychometric measure of health-related quality of life. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 1999, 8, 209–224. [Google Scholar] [CrossRef] [PubMed]
- Feldman, G.J. Improving the quality of life in patients with chronic obstructive pulmonary disease: Focus on indacaterol. Int. J. Chron. Obs. Pulmon. Dis. 2013, 8, 89. [Google Scholar] [CrossRef] [PubMed]
- Godtfredsen, N.S.; Lam, T.H.; Hansel, T.T.; Leon, M.; Gray, N.; Dresler, C.; Burns, D.; Prescott, E.; Vestbo, J. COPD-related morbidity and mortality after smoking cessation: Status of the evidence. Eur. Respir. J. 2008, 32, 844–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamarro, C.G.; Bernabé, M.B.; Santamaría, B.R.; Rodríguez, J.H. Smoking in COPD. Arch. De Bronconeumol. 2011, 47, 3–9. [Google Scholar]
- Antus, B. Pharmacotherapy of Chronic Obstructive Pulmonary Disease: A Clinical Review. ISRN Pulmonol. 2013, 2013, 11. [Google Scholar] [CrossRef]
- Safka, K.A.; McIvor, R.A. Non-pharmacological management of chronic obstructive pulmonary disease. Ulst. Med. J. 2015, 84, 13–21. [Google Scholar]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anesth. 2018, 71, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Gregersen, T.L.; Green, A.; Frausing, E.; Ringbæk, T.; Brøndum, E.; Suppli Ulrik, C. Do telemedical interventions improve quality of life in patients with COPD? A systematic review. Int. J. Chron. Obs. Pulmon. Dis. 2016, 11, 809–822. [Google Scholar] [CrossRef] [Green Version]
- Coronini-Cronberg, S.; Heffernan, C.; Robinson, M. Effective smoking cessation interventions for COPD patients: A review of the evidence. JRSM Short Rep. 2011, 2, 1–12. [Google Scholar] [CrossRef]
- Papadopoulos, G.; Vardavas, C.I.; Limperi, M.; Linardis, A.; Georgoudis, G.; Behrakis, P. Smoking cessation can improve quality of life among COPD patients: Validation of the clinical COPD questionnaire into Greek. BMC Pulm. Med. 2011, 11, 13. [Google Scholar] [CrossRef] [Green Version]
- Ubolnuar, N.; Tantisuwat, A.; Thaveeratitham, P.; Lertmaharit, S.; Kruapanich, C.; Mathiyakom, W. Effects of Breathing Exercises in Patients With Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis. Ann. Rehabil. Med. 2019, 43, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, G.R.; Vanz, S.A.S.; Barbosa, M.C. Scientometric indicators for Brazilian research on High Energy Physics, 1983–2013. An. Da Acad. Bras. De Ciências 2017, 89, 2525–2543. [Google Scholar] [CrossRef] [PubMed]
- Begum, M.; Lewison, G.; Wright, J.S.; Pallari, E.; Sullivan, R. European non-communicable respiratory disease research, 2002–2013: Bibliometric study of outputs and funding. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweileh, W.M.; Al-Jabi, S.W.; Sa′ed, H.Z.; Sawalha, A.F. Bronchial asthma and chronic obstructive pulmonary disease: Research activity in Arab countries. Multidiscip. Respir. Med. 2014, 9, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín-Martín, A.; Orduna-Malea, E.; Delgado López-Cózar, E. Coverage of highly-cited documents in Google Scholar, Web of Science, and Scopus: A multidisciplinary comparison. Scientometrics 2018, 116, 2175–2188. [Google Scholar] [CrossRef] [Green Version]
- Clarivate Analytics. Web of Science databases. Available online: https://clarivate.com/products/web-of-science/databases/ (accessed on 26 June 2019).
