The Roma Population Living in Segregated Settlements in Eastern Slovakia Has a Higher Prevalence of Metabolic Syndrome, Kidney Disease, Viral Hepatitis B and E, and Some Parasitic Diseases Compared to the Majority Population

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
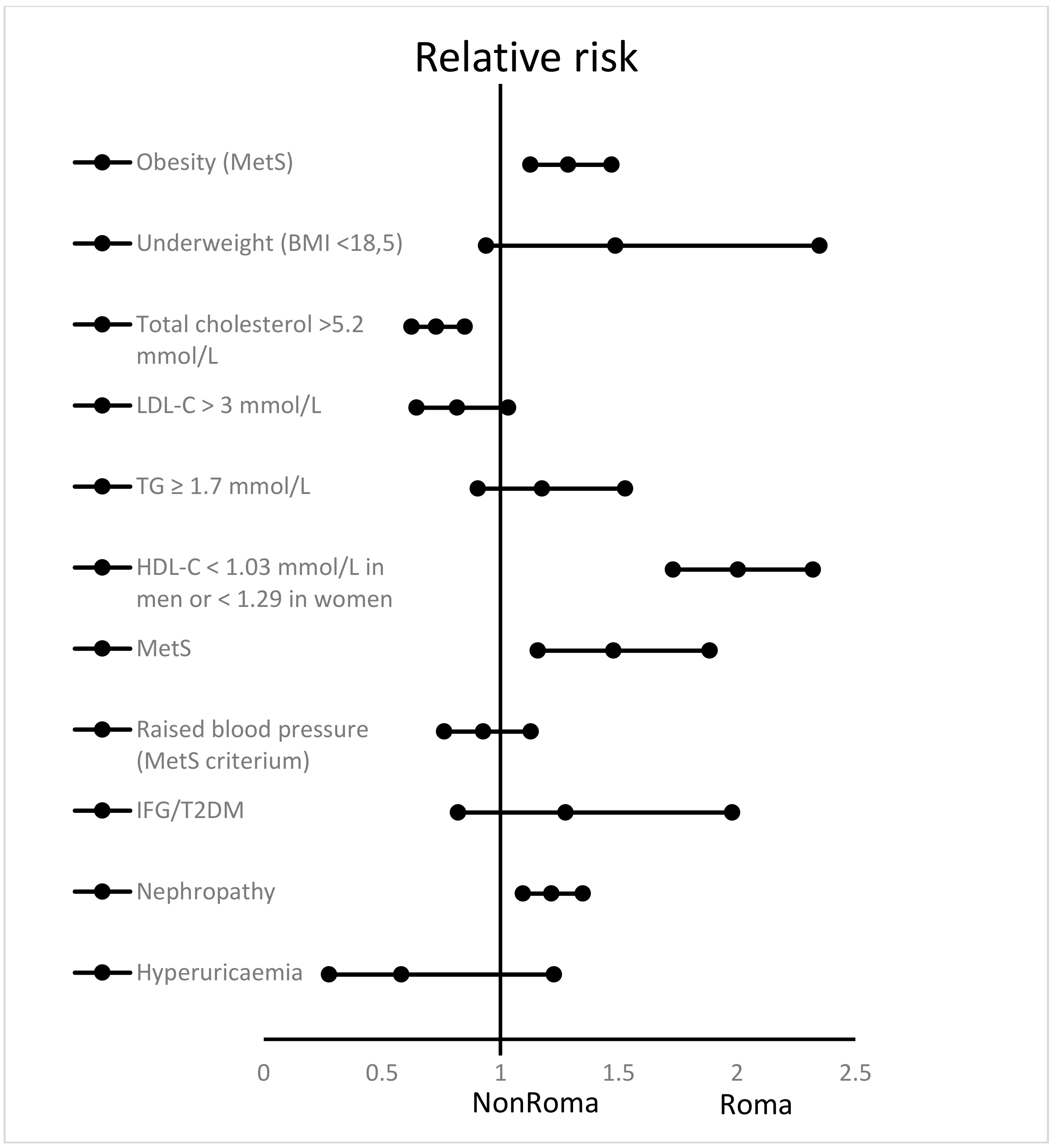
- A raised level of triglycerides (TG) ≥ 150 mg/dL (1.7 mmol/L), or specific treatment for this lipid abnormality.
