Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
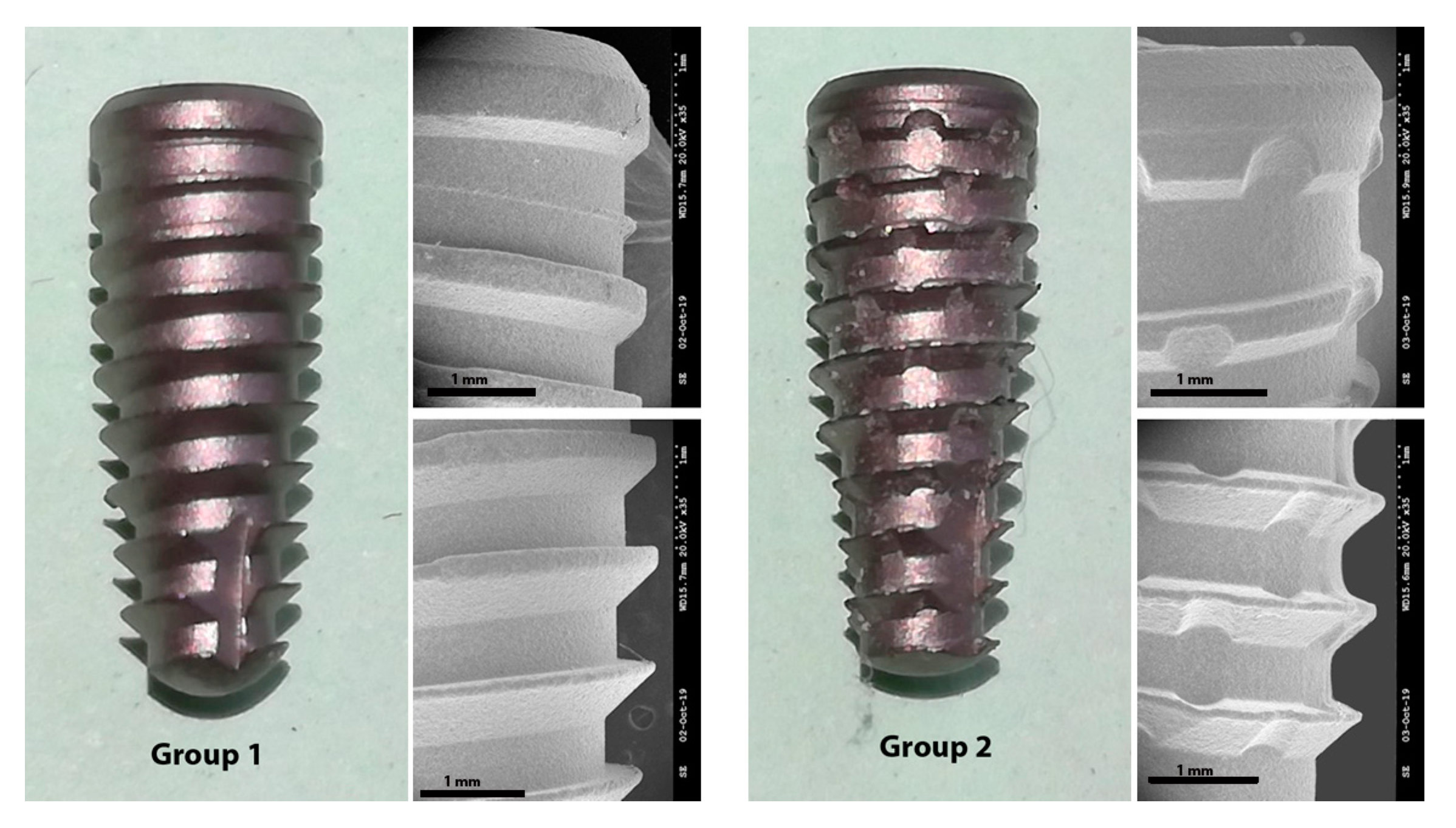
2.1. Implants Preparation and Groups Formation