- Li, Y.; Rapkin, B.; Atkinson, T.M.; Schofield, E.; Bochner, B.H. Leveraging Latent Dirichlet Allocation in processing free-text personal goals among patients undergoing bladder cancer surgery. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2019. [Google Scholar] [CrossRef]
- Valle, D.; Albuquerque, P.; Zhao, Q.; Barberan, A.; Fletcher, R.J., Jr. Extending the Latent Dirichlet Allocation model to presence/absence data: A case study on North American breeding birds and biogeographical shifts expected from climate change. Glob. Chang. Biol. 2018, 24, 5560–5572. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Zare, A.; Trinh, H.N.; Omotara, G.O.; Cobb, J.T.; Lagaunne, T.A. Partial Membership Latent Dirichlet Allocation for Soft Image Segmentation. IEEE Trans. Image Process. A Publ. IEEE Signal. Process. Soc. 2017, 26, 5590–5602. [Google Scholar] [CrossRef]
- Lu, H.M.; Wei, C.P.; Hsiao, F.Y. Modeling healthcare data using multiple-channel latent Dirichlet allocation. J. Biomed. Inform. 2016, 60, 210–223. [Google Scholar] [CrossRef]
- Gross, A.; Murthy, D. Modeling virtual organizations with Latent Dirichlet Allocation: A case for natural language processing. Neural Netw. Off. J. Int. Neural Netw. Soc. 2014, 58, 38–49. [Google Scholar] [CrossRef]
- Rabe, K.F.; Hurd, S.; Anzueto, A.; Barnes, P.J.; Buist, S.A.; Calverley, P.; Fukuchi, Y.; Jenkins, C.; Rodriguez-Roisin, R.; van Weel, C.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2007, 176, 532–555. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD; Global Initiative for Chronic Obstructive Lung Disease, Inc.: Fontana, WI, USA, 2019. [Google Scholar]
- Troosters, T.; Gosselink, R.; Janssens, W.; Decramer, M. Exercise training and pulmonary rehabilitation: New insights and remaining challenges. Eur. Respir. Rev. 2010, 19, 24–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- STATA. Cluster Dendrogram—Dendrograms for Hierarchical Cluster Analysis. Available online: https://www.stata.com/manuals13/mvclusterdendrogram.pdf (accessed on 22 April 2020).
- Moffat, D.; Ronan, D.; Reiss, J.D. Unsupervised taxonomy of sound effects. Context 2017, 6, 7. [Google Scholar]