- A reduced level of high-density lipoprotein cholesterol (HDL-C) < 40 mg/dL (1.03 mmol/L) in males, <50 mg/dL (1.29 mmol/L) in females, or specific treatment for this lipid abnormality.
- Elevated blood pressure, systolic ≥ 130 or diastolic ≥ 85 mmHg, or treatment of previously diagnosed hypertension.
- A raised fasting plasma glucose ≥ 100 mg/dL (5.6 mmol/L), or previously diagnosed type 2 diabetes mellitus (T2DM) [10].
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Sedlakova, D. Low socioeconomic status and unhealthy lifestyle lead to high morbidity in young Roma of East Slovakia. Cent. Eur. J. Public Health 2014, 22, S3–S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geckova, A.M.; Jarcuska, P.; Marekova, M.; Pella, D.; Siegfried, L.; Jarcuska, P.; Halanova, M.; HepaMeta, T. Hepameta—Prevalence of hepatitis B/C and metabolic syndrome in population living in separated and segregated Roma settlements: A methodology for a cross-sectional population-based study using community-based approach. Cent. Eur. J. Public Health 2014, 22, S6–S11. [Google Scholar] [PubMed]
- Geckova, A.M.; Babinska, I.; Bobakova, D.; Veselska, Z.D.; Bosakova, L.; Kolarcik, P.; Jarcuska, P.; Pella, D.; Halanova, M.; HepaMeta, T. Socioeconomic characteristics of the population living in Roma settlements and their association with health and health-related behaviour. Cent. Eur. J. Public Health 2014, 22, S57–S64. [Google Scholar] [PubMed] [Green Version]
- Jarcuska, P.; Bobakova, D.; Uhrin, J.; Bobak, L.; Babinska, I.; Kolarcik, P.; Veselska, Z.; Madarasova Geckova, A.; HEPA-META team. Are barriers in accessing health services in the Roma population associated with worse health status among Roma? Int. J. Public Health 2013, 58, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolak, F.; Sedova, L.; Novakova, D.; Olisarova, V. Approach to prevention of obesity of Roma population in the Region of South Bohemia with focus on selected eating behaviors. Neuro Endocrinol. Lett. 2016, 37, 46–51. [Google Scholar] [PubMed]
- Hajioff, S. The health of the Roma people: A review of the published literature. J. Epidemiol. Community Health 2000, 54, 864–869. [Google Scholar]
- Parekh, N.; Rose, T. Health inequalities of the Roma in Europe: A literature review. Cent. Eur. J. Public Health 2011, 19, 139–142. [Google Scholar]
- Pasco, J.A.; Holloway, K.L.; Dobbins, A.G.; Kotowicz, M.A.; Williams, L.J.; Brennan, S.L. Body mass index and measures of body fat for defining obesity and underweight: A cross-sectional, population-based study. BMC Obes. 2014, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. Obesity Management Task Force of the European Association for the Study of, O. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; Group, I.D.F.E.T.F.C. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar]