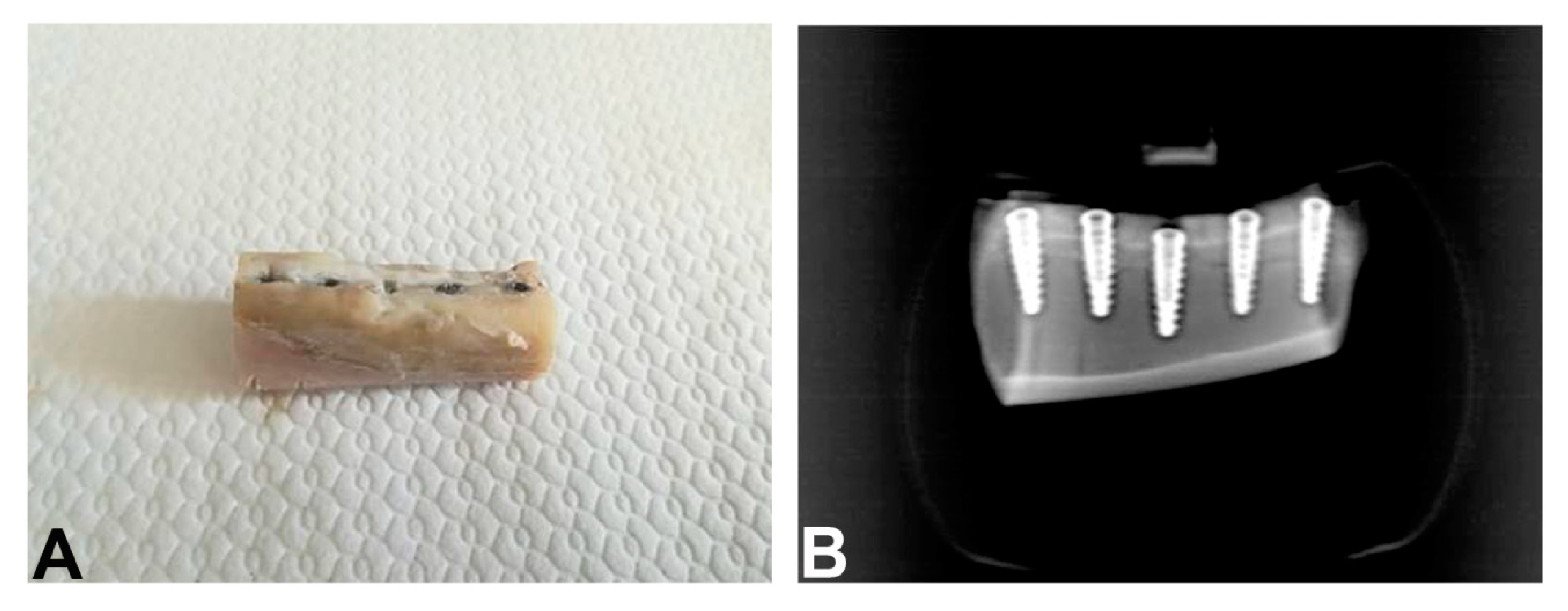
2.2. Animal Experimentation
2.3. Postoperative Care
2.4. Histology
2.5. Statistical Analysis