- Laniado-Laborin, R. Smoking and chronic obstructive pulmonary disease (COPD). Parallel epidemics of the 21 century. Int. J. Environ. Res. Public Health 2009, 6, 209–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, B.X.; Nguyen, L.H.; Pham, N.M.; Vu, H.T.T.; Nguyen, H.T.; Phan, D.H.; Ha, G.H.; Pham, H.Q.; Nguyen, T.P.; Latkin, C.A. Global Mapping of Interventions to Improve Quality of Life of People with Diabetes in 1990–2018. Int. J. Environ. Res. Public Health 2020, 17, 1597. [Google Scholar] [CrossRef] [Green Version]
- Vu, G.T.; Tran, B.X. Global Research on Quality of Life of Patients with HIV/AIDS: Is It Socio-Culturally Addressed? (GAP(RESEARCH)). Int. J. Environ. Res. Public Health 2020, 17, 2127. [Google Scholar] [CrossRef] [Green Version]
- Torres-Duque, C.; Maldonado, D.; Perez-Padilla, R.; Ezzati, M.; Viegi, G. Biomass fuels and respiratory diseases: A review of the evidence. Proc. Am. Thorac. Soc. 2008, 5, 577–590. [Google Scholar] [CrossRef]
- Pleasants, R.A.; Riley, I.L.; Mannino, D.M. Defining and targeting health disparities in chronic obstructive pulmonary disease. Int. J. Chron. Obs. Pulmon. Dis. 2016, 11, 2475–2496. [Google Scholar] [CrossRef] [Green Version]
- Bezuidenhout, L.; Chakauya, E. Hidden concerns of sharing research data by low/middle-income country scientists. Glob. Bioeth. Probl. Di Bioet. 2018, 29, 39–54. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, L.M.P.; Khan, S.; Moore, J.E.; Timmings, C.; van Lettow, M.; Vogel, J.P.; Khan, D.N.; Mbaruku, G.; Mrisho, M.; Mugerwa, K. Low-and middle-income countries face many common barriers to implementation of maternal health evidence products. J. Clin. Epidemiol. 2016, 76, 229–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuwayhid, I.A. Occupational health research in developing countries: A partner for social justice. Am. J. Public Health 2004, 94, 1916–1921. [Google Scholar] [CrossRef] [PubMed]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montuschi, P. Pharmacological treatment of chronic obstructive pulmonary disease. Int. J. Chron. Obs. Pulmon. Dis. 2006, 1, 409. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, J.; Li, H.; Zhu, X.; Wang, G. Efficacy of integrative respiratory rehabilitation training in exercise ability and quality of life of patients with chronic obstructive pulmonary disease in stable phase: A randomized controlled trial. Zhong Xi Yi Jie He Xue Bao J. Chin. Integr. Med. 2010, 8, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Lobato, S.; Alises, S.M.; Rodríguez, E.P. Current status of noninvasive ventilation in stable COPD patients. Int. J. Chron. Obs. Pulmon. Dis. 2006, 1, 129–135. [Google Scholar] [CrossRef]