- Menon, V.; Kopple, J.D.; Wang, X.; Beck, G.J.; Collins, A.J.; Kusek, J.W.; Greene, T.; Levey, A.S.; Sarnak, M.J. Effect of a very low-protein diet on outcomes: Long-term follow-up of the Modification of Diet in Renal Disease (MDRD) Study. Am. J. Kidney Dis. 2009, 53, 208–217. [Google Scholar] [PubMed] [Green Version]
- Drazilova, S.; Janicko, M.; Kristian, P.; Schreter, I.; Halanova, M.; Urbancikova, I.; Madarasova-Geckova, A.; Marekova, M.; Pella, D.; Jarcuska, P.; et al. Prevalence and Risk Factors for Hepatitis B Virus Infection in Roma and Non-Roma People in Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 1047. [Google Scholar]
- Halanova, M.; Veseliny, E.; Kalinova, Z.; Jarcuska, P.; Janicko, M.; Urbancikova, I.; Pella, D.; Drazilova, S.; Babinska, I.; HepaMeta, T. Seroprevalence of Hepatitis E Virus in Roma Settlements: A Comparison with the General Population in Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 904. [Google Scholar] [CrossRef] [Green Version]
- Halanova, M.; Jarcuska, P.; Kalinova, Z.; Carikova, K.; Oravcova, J.; Jarcuska, P.; Pella, D.; Marekova, M.; Geckova, A.M.; Cislakova, L.; et al. The prevalence of Chlamydia trachomatis in the population living in Roma settlements: A comparison with the majority population. Cent. Eur. J. Public Health 2014, 22, S32–S36. [Google Scholar]
- Antolova, D.; Halanova, M.; Janicko, M.; Jarcuska, P.; Reiterova, K.; Jarosova, J.; Madarasova Geckova, A.; Pella, D.; Drazilova, S.; HepaMeta, T. A Community-Based Study to Estimate the Seroprevalence of Trichinellosis and Echinococcosis in the Roma and Non-Roma Population of Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 251. [Google Scholar] [CrossRef] [Green Version]
- Antolova, D.; Janicko, M.; Halanova, M.; Jarcuska, P.; Geckova, A.M.; Babinska, I.; Kalinova, Z.; Pella, D.; Marekova, M.; Veseliny, E.; et al. Exposure to Toxoplasma gondii in the Roma and Non-Roma Inhabitants of Slovakia: A Cross-Sectional Seroprevalence Study. Int. J. Environ. Res. Public Health 2018, 15, 408. [Google Scholar] [CrossRef] [Green Version]
- Antolova, D.; Jarcuska, P.; Janicko, M.; Madarasova-Geckova, A.; Halanova, M.; Cislakova, L.; Kalinova, Z.; Reiterova, K.; Skutova, M.; Pella, D.; et al. Seroprevalence of human Toxocara infections in the Roma and non-Roma populations of Eastern Slovakia: A cross-sectional study. Epidemiol. Infect. 2015, 143, 2249–2258. [Google Scholar]
- Rosenberger, J.; Majernikova, M.; Jarcuska, P.; Pella, D.; Marekova, M.; Geckova, A.M.; Halanova, M.; HepaMeta, T. Higher prevalence of nephropathy in young Roma females compared with non-Roma females. Cent. Eur. J. Public Health 2014, 22, S28–S31. [Google Scholar]
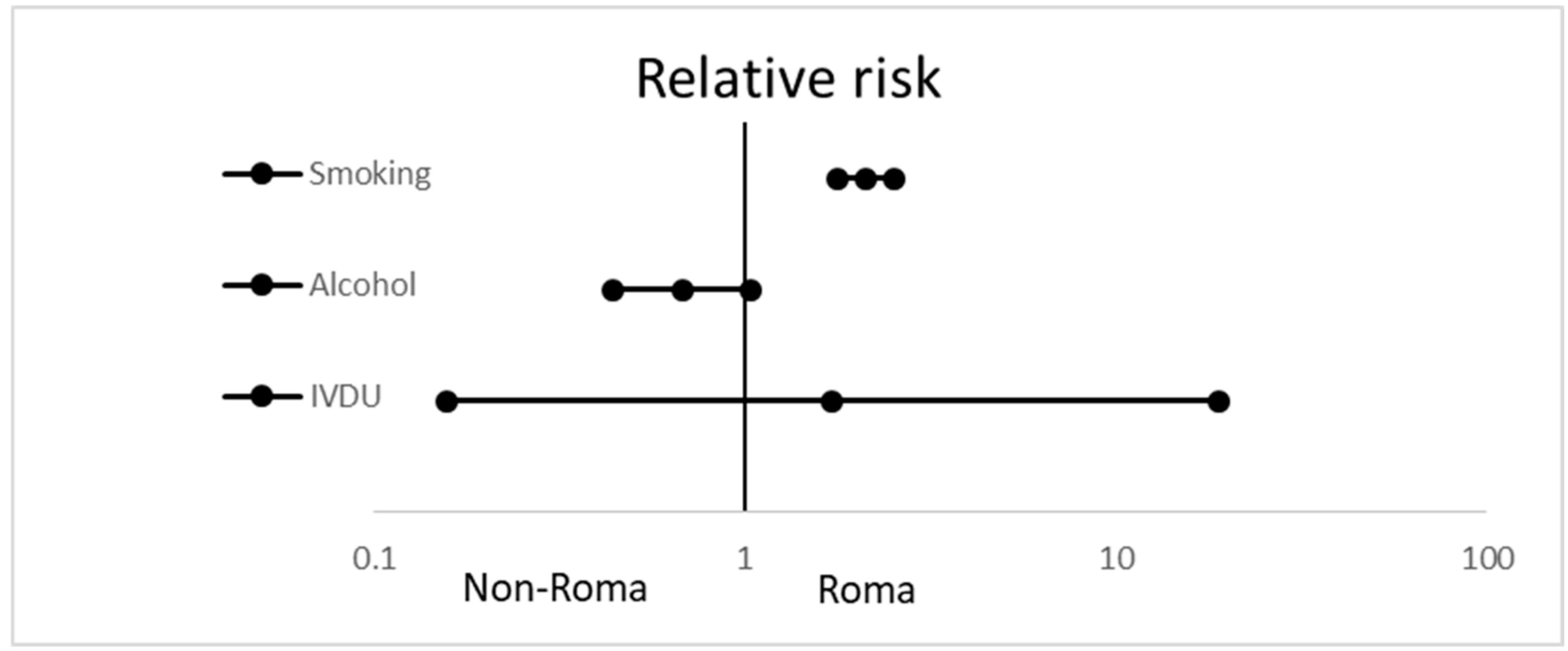
- Babinska, I.; Geckova, A.M.; Jarcuska, P.; Pella, D.; Marekova, M.; Stefkova, G.; Veselska, Z.D.; HepaMeta, T. Does the population living in Roma settlements differ in physical activity, smoking and alcohol consumption from the majority population in Slovakia? Cent. Eur. J. Public Health 2014, 22, S22–S27. [Google Scholar]