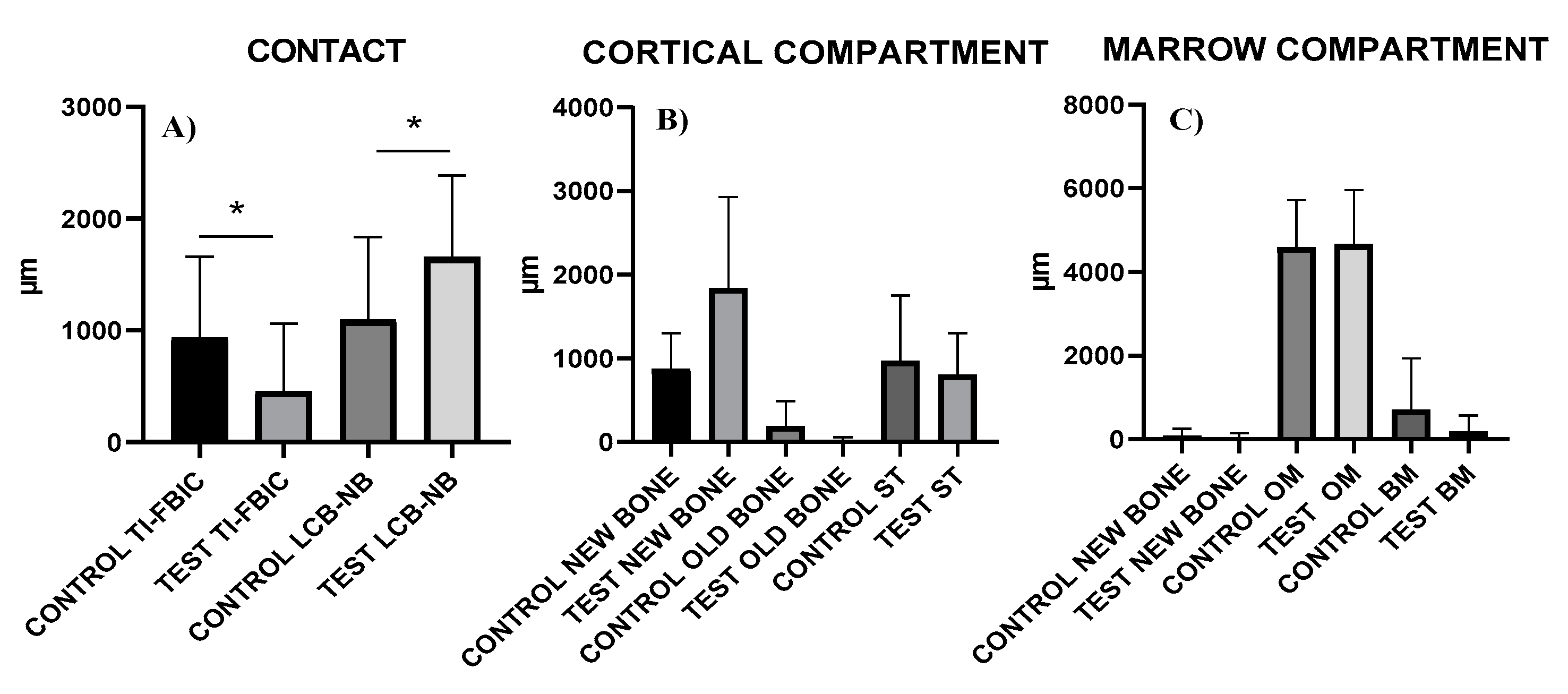
3. Results
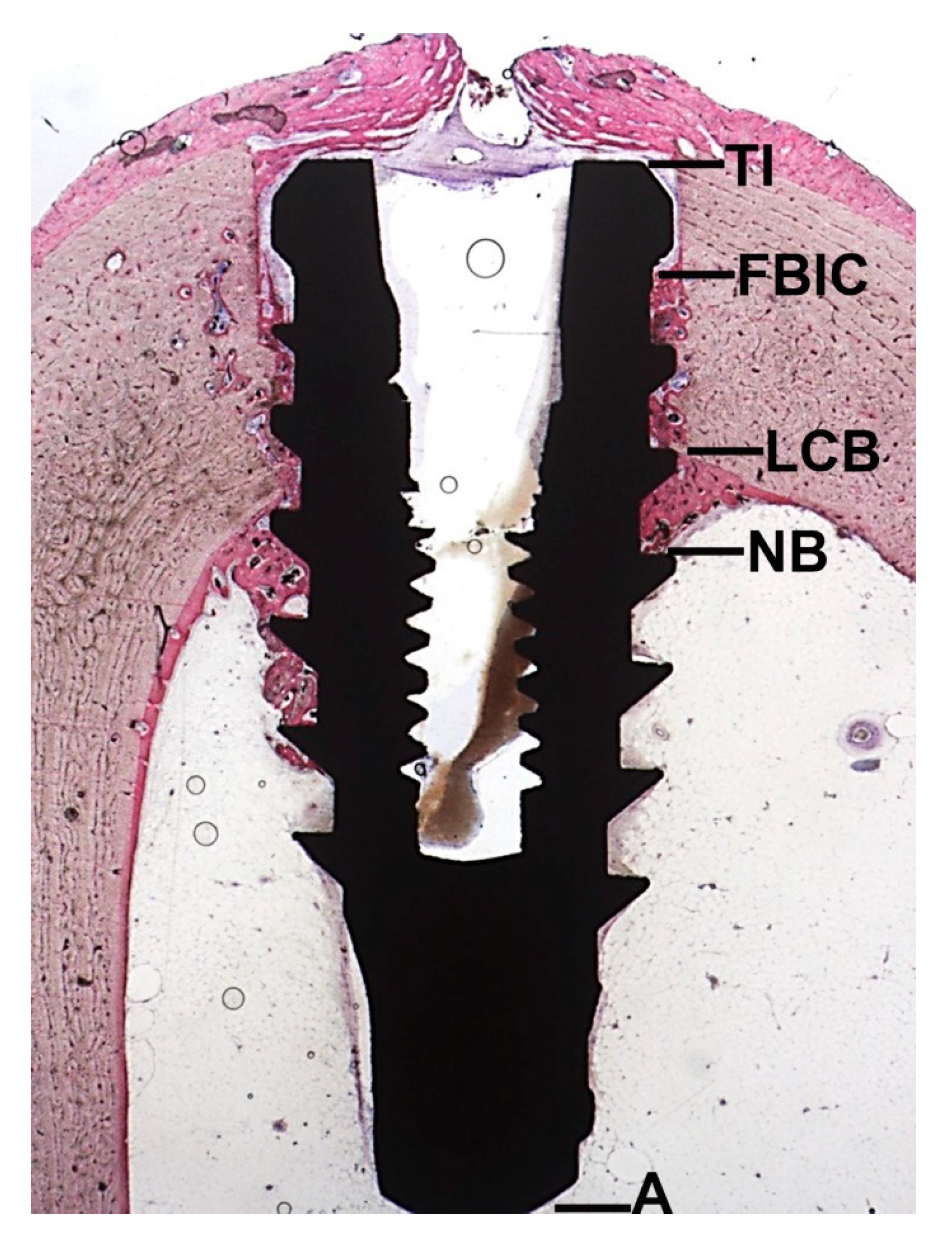
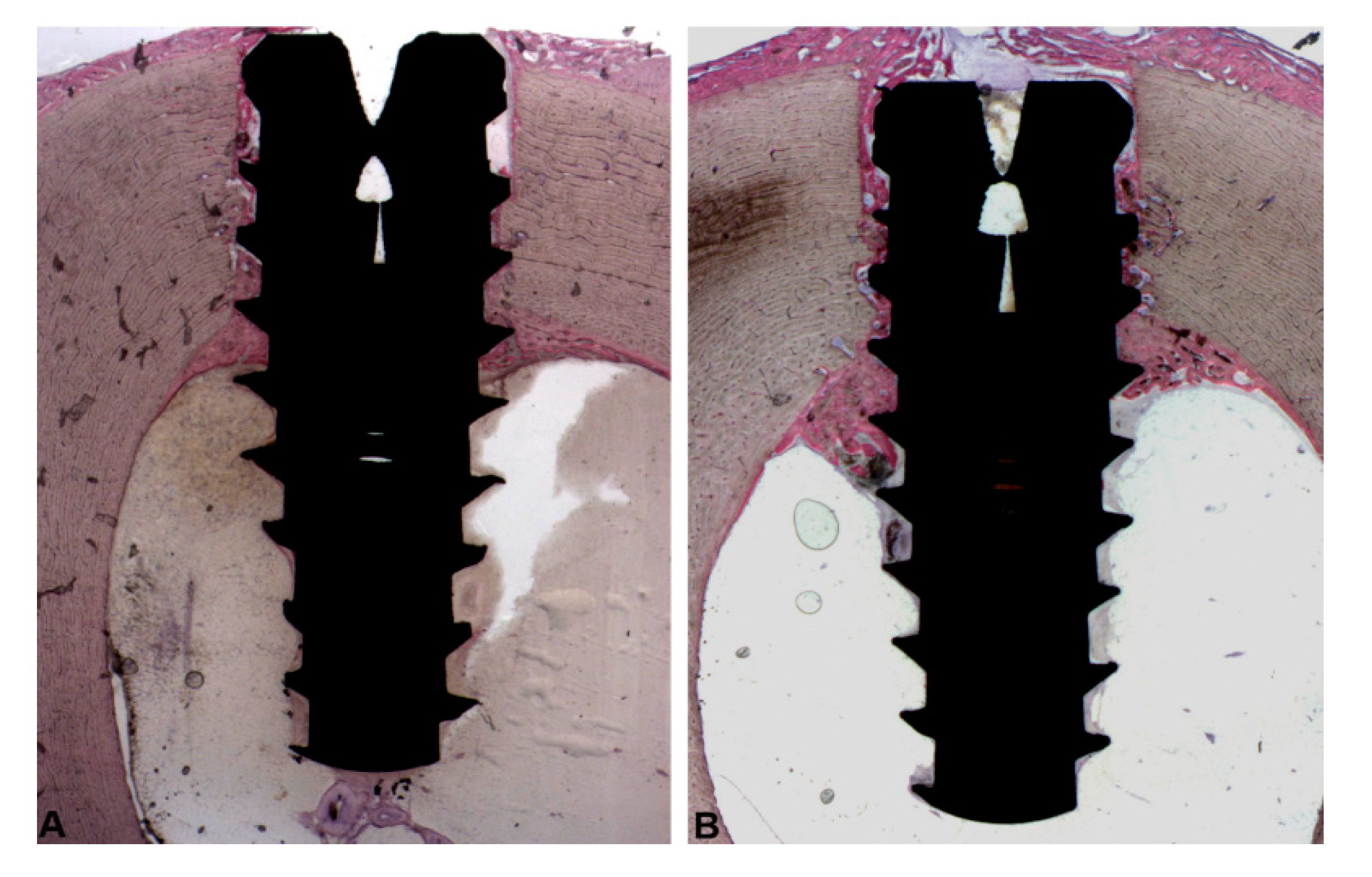