- Murphy, P.B.; Rehal, S.; Arbane, G.; Bourke, S.; Calverley, P.M.A.; Crook, A.M.; Dowson, L.; Duffy, N.; Gibson, G.J.; Hughes, P.D.; et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. JAMA 2017, 317, 2177–2186. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Chronic Obstructive Pulmonary Disease in over 16s: Diagnosis and Management Evidence Reviews for Self Management, Education and Telehealth; National Institute for Health and Care Excellence: London, UK, 2018. [Google Scholar]
- Zwerink, M.; Brusse-Keizer, M.; van der Valk, P.D.; Zielhuis, G.A.; Monninkhof, E.M.; van der Palen, J.; Frith, P.A.; Effing, T. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Smith, M.C.; Wrobel, J.P. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int. J. Chron. Obs. Pulmon. Dis. 2014, 9, 871. [Google Scholar] [CrossRef] [Green Version]
- Cavaillès, A.; Brinchault-Rabin, G.; Dixmier, A.; Goupil, F.; Gut-Gobert, C.; Marchand-Adam, S.; Meurice, J.-C.; Morel, H.; Person-Tacnet, C.; Leroyer, C. Comorbidities of COPD. Eur. Respir. Rev. 2013, 22, 454–475. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. COPD, associated Comorbidities and Risk Factors. Available online: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd-associated-comorbidities-risk-factors/contents/about-copd-and-associated-comorbidities (accessed on 17 June 2019).
- Khanal, P. Bringing all together for research capacity building in LMICs. Lancet Glob. Health 2017, 5, e868. [Google Scholar] [CrossRef] [Green Version]
- ESSENCE on Health Research. Seven Principle for Strengthening Research Capacity in Low-and-middle-income Countries: Simple Ideas in a Complex World; TDR/World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Ali, N.; Hill, C.; Kennedy, A.; IJsselmuiden, C.C. COHRED Record Paper 5. In What Factors Influence National Health Research Agendas in Low and Middle Income Countries? Council on Health Research for Development (COHRED): Geneva, Switzerland, 2006. [Google Scholar]