- Hijova, E.; Geckova, A.M.; Babinska, I.; HepaMeta, T. Do eating habits of the population living in Roma settlements differ from those of the majority population in Slovakia? Cent. Eur. J. Public Health 2014, 22, S65–S68. [Google Scholar]
- Olisarova, V.; Tothova, V.; Bartlova, S.; Dolak, F.; Kajanova, A.; Novakova, D.; Prokesova, R.; Sedova, L. Cultural Features Influencing Eating, Overweight, and Obesity in the Roma People of South Bohemia. Nutrients 2018, 10, 838. [Google Scholar]
- Sedova, L.; Tothova, V.; Novakova, D.; Olisarova, V.; Bartlova, S.; Dolak, F.; Kajanova, A.; Prokesova, R.; Adamkova, V. Qualification of Food Intake by the Roma Population in the Region of South Bohemia. Int. J. Environ. Res. Public Health 2018, 15, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tothova, V.; Bartlova, S.; Sedova, L.; Olisarova, V.; Prokesova, R.; Adamkova, V.; Mauritzova, I.; Treslova, M.; Chloubova, I.; Miksova, Z. The importance of self-management in the prevention and treatment of excessive weight and obesity. Neuro Endocrinol. Lett. 2015, 36, 5–10. [Google Scholar]
- Adamkova, V.; Hubacek, J.A.; Novakova, D.; Dolak, F.; Adamek, V.; Lanska, V.; Tothova, V.; Sedova, L. Genetic and biochemical characteristics in the Roma minority in the South Bohemia Region. Neuro Endocrinol. Lett. 2015, 36, 29–34. [Google Scholar]
- Nagy, K.; Fiatal, S.; Sandor, J.; Adany, R. Distinct Penetrance of Obesity-Associated Susceptibility Alleles in the Hungarian General and Roma Populations. Obes. Facts 2017, 10, 444–457. [Google Scholar]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Genetic factors exist behind the high prevalence of reduced high-density lipoprotein cholesterol levels in the Roma population. Atherosclerosis 2017, 263, 119–126. [Google Scholar]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Data to genetic risk assessment on high-density cholesterol level associated polymorphisms in Hungarian general and Roma populations. Data Brief 2017, 14, 354–359. [Google Scholar] [CrossRef]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Generalizability and applicability of results obtained from populations of European descent regarding the effect direction and size of HDL-C level-associated genetic variants to the Hungarian general and Roma populations. Gene 2019, 686, 187–193. [Google Scholar]
- Piko, P.; Fiatal, S.; Werissa, N.A.; Bekele, B.B.; Racz, G.; Kosa, Z.; Sandor, J.; Adany, R. The Effect of Haplotypes in the CETP and LIPC Genes on the Triglycerides to HDL-C Ratio and Its Components in the Roma and Hungarian General Populations. Genes 2020, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Werissa, N.A.; Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. SNP-Based Genetic Risk Score Modeling Suggests No Increased Genetic Susceptibility of the Roma Population to Type 2 Diabetes Mellitus. Genes 2019, 10, 942. [Google Scholar] [CrossRef] [Green Version]