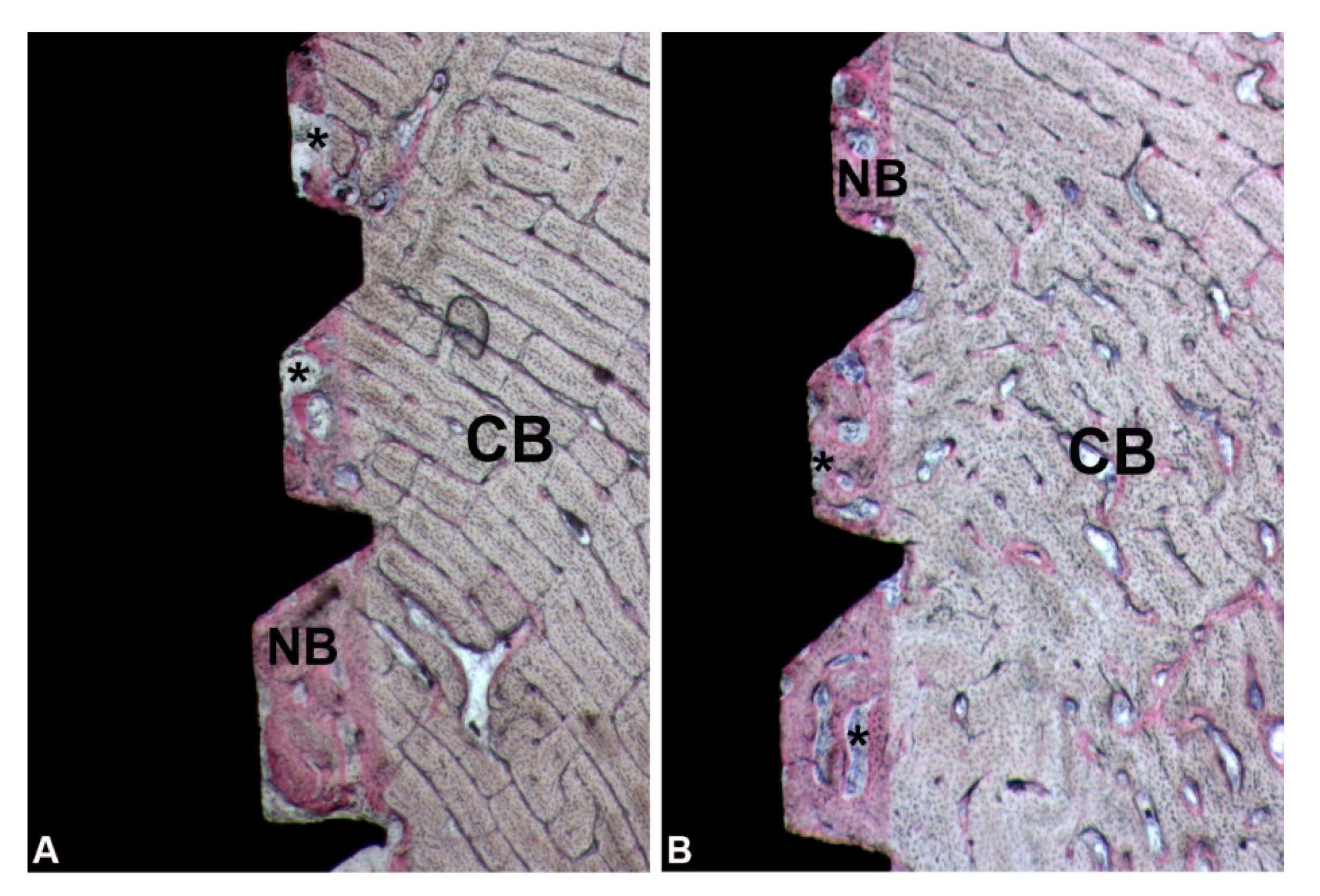
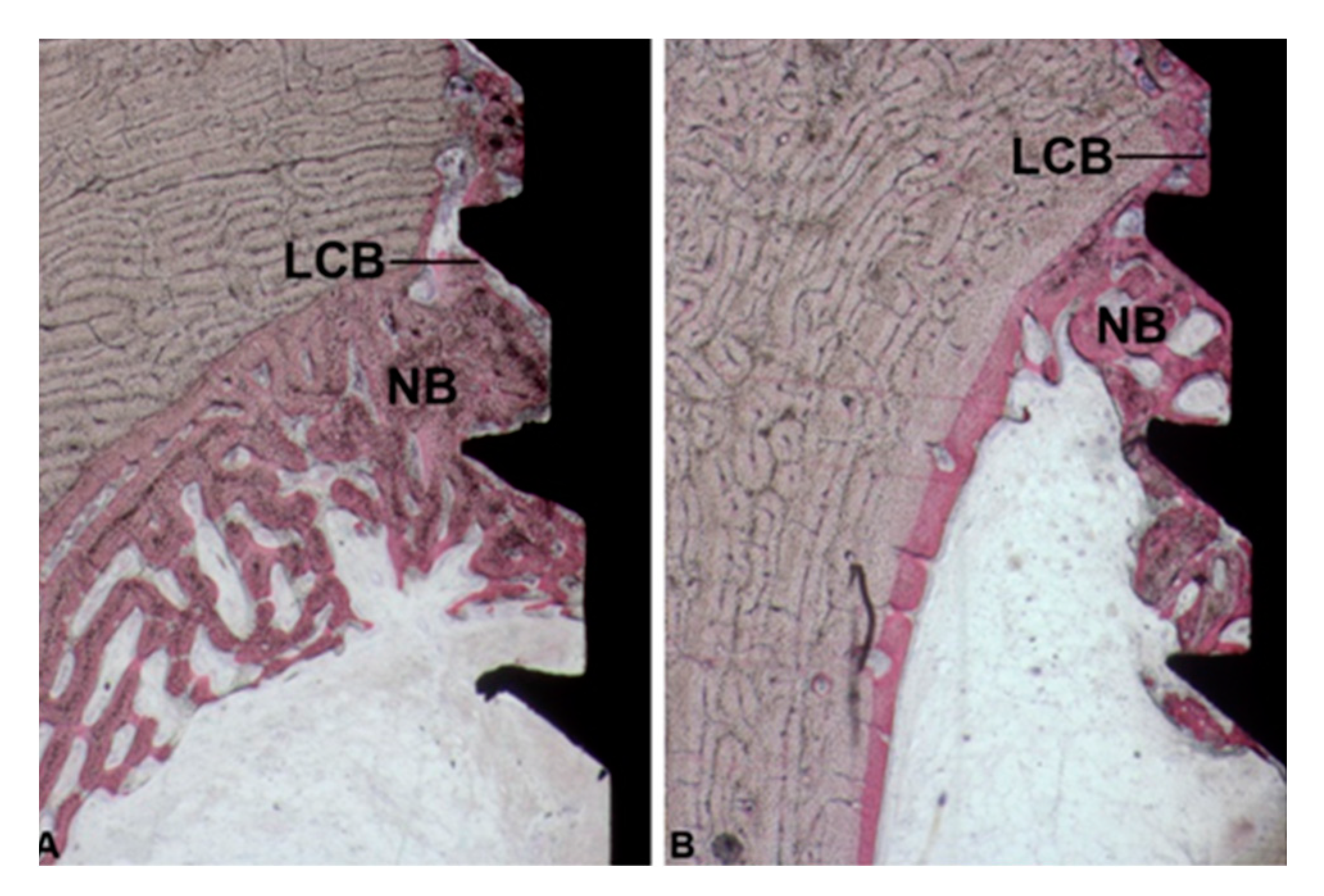
3.1. Cortical Portion
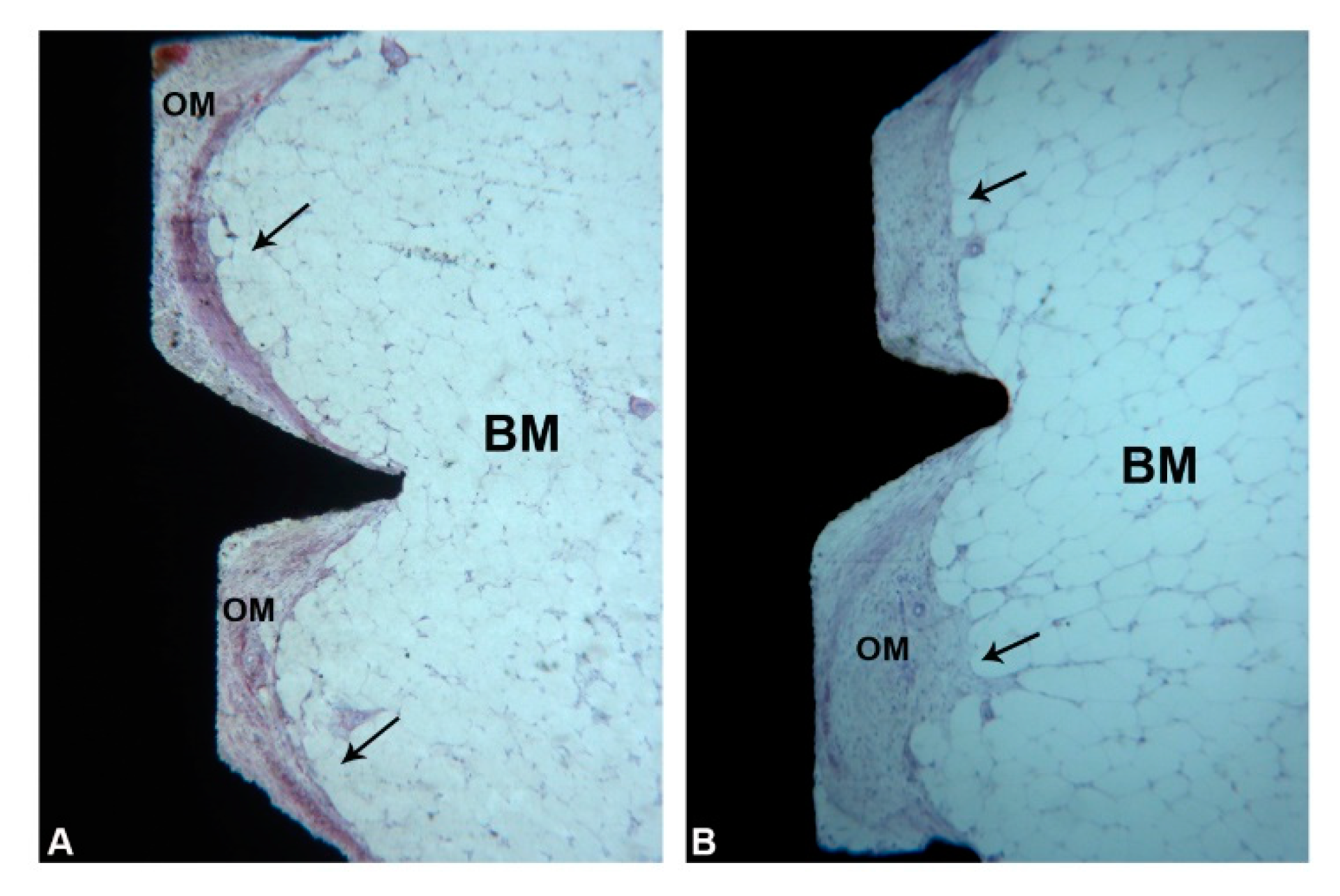