- Wang, H.; Wu, F.; Lu, W.; Yang, Y.; Li, X.; Li, X.; Zhuang, Y. Identifying Objective and Subjective Words via Topic Modeling. IEEE Trans. Neural Netw. Learn. Syst. 2018, 29, 718–730. [Google Scholar] [CrossRef] [PubMed]




| Type of Data | Unit of Analysis | Analytical Methods | Presentations of Results |
|---|---|---|---|
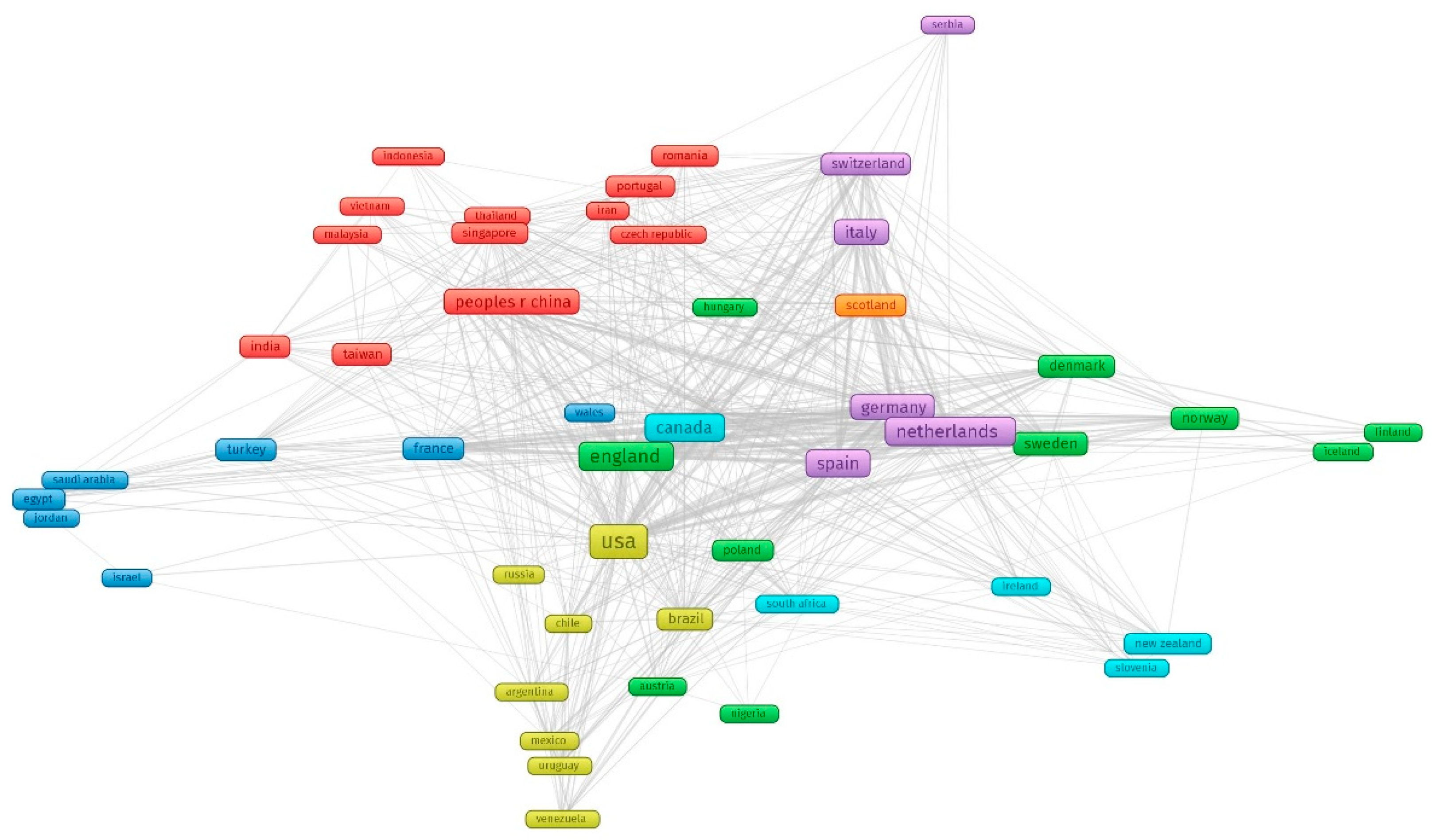
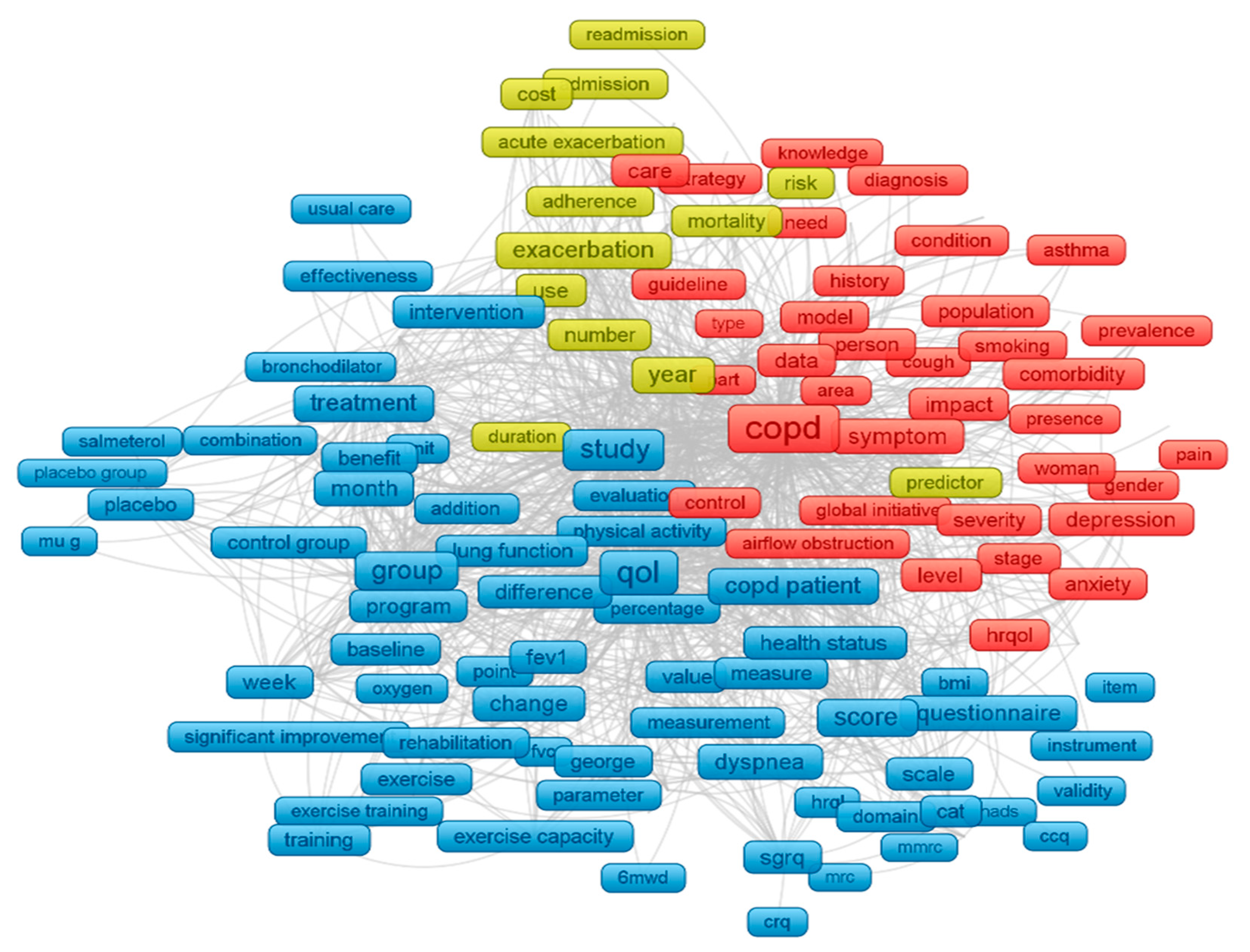
| Terms, Countries | Words | Frequency of co-occurrence | Map of terms co-occurrence clusters |
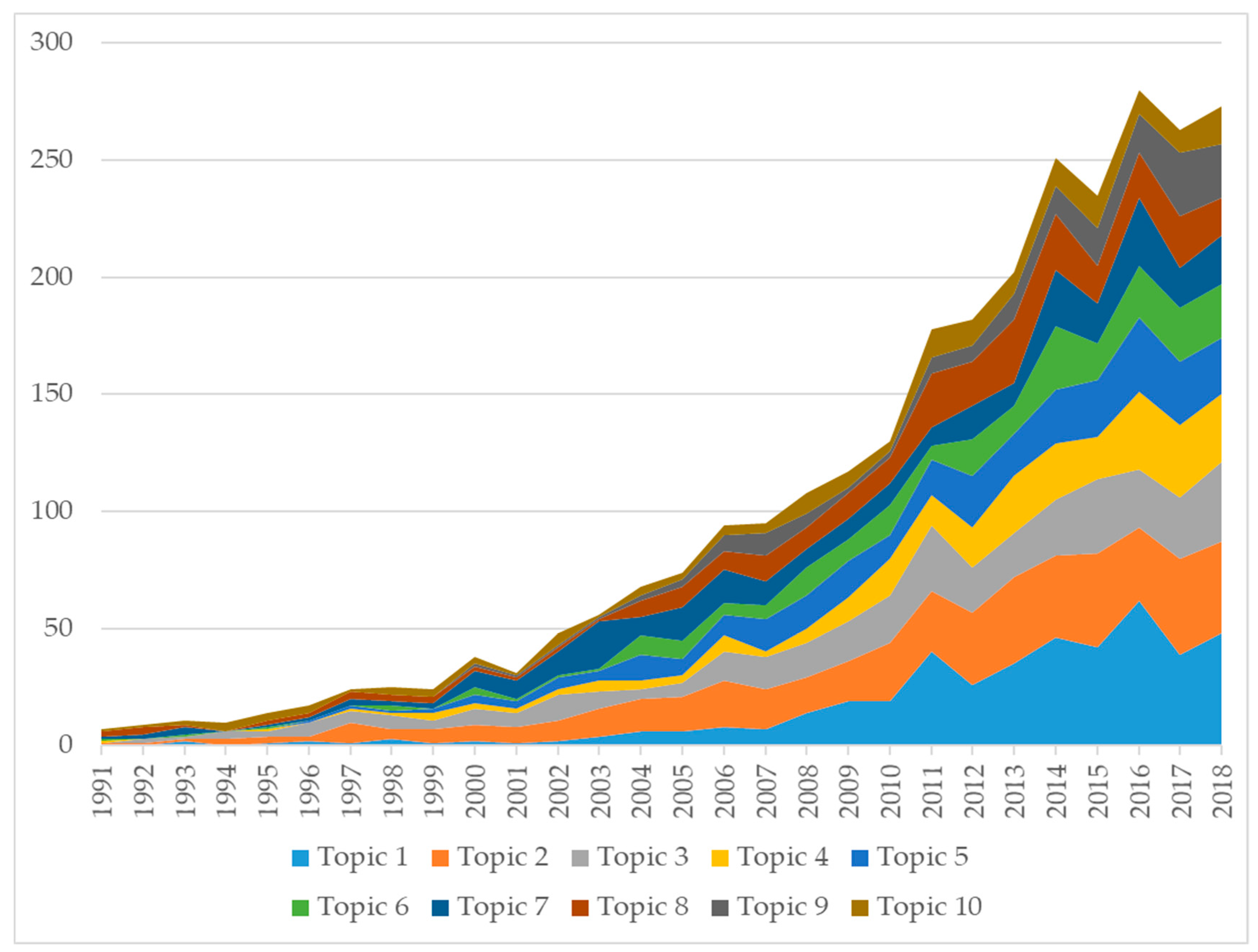
| Abstracts | Papers | Latent Dirichlet Allocation | Ten classifications of research topics |
| WoS classification of research areas | WoS research areas | Frequency of co-occurrence | Dendrogram of research disciplines (WoS classification) |
| Year Published | Total Number of Papers | Total Citations | Mean Cite Rate per Year | Total Usage Last 6 Month | Total Usage Last 5 Years | Mean Use Rate Last 6 Month | Mean Use Rate Last 5 Year |
|---|---|---|---|---|---|---|---|
| 2018 | 314 | 197 | 0.6 | 562 | 822 | 1.8 | 0.5 |
| 2017 | 295 | 1763 | 3.0 | 356 | 1756 | 1.2 | 1.2 |
| 2016 | 306 | 1946 | 2.1 | 254 | 2055 | 0.8 | 1.3 |
| 2015 | 270 | 3311 | 3.1 | 219 | 2198 | 0.8 | 1.6 |
| 2014 | 284 | 5101 | 3.6 | 177 | 2753 | 0.6 | 1.9 |
| 2013 | 234 | 3970 | 2.8 | 128 | 2451 | 0.5 | 2.1 |
| 2012 | 199 | 4653 | 3.3 | 78 | 1825 | 0.4 | 1.8 |
| 2011 | 189 | 6880 | 4.6 | 90 | 1424 | 0.5 | 1.5 |
| 2010 | 144 | 5733 | 4.4 | 75 | 1146 | 0.5 | 1.6 |
| 2009 | 128 | 5719 | 4.5 | 61 | 823 | 0.5 | 1.3 |
| 2008 | 127 | 6549 | 4.7 | 36 | 819 | 0.3 | 1.3 |
| 2007 | 109 | 5158 | 3.9 | 33 | 492 | 0.3 | 0.9 |
| 2006 | 107 | 6800 | 4.9 | 28 | 514 | 0.3 | 1.0 |
| 2005 | 86 | 4625 | 3.8 | 37 | 422 | 0.4 | 1.0 |
| 2004 | 75 | 5445 | 4.8 | 30 | 448 | 0.4 | 1.2 |
| 2003 | 62 | 6317 | 6.4 | 20 | 385 | 0.3 | 1.2 |
| 2002 | 56 | 5847 | 6.1 | 15 | 257 | 0.3 | 0.9 |
| 2001 | 40 | 2757 | 3.8 | 3 | 157 | 0.1 | 0.8 |
| 2000 | 43 | 5670 | 6.9 | 28 | 324 | 0.7 | 1.5 |
| 1999 | 28 | 1612 | 2.9 | 6 | 112 | 0.2 | 0.8 |
| 1998 | 32 | 3324 | 4.9 | 14 | 196 | 0.4 | 1.2 |
| 1997 | 29 | 2223 | 3.5 | 8 | 146 | 0.3 | 1.0 |
| 1996 | 18 | 2275 | 5.5 | 3 | 91 | 0.2 | 1.0 |