- Petrikova, J.; Janicko, M.; Fedacko, J.; Drazilova, S.; Madarasova Geckova, A.; Marekova, M.; Pella, D.; Jarcuska, P. Serum Uric Acid in Roma and Non-Roma-Its Correlation with Metabolic Syndrome and Other Variables. Int. J. Environ. Res. Public Health 2018, 15, 1412. [Google Scholar] [CrossRef] [Green Version]
- Fedacko, J.; Pella, D.; Jarcuska, P.; Siegfried, L.; Janicko, M.; Veseliny, E.; Sabol, F.; Jarcuska, P.; Marekova, M.; Geckova, A.M.; et al. Clinical and biochemical determinants of metabolic syndrome among Roma and non-Roma subjects in the eastern part of Slovakia. Cent. Eur. J. Public Health 2014, 22, S75–S80. [Google Scholar] [PubMed] [Green Version]
- Jarcuska, P.; Janicko, M.; Drazilova, S.; Senajova, G.; Veseliny, E.; Fedacko, J.; Siegfried, L.; Kristian, P.; Tkac, M., Jr.; Pella, D.; et al. Gamma-glutamyl transpeptidase level associated with metabolic syndrome and proinflammatory parameters in the young Roma population in eastern Slovakia: A population-based study. Cent. Eur. J. Public Health 2014, 22, S43–S50. [Google Scholar] [PubMed] [Green Version]
- Babinska, I.; Veselska, Z.D.; Bobakova, D.; Pella, D.; Panico, S.; Reijneveld, S.A.; Jarcuska, P.; Jarcuska, P.; Zezula, I.; Geckova, A.M.; et al. Is the cardiovascular risk profile of people living in Roma settlements worse in comparison with the majority population in Slovakia? Int. J. Public Health 2013, 58, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Usera-Clavero, M.; La Parra-Casado, D.; Caballero, P.; Vives-Cases, C.; Gil-Gonzalez, D. Smoking Prevalence Inequalities Among Roma and Non-Roma Population in Spain Between 2006 and 2014. J. Immigr. Minor. Health 2019, 21, 1282–1289. [Google Scholar]
- Fiatal, S.; Toth, R.; Moravcsik-Kornyicki, A.; Kosa, Z.; Sandor, J.; McKee, M.; Adany, R. High Prevalence of Smoking in the Roma Population Seems to Have No Genetic Background. Nicotine Tob. Res. 2016, 18, 2260–2267. [Google Scholar]
- Dobranici, M.; Buzea, A.; Popescu, R. The cardiovascular risk factors of the Roma (Gypsies) people in Central-Eastern Europe: A review of the published literature. J. Med. Life 2012, 5, 382–389. [Google Scholar]
- Weiss, E.; Japie, C.; Balahura, A.M.; Bartos, D.; Badila, E. Cardiovascular risk factors in a Roma sample population from Romania. Rom. J. Intern. Med. 2018, 56, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Kolvek, G.; Podracka, L.; Rosenberger, J.; Stewart, R.E.; van Dijk, J.P.; Reijneveld, S.A. Kidney diseases in Roma and non-Roma children from eastern Slovakia: Are Roma children more at risk? Int. J. Public Health 2014, 59, 1023–1026. [Google Scholar]
- Kolvek, G.; Rosicova, K.; Rosenberger, J.; Podracka, L.; Stewart, R.E.; Nagyova, I.; Reijneveld, S.A.; van Dijk, J.P. End-stage renal disease among Roma and non-Roma: Roma are at risk. Int. J. Public Health 2012, 57, 751–754. [Google Scholar]