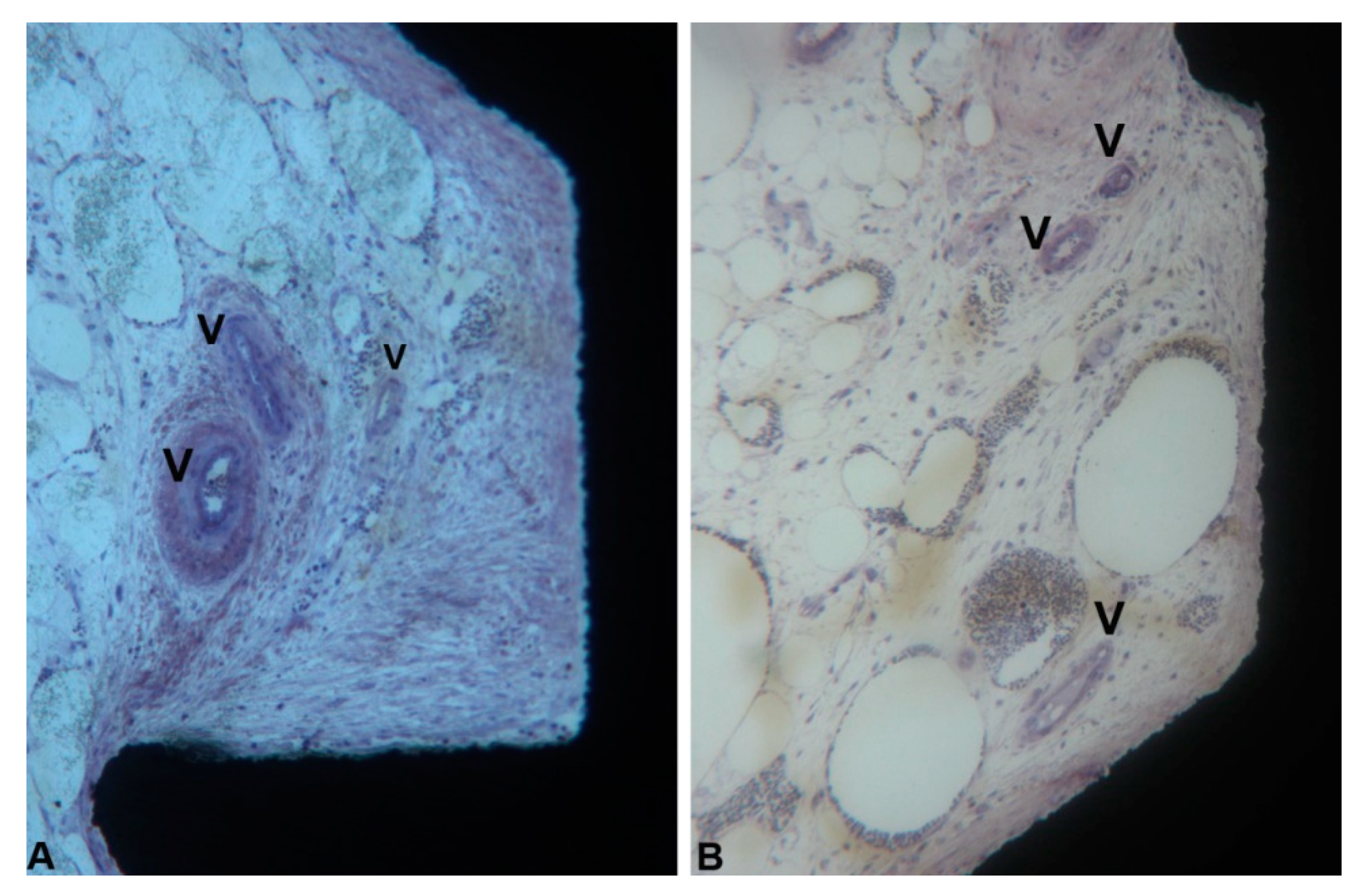
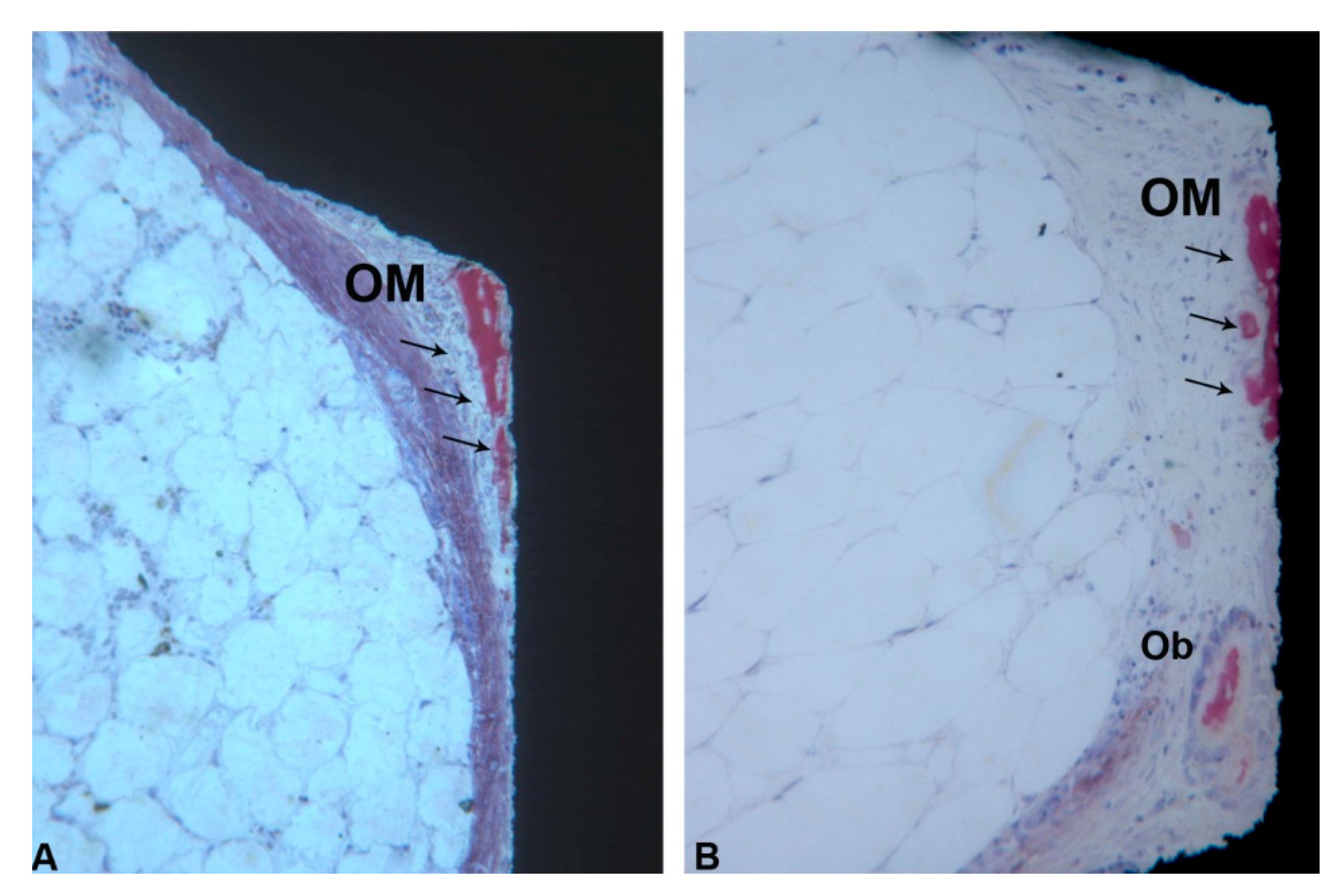
3.2. Marrow Compartment
4. Discussion
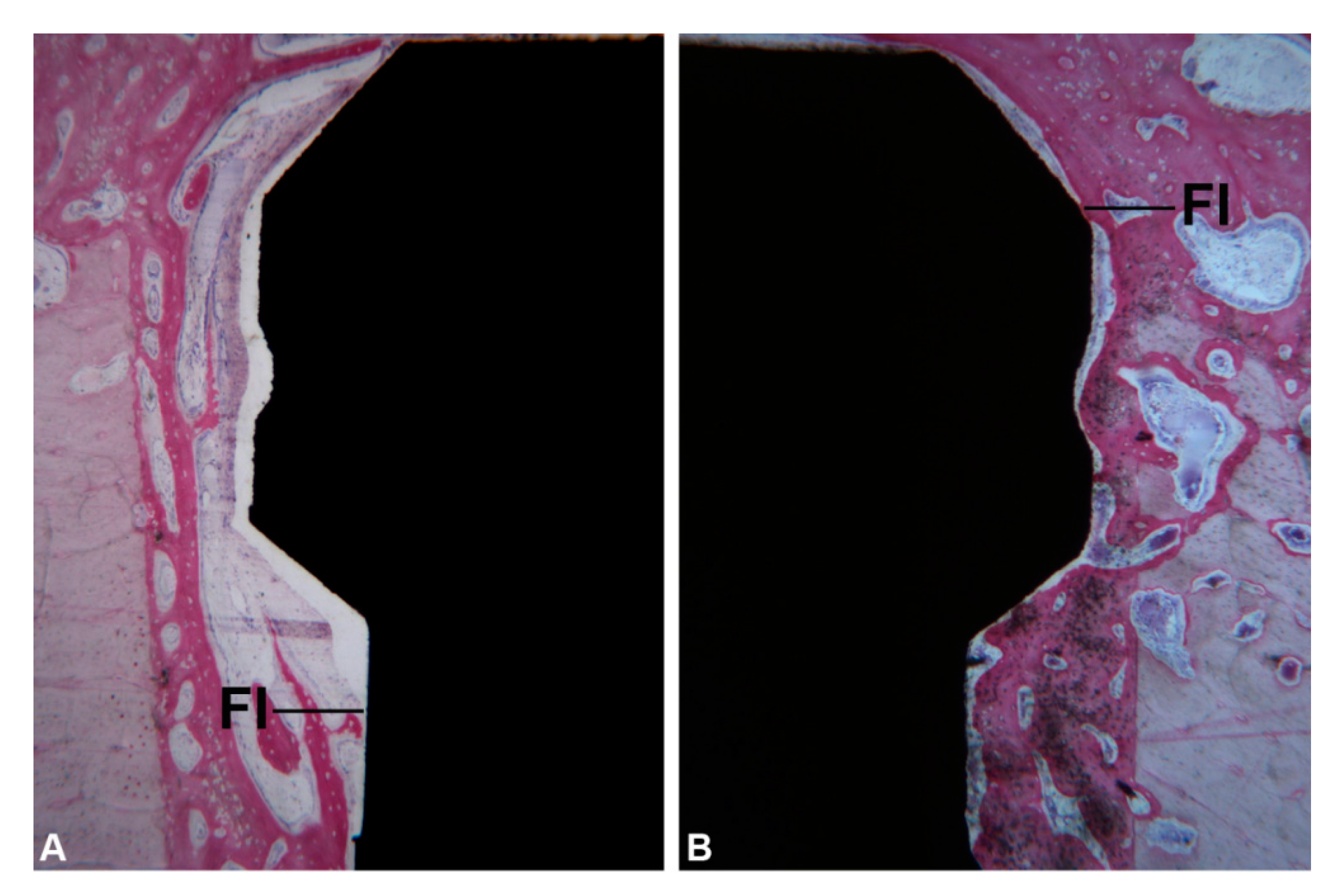
- the statistically significantly higher percentage of newly formed formed bone in the implants where the healing chambers were present.