| 1995 | 16 | 1681 | 4.4 | 9 | 80 | 0.6 | 1.0 |
| 1994 | 10 | 1060 | 4.2 | 0 | 40 | 0.0 | 0.8 |
| 1993 | 12 | 559 | 1.8 | 4 | 20 | 0.3 | 0.3 |
| 1992 | 9 | 420 | 1.7 | 2 | 14 | 0.2 | 0.3 |
| 1991 | 7 | 426 | 2.2 | 0 | 11 | 0.0 | 0.3 |
| No | Title | Total Citation | Published Year | Cite Rate |
|---|---|---|---|---|
| 1 | The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease | 2046 | 2004 | 136.4 |
| 2 | A 4-year trial of tiotropium in chronic obstructive pulmonary disease | 1390 | 2008 | 126.4 |
| 3 | Susceptibility to Exacerbation in Chronic Obstructive Pulmonary Disease. | 1298 | 2010 | 144.2 |
| 4 | Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease | 1223 | 1998 | 58.2 |
| 5 | Randomised, double blind, placebo-controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the ISOLDE trial* | 964 | 2000 | 50.7 |
| 6 | Development and first validation of the COPD Assessment Test | 933 | 2009 | 93.3 |
| 7 | Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease | 868 | 2005 | 62.0 |
| 8 | Outcomes following acute exacerbation of severe chronic obstructive lung disease | 863 | 1996 | 37.5 |
| 9 | Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial | 749 | 2003 | 46.8 |
| 10 | Chronic obstructive pulmonary disease: current burden and future projections | 698 | 2006 | 53.7 |
| 11 | Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease | 655 | 2000 | 34.5 |
| 12 | A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease | 609 | 2002 | 35.8 |
| 13 | Azithromycin for Prevention of Exacerbations of COPD | 578 | 2011 | 72.3 |
| 14 | Reduction of hospital utilization in patients with chronic obstructive pulmonary disease—A disease-specific self-management intervention | 576 | 2003 | 36.0 |
| 15 | Effects of pulmonary rehabilitation on physiological and psychosocial outcomes in patients with chronic obstructive pulmonary disease | 568 | 1995 | 23.7 |
| 16 | Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease | 550 | 2003 | 34.4 |
| 17 | Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: a randomised controlled trial | 536 | 2000 | 28.2 |
| 18 | Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD | 500 | 2002 | 29.4 |
| 19 | Improved health outcomes in patients with COPD during 1 year’s treatment with tiotropium | 492 | 2002 | 28.9 |