- Basic-Jukic, N.; Novosel, D.; Juric, I.; Kes, P. Renal transplantation in the Roma ethnicity-do all patients have equal chance for transplantation? Transplant. Proc. 2013, 45, 3190–3191. [Google Scholar] [PubMed]
- Molnar, M.Z.; Langer, R.M.; Remport, A.; Czira, M.E.; Rajczy, K.; Kalantar-Zadeh, K.; Kovesdy, C.P.; Novak, M.; Mucsi, I.; Rosivall, L. Roma ethnicity and clinical outcomes in kidney transplant recipients. Int. Urol. Nephrol. 2012, 44, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Ferak, V.; Sivakova, D.; Sieglova, Z. [The Slovak Gypsies (Romany)—A population with the highest coefficient of inbreeding in Europe]. Bratisl. Lek. Listy 1987, 87, 168–175. [Google Scholar] [PubMed]
- Kalaydjieva, L.; Gresham, D.; Calafell, F. Genetic studies of the Roma (Gypsies): A review. BMC Med. Genet. 2001, 2, 5. [Google Scholar]
- Dluholucký, S.; Knapková, M. The First Results of Extended Newborn Screening in Slovakia—Differences between the Majority and the Roma Ethnic Group. Int. J. Neonatal Screen. 2017, 3, 25. [Google Scholar] [CrossRef] [Green Version]
- Gencikova, A.; Gencik, A. Congenital glaucoma in Gypsies from Slovakia. Hum. Hered. 1982, 32, 270–273. [Google Scholar]
- Lisyová, J.; Chandoga, J.; Jungová, P.; Repiský, M.; Knapková, M.; Machková, M.; Dluholucký, S.; Behúlová, D.; Šaligová, J.; Potočňáková, Ľ.; et al. An unusually high frequency of SCAD deficiency caused by two pathogenic variants in the ACADS gene and its relationship to the ethnic structure in Slovakia. BMC Med. Genet. 2018, 19. [Google Scholar] [CrossRef] [Green Version]
- Gregory, A.; Vedio, A.; Stone, B.; Green, S.; Bronsdon, C. Targeted testing in primary care demonstrates high prevalence of hepatitis B infection within the Slovak-Roma population in Sheffield, UK. J. Viral Hepat. 2014, 21, e138–e139. [Google Scholar]
- Michos, A.; Terzidis, A.; Kalampoki, V.; Pantelakis, K.; Spanos, T.; Petridou, E.T. Seroprevalence and risk factors for hepatitis A, B, and C among Roma and non-Roma children in a deprived area of Athens, Greece. J. Med. Virol. 2008, 80, 791–797. [Google Scholar]
- Virto Ruiz, M.T.; Marin Alcala, M.P.; Pascual Val, T.; Lopez Morras, C.; Aramburu Bergua, I.; Zubicoa Ventura, J. [Endemic hepatitis B in 2 marginal ethnic minorities. Comparative study]. Med. Clin. (Barc.) 1993, 101, 245–248. [Google Scholar]
- Do, S. The natural history of hepatitis B in Asian Americans. Asian Am. Pac. Isl. J. Health 2001, 9, 141–153. [Google Scholar] [PubMed]
- Veseliny, E.; Janicko, M.; Drazilova, S.; Siegfried, L.; Pastvova, L.; Schreter, I.; Kristian, P.; Viag, L.; Jarcuska, P.; Valkova, I.; et al. High hepatitis B and low hepatitis C prevalence in Roma population in eastern Slovakia. Cent. Eur. J. Public Health 2014, 22 Suppl, S51–S56. [Google Scholar]