- a larger area, in the implants provided with healing chambers, of an osteogenic stroma, rich in blood vessels, where small, thin newly-formed bone trabeculae could be found, in close and tight contact with the implant portion immersed in the marrow compartment.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fini, M.; Giavaresi, G.; Torricelli, P.; Borsari, V.; Giardino, R.; Nicolini, A.; Carpi, A. Osteoporosis and biomaterial osteointegration. Biomed. Pharmacother. 2004, 58, 487–493. [Google Scholar] [CrossRef]
- Rigo, E.C.S.; Boschi, A.O.; Yoshimoto, M.; Allegrini, S., Jr.; Konig, B., Jr.; Carbonari, M.J. Evaluation in vitro and in vivo of biomimetic hydroxyapatite coated on titanium dental implants. Mater. Sci. Eng. 2004, 24, 647–651. [Google Scholar] [CrossRef]
- Soballe, K.; Hansen, E.S.; Brockstedt-Rasmussen, H.; Bünger, C. Hydroxyapatite coating converts fibrous tissueto bone around loaded implants. J. Bone Jt. Surg. Br. 1993, 75, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E. Mechanisms of endosseous integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar] [PubMed]
- Cehreli, M.; Duyck, J.; De Cooman, M.; Puers, R.; Naert, I. Implant design and interface force transfer. A photoelastic and strain-gauge analysis. Clin. Oral Implants Res. 2004, 15, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Chieruzzi, M.; Pagano, S.; Cianetti, S.; Lombardo, G.; Kenny, J.M.; Torre, L. Effect of fibre posts, bone losses and fibre content on the biomechanical behaviour of endodontically treated teeth: 3D-finite element analysis. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 74, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Campos, F.E.B.; Jimbo, R.; Bonfante, E.A.; Barbosa, D.Z.; Oliveira, M.T.F.; Janal, M.N.; Coelho, P.G. Are insertion torque and early osseointegration proportional? A histologic evaluation. Clin. Oral Implants Res. 2015, 26, 1256–1260. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Eliers Treichel, T.L.; Pérez-Díaz, L.; Calvo-Guirado, J.L.; Aramburú Júnior, J.; Mazón, P.; de Aza, P.N. Impact of Different Titanium Implant Thread Designs on Bone Healing: A Biomechanical and Histometric Study with an Animal Model. J. Clin. Med. 2019, 8, 777. [Google Scholar] [CrossRef] [Green Version]
- Gehrke, S.A.; Pérez-Díaz, L.; Mazón, P.; De Aza, P.N. Biomechanical Effects of a New Macrogeometry Design of Dental Implants: An In Vitro Experimental Analysis. J. Funct. Biomater. 2019, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- Jimbo, R.; Tovar, N.; Anchieta, R.B.; Machado, L.S.; Marin, C.; Teixeira, H.S.; Coelho, P.G. The combined effects of undersized drilling and implant macrogeometry on bone healing around dental implants: An experimental study. Int. J. Oral Maxillofac. Surg. 2014, 43, 1269–1275. [Google Scholar] [CrossRef]
- Coelho, P.G.; Marin, C.; Granato, R.; Suzuki, M. Histomorphologic analysis of 30 plateau root form implants retrieved after 8 to 13 years in function. A human retrieval study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 91, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Suzuki, M.; Guimaraes, M.V.M.; Marin, C.; Granato, R.; Gil, J.N.; Miller, R.J. Early bone healing around different implant bulk designs and surgical techniques: A study in dogs. Clin. Implant Dent. Relat. Res. 2010, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Marão, H.F.; Jimbo, R.; Neiva, R.; Gil, L.F.; Bowers, M.; Bonfante, E.A.; Tovar, N.; Janal, M.N.; Coelho, P.G. Cortical and Trabecular Bone Healing Patterns and Quantification for Three Different Dental Implant Systems. Int. J. Oral Maxillofac. Implants 2017, 32, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, P.G.; Bonfante, E.A.; Marin, C.; Granato, R.; Giro, G.; Suzuki, M. A human retrieval study of plasma-sprayed hydroxyapatite-coated plateau root form implants after 2 months to 13 years in function. J. Long Term Eff. Med. Implants 2010, 20, 335–342. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Aramburú Júnior, J.; Pérez-Díaz, L.; Treichel, T.L.E.; Dedavid, B.A.; De Aza, P.N.; Prados-Frutos, J.C. New Implant Macrogeometry to Improve and Accelerate the Osseointegration: An In Vivo Experimental Study. Appl. Sci. 2019, 9, 3181. [Google Scholar] [CrossRef] [Green Version]
- Piattelli, A.; Scarano, A.; Quaranta, M. High-precision, cost-effective cutting system for producing thin sections of oral tissues containing dental implants. Biomaterials 1997, 18, 577–579. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R. Osseointegration of metallic devices: Current trends based on implant hardware design. Arch. Biochem. Biophys. 2014, 561, 99–108. [Google Scholar] [CrossRef]
- Meirelles, L.; Brånemark, P.-I.; Albrektsson, T.; Feng, C.; Johansson, C. Histological evaluation of bone formation adjacent to dental implants with a novel apical chamber design: Preliminary data in the rabbit model. Clin. Implant Dent. Relat. Res. 2015, 17, 453–460. [Google Scholar] [CrossRef]
- Ribeiro da Silva, J.; Castellano, A.; Malta Barbosa, J.P.; Gil, L.F.; Marin, C.; Granato, R.; Bonfante, E.A.; Tovar, N.; Janal, M.N.; Coelho, P.G. Histomorphological and Histomorphometric Analyses of Grade IV Commercially Pure Titanium and Grade V Ti-6Al-4V Titanium Alloy Implant Substrates: An In Vivo Study in Dogs. Implant Dent. 2016, 25, 650–655. [Google Scholar] [CrossRef]
- Marin, C.; Granato, R.; Suzuki, M.; Gil, J.N.; Janal, M.N.; Coelho, P.G. Histomorphologic and histomorphometric evaluation of various endosseous implant healing chamber configurations at early implantation times: A study in dogs. Clin. Oral Implants Res. 2010, 21, 577–583. [Google Scholar] [CrossRef]
- Lee, H.-C.; Tsai, P.-I.; Huang, C.-C.; Chen, S.-Y.; Chao, C.-G.; Tsou, N.-T. Numerical Method for the Design of Healing Chamber in Additive-Manufactured Dental Implants. Biomed. Res. Int. 2017, 2017. [Google Scholar] [CrossRef]