| 20 | Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease | 472 | 2003 | 29.5 |
| 21 | Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report | 467 | 2017 | 233.5 |
| 22 | Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations | 458 | 2000 | 24.1 |
| 23 | Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease—A randomized trial | 448 | 2007 | 37.3 |
| 24 | Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease | 443 | 1996 | 19.3 |
| 25 | Risk factors of readmission to hospital for a COPD exacerbation: a prospective study | 421 | 2003 | 26.3 |
| 26 | Mortality after hospitalization for COPD | 380 | 2002 | 22.4 |
| 27 | Depressive symptoms and chronic obstructive pulmonary disease—Effect on mortality, hospital readmission, symptom burden, functional status, and quality of life | 369 | 2007 | 30.8 |
| 28 | How well do we care for patients with end stage chronic obstructive pulmonary disease (COPD)? A comparison of palliative care and quality of life in COPD and lung cancer | 338 | 2000 | 17.8 |
| 29 | Randomized controlled trial of respiratory rehabilitation | 337 | 1994 | 13.5 |
| 30 | Early therapy improves of chronic obstructive outcomes of exacerbations pulmonary disease | 335 | 2004 | 22.3 |
| 31 | Quality of life changes in COPD patients treated with salmeterol | 331 | 1997 | 15.0 |
| 32 | Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities | 323 | 2009 | 32.3 |
| 33 | A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol | 323 | 2002 | 19.0 |
| 34 | Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD | 317 | 2003 | 19.8 |
| 35 | Roflumilast—an oral anti-inflammatory treatment for chronic obstructive pulmonary disease: a randomised controlled trial | 315 | 2005 | 22.5 |
| 36 | Analysis of the factors related to mortality in chronic obstructive pulmonary disease—Role of exercise capacity and health status | 314 | 2003 | 19.6 |
| 37 | Interpreting thresholds for a clinically significant change in health status in asthma and COPD | 313 | 2002 | 18.4 |
| 38 | Short- and long-term effects of outpatient rehabilitation in patients with chronic obstructive pulmonary disease: A randomized trial | 308 | 2000 | 16.2 |
| 39 | Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease: a 2 year follow up study | 299 | 2004 | 19.9 |