- Kristian, P.; Veselska, Z.D.; Paralicova, Z.; Jarcuska, P.; Virag, L.; Valkova, I.; Schreter, I. Regional and ethnic aspects of viral hepatitis B among pregnant women. Cent. Eur. J. Public Health 2013, 21, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Drazilova, S.; Janicko, M.; Kristian, P.; Schreter, I.; Kucinsky, B.; Kozlej, M.; Hockickova, I.; Jarcuska, P. Lower Viral Response to Pegylated Interferon Alpha 2a Treatment of Chronic Hepatitis B in Roma People in Eastern Slovakia. Gastroenterol. Res. Pract. 2016, 2016, 6. [Google Scholar] [PubMed] [Green Version]
- Vechetova, S.; Krekulova, L.; Oktabec, Z.; Rehak, V. A high prevalence of viral hepatitis C in a socially excluded Roma community in Brno. Epidemiol. Mikrobiol. Imunol. 2019, 68, 115–121. [Google Scholar] [PubMed]
- Simko, V.; Ginter, E. Short life expectancy and metabolic syndrome in Romanies (Gypsies) in Slovakia. Cent. Eur. J. Public Health 2010, 18, 16–18. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluated Variable | Roma | Non-Roma | p |
|---|---|---|---|
| Total number | 452 | 403 | |
| Male sex | 159 (35.2%) | 185 (45.9%) | 0.001 |
| Education primary | 360 (81.3%) | 9 (2.3%) | <0.0001 |
| Education vocational | 73 (16.5%) | 84 (21.4%) | |
| Education higher | 10 (2.3%) | 300 (76.3%) | |
| Unemployment | 396 (89.6%) | 102 (26.4%) | <0.0001 |
| Lack of household equipment * | 281 (62.2%) | 78 (19.4%) | <0.0001 |
| Payment problems ** | 218 (48.2%) | 49 (12.2%) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macejova, Z.; Kristian, P.; Janicko, M.; Halanova, M.; Drazilova, S.; Antolova, D.; Marekova, M.; Pella, D.; Madarasova-Geckova, A.; Jarcuska, P.; et al. The Roma Population Living in Segregated Settlements in Eastern Slovakia Has a Higher Prevalence of Metabolic Syndrome, Kidney Disease, Viral Hepatitis B and E, and Some Parasitic Diseases Compared to the Majority Population. Int. J. Environ. Res. Public Health 2020, 17, 3112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093112
Macejova Z, Kristian P, Janicko M, Halanova M, Drazilova S, Antolova D, Marekova M, Pella D, Madarasova-Geckova A, Jarcuska P, et al. The Roma Population Living in Segregated Settlements in Eastern Slovakia Has a Higher Prevalence of Metabolic Syndrome, Kidney Disease, Viral Hepatitis B and E, and Some Parasitic Diseases Compared to the Majority Population. International Journal of Environmental Research and Public Health. 2020; 17(9):3112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093112
Chicago/Turabian StyleMacejova, Zelmira, Pavol Kristian, Martin Janicko, Monika Halanova, Sylvia Drazilova, Daniela Antolova, Maria Marekova, Daniel Pella, Andrea Madarasova-Geckova, Peter Jarcuska, and et al. 2020. "The Roma Population Living in Segregated Settlements in Eastern Slovakia Has a Higher Prevalence of Metabolic Syndrome, Kidney Disease, Viral Hepatitis B and E, and Some Parasitic Diseases Compared to the Majority Population" International Journal of Environmental Research and Public Health 17, no. 9: 3112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093112