- Beutel, B.G.; Danna, N.R.; Granato, R.; Bonfante, E.A.; Marin, C.; Tovar, N.; Suzuki, M.; Coelho, P.G. Implant design and its effects on osseointegration over time within cortical and trabecular bone. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 1091–1097. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Linder, E.; Lang, N.P.; Lindhe, J. Early bone formation adjacent to rough and turned endosseous implant surfaces. An experimental study in the dog. Clin. Oral Implants Res. 2004, 15, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Broggini, N.; Wieland, M.; Schenk, R.K.; Denzer, A.J.; Cochran, D.L.; Hoffmann, B.; Lussi, A.; Steinemann, S.G. Enhanced bone apposition to a chemically modified SLA titanium surface. J. Dent. Res. 2004, 83, 529–533. [Google Scholar] [CrossRef]
- Granato, R.; Marin, C.; Suzuki, M.; Gil, J.N.; Janal, M.N.; Coelho, P.G. Biomechanical and histomorphometric evaluation of a thin ion beam bioceramic deposition on plateau root form implants: An experimental study in dogs. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 90, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Perrotti, V.; Artese, L.; Degidi, M.; Degidi, D.; Piattelli, A.; Iezzi, G. Blood vessels are concentrated within the implant surface concavities: A histologic study in rabbit tibia. Odontology 2014, 102, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Degidi, M.; Perrotti, V.; Degidi, D.; Piattelli, A.; Iezzi, G. Experimental evaluation in rabbits of the effects of thread concavities in bone formation with different titanium implant surfaces. Clin. Implant Dent. Relat. Res. 2014, 16, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Buser, D.; Lindhe, J. The jumping distance revisited: An experimental study in the dog. Clin. Oral Implants Res. 2003, 14, 35–42. [Google Scholar] [CrossRef]
- Favero, V.; Sakuma, S.; Apaza Alccayhuaman, K.A.; Benedetto, G.A.; Bengazi, F.; Botticelli, D. Healing at sites prepared using different drilling protocols. An experimental study in the tibiae of sheep. PLoS ONE 2018, 13, e0202957. [Google Scholar] [CrossRef]
- Gil, L.F.; Suzuki, M.; Janal, M.N.; Tovar, N.; Marin, C.; Granato, R.; Bonfante, E.A.; Jimbo, R.; Gil, J.N.; Coelho, P.G. Progressive plateau root form dental implant osseointegration: A human retrieval study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 103, 1328–1332. [Google Scholar] [CrossRef]
- Bonfante, E.A.; Granato, R.; Marin, C.; Suzuki, M.; Oliveira, S.R.; Giro, G.; Coelho, P.G. Early bone healing and biomechanical fixation of dual acid-etched and as-machined implants with healing chambers: An experimental study in dogs. Int. J. Oral Maxillofac. Implants 2011, 26, 75–82. [Google Scholar] [PubMed]
- Witek, L.; Marin, C.; Granato, R.; Bonfante, E.A.; Campos, F.E.B.; Gomes, J.B.; Suzuki, M.; Coelho, P.G. Surface characterization, biomechanical, and histologic evaluation of alumina and bioactive resorbable blasting textured surfaces in titanium implant healing chambers: An experimental study in dogs. Int. J. Oral Maxillofac. Implants 2013, 28, 694–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, P.G.; Suzuki, M.; Marin, C.; Granato, R.; Gil, L.F.; Tovar, N.; Jimbo, R.; Neiva, R.; Bonfante, E.A. Osseointegration of Plateau Root Form Implants: Unique Healing Pathway Leading to Haversian-Like Long-Term Morphology. Adv. Exp. Med. Biol. 2015, 881, 111–128. [Google Scholar] [PubMed]
- Bertassoni, L.E.; Coelho, P.G. Advances in Experimental Medicine and Biology. In Engineering Mineralized and Load Bearing Tissues; Springer: Berlin, Germany, 2015; Volume 881. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contact (μm) | Control Ti-Fbic | Test Ti-Fbic | Control Lcb-Nb | Test Lcb-Nb |
|---|---|---|---|---|
| Minimum | 0.000 | 0.000 | 0.000 | 537.0 |
| Maximum | 2310 | 2377 | 2640 | 4116 |
| Range | 2310 | 2377 | 2640 | 3579 |
| Mean | 932.0 | 453.3 | 1095 | 1658 |
| Std. Deviation | 729.7 | 605.3 | 743.1 | 727.9 |
| Std. Error of Mean | 155.6 | 114.4 | 158.4 | 137.6 |
| Cortical Compartment (μm) | New Bone | Old Bone | Soft Tissue | |||
|---|---|---|---|---|---|---|
| Control | Test | Control | Test | Control | Test | |
| Minimum | 302,0 | 179.0 | 0.000 | 0.000 | 0.000 | 0.000 |
| Maximum | 1949 | 4857 | 979.1 | 257.3 | 3351 | 1746 |
| Range | 1647 | 4678 | 979.1 | 257.3 | 3351 | 1746 |
| Mean | 873.6 | 1839 | 192.1 | 9.188 | 969.0 | 805.2 |
| Std. Deviation | 428.3 | 1088 | 297.7 | 48.62 | 782.5 | 497.7 |
| Lower 95% CI of mean | 302.0 | 179.0 | 0,000 | 0.000 | 0.000 | 0.000 |
| Upper 95% CI of mean | 1949 | 4857 | 979.1 | 257.3 | 3351 | 1746 |
| Marrow Compartment (μm) | New Bone | Osteogenic Matrix | Bone Marrow | |||
|---|---|---|---|---|---|---|
| Control | Test | Control | Test | Control | Test | |
| Minimum | 0.000 | 0.000 | 1612 | 1458 | 0,000 | 0.000 |
| Maximum | 715.9 | 316.4 | 6557 | 6823 | 4926 | 1588 |
| Range | 715.9 | 316.4 | 4944 | 5366 | 4926 | 1588 |
| Mean | 74.55 | 42.92 | 4587 | 4660 | 700,1 | 187.0 |
| Std. Deviation | 177.4 | 97.53 | 1132 | 1294 | 1233 | 375.7 |
| Lower 95% CI of mean | −4.108 | 5.100 | 4085 | 4158 | 153,4 | 41.30 |
| Upper 95% CI of mean | 153.2 | 80.74 | 5089 | 5162 | 1247 | 332.6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gehrke, S.A.; Tumedei, M.; Aramburú Júnior, J.; Treichel, T.L.E.; Kolerman, R.; Lepore, S.; Piattelli, A.; Iezzi, G. Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study. Int. J. Environ. Res. Public Health 2020, 17, 3477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103477
Gehrke SA, Tumedei M, Aramburú Júnior J, Treichel TLE, Kolerman R, Lepore S, Piattelli A, Iezzi G. Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103477
Chicago/Turabian StyleGehrke, Sergio Alexandre, Margherita Tumedei, Jaime Aramburú Júnior, Tiago Luis Eirles Treichel, Roni Kolerman, Stefania Lepore, Adriano Piattelli, and Giovanna Iezzi. 2020. "Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study" International Journal of Environmental Research and Public Health 17, no. 10: 3477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103477