| 40 | Phosphodiesterase-4 inhibitors for asthma and chronic obstructive pulmonary disease | 298 | 2005 | 21.3 |
| Rank by the Highest Volume | Research Topics | N | Percent |
|---|---|---|---|
| Topic 2 | Pulmonary rehabilitation for COPD | 468 | 16.30% |
| Topic 1 | Comorbidities, mental health and QoL in COPD patients | 436 | 15.20% |
| Topic 3 | QoL of patients with COPD: validity of questionnaire | 355 | 12.40% |
| Topic 5 | Predictors for mortality due to acute exacerbation of COPD | 287 | 10.00% |
| Topic 7 | Pharmacological Therapy and COPD | 272 | 9.50% |
| Topic 8 | Management of COPD | 257 | 9.00% |
| Topic 4 | Multicomponent interventions: home care, rehabilitation, self-care education, integrated care, and pharmacy-led management | 255 | 8.90% |
| Topic 6 | Perception and QoL of patients living with COPD and their caregivers | 217 | 7.60% |
| Topic 10 | Noninvasive Ventilation and Oxygen Therapy in patient with COPD | 160 | 5.60% |
| Topic 9 | COPD Phenotype and quality of life | 157 | 5.50% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vu, G.V.; Ha, G.H.; Nguyen, C.T.; Vu, G.T.; Pham, H.Q.; Latkin, C.A.; Tran, B.X.; Ho, R.C.M.; Ho, C.S.H. Interventions to Improve the Quality of Life of Patients with Chronic Obstructive Pulmonary Disease: A Global Mapping During 1990–2018. Int. J. Environ. Res. Public Health 2020, 17, 3089. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093089
Vu GV, Ha GH, Nguyen CT, Vu GT, Pham HQ, Latkin CA, Tran BX, Ho RCM, Ho CSH. Interventions to Improve the Quality of Life of Patients with Chronic Obstructive Pulmonary Disease: A Global Mapping During 1990–2018. International Journal of Environmental Research and Public Health. 2020; 17(9):3089. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093089
Chicago/Turabian StyleVu, Giap Van, Giang Hai Ha, Cuong Tat Nguyen, Giang Thu Vu, Hai Quang Pham, Carl A. Latkin, Bach Xuan Tran, Roger C. M. Ho, and Cyrus S. H. Ho. 2020. "Interventions to Improve the Quality of Life of Patients with Chronic Obstructive Pulmonary Disease: A Global Mapping During 1990–2018" International Journal of Environmental Research and Public Health 17, no. 9: 3089. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